
Application of Magnetic Resonance Strain Analysis Using Feature Tracking in a Myocardial Infarction Model

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal Preparation
2.2. Magnetic Resonance Imaging
2.3. MRI Data Analysis
2.4. Statistical Analysis
3. Results
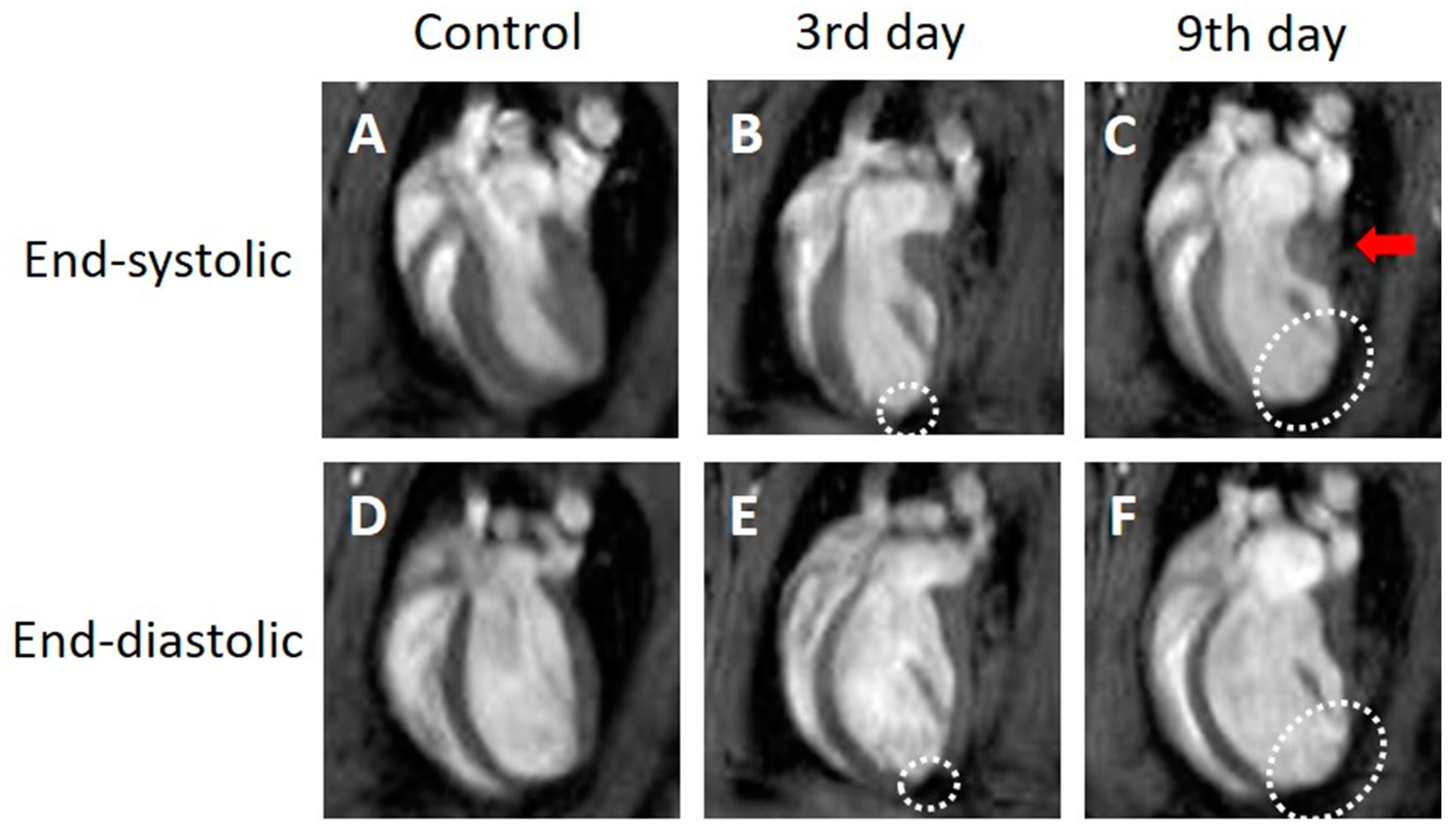
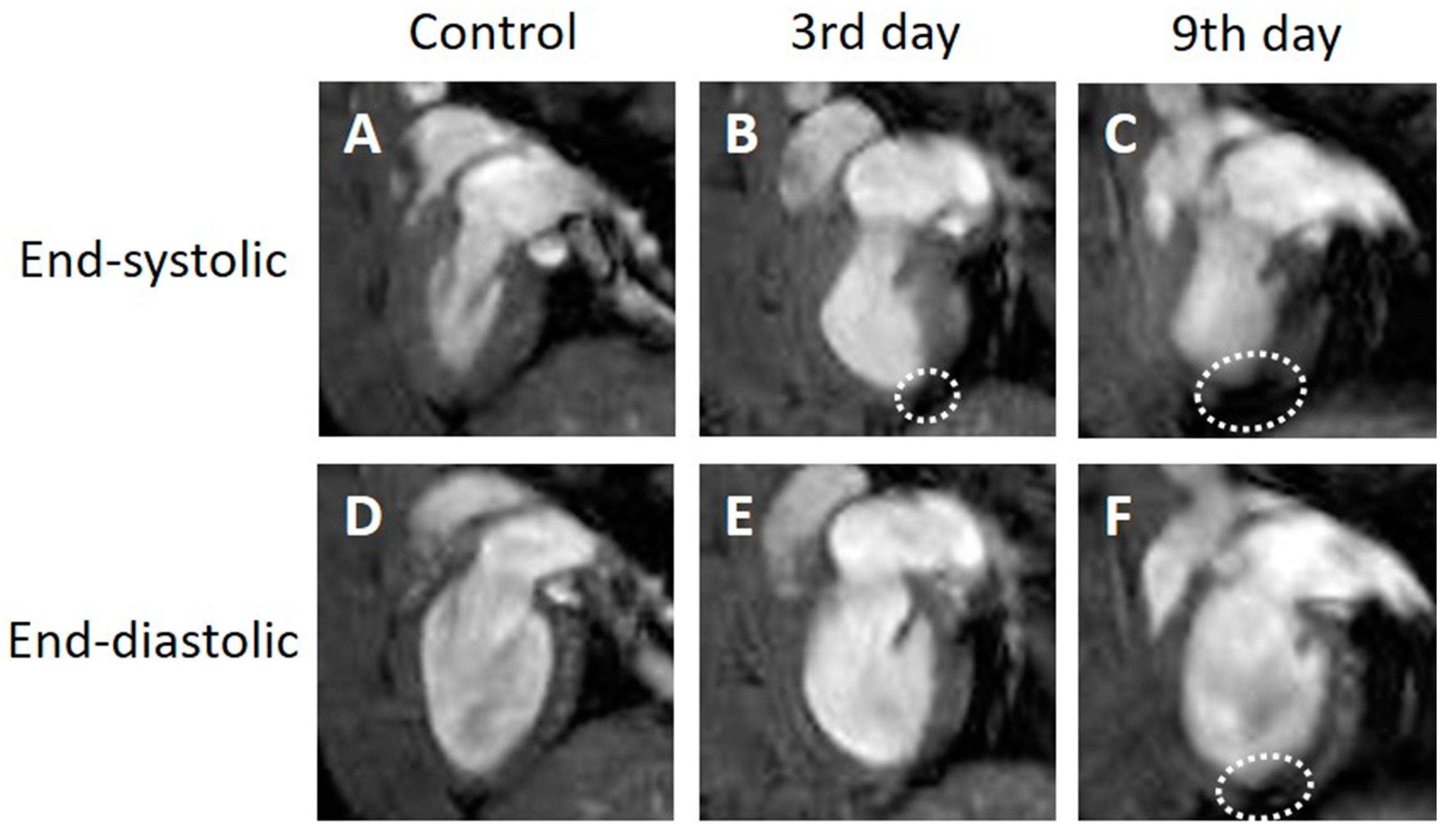
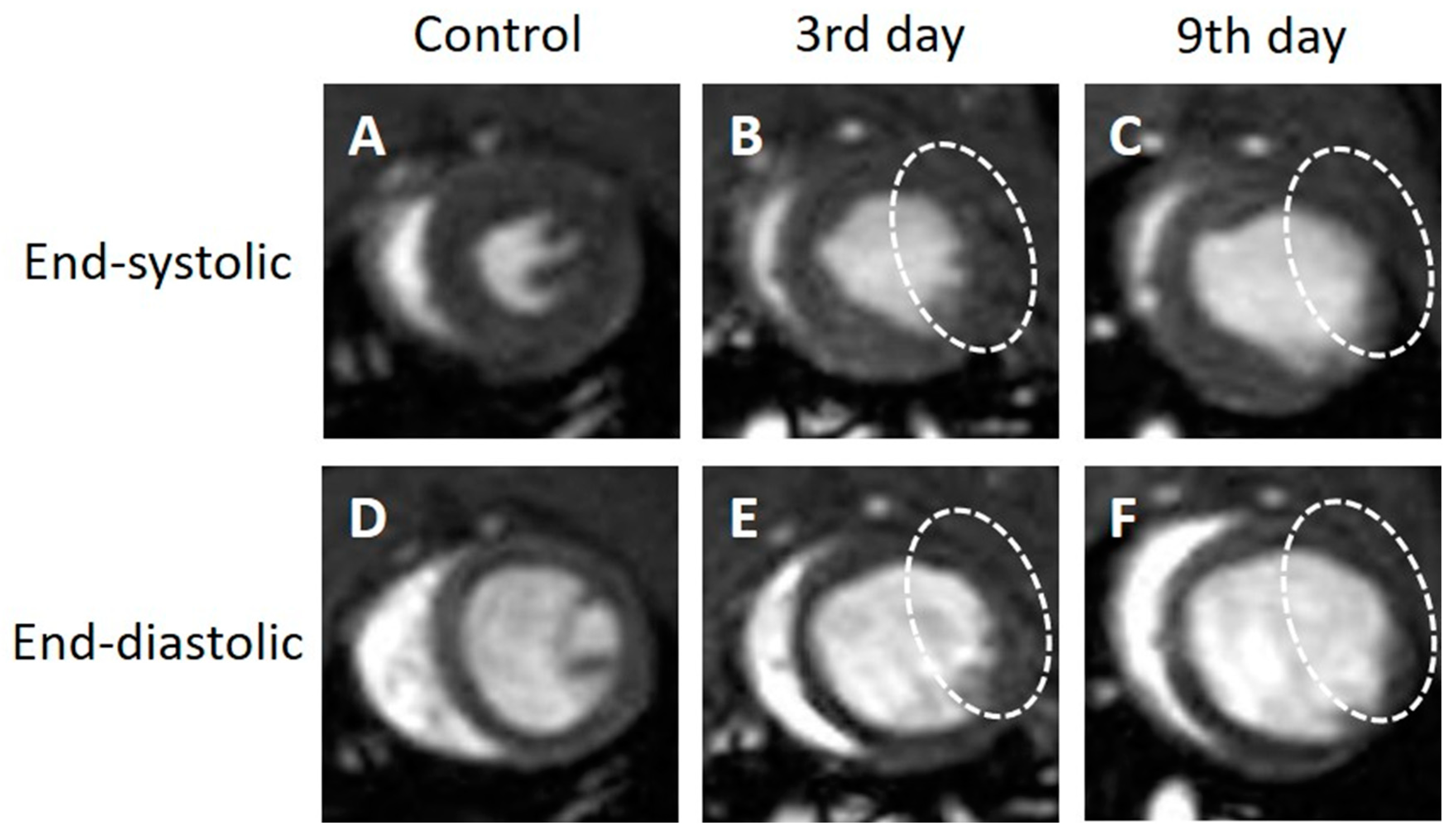
3.1. Observation with Cine Imaging
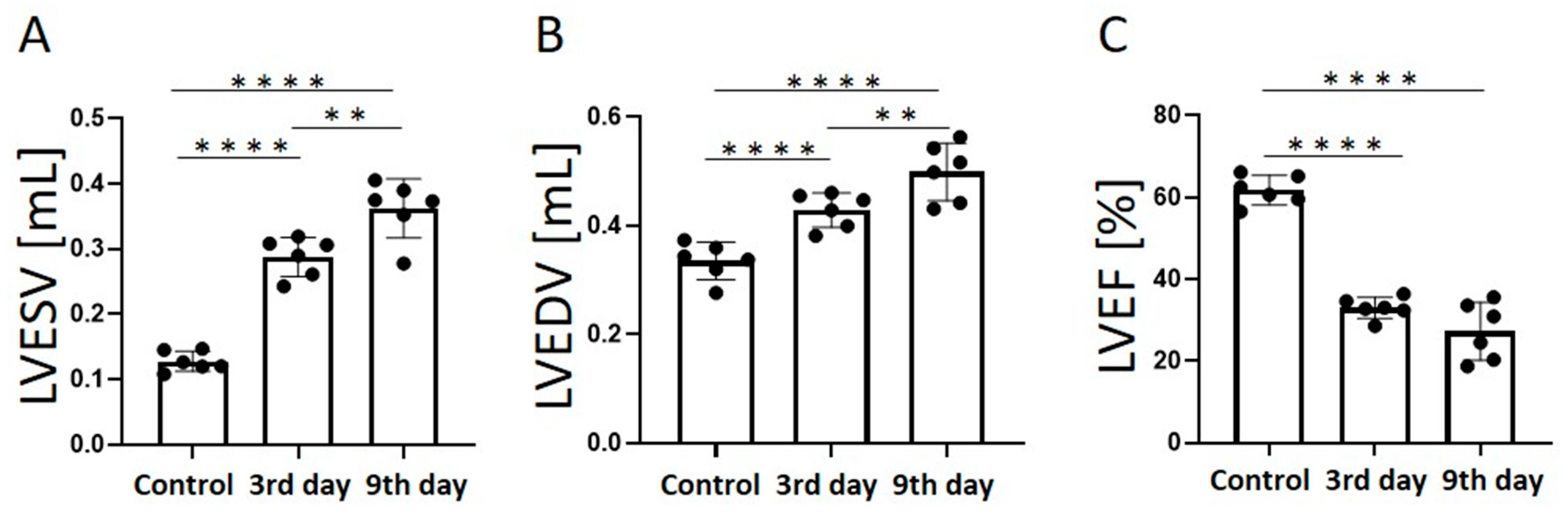
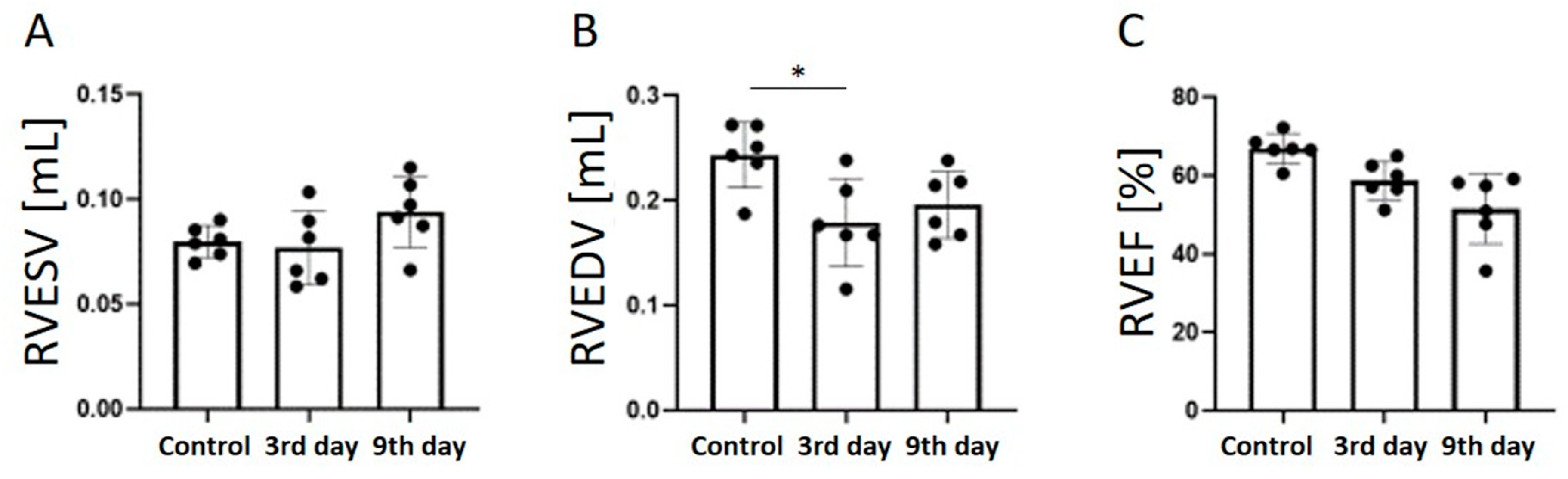
3.2. Comparison of Quantitative Values
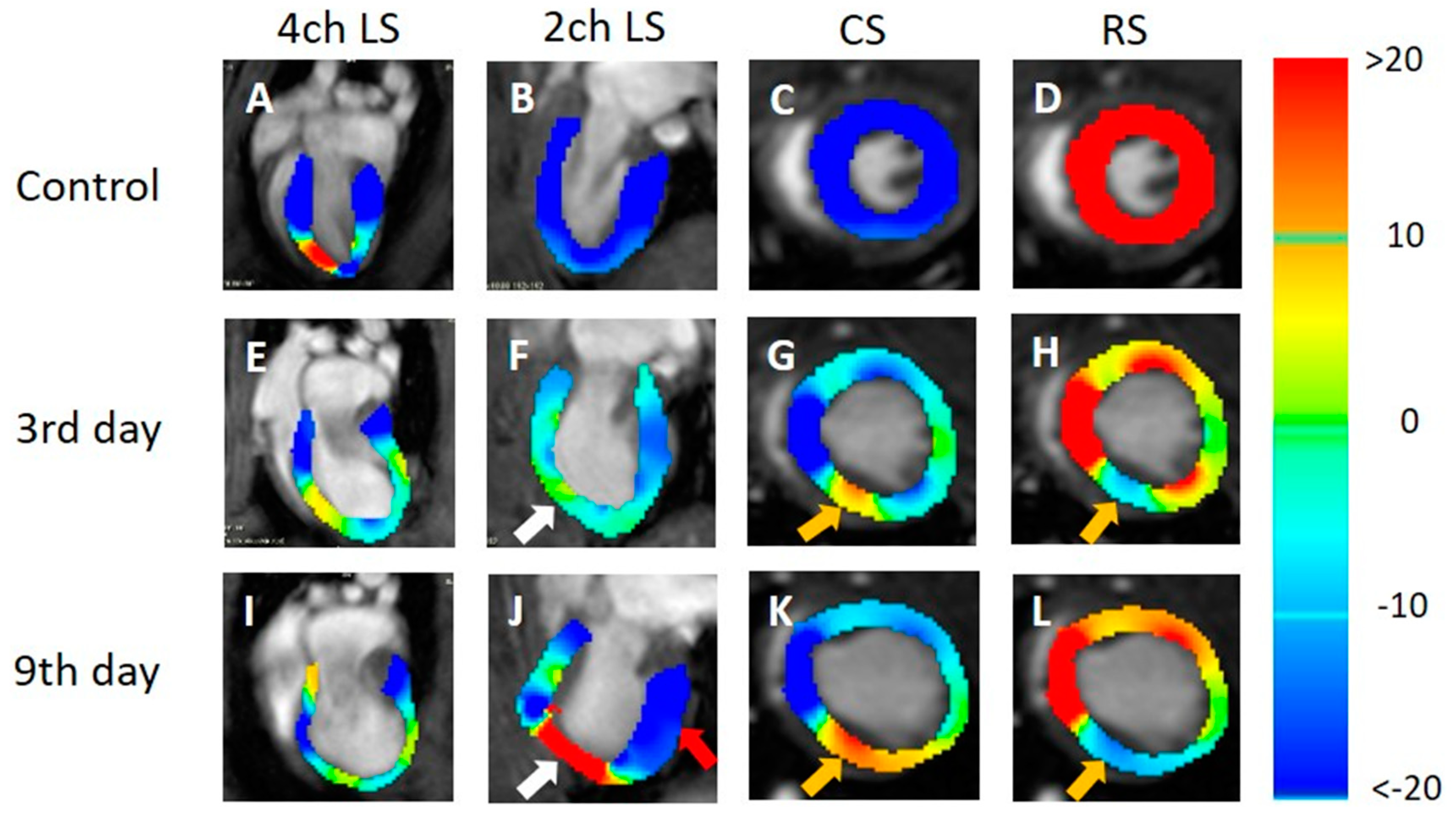
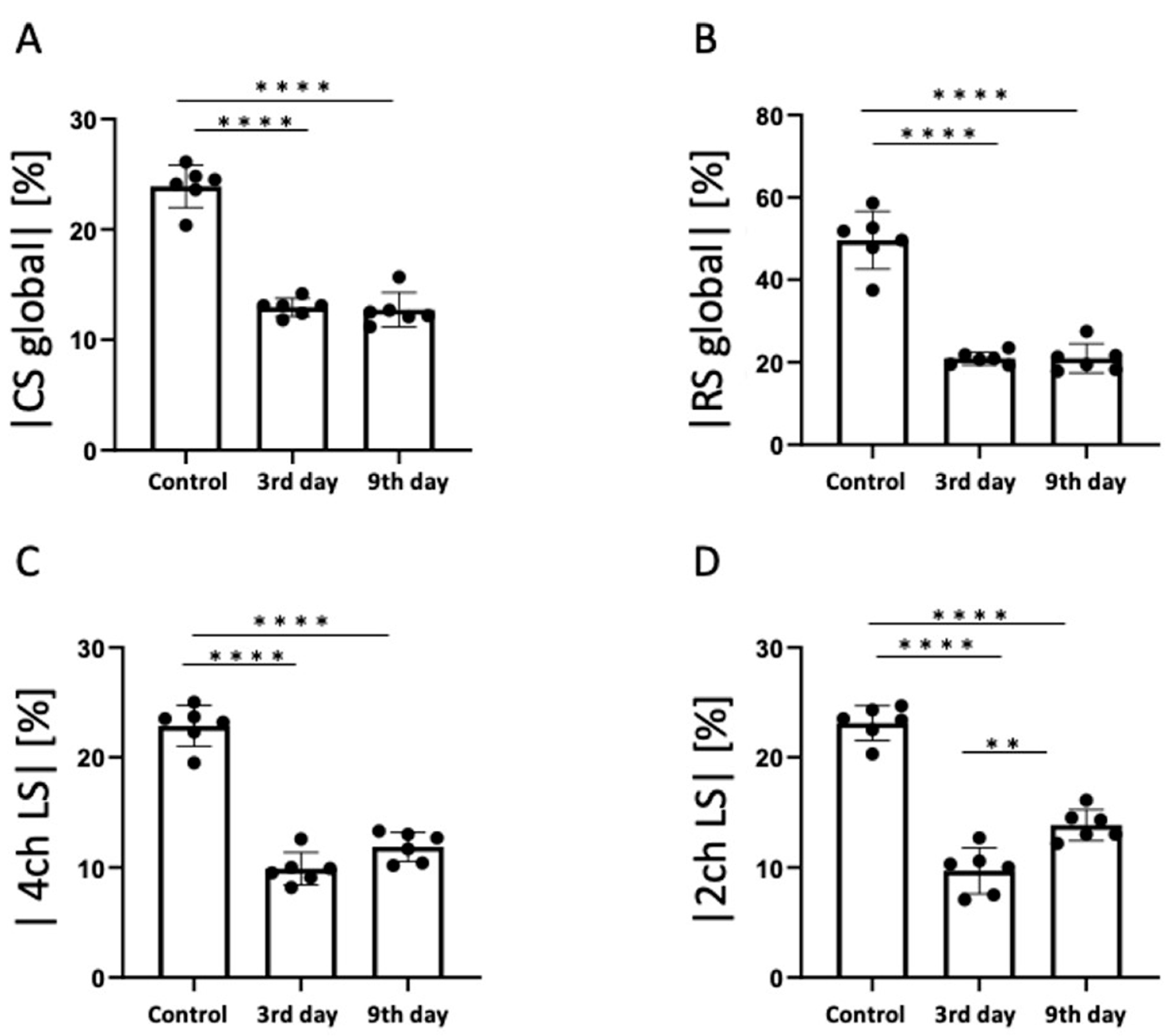
3.3. Strain Analysis Results
4. Discussion
4.1. Cardiac Function of the MI Model
4.2. LS Analysis of the MI Model
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lu, L.; Liu, M.; Sun, R.; Zheng, Y.; Zhang, P. Myocardial Infarction: Symptoms and Treatments. Cell Biochem. Biophys. 2015, 72, 865–867. [Google Scholar] [CrossRef]
- Manka, R.; Jahnke, C.; Hucko, T.; Dietrich, T.; Gebker, R.; Schnackenburg, B.; Graf, K.; Paetsch, I. Reproducibility of small animal cine and scar cardiac magnetic resonance imaging using a clinical 3.0 tesla system. BMC Med. Imaging 2013, 13, 44. [Google Scholar] [CrossRef] [PubMed]
- Hara, A.; Kobayashi, H.; Asai, N.; Saito, S.; Higuchi, T.; Kato, K.; Okumura, T.; Bando, Y.K.; Takefuji, M.; Mizutani, Y.; et al. Roles of the Mesenchymal Stromal/Stem Cell Marker Meflin in Cardiac Tissue Repair and the Development of Diastolic Dysfunction. Circ. Res. 2019, 125, 414–430. [Google Scholar] [CrossRef]
- Saito, S.; Masuda, K.; Mori, Y.; Nakatani, S.; Yoshioka, Y.; Murase, K. Mapping of left ventricle wall thickness in mice using 11.7-T magnetic resonance imaging. Magn. Reson. Imaging 2017, 36, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Tanoue, M.; Masuda, K.; Mori, Y.; Nakatani, S.; Yoshioka, Y.; Murase, K. Longitudinal observations of progressive cardiac dysfunction in a cardiomyopathic animal model by self-gated cine imaging based on 11.7-T magnetic resonance imaging. Sci. Rep. 2017, 7, 9106. [Google Scholar] [CrossRef]
- Price, A.N.; Cheung, K.K.; Cleary, J.O.; Campbell, A.E.; Riegler, J.; Lythgoe, M.F. Cardiovascular magnetic resonance imaging in experimental models. Open Cardiovasc. Med. J. 2010, 4, 278–292. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Abaei, A.; Metze, P.; Just, S.; Lu, Q.; Rasche, V. Technical Aspects of in vivo Small Animal CMR Imaging. Front. Phys. 2020, 8, 183. [Google Scholar] [CrossRef]
- Lopez, D.; Pan, J.A.; Pollak, P.M.; Clarke, S.; Kramer, C.M.; Yeager, M.; Salerno, M. Multiparametric CMR imaging of infarct remodeling in a percutaneous reperfused Yucatan mini-pig model. NMR Biomed. 2017, 30, e3693. [Google Scholar] [CrossRef]
- Cadeddu Dessalvi, C.; Deidda, M.; Farci, S.; Longu, G.; Mercuro, G. Early ischemia identification employing 2D speckle tracking selective layers analysis during dobutamine stress echocardiography. Echocardiography 2019, 36, 2202–2208. [Google Scholar] [CrossRef] [PubMed]
- Romano, S.; Judd, R.M.; Kim, R.J.; Kim, H.W.; Klem, I.; Heitner, J.F.; Shah, D.J.; Jue, J.; White, B.E.; Indorkar, R.; et al. Feature-Tracking Global Longitudinal Strain Predicts Death in a Multicenter Population of Patients With Ischemic and Nonischemic Dilated Cardiomyopathy Incremental to Ejection Fraction and Late Gadolinium Enhancement. JACC Cardiovasc. Imaging 2018, 11, 1419–1429. [Google Scholar] [CrossRef]
- Garot, J.; Bluemke, D.A.; Osman, N.F.; Rochitte, C.E.; McVeigh, E.R.; Zerhouni, E.A.; Prince, J.L.; Lima, J.A. Fast determination of regional myocardial strain fields from tagged cardiac images using harmonic phase MRI. Circulation 2000, 101, 981–988. [Google Scholar] [CrossRef]
- Li, W.; Yu, X. Quantification of myocardial strain at early systole in mouse heart: Restoration of undeformed tagging grid with single-point HARP. J. Magn. Reson. Imaging 2010, 32, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Lavelle-Jones, M.; Scott, M.H.; Kolterman, O.; Moossa, A.R.; Olefsky, J.M. Non-insulin-mediated glucose uptake predominates in postabsorptive dogs. Am. J. Physiol. 1987, 252, E660–E666. [Google Scholar] [CrossRef] [PubMed]
- Espe, E.K.S.; Aronsen, J.M.; Norden, E.S.; Zhang, L.; Sjaastad, I. Regional right ventricular function in rats: A novel magnetic resonance imaging method for measurement of right ventricular strain. Am. J. Physiol. Heart Circ. Physiol. 2020, 318, H143–H153. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.Q.; Zhang, X.; Wenk, J.F. Quantification of regional right ventricular strain in healthy rats using 3D spiral cine dense MRI. J. Biomech. 2019, 94, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Bhatti, S.; Vallurupalli, S.; Ambach, S.; Magier, A.; Watts, E.; Truong, V.; Hakeem, A.; Mazur, W. Myocardial strain pattern in patients with cardiac amyloidosis secondary to multiple myeloma: A cardiac MRI feature tracking study. Int. J. Cardiovasc. Imaging 2018, 34, 27–33. [Google Scholar] [CrossRef]
- Tsadok, Y.; Friedman, Z.; Haluska, B.A.; Hoffmann, R.; Adam, D. Myocardial strain assessment by cine cardiac magnetic resonance imaging using non-rigid registration. Magn. Reson. Imaging 2016, 34, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Houser, S.R.; Margulies, K.B.; Murphy, A.M.; Spinale, F.G.; Francis, G.S.; Prabhu, S.D.; Rockman, H.A.; Kass, D.A.; Molkentin, J.D.; Sussman, M.A.; et al. Animal models of heart failure: A scientific statement from the American Heart Association. Circ. Res. 2012, 111, 131–150. [Google Scholar] [CrossRef]
- Saito, S.; Takahashi, Y.; Ohki, A.; Shintani, Y.; Higuchi, T. Early detection of elevated lactate levels in a mitochondrial disease model using chemical exchange saturation transfer (CEST) and magnetic resonance spectroscopy (MRS) at 7T-MRI. Radiol. Phys. Technol. 2019, 12, 46–54. [Google Scholar] [CrossRef]
- Ohki, A.; Saito, S.; Hirayama, E.; Takahashi, Y.; Ogawa, Y.; Tsuji, M.; Higuchi, T.; Fukuchi, K. Comparison of Chemical Exchange Saturation Transfer Imaging with Diffusion-weighted Imaging and Magnetic Resonance Spectroscopy in a Rat Model of Hypoxic-ischemic Encephalopathy. Magn. Reson. Med. Sci. 2020, 19, 359–365. [Google Scholar] [CrossRef]
- Bucius, P.; Erley, J.; Tanacli, R.; Zieschang, V.; Giusca, S.; Korosoglou, G.; Steen, H.; Stehning, C.; Pieske, B.; Pieske-Kraigher, E.; et al. Comparison of feature tracking, fast-SENC, and myocardial tagging for global and segmental left ventricular strain. ESC Heart Fail. 2020, 7, 523–532. [Google Scholar] [CrossRef]
- Yang, L.; Cao, S.; Liu, W.; Wang, T.; Xu, H.; Gao, C.; Zhang, L.; Wang, K. Cardiac Magnetic Resonance Feature Tracking: A Novel Method to Assess Left Ventricular Three-Dimensional Strain Mechanics After Chronic Myocardial Infarction. Acad. Radiol. 2021, 28, 619–627. [Google Scholar] [CrossRef]
- Thomas, D.; Ferrari, V.A.; Janik, M.; Kim, D.H.; Pickup, S.; Glickson, J.D.; Zhou, R. Quantitative assessment of regional myocardial function in a rat model of myocardial infarction using tagged MRI. MAGMA 2004, 17, 179–187. [Google Scholar] [CrossRef]
- Kerkhof, P.L.M.; van de Ven, P.M.; Yoo, B.; Peace, R.A.; Heyndrickx, G.R.; Handly, N. Ejection fraction as related to basic components in the left and right ventricular volume domains. Int. J. Cardiol. 2018, 255, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, H.; Taki, J.; Inaki, A.; Hiromasa, T.; Yamase, T.; Akatani, N.; Okuda, K.; Shibutani, T.; Shiba, K.; Kinuya, S. Prognostic Value of Early Evaluation of Left Ventricular Dyssynchrony After Myocardial Infarction. Mol. Imaging Biol. 2019, 21, 654–659. [Google Scholar] [CrossRef] [PubMed]
- Espe, E.K.S.; Aronsen, J.M.; Eriksen, M.; Sejersted, O.M.; Zhang, L.; Sjaastad, I. Regional Dysfunction After Myocardial Infarction in Rats. Circ. Cardiovasc. Imaging 2017, 10, e005997. [Google Scholar] [CrossRef] [PubMed]
- Epstein, F.H.; Yang, Z.; Gilson, W.D.; Berr, S.S.; Kramer, C.M.; French, B.A. MR tagging early after myocardial infarction in mice demonstrates contractile dysfunction in adjacent and remote regions. Magn. Reson. Med. 2002, 48, 399–403. [Google Scholar] [CrossRef]
- Lapinskas, T.; Kelle, S.; Grune, J.; Foryst-Ludwig, A.; Meyborg, H.; Jeuthe, S.; Wellnhofer, E.; Elsanhoury, A.; Pieske, B.; Gebker, R.; et al. Serelaxin Improves Regional Myocardial Function in Experimental Heart Failure: An In Vivo Cardiac Magnetic Resonance Study. J. Am. Heart Assoc. 2020, 9, e013702. [Google Scholar] [CrossRef]
- Lapinskas, T.; Grune, J.; Zamani, S.M.; Jeuthe, S.; Messroghli, D.; Gebker, R.; Meyborg, H.; Kintscher, U.; Zaliunas, R.; Pieske, B.; et al. Cardiovascular magnetic resonance feature tracking in small animals—A preliminary study on reproducibility and sample size calculation. BMC Med. Imaging 2017, 17, 51. [Google Scholar] [CrossRef]
- Ricci, D.R.; Orlick, A.E.; Alderman, E.L.; Ingels, N.B., Jr.; Daughters, G.T., 2nd; Stinson, E.B. Influence of heart rate on left ventricular ejection fraction in human beings. Am. J. Cardiol. 1979, 44, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Boettler, P.; Hartmann, M.; Watzl, K.; Maroula, E.; Schulte-Moenting, J.; Knirsch, W.; Dittrich, S.; Kececioglu, D. Heart rate effects on strain and strain rate in healthy children. J. Am. Soc. Echocardiogr. 2005, 18, 1121–1130. [Google Scholar] [CrossRef] [PubMed]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Onishi, R.; Ueda, J.; Ide, S.; Koseki, M.; Sakata, Y.; Saito, S. Application of Magnetic Resonance Strain Analysis Using Feature Tracking in a Myocardial Infarction Model. Tomography 2023, 9, 871-882. https://doi.org/10.3390/tomography9020071
Onishi R, Ueda J, Ide S, Koseki M, Sakata Y, Saito S. Application of Magnetic Resonance Strain Analysis Using Feature Tracking in a Myocardial Infarction Model. Tomography. 2023; 9(2):871-882. https://doi.org/10.3390/tomography9020071
Chicago/Turabian StyleOnishi, Ryutaro, Junpei Ueda, Seiko Ide, Masahiro Koseki, Yasushi Sakata, and Shigeyoshi Saito. 2023. "Application of Magnetic Resonance Strain Analysis Using Feature Tracking in a Myocardial Infarction Model" Tomography 9, no. 2: 871-882. https://doi.org/10.3390/tomography9020071