


The Efficacy of CT Temporal Subtraction Images for Fibrodysplasia Ossificans Progressiva
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Generation of TS Images
2.3. Searching Ectopic Bone Lesions
2.4. Evaluation of TS Images
- Survey 1: The visibility of lesion changes on a per-lesion basis (0, difficult to see; 1, slightly difficult to see; 2, neither hard nor easy to see; 3, slightly easy to see; 4, easy to see).
- Survey 2: The usefulness of TS images to identify lesions on a per-lesion basis (0, useless; 1, not very useful; 2, somewhat useful; 3, very useful; 4, extremely useful).
- Survey 3: The confidence level of the interpreter in their interpretation of each scan (0, very low; 1, low; 2, moderate; 3, high; 4, very high).
2.5. Statistical Analysis
3. Results
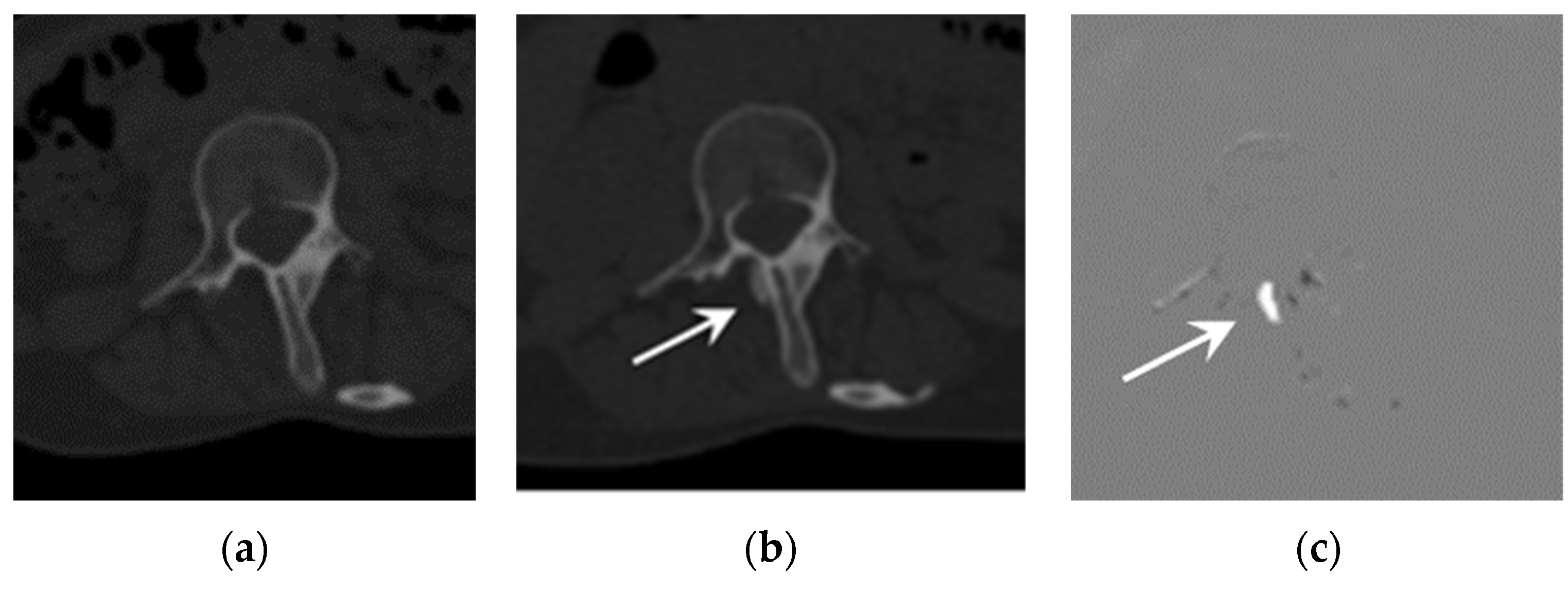
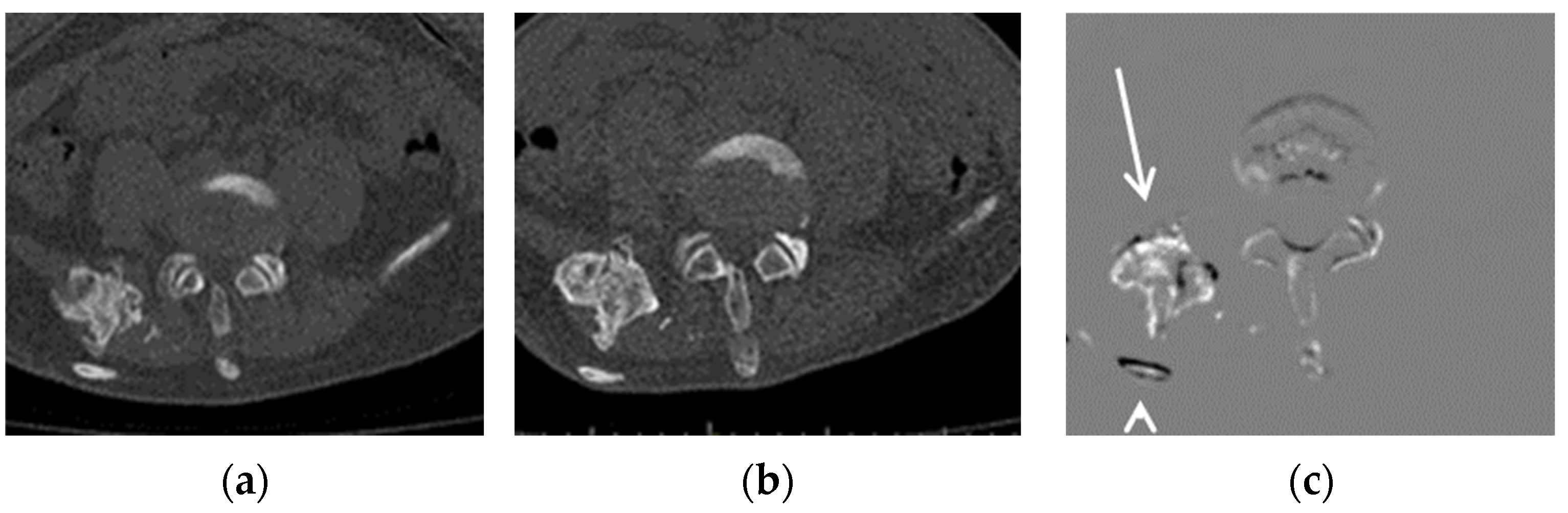
Representative Cases
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pignolo, R.J.; Baujat, G.; Brown, M.A.; De Cunto, C.; Di Rocco, M.; Hsiao, E.C.; Keen, R.; Mukaddam, M.A.; Sang, K.-H.L.Q.; Wilson, A.; et al. Natural history of fibrodysplasia ossificans progressiva: Cross-sectional analysis of annotated baseline phenotypes. Orphanet J. Rare Dis. 2019, 14, 98. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, F.S.; Zasloff, M.A.; Kitterman, J.A.; Shore, E.M.; Hong, C.C.; Rocke, D.M. Early mortality and cardiorespiratory failure in patients with fibrodysplasia ossificans progressiva. J. Bone Jt. Surg. Am. Vol. 2010, 92, 686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smilde, B.J.; Botman, E.; de Ruiter, R.D.; Smit, J.M.; Teunissen, B.P.; Lubbers, W.D.; Schwarte, L.A.; Schober, P.; Eekhoff, E.M.W. Monitoring and Management of Fibrodysplasia Ossificans Progressiva: Current Perspectives. Orthop. Res. Rev. 2022, 14, 113. [Google Scholar] [CrossRef] [PubMed]
- Al Mukaddam, M.; Rajapakse, C.S.; Pignolo, R.J.; Kaplan, F.S.; Smith, S.E. Imaging assessment of fibrodysplasia ossificans progressiva: Qualitative, quantitative and questionable. Bone 2018, 109, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Rajapakse, C.S.; Lindborg, C.; Wang, H.; Newman, B.T.; Kobe, E.A.; Chang, G.; Shore, E.M.; Kaplan, F.S.; Pignolo, R.J. Analog method for radiographic assessment of heterotopic bone in fibrodysplasia ossificans progressiva. Acad. Radiol. 2017, 24, 321–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warner, S.E.; Kaplan, F.S.; Pignolo, R.J.; Smith, S.E.; Hsiao, E.C.; De Cunto, C.; Rocco, M.D.; Harnett, K.; Grogan, D.; Genant, H.K. Whole-body Computed Tomography Versus Dual Energy X-ray Absorptiometry for Assessing Heterotopic Ossification in Fibrodysplasia Ossificans Progressiva. Calcif. Tissue Int. 2021, 109, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Ishida, T.; Ashizawa, K.; Engelmann, R.; Katsuragawa, S.; MacMahon, H.; Doi, K. Application of temporal subtraction for detection of interval changes on chest radiographs: Improvement of subtraction images using automated initial image matching. J. Digit. Imaging 1999, 12, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abe, H.; Ishida, T.; Shiraishi, J.; Li, F.; Katsuragawa, S.; Sone, S.; MacMahon, H.; Doi, K. Effect of temporal subtraction images on radiologists’ detection of lung cancer on CT: Results of the observer performance study with use of film computed tomography images1. Acad. Radiol. 2004, 11, 1337–1343. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, R.; Mori, S.; Miller, M.I.; Okada, T.; Togashi, K. Detection of time-varying structures by large deformation diffeomorphic metric mapping to aid reading of high-resolution CT images of the lung. PLoS ONE 2014, 9, e85580. [Google Scholar] [CrossRef] [PubMed]
- Aoki, T.; Murakami, S.; Kim, H.; Fujii, M.; Takahashi, H.; Oki, H.; Hayashida, Y.; Katsuragawa, S.; Shiraishi, J.; Korogi, Y. Temporal subtraction method for lung nodule detection on successive thoracic CT soft-copy images. Radiology 2014, 271, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Hoff, B.A.; Toole, M.; Yablon, C.; Ross, B.D.; Luker, G.D.; Van Poznak, C.; Galbán, C.J. Potential for Early Fracture Risk Assessment in Patients with Metastatic Bone Disease Using Parametric Response Mapping of CT Images. Tomography 2015, 1, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, R.; Yakami, M.; Fujimoto, K.; Nakagomi, K.; Kubo, T.; Emoto, Y.; Akasaka, T.; Aoyama, G.; Yamamoto, H.; Miller, M.I.; et al. Temporal subtraction of serial CT images with large deformation diffeomorphic metric mapping in the identification of bone metastases. Radiology 2017, 285, 629–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akasaka, T.; Yakami, M.; Nishio, M.; Onoue, K.; Aoyama, G.; Nakagomi, K.; Iizuka, Y.; Kubo, T.; Emoto, Y.; Satoh, K.; et al. Detection of suspected brain infarctions on CT can be significantly improved with temporal subtraction images. Eur. Radiol. 2019, 29, 759–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onoue, K.; Nishio, M.; Yakami, M.; Aoyama, G.; Nakagomi, K.; Iizuka, Y.; Kubo, T.; Emoto, Y.; Akasaka, T.; Satoh, K.; et al. CT temporal subtraction improves early detection of bone metastases compared to SPECT. Eur. Radiol. 2019, 29, 5673–5681. [Google Scholar] [CrossRef] [PubMed]
- Onoue, K.; Yakami, M.; Nishio, M.; Sakamoto, R.; Aoyama, G.; Nakagomi, K.; Iizuka, Y.; Kubo, T.; Emoto, Y.; Akasaka, T.; et al. Temporal subtraction CT with nonrigid image registration improves detection of bone metastases by radiologists: Results of a large-scale observer study. Sci. Rep. 2021, 11, 18422. [Google Scholar] [CrossRef]
- Pignolo, R.J.; Shore, E.M.; Kaplan, F.S. Fibrodysplasia ossificans progressiva: Diagnosis, management, and therapeutic horizons. Pediatr. Endocrinol. Rev. 2013, 10 (Suppl. S2), 437–448. [Google Scholar] [PubMed]
- Aoki, T.; Kamiya, T.; Lu, H.; Terasawa, T.; Ueno, M.; Hayashida, Y.; Murakami, S.; Korogi, Y. CT temporal subtraction: Techniques and clinical applications. Quant. Imaging Med. Surg. 2021, 11, 2214. [Google Scholar] [CrossRef] [PubMed]
- Carlier, R.Y.; Safa, D.M.L.; Parva, P.; Mompoint, D.; Judet, T.; Denormandie, P.; Vallée, C.A. Ankylosing neurogenic myositis ossificans of the hip: An enhanced volumetric CT study. J. Bone Jt. Surg. Br. Vol. 2005, 87, 301–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Interval 1 | Interval 2 | Interval 3 | |||||
|---|---|---|---|---|---|---|---|
| Emerging | Growing | Emerging | Growing | Emerging | Growing | ||
| Case A | 0 | 6 | 0 | 5 | n/a | n/a | |
| Case B | 0 | 2 | 0 | 3 | n/a | n/a | |
| Case C | 4 | 4 | 4 | 6 | 4 | 5 | |
| Total | 4 | 12 | 4 | 14 | 4 | 5 | 43 |
| Resident A | Resident B | Radiologist A | Radiologist B | ||
|---|---|---|---|---|---|
| Sensitivity (%) | Without TS | 25.6 | 14.0 | 16.3 | 20.9 |
| With TS | 51.2 | 30.2 | 41.9 | 46.5 | |
| Number of false-positive cases | Without TS | 0 | 0 | 2 | 0 |
| With TS | 7 | 3 | 1 | 1 |
| Resident A | Resident B | Radiologist A | Radiologist B | ||
|---|---|---|---|---|---|
| Survey 1 | Without TS | 2 (0–4) | 2 (0–3) | 2 (0–4) | 4 (0–4) |
| With TS | 1.5 (0–4) | 2 (1–3) | 2 (1–4) | 4 (3–4) | |
| Survey 2 | 3 (0–4) | 3 (1–4) | 4 (0–4) | 4 (1–4) | |
| Survey 3 | Without TS | 3 (1–3) | 0 (0–2) | 2 (1–3) | 4 (4–4) |
| With TS | 2 (2–4) | 0 (0–2) | 3 (3–4) * | 3 (1–4) | |
| Reading time | Without TS | 718 ± 266 | 1543 ± 477 | 814 ± 162 | 429 ± 160 |
| With TS | 1920 ± 876 | 891 ± 258 | 780 ± 211 | 437 ± 161 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iima, M.; Sakamoto, R.; Kakigi, T.; Yamamoto, A.; Otsuki, B.; Nakamoto, Y.; Toguchida, J.; Matsuda, S. The Efficacy of CT Temporal Subtraction Images for Fibrodysplasia Ossificans Progressiva. Tomography 2023, 9, 768-775. https://doi.org/10.3390/tomography9020062
Iima M, Sakamoto R, Kakigi T, Yamamoto A, Otsuki B, Nakamoto Y, Toguchida J, Matsuda S. The Efficacy of CT Temporal Subtraction Images for Fibrodysplasia Ossificans Progressiva. Tomography. 2023; 9(2):768-775. https://doi.org/10.3390/tomography9020062
Chicago/Turabian StyleIima, Mami, Ryo Sakamoto, Takahide Kakigi, Akira Yamamoto, Bungo Otsuki, Yuji Nakamoto, Junya Toguchida, and Shuichi Matsuda. 2023. "The Efficacy of CT Temporal Subtraction Images for Fibrodysplasia Ossificans Progressiva" Tomography 9, no. 2: 768-775. https://doi.org/10.3390/tomography9020062