1. Introduction
Food allergies have been increasing in prevalence in the last two to three decades, with an overall life-time self-reported prevalence of 6% in Europe [
1]. Children diagnosed with a food allergy have a negatively impacted health-related quality of life (HRQL) [
2] and require specialist care from a paediatric allergist, allergy nurse, and dieticians to learn how to best avoid the allergen, as well as to know the correct management of allergic reactions in the case of accidental exposure.
Anaphylaxis is considered to be a severe allergic reaction associated with lower respiratory or cardiovascular features [
3], which is rapid in onset and occasionally fatal [
4]. The literature reports a global (United Kingdom, Europe, United States, Australia, New Zealand) increase in incidence of hospitalizations for anaphylaxis [
5], with the highest incidence of fatal anaphylaxis due to food allergy occurring in the second decade of life [
6].
Adrenaline is the mainstay of treatment of anaphylaxis [
4]. In a community setting, an adrenaline auto-injector (AAI) is used [
3]. Parents and children who have been prescribed an AAI should be given instruction and guidance on when and how to use it by a trained healthcare professional [
3]. However, in a systematic review, a correct AAI administration technique was shown to be low, with only 32% of parents/caregivers successfully demonstrating correct AAI technique [
7]. Similar findings were found in a recent review of the literature, regarding the effectiveness of educational intervention on AAI administration ability, where it was found that the AAI administration success among parents ranged significantly, and the success rates varied from 5.6 to 84% [
8]. This may reflect several issues, including training effectiveness or lack of training, user stress during administration, or inherent differences consequent of the design of the individual auto-injector [
3].
Adrenaline can be administered by several different brands of AAI, each with a unique design. There are four brands of AAI available in Ireland—Epipen
®, Jext
®, and Anapen
® are three. Another brand, Emerade
®, has been recalled from the market in recent years [
9]. As the number of different AAI designs has increased, device switches could become a significant clinical issue [
6].
There has been no previous research in Ireland documenting the prevalence of AAI brands or the frequency at which caregivers switch brands. Similarly, possible factors, which influence the switching of brands of AAI, have not been explored.
The aim of this study is to explore the usage of different brands of adrenaline auto-injectors among caregivers of children with food allergies in Ireland.
2. Methods
2.1. Study Setting and Sample
This is a cross-sectional study, which took place in the paediatric allergy clinic in Cork University Hospital, Cork, Ireland. Participants were caregivers of children with food allergies who had attended the paediatric allergy clinic. Inclusion criteria were parents or guardians of children under the age of 18, who had been diagnosed with an IgE-mediated food allergy, who had received previous training in anaphylaxis management and AAI administration, and who were currently prescribed an adrenaline auto injector for their food allergy. Exclusion criteria were patients with drug or venom allergies. Ethical approval was received by the Clinical Research Ethics Committee of the Cork Teaching Hospitals (Reference code: ECM 4 (hh) 12/01/2021 & 3 (w) 09/03/2021).
2.2. Data Collection Methods
An online questionnaire was designed for data collection in this study. This questionnaire was designed as part of a larger study entitled Telemedicine as an Educational Tool Regarding Adrenaline Auto Injectors and Anaphylaxis Management (TEAAMs), with a section of this questionnaire dedicated to data collection for this study. As there were no such questions found focusing on usage of different brands of AAI in the literature, questions were designed and validated amongst a pilot group of three parents, a consultant paediatric allergist, and an allergy nurse specialist. Small modifications were made based on the feedback from this pilot group before inclusion in the final questionnaire.
2.3. Data Collection
Considering the COVID 19 pandemic, participants were identified from a retrospective chart review to minimize patient contact and adhere to social distancing restrictions, and informed consent was obtained remotely.
Potential study participants were contacted initially by phone and asked if they were interested in taking part in the larger TEAAMs study, as well as the present study. Phone call attempts were made to each caregiver at least twice. During this telephone call, they were screened for eligibility, which may not have been apparent in their patient file. Eligible participants were sent an e-mail containing detailed study information. They were given the opportunity to ask further questions by email or telephone. Once happy to proceed, they remotely completed informed consent and completed the online questions. Emails to remind interested caregivers to complete the questionnaire were sent three times if they had not completed the questionnaire. Google Forms was used to capture study responses.
Participants were asked questions relating to: socio-economic demographics (age of child, age of parent, gender of child, relationship to child household income, and level of education reached by caregiver), the child’s allergy history, and questions relating to AAI usage, such as whether participants have changed brands of AAI before and what influenced this change, what training they received from a healthcare professional when they changed the brand of AAI they used, which brands of AAI they have used, and what preferences they may have and open questions asking why they preferred an AAI brand/found an AAI brand easier to use.
2.4. Statistical Analysis
SPSS version 28 (IBM, n.d.) [
10] was employed for statistical analysis. Descriptive statistical methods, including observation ranking using mean, was used. These descriptive methods were employed to characterize the population, e.g., age of child, age of parent, type of allergy, and mean household income, and they were used to explore the proportion of caregivers that have different brands of AAI. Chi-square tests were used to explore associations between demographic data and responses, with differences at a level of 95% confidence probability and above regarded as statistically significant. Examples of this include the age of the child and whether they have changed brands of AAI. Free-text responses, regarding why they preferred a particular brand of AAI, were entered into MS Word and were thematically analysed, as outlined by Braun and Clarke 2006 [
11].
3. Results
3.1. Study Participants
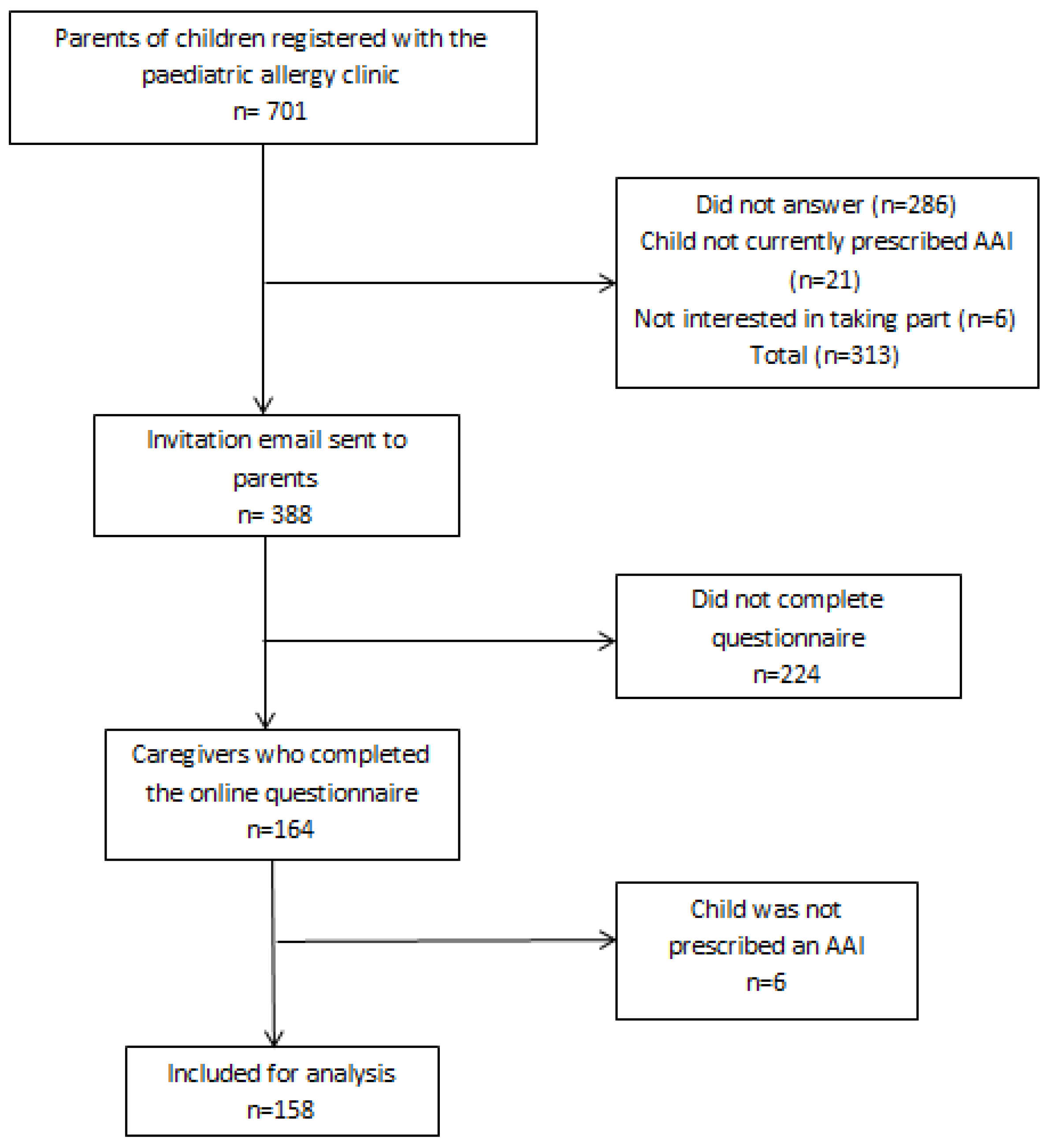
A total of 701 parents were contacted between June 2021 and May 2022. Of them, 313 could not be reached by telephone or did not meet eligibility criteria when screened. An invitation email was sent to 388 parents to take part in the study. A total of 164 responses were received to the Google Forms questionnaire. This equates to a response rate of 42.2%. Six responses were excluded from analysis on further inspection, as they responded ‘No’ when asked if their child had been prescribed an AAI. Thus, 158 participants were included in the study. A flow diagram depicting the recruitment of participants to the study is shown in
Figure 1. A summary of participant demographics is shown in
Table 1.
3.2. Brands of AAI Used by Caregivers
Of the 158 participants whose child was prescribed an AAI, 121 (75.58%) reported their child carried Epipen®, 25 (15.82%) carried Jext®, and 12 (7.59%) carried Anapen®. No child carried Emerade®.
3.3. Switching Brands of AAI
An amount of 48.73% (n = 77) of caregivers had switched brands of AAI at least once before, with 20.9% (n = 33) switching brands once, 13.9% (n = 22) switching two times, 9.5% (n = 15) switching three times, and 4.43% (n = 7) switching more than three times.
Those who had switched brands in the past were asked the reason they switched brands. An amount of 46 (59.74%) caregivers said this was due to lack of availability of their previous AAI at their pharmacy, 16 (20.7%) said the expiration date of the new AAI was longer than their previous AAI, seven (9.1%) said the new AAI was recommended by their pharmacy, four (5.2%) stated the new brand was easier to use, two participants stated that their old AAI had been recalled from the market, and one participant stated that the previous AAI was too big and bulky for their child to carry.
An amount of 59.74% (n = 46) parents who had switched brands of AAI in the past did not receive formal training when they were switched to a new brand.
An amount of 153 caregiversresponded when asked what brands they had received training in. An amount of 112 (73.2%) stated they had received training in one brand of AAI in the past (87 Epipen®, 16 Jext®, 7 Anapen®, 2 Emerade®). An amount of 25 (16.3%) had received training in two of the four brands of AAI in the past. An amount of 13 (8.4%) stated to have received training in all three available brands of AAI in Ireland (Epipen®, Anapen®, Jext®).
There was an association between caregiver’s age and changing AAI (p = 0.02). In additions, it was found that 32.8% of patients whose parents are less than 40 years old changed AAI brand, while 59.6% of patients whose parents are ≥40 years old did change brands (p < 0.01). Globally, there was no association between household income and changing brand of AAI (p = 0.32). However, of patients with a house income >100,000 €, 14 (70%) changed AAI brand, while 61 (44.9%) of the 136 caregivers with a household income of <100,000 € changed brands (p = 0.04). An association was not found between any history of anaphylaxis and switching AAI brands (p = 0.195). However, a clear trend can be seen between increasing episodes of anaphylaxis and changing AAI brands. However, due to the small number of patients who had experienced multiple episodes of anaphylaxis, no statistical significance was found (p = 0.481). No association was found between changing brands of AAI and the child’s age (p = 0.09) or parent’s educational level (p = 0.44).
3.4. Preference of AAI
An amount of 65 caregivers who had switched brands of AAI at least once in the past responded when asked which brand of AAI, if any they preferred. 63.1% (n = 41) caregivers preferred Epipen®, 23.1% (n = 15) preferred Jext®, 6.15% (n = 4) preferred Emerade®, and 7.69 (n = 5) preferred Anapen®.
An amount of 53 participants responded to the open question, asking them to explain why they preferred a different brand. When responses were coded, the most common themes regarding preferred AAI brand referred to the device’s design, layout, training, and instructions.
3.4.1. Design
Many parents referred to the colour coding of the AAI device, which they believed helped them remember the correct steps of AAI administration.
“Different coloured parts, easier to differentiate between steps.”
“…blue to the sky/orange to the thigh.”
Caregivers also preferred AAI brands, which they described as having fewer steps involved in AAI administration and were therefore ‘more straightforward’.
“There were only 2 steps to the process of administering the AAI.”
“It’s a two step process pull out the blue stop and jab and hold.”
3.4.2. Layout
Caregivers preferred AAI brands, which gave clear and simple instructions on the device that could be followed with ease in an emergency.
“Visibly easier to use, as had arrows on pen to point which direction to use first.”
“Clear instructions, label not cluttered.”
3.4.3. Training
Many of the caregivers preferred an AAI brand because this was the brand they had received formal training in from a healthcare professional.
“This is the only brand I was trained in.”
“Because it was the one I was shown how to use in the first place.”
Many parents also appreciated receiving a trainer pen of this brand so that they could simulate its administration.
“I have a trainer pen for this type.”
Some parents also had more confidence in a particular AAI brand, as they have had to administer it in the past.
“I’m just more used to it. We have only ever actually used it once.”
3.4.4. Resources
Caregivers appreciated online resources available on different AAI brand websites. Others appreciated that the company sent a SMS when the device was expiring to remind the parent to obtain a new device.
“Jext have good online information.”
“…the EpiPen website also offers a free SMS expiry reminder system.”
Figure 2 summarises what features the ‘ideal’ AAI device should have based on the responses from caregivers.
4. Discussion
This study explores the perspective of different AAI devices by caregiversof children with food allergies in a paediatric allergy clinic in the south of Ireland.
Epipen
® appears to be the most used AAI among children with food allergies, followed by Jext and then Anapen
®. No children carried Emerade
®. This is significant, as, since Emerade
® was recalled from the Irish market in 2019 [
9], it was necessary to evaluate whether any parents were not aware of its recall and continued to carry it.
The finding of Epipen
® being the most carried pen was in line with our predictions. While the paediatric allergy clinic in Cork University Hospital does not recommend a particular brand when prescribing adrenaline, parents, children, and the general public consider ‘epipen’ to be synonymous with ‘adrenaline auto injector’. The wide availability of Epipen
® devices in pharmacies is the likely factor which influences the commonality of this device among those with food allergy. While no such similar studies have been conducted in Ireland or other European countries to our knowledge, these findings are supported by the previous literature from Canada, which found that Epipen
® and Epipen Jnr
® were the most commonly dispensed adrenaline devices over a five-year period (68.5% and 17.2%, respectively) [
12].
Switching brands of AAI is a common occurrence among parents of children with allergies, with almost half (48.73%) having switched brands at least once before. Patients of parents older than 40 years of age were more likely to have switched brands in the past. This is most likely associated with the longer duration of their child’s food allergy.
While switching devices occurs commonly in the community, parents’ preference is not the most common reason for switching, rather factors relating to the pharmacy are the most common reasons for switching. The majority of parents stated that their reason for switching devices was because their usual device was not available at their pharmacy or that their usual device had a shorter expiry. This is significant, as, while parents are often required to switch brands due to pharmacy factors, almost 2/3rds of the parents do not receive training in the administration of the new AAI. This is supported by the literature, which explored AAI training practices among pharmacists in the Netherlands, where only half (50%) of pharmacists demonstrated the use of the AAI when asked to fill out a prescription [
13]. Apart from many not offering training, none of the pharmacists in the study successfully demonstrated the correct use of the AAI [
13]. There is a need to explore the perspectives, beliefs, and attitudes of pharmacists in Ireland when prescribing adrenaline in order to develop practice guidelines for adequate prescribing of adrenaline in the community.
The high occurrence of switching brands of AAI among caregivers, as well as the suboptimal training in the different brands of AAI, are concerning findings. Research comparing the administration of different AAI devices and the effects of brand switching is sparse, with a recent review finding only three previous such studies [
8]. One study found that success rates dropped after switching between a one-cap (Epipen
® or Jext
®) and a two-cap (Anapen
®) device without training, (16/45, 36%), compared with participants switched between different single-cap devices (49/63, 78%;
p < 0.0001) [
14]. While the study found that AAI design, as well as adequate AAI training affect successful AAI administration, this study confirms the common occurrence of switching devices without receiving adequate training. There is, therefore, a need to examine the effects of the phenomenon of device switching on AAI administration among caregivers in Ireland.
It was found that most caregivers preferred the Epipen
® device (63%). This most likely correlates with Epipen
® being the most carried device and the familiarity of Epipen
® in the community. When parents who had switched brands in the past were asked why they preferred a particular brand, the main themes that emerged were layout, design, training, and online resources. Based on these findings, a figure representing the ‘ideal’ AAI device was created visually explaining these findings. These factors should also be considered when assessing AAI carriage among parents and young patients, as one recent review found that poor AAI design reduced the likelihood of AAI carriage among adolescents and young adults with food allergies [
15]. Of note was the high number of parents, which recited the rhyme ‘blue to the sky, orange to the thigh’, highlighting the value of clear and simple colour coding that is easily recalled in an emergency. Although it can be said that Epipen
® may be the most preferred AAI due to the high number of parents who carry it, it can be implied from parent responses that this may also be due to having only ever received training in the Epipen
® device, or that they have received training in this device most frequently, or even because they have had to use in a real-life scenario. These findings support EACCI recommendation of further study into the benefits of caregiver administration of an adrenaline auto injector during anaphylaxis during a hospital-based oral food challenge [
16]. This is supported by a randomised control trial, which found that anaphylaxis at food challenge, followed by self-administration of injected adrenaline, was associated with an increase in health-related quality of life (HRQL) and self-efficacy in young people with peanut allergy [
17].
4.1. Implications for Practitioners
Our study indicates that parents hold training and experience in the use of the AAI under the supervision of a trained healthcare professional in high esteem, regardless of the brand of AAI carried. This study supports the recommendation of EACCI in the long-term management of anaphylaxis to reinforce the use of the AAI at regular intervals [
16]. Our study also shows, for the first time, the incidence of switching brands of AAI among caregivers of children with food allergies, and therefore supports the relevance of the EACCI guideline to retrain on the new device when devices are switched [
16]. Therefore, caregivers should be trained on all available brands of AAI in order to improve self-efficacy and HRQL.
4.2. Implications on Future Research
This study highlights the need for the design and validation of educational interventions for caregivers, patients, and healthcare professionals in the use of different brands of adrenaline auto injectors. As device switches have been shown to be a common occurrence, randomized control trials should be conducted to elucidate differences in the successful use of different brands of AAI available in Ireland, as well as the effects of switching brands on administration with or without adequate training. The knowledge and perspectives of pharmacists on training patients and caregivers in different brands of AAI should be explored in more detail. As well as this, knowledge of healthcare professionals in the knowledge of the use of different AAI brands should be assessed in order to determine the readiness of those working in emergency medicine, general practice, allergy, and paediatrics to train caregivers successfully in all AAI brands. Finally, further study should be conducted to assess caregiver-administered adrenaline in a hospital environment on knowledge of anaphylaxis and AAI administration.
4.3. Strengths and Limitations
The strengths of this study include the use of both multiple choice and open-ended questions to gain an in-depth perspective of caregiver’s perceptions of different brands of AAI. The socio-economic demographics and allergy related history were collected through the online questionnaire, which provided an understanding of how these factors may affect the switching between brands of AAI or preference of AAI brand.
There are limitations to this study, which must be considered. Firstly, the relatively low response rate of parents to the online questionnaire may potentially influence the results of this study due to participant bias. Secondly, most respondents to the questionnaire were mothers. Therefore, it was not possible to accurately compare the knowledge of the child’s history of allergy and the practice of switching AAI devices between mothers, fathers, and whether the knowledge of the management of the child’s food allergies is shared among parents.


 ,
, 


{kind=link}
{kind=link}