
A Brief Review of Local Bacteriotherapy for Preventing Respiratory Infections


1
Allergy Clinic, Casa di Cura Villa Montallegro, 16100 Genoa, Italy
2
Medical Department, DMG Italia, 00040 Pomezia, Italy
3
Allergy Center, IRCCS Giannina Gaslini, 16100 Genoa, Italy
*
Author to whom correspondence should be addressed.
Allergies 2022, 2(4), 138-145; https://doi.org/10.3390/allergies2040013
Submission received: 17 August 2022
/
Revised: 3 October 2022
/
Accepted: 18 October 2022
/
Published: 7 November 2022
(This article belongs to the Special Issue Probiotics in Allergy, Asthma and Respiratory Infections)
Abstract
:Recurrent respiratory infections (RRIs) account for relevant economic and social implications and significantly affect family life. Local Bacteriotherapy (LB) represents an innovative option in preventing RRIs. Local bacteriotherapy consists of administering “good” and safe bacteria (probiotics) by nasal or oral route. In particular, two strains (Streptococcus salivarius 24SMB and Streptococcus oralis 89a) are commonly used. The present article presents and discusses the literature concerning LB. Infections of airways include the upper and lower respiratory tract. A series of clinical trials investigated the preventive role of LB in preventing upper and lower RIs. These studies demonstrated that LB safely reduced the prevalence and severity of RIs, the use of antibiotics, and absences from school. Therefore, Local Bacteriotherapy may be considered an interesting therapeutic option in RRI prevention.
1. Introduction
Infections of the respiratory tract have a profound impact on society. Namely, respiratory infections (RIs) entail a relevant socioeconomic burden for society and for families [1,2,3]. In addition, RIs present a compelling challenge for pediatricians, otolaryngologists, general practitioners, and allergists [4]. Frequent RI configures a rather common clinical picture in childhood and is referred to as recurrent respiratory infection (RRI). Previously, inclusion criteria for RRI encompassed a history of more than six RIs yearly, excluding primary and secondary immunodeficiency, cystic fibrosis, primary ciliary dyskinesia, and airway malformations [5]. Successively, further RRI classifications were added, also considering localized infections [6,7,8,9,10,11].
Inadequate management of RRIs results in frequent doctor’s office visits, hospital admissions, overuse/abuse of antibiotics, and school and parental work absences.
Consequently, it is important to attempt to identify risk factors associated with RRI. In this regard, a relevant role is to be attributed to prematurity, preschool age (for relative immaturity of the immune system), early attendance at nursery school, indoor and outdoor pollution, home dampness, passive exposure to tobacco or vape fumes, low socio-economic level, overcrowding, and allergic diseases [12]. Indeed, allergic diseases may significantly predispose an individual to RI recurrence through different pathophysiologic mechanisms [13,14]. Type 2 immunity presumes a consequential defect of type 1 immune response that contributes to fighting infections [15]. As a result, allergic subjects are prone to contract infections more frequently and severely than healthy subjects [16]. As proof of this mechanism, allergen-specific immunotherapy, restoring a normal balance between type 1 and 2 immunity, consequently reduces predisposition to RI [17]. Namely, this study demonstrated that subjects undergoing allergen-specific immunotherapy had significantly less respiratory infections than control allergic subjects who did not undergo this treatment.
Another important concept should be noted: viral infections reduce the mechanisms of immune defense, thereby promoting infection recurrence [18]. Additionally, viral infections are frequently associated with bacterial super-infections, which in turn prompts doctors to prescribe antibiotics, further reducing immune defenses and promoting antibiotic resistance [19,20]. Furthermore, bacterial overgrowth induces the generation of biofilm, i.e., surface-attached, structured microbial communities containing sessile cells (bacteria and/or fungi) embedded in a self-produced extracellular matrix composed of polysaccharides, DNA, and other components, making them more resistant to bacteria and promoting their in situ permanence [21,22]. Notably, biofilm may be envisaged as an “influencer” of repeated infections that favors bacterial survival and contrasts host aggression [23].
Last but not least, infections per se cause dysbiosis both at intestinal and respiratory levels, thus contributing to the maintenance of the vicious circle that allows RRI [23]. Taking into consideration all these concepts, being able to prevent RRIs is crucial in reducing costs and complications, as well as improving socioeconomic aspects. In this regard, many attempts have been made to prevent RRI. Therefore, using “good” bacteria (probiotics) through local administration could be an attractive strategy [24].
2. The Meaning of Local Bacteriotherapy
Microbiota includes the microorganisms living inside the human body, mainly harboring on organs communicating with the outside environment [25,26]. A close relationship between the microbiota and human body (symbiosis) is well established [27,28]. Indeed, it is well known that probiotics interfere with pathogen growth [29]. Probiotics are live bacteria which, when given in adequate amounts, confer a benefit to the consumer, as stated by World Health Organization.
Consistent colonization by bacteria able to “interfere” with pathogen growth restores eubiosis and may prevent RI [30]. This phenomenon can occur as it has been evidenced that some strains of a-Streptococci produce substances characterized by microbicidal activity against pathogens, which have been called bacteriocin-like inhibitory substances (BLIS) [31]. As a result, the manipulation and use of probiotics in relation to the microbiota of upper airways could be an attractive strategy for preventing RI [32]. This practice was first proposed over 70 years ago, coining the term “Bacteriotherapy” [33].
Preliminary attempts were performed in the early 1950s [34,35,36]. As bacteria were usually administered directly into the airways, the term “Local Bacteriotherapy” became popular.
Recently, there has been a revival of interest in this medical practice, especially following the great success of the use of probiotics in medicine. Probiotics have been proposed to maintain or restore eubiosis in conditions characterized by dysbiosis.
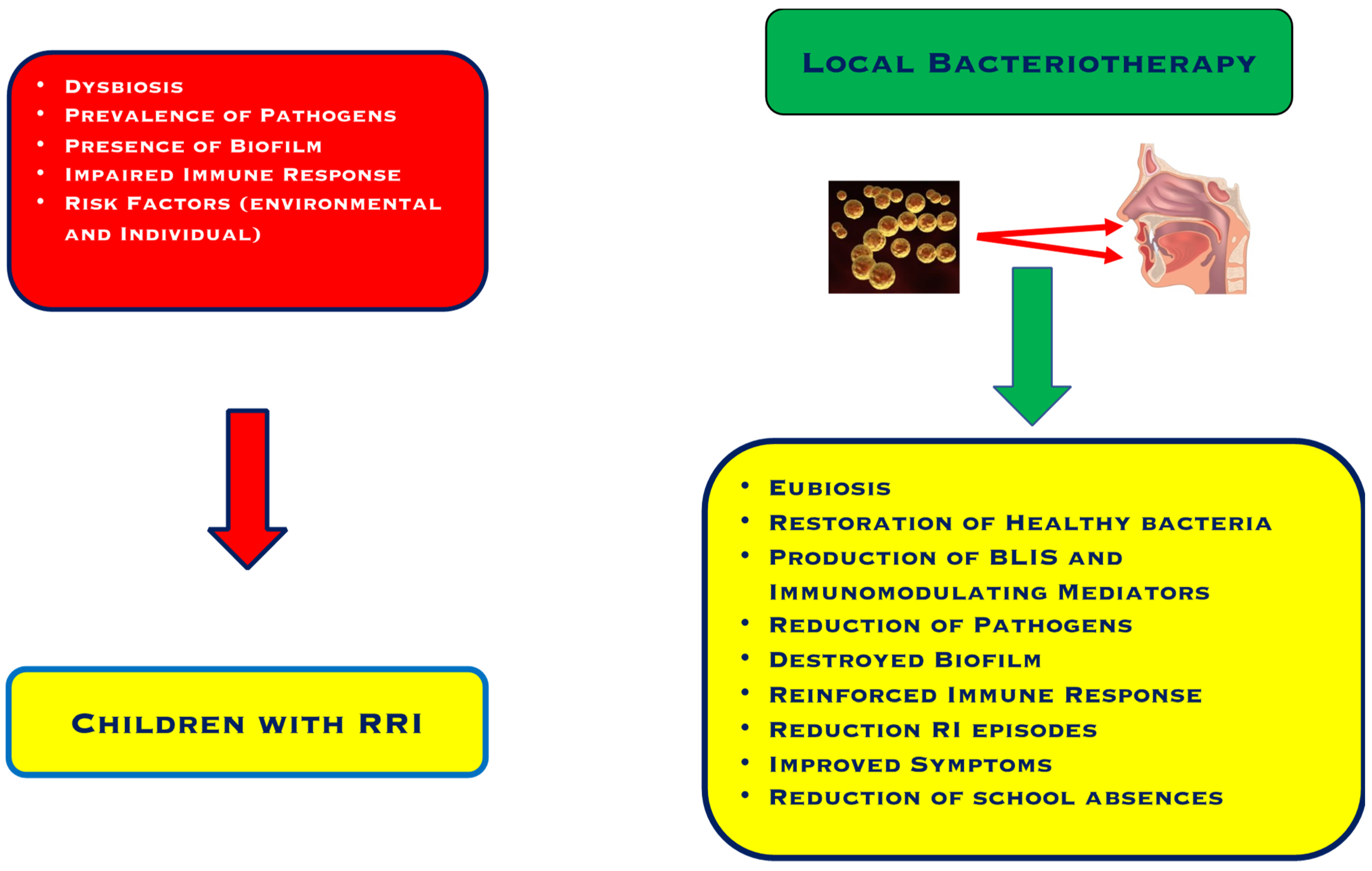
To explain the efficacy of this practice, different mechanisms have been explored. The main mechanism consists of interference and/or inhibition of pathogens as a result of the production of proteins with microbicidal activity and mediators with immunomodulating properties, as outlined in Figure 1 [31].
In particular, preliminary studies investigated the potential of one streptococcal strain, Streptococcus salivarius 24SMB. S salivarius is a non-pathogenic species able to colonize the oral cavity and can be considered a primary BLIS producer [37]. This strain exerted significant activity against S pneumoniae, was harmless to other S salivarius species, was non-pathogenic, and adhered to human larynx cells [38]. Successively, the topical administration of S salivarius by nasal spray allowed its colonization into the nasopharynx [39]. These preliminary experiences opened the way to new applications based on the local administration of probiotics, such as those in Local Bacteriotherapy. This approach allowed upper airways to be re-colonized with healthy microbes and led to pathogens being displaced by bacterial interference, in contrast with the present dysbiosis [39].
3. Local Bacteriotherapy: The Evidence
A series of clinical trials investigated the efficacy and safety of Local Bacteriotherapy, as summarized in Table 1.
The first trial was designed as a randomized, double-blind, placebo-controlled study and included 100 children suffering from recurrent otitis media between the ages of 1 and 5 [40]. The study showed that Streptococcus salivarius 24SMB nasal spray reduced the number of otitis episodes and the use of antibiotics.
A real-life study was performed to confirm the previous trial and 267 children with predisposition to recurrent otitis were enrolled [50]. Children were stratified into two groups: 159 were treated with a nasal spray containing a bacterial mixture, containing Streptococcus salivarius 24SMB and Streptococcus oralis 89a, and 108 served as control. A previous study isolated Streptococcus oralis 89a from a child suffering from recalcitrant tonsillitis and showed that this strain inhibited the growth of Group A Streptococci [41]. The real-life study demonstrated that LB significantly reduced the frequency and severity of otitis episodes.
A further in vitro study demonstrated that both strains inhibited biofilm formation and dissolved preformed biofilms [51].
A prospective trial, conducted on 42 children presenting sleep-disordered breathing and RRI, showed that LB with both strains improved sleep characteristics and nasal airflow and reduced oral breathing after 3 months [42].
A further clinical study that enrolled 80 children with RRI reported that LB halved respiratory infections and reduced school and parental work absences [43].
Another study explored the possibility of preventing adenoidectomy using LB [44]. Forty-four children were waitlisted for adenoidectomy and tympanocentesis due to being diagnosed with adenoid hypertrophy or otitis media with effusion. Children were subdivided into two groups: 22 treated with LB nasal spray and 22 with hypertonic saline. The study evidenced that LB significantly reduced the need for surgery and improved tympanometry.
A successive study included 202 children with RRI that were treated with LB [45]. Local Bacteriotherapy significantly diminished RI episodes compared to the previous year.
An observational trial enrolled 79 children (1–6 years of age) with recurrent otitis and treated them with LB nasal spray, and a further 70 children were used as the control group [46]. Local bacteriotherapy significantly diminished otitis episodes.
The last study included 91 children suffering from RRI [47]. Local Bacteriotherapy nasal spray reduced respiratory symptoms and otalgia. Older children were more responsive than younger.
Recently, a new administration route was proposed for LB. It consists of an oral formulation containing Streptococcus salivarius 24SMB and Streptococcus oralis 89a, as well as the nasal spray formulation. Therefore, two trials explored the efficacy and safety of oral LB.
The first randomized controlled trial concerned 82 children suffering from recurrent streptococcal pharyngotonsillitis caused by Group A Streptococci [48]. The results confirmed that oral LB also diminished the prevalence and duration of GABHS infections, antibiotic consumption, and school absences.
The second trial was conducted as a real-life study and included 51 children (mean age of 4.8 years) with RRI [49]. This experience also confirmed that oral LB reduced RI and school absences.
4. Practical Considerations
Preventing respiratory infections represents an urgent need, especially considering the antibiotic resistance problem, the absence of new antibiotics, and the concomitant pandemic. As a result, new preventive strategies are welcome [52]. In this context, the possibility of using LB against contrasting pathogens may represent an intriguing option. In addition, LB is a safe and effective approach in clinical practice. The application of “natural” substances, such as non-pathogenic bacteria, directly into the upper airways guarantees the possibility of manipulating the immune system at the site of infection [53].
However, three requirements must be fulfilled: colonization in airways, inhibition of pathogens, and microbiota maintenance [54].
On the other hand, it is well known that overuse of antibiotics creates dysbiosis that promotes pathogen growth. Local Bacteriotherapy is the “transplant” of probiotics that displaces pathogens, assuring long-lasting protection against infections. Importantly, the use of oral probiotics is now an established practice in the management of numerous diseases. However, LB offers an additional advantage as it acts directly in the airways, thus not relying on the digestive tract.
In addition, LB could also be an intriguing option in the COVID era. Indeed, LB could help reinforce immune defense, mainly in relation to innate immunity. As a result, the treated subjects could be less prone to contracting SARS CoV2 infection. This might represent a new scenario where LB could be challenged. Of course, methodologically robust trials have to conducted to confirm this suggestive hypothesis.
5. Conclusions
Infectious diseases have always been a constant problem for humans, especially in the pre-antibiotic era. One of the main causes of death was infection. Even today, infectious diseases claim millions of lives each year. Moreover, the current pandemic has further contributed to the need to be able to prevent and fight infections. Respiratory infections especially affect the most fragile segments of the population, namely children and the elderly. Thus, modulating microbiota could represent an outstanding opportunity in the war against infections.
Local Bacteriotherapy could be an advantageous strategy in preventing and treating infections. In this regard, the study of microbiota could represent a typical example of Precision Medicine where the ideal bacteriotherapy is defined, such as in the classical concept of Personalized Medicine. In other words, identifying the microbioma of the single subject is the prerequisite for tailoring more appropriate LB. In this regard, a relevant concept is the choice of specific strains, such as those characterized by an efficacy and safety profile in that subject.
In addition, the area of probiotic products is continuous expanding and the market is still growing. In this regard, LB could represent a safe and effective option.
However, a meta-analysis should be performed to provide convincing evidence about LB.
In conclusion, Local Bacteriotherapy could be considered an attractive option in managing patients with recurrent respiratory infections as published studies have provided positive outcomes. In addition, LB could also even be fruitful in preventing respiratory infections in subjects not prone to infection recurrence.
Author Contributions
Conceptualization, G.C. and M.A.T.; Methodology, V.C.; Data curation, V.D. and V.C.; Writing and editing, G.C.; Reviewing, M.A.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The data derived from published articles.
Conflicts of Interest
V.M. is an employee of DMG Italia. The other authors report no conflict of interest.
References
- Mansback, A.I.; Brihave, P.; Casimir, G.; Dhooge, I.; Gordts, F.; Halewyck, S.; Hanssens, L. Clinical aspects of chronic ENT inflammation in children. B-ENT 2012, 8 (Suppl. S19), 83–101. [Google Scholar]
- Orlandi, R.R.; Kingdom, T.T.; Smith, T.L.; Bleier, B.; DeConde, A.; Luong, A.U.; Poetker, D.M.; Hwang, P.H. International Consensus Statement on Allergy and Rhinology: Rhinosinusitis. Int. Forum Allergy Rhinol. 2016, 6 (Suppl. S1), S22–S209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fokkens, W.J.; Lund, V.J.; Mullol, J.; Bachert, C.; Alobid, I.; Baroody, F.; Cohen, N.; Cervin, A.; Douglas, R.; Gevaert, P.; et al. EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinology 2012, 50, 1–12. [Google Scholar] [CrossRef] [PubMed]
- De Martino, M.; Vierucci, A.; Appendino, C. Children with recurrent respiratory infections. Immunol. Ped. 1981, 4, 76–81. [Google Scholar]
- De Martino, M.; Ballotti, S. The child with recurrent respiratory infections: Normal or not? Ped. Allergy. Immunol. 2007, 18 (Suppl. S18), 13–18. [Google Scholar] [CrossRef]
- Paradise, J.L.; Bluestone, C.D.; Colborn, D.K.; Bernard, B.S.; Rockette, H.E.; Kurs-Lasky, M. Tonsillectomy and adenotonsillectomy for recurrent throat infection in moderately affected children. Pediatrics 2002, 110, 7–15. [Google Scholar] [CrossRef]
- Greenberg, D.; Bilenko, N.; Liss, Z. The burden of acute otitis media on the patient and family. Eur. J. Pediatr. 2003, 162, 576–581. [Google Scholar] [CrossRef]
- De Benedictis, F.M.; Bush, A. Recurrent lower respiratory tract infections in children. BMJ 2018, 362, k2698. [Google Scholar] [CrossRef]
- Karevold, G.; Kvestad, E.; Nafstad, P.; Kvaerner, K.J. Respiratory infections in schoolchildren: Co-morbidity and risk factors. Arch. Dis. Child 2006, 91, 391–395. [Google Scholar] [CrossRef] [Green Version]
- Thompson, M.; Vodicka, T.A.; Blair, P.S.; Buckley, D.I.; Heneghan, C.; Hay, B. ADTARGET Programme Team. Duration of symptoms of respiratory tract infections in children: Systematic review. BMJ 2013, 347, f7027. [Google Scholar] [CrossRef] [Green Version]
- Toivonen, L.; Karppinen, S.; Schuez-Havupalo, L.; Teros-Jaakkola, T.; Vuononvirta, J. Burden of Recurrent Respiratory Tract Infections in Children: A Prospective Cohort Study. Pediatr. Infect. Dis. J. 2016, 35, e362–e369. [Google Scholar] [CrossRef] [PubMed]
- Patria, M.F.; Esposito, S. Recurrent lower respiratory tract infections in children: A practical approach to diagnosis. Paediatr. Respir. Rev. 2013, 14, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Fahy, J.V. Type 2 inflammation in asthma—Present in most, absent in many. Nat. Rev. Immunol. 2015, 15, 57–65. [Google Scholar] [CrossRef] [Green Version]
- Ciprandi, G.; Tosca, M.A.; Silvestri, M.; Ricciardolo, F.L.M. Inflammatory biomarkers for asthma endotyping and personalized therapy. Exp. Rev. Clin. Immunol. 2017, 13, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Ciprandi, G.; Tosca, M.A.; Fasce, L. Allergic children have more numerous and severe respiratory infections than non-allergic children. Pediatr. Allergy Immunol. 2006, 17, 389–391. [Google Scholar] [CrossRef]
- Cirillo, I.; Marseglia, G.L.; Klersy, C.; Ciprandi, G. Allergic patients have more numerous and prolonged respiratory infections than non-allergic subjects. Allergy 2007, 62, 1087–1090. [Google Scholar] [CrossRef] [PubMed]
- Ciprandi, G.; Sormani, M.P.; Cirillo, I. Upper respiratory infections and SLIT: Preliminary evidence. Ann. Allergy 2009, 102, 262–263. [Google Scholar] [CrossRef]
- Griffin, M.R.; Walker, F.J.; Iwane, M.K. New vaccine surveillance network study group: Epidemiology of respiratory infections in young children: Insights from the new vaccine surveillance network. Pediatr. Infect. Dis. J. 2004, 23, 188–192. [Google Scholar] [CrossRef]
- Li, J.; Song, X.; Yang, T.; Chen, Y.; Gong, Y.; Yin, X.; Lu, Z. A Systematic Review of Antibiotic Prescription Associated with Upper Respiratory Tract Infections in China. Medicine 2016, 95, e3587. [Google Scholar] [CrossRef]
- Alexandrino, A.S.; Santos, R.; Melo, C.; Bastos, J.M.; Postiaux, G. Caregivers’ education vs. rhinopharyngeal clearance in children with upper respiratory infections: Impact on children’s health outcomes. Eur. J. Pediatr. 2017, 176, 1375–1383. [Google Scholar] [CrossRef]
- Regli, A.; Becke, K.; von Ungern-Sternberg, B.S. An update on the perioperative management of children with upper respiratory tract infections. Curr. Opin. Anaesthesiol. 2017, 30, 362–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nazzari, E.; Torretta, S.; Pignataro, L. Role of biofilm in children with recurrent upper respiratory tract infections. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Drago, L.; Pignataro, L.; Torretta, S. Microbiological aspects of acute and chronic pediatric rhinosinusitis. J. Clin. Med. 2019, 8, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchisio, P.; Nazzari, E.; Torretta, S.; Esposito, S.; Principi, N. Medical prevention of recurrent acute otitis media: An updated overview. Expert Rev. Anti-Infect. Ther. 2014, 12, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Yamanishi, S.; Pawankar, R. Current advances on the microbiome and role of probiotics in upper airways. Curr. Opin. Allergy Clin. Immunol. 2020, 20, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.; DuPont, H.L. New approaches for Bacteriotherapy: Prebiotics, new-generation probiotics, and synbiotics. Clin. Infect. Dis. 2015, 60 (Suppl. S2), S108–S121. [Google Scholar] [CrossRef]
- Faden, H.; Waz, M.J.; Bernstein, J.M.; Brodsky, L.; Stanievich, J.; Ogra, P.L. Nasopharyngeal flora in the first three years of life in normal and otitis-prone children. Ann. Otol. Rhinol. Laryngol. 1991, 100, 612–615. [Google Scholar] [CrossRef]
- Bernstein, J.M.; Faden, H.F.; Dryia, D.M.; Wactawski-Wende, J. Micro-ecology of the nasopharyngeal bacterial flora in otitis-prone and non-otitis prone children. Acta Otolaryngol. 1993, 113, 88–92. [Google Scholar] [CrossRef]
- Gao, Z.; Kang, Y.; Yu, J.; Ren, L. Human pharyngeal microbiome may play a protective role in respiratory tract infections. Genom. Proteom. Bioinform. 2014, 12, 144–150. [Google Scholar] [CrossRef] [Green Version]
- Roos, K.; Grahn Hakansson, E.; Holm, S. Effect of recolonization with “interfering” α streptococci on recurrences of acute and secretory otitis media in children: Randomised placebo-controlled trial. BMJ 2001, 322, 210–212. [Google Scholar] [CrossRef]
- Walls, T.; Power, D.; Tagg, J. Bacteriocin-like inhibitory substances (BLIS) production by the normal flora of the nasopharynx: Potential to protect against otitis media? J. Med. Microbiol. 2003, 52, 829–833. [Google Scholar] [CrossRef] [PubMed]
- Marsh, R.L.; Aho, C.; Beissbarth, J.; Bialasiewicz, S.; Binks, M.; Cervin, A. Recent advances in understanding the natural history of the otitis media microbiome and its response to environmental pressures. Int. J. Ped. Otorhinolaryngol. 2020, 130 (Suppl. S1), 109836. [Google Scholar] [CrossRef] [PubMed]
- Torrent, H. La bacteriothérapie lactique; ses applications actuelles. Vie Med. 1949, 30, 39. [Google Scholar] [PubMed]
- Lanza Castelli, R.A.; Elkeles, G. Bacteriology and Bacteriotherapy in otorhinolaryngology. Ann. Otolaryngol. 1950, 67, 152–160. [Google Scholar] [PubMed]
- Larget, M.; Lamare, J.P. Bacterio-therapy Is Still Useful. Sem. Hosp. 1953, 29, 1331–1333. [Google Scholar]
- Lopez LaCarrere, E.; Viale del Carril, A. Remote results of Bacteriotherapy in otorhinolaryngology. Rev. Fac. Cienc. Med. 1953, 11, 453–461. [Google Scholar]
- Wescombe, P.A.; Heng, N.C.; Burton, J.P.; Chilcott, C.N.; Tagg, J.R. Streptococcal bacteriocins and the case for Streptococcus salivarius as model oral probiotics. Future Microbiol. 2009, 4, 819–835. [Google Scholar] [CrossRef] [Green Version]
- Santagati, M.; Scillato, M.; Patanè, F.; Aiello, C.; Stefani, S. Bacteriocin-producing oral streptococci and inhibition of respiratory pathogens. FEMS Immunol. Med. Microbiol. 2012, 65, 23–31. [Google Scholar] [CrossRef] [Green Version]
- Santagati, M.; Scillato, M.; Muscaridola, N.; Metoldo, V.; La Mantia, I.; Stefani, S. Colonization, safety, and tolerability study of the Streptococcus salivarius 24SMBc nasal spray for its application in upper respiratory tract infections. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 2075–2080. [Google Scholar] [CrossRef]
- Marchisio, P.; Santagati, M.; Scillato, M.; Baggi, E.; Fattizzo, M.; Rosazza, C. Streptococcus salivarius 24SMB administered by nasal spray for the prevention of acute otitis media in otitis-prone children. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 2377–2383. [Google Scholar] [CrossRef]
- La Mantia, I.; Varricchio, A.; Ciprandi, G. Bacteriotherapy with Streptococcus salivarius 24SMB and Streptococcus oralis 89a nasal spray for preventing recurrent acute otitis media in children: A real-life clinical experience. Int. J. Gen. Med. 2017, 10, 171–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellussi, L.M.; Villa, M.P.; Degiorgi, G.; Passali, F.M.; Evangelisti, M.; Innocenti Paganelli, I. Preventive nasal bacteriotherapy for the treatment of upper respiratory tract infections and sleep-disordered breathing in children. Int. J. Ped. Otorhinolaryngol. 2018, 110, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Tarantino, V.; Savaia, V.; D’Agostino, R.; Silvestri, M.; Ciprandi, G. Bacteriotherapy for preventing recurrent upper respiratory infections in children: A real-world experience. Otolaryngol. Pol. 2018, 72, 33–38. [Google Scholar] [PubMed] [Green Version]
- La Mantia, I.; Varricchio, A.; Di Girolamo, S.; Minni, A.; Passali, G.C.; Ciprandi, G. The role of bacteriotherapy in the prevention of adenoidectomy. Eur. Rev. Med. Pharmacol. Sci. 2019, 23 (Suppl. S1), 44–47. [Google Scholar] [PubMed]
- Passali, D.; Passali, G.C.; Vesperini, E.; Cocca, S.; Visconti, I.C.; Ralli, M. The efficacy and tolerability of Streptococcus salivarius 24SMB and Streptococcus oralis 89° administered as nasal spray in the treatment of recurrent upper respiratory tract infections in children. Eur. Rev. Med. Pharmacol. Sci. 2019, 23 (Suppl. S1), 67–72. [Google Scholar]
- Cantarutti, A.; Rea, F.; Donà, D.; Cantarutti, L.; Passarella, A.; Scamarcia, A. Preventing recurrent acute otitis media with Streptococcus salivarius 24SMB and Streptococcus oralis 89a five months intermittent treatment: An observational prospective cohort study. Int. J. Ped. Otorhinolaryngol. 2020, 132, 109921. [Google Scholar] [CrossRef]
- Manti, S.; Parisi, G.F.; Papale, M.; Licari, A.; Salpietro, C.; Miraglia del Giudice, M.; Maresglia, G.L. Bacteriotherapy with Streptococcus salivarius 24SMB and Streptococcus oralis 89a nasal spray for treatment of upper respiratory tract infections in children: A pilot study on short-term efficacy. Ital. J. Pediatr. 2020, 46, 42. [Google Scholar] [CrossRef] [Green Version]
- Andaloro, C.; Santagati, M.; Stefani, S.; La Mantia, I. Bacteriotherapy with Streptococcus salivarius 24SMB and Streptococcus oralis 89a oral spray for children with recurrent streptococcal pharyngotonsillitis: A randomized placebo-controlled clinical study. Eur. Arch. Otorhinolaryngol. 2019, 276, 879–887. [Google Scholar] [CrossRef]
- Tarantino, V.; Savaia, V.; D’Agostino, R.; Damiani, V.; Ciprandi, G. Oral bacteriotherapy in children with recurrent respiratory infections: A real-life study. Acta Biomed. 2020, 91 (Suppl. S1), 73–76. [Google Scholar]
- Grahn, E.; Holm, S.E. Bacterial interference in the throat flora during a streptococcal tonsillitis outbreak in an apartment house area. Zentralbl. Bakteriol. Mikrobiologie Hyg. 1983, 256, 72–79. [Google Scholar] [CrossRef]
- Bidossi, A.; De Grandi, R.; Toscano, M.; Bottagisio, M.; De Vecchi, E.; Gelardi, M. Probiotics Streptococcus salivarius 24SMB and Streptococcus oralis 89a interfere with biofilm formation of pathogens of the upper respiratory tract. BMC Infect. Dis. 2018, 18, 653. [Google Scholar] [CrossRef] [PubMed]
- Bellussi, L.M.; Passali, F.M.; Ralli, M.; De Vincentiis, M.; Greco, A.; Passali, D. An overview on upper respiratory tract infections and Bacteriotherapy as innovative therapeutic strategy. Eur. Rev. Med. Pharmacol. Sci. 2019, 23 (Suppl. S1), 27–38. [Google Scholar] [PubMed]
- Varricchio, A.; La Mantia, I.; Brunese, F.P.; Ciprandi, G. Inflammation, infection, and allergy of upper airways: New insights from national and real-world studies. Ital. J. Pediatr. 2020, 46, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campanella, V.; Syed, J.; Santacroce, L.; Sain, R.; Ballini, A.; InchIngolo, F. Oral probiotics influence oral and respiratory tract infections in pediatric population: A randomized double-blinded placebo-controlled pilot study. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 8034–8041. [Google Scholar] [PubMed]
Figure 1.
Characteristics of children with recurrent respiratory infections and the effects of Local Bacteriotherapy.
Figure 1.
Characteristics of children with recurrent respiratory infections and the effects of Local Bacteriotherapy.


{kind=link}
Table 1.
Studies that investigated Local Bacteriotherapy when administered as a nasal spray or oral spray (RAOM = recurrent acute otitis media; RRI = recurrent respiratory infection; SDB = sleep-disordered breathing; AH = adenoid hypertrophy; OME = otitis media with effusion; m = median; RPT = recurrent pharyngotonsillitis).
Table 1.
Studies that investigated Local Bacteriotherapy when administered as a nasal spray or oral spray (RAOM = recurrent acute otitis media; RRI = recurrent respiratory infection; SDB = sleep-disordered breathing; AH = adenoid hypertrophy; OME = otitis media with effusion; m = median; RPT = recurrent pharyngotonsillitis).
| Authors (Ref) | Disease | Patients | Age (Years) | Schedule | Duration | Control | Outcomes for Treatment | Rate of Improvement | Side Effects |
|---|---|---|---|---|---|---|---|---|---|
| Nasal Bacteriotherapy | |||||||||
| Marchisio et al. [40] | RAOM | 50 treated 50 controls | 1–5 | Twice/daily for 5 days/month | 3 courses | Placebo | AOM episodes Antibiotic use |
| None |
| La Mantia et al. [41] | RAOM | 159 treated 108 controls | 3–10 | Twice/daily for 7 days/month | 3 courses | Treatment as needed | AOM episodes Severity |
| None |
| Bellussi et al. [42] | RRI SDB | 42 | <18 | Twice/daily for 7 days/month | 3 courses | No | Sleep symptoms |
| None |
| Tarantino et al. [43] | RRI | 80 | 3–14 | Twice/daily for 7 days/month | 3 courses | No | RI episodes school absence working absence |
| None |
| La Mantia et al. [44] | AH OME | 44 | 3–6 | Twice/daily for 7 days/month | 3 courses | Hypertonic saline | Surgery need Adenoid size IV Tympanometry B |
| None |
| Passali et al. [45] | RRI | 202 | 7.5 | Twice/daily for 7 days/month | 3 courses | No | RI episodes |
| None |
| Cantarutti et al. [46] | RAOM | 79 treated 70 controls | 1–6 | Twice/daily for 7 days/month | 5 courses | Treatment as needed | AOM ≥3 Antibiotic use |
| 1 patient reported mild cough with LB |
| Manti et al. [47] | RRI | 91 | 1–12 | Twice/daily for 7 days/month | 3 courses | Open study | Fever Cough Rhinorrhea Otalgia |
| 9 patients experienced nasal burning after LB |
| Oral Bacteriotherapy | |||||||||
| Andaloro et al. [48] | RPT | 41 treated 41 placebo | 6–11 | Once/daily for 30 days/month | 3 courses | Placebo | Infections episodes Duration (days) Antibiotic use School absences |
| None |
| Tarantino et al. [49] | RRI | 51 | 3–10 | Once/daily for 30 days/month | 3 courses | Open | RI episodes School absences |
| None |
* in children with colonization.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ciprandi, G.; Damiani, V.; Cordara, V.; Tosca, M.A. A Brief Review of Local Bacteriotherapy for Preventing Respiratory Infections. Allergies 2022, 2, 138-145. https://doi.org/10.3390/allergies2040013
AMA Style
Ciprandi G, Damiani V, Cordara V, Tosca MA. A Brief Review of Local Bacteriotherapy for Preventing Respiratory Infections. Allergies. 2022; 2(4):138-145. https://doi.org/10.3390/allergies2040013
Chicago/Turabian StyleCiprandi, Giorgio, Valerio Damiani, Vittorio Cordara, and Maria Angela Tosca. 2022. "A Brief Review of Local Bacteriotherapy for Preventing Respiratory Infections" Allergies 2, no. 4: 138-145. https://doi.org/10.3390/allergies2040013