
Construction Health and Safety Agent Collaboration and Its Influence on Health and Safety Performance in the South African Construction Industry


Abstract
:1. Introduction
2. Literature Review
2.1. Construction Industry and Health and Safety Management
2.2. Factors of Collaboration
2.3. Collaboration and Performance
3. Methodology
3.1. Results and Discussion
3.1.1. Delphi Study Demographic Characteristics of Experts
Delphi Study Process
3.1.2. Questionnaire Survey Results and Discussion
Respondents’ Profile
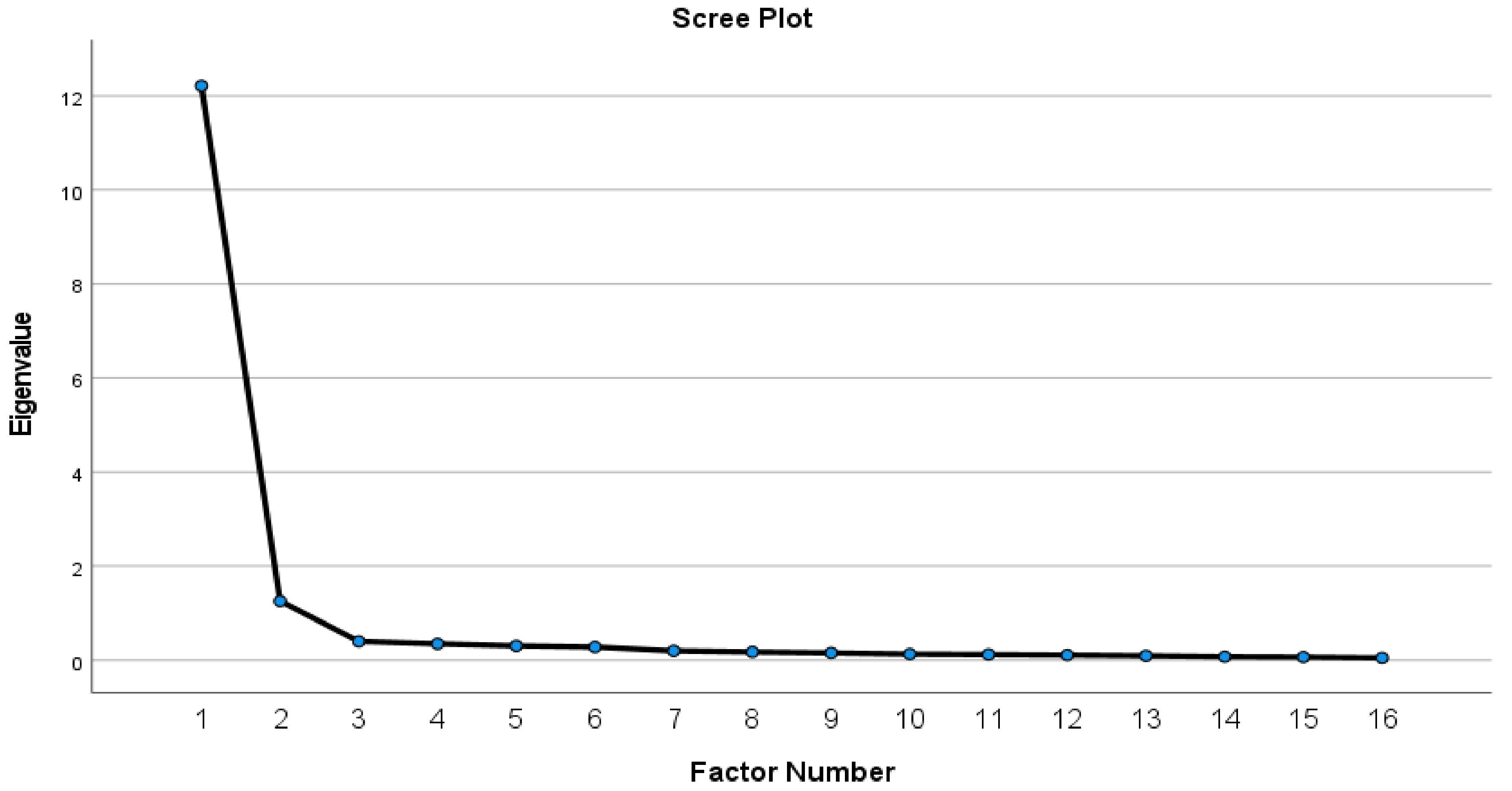
3.1.3. Factor Analysis
The Results of Two Dependent Factors, Namely CHSA Collaboration and H&S Performance
3.1.4. Assessment of Measurement Model for Each Construct
3.2. Path Analysis Results
3.3. Path Analysis Model
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Neale, R. Ten factors to improve occupational safety and health in construction projects. Afr. Newsl. Occup. Health Saf. 2013, 23, 52–54. [Google Scholar]
- Goldswain, C.C. Architectural Design Interventions toward Improvement of Construction Health, Safety and Ergonomics in South Africa. Ph.D. Thesis, Nelson Mandela Metropolitan University, Gqeberha, South Africa, 2014. [Google Scholar]
- Deacon, C. The Effect of the Integration of Design, Procurement, and Construction Relative to Health and Safety. Unpublished. Ph.D. Thesis, Nelson Mandela University, Port Elizabeth, South Africa, 2016. [Google Scholar]
- Health and Safety Executive. Managing Health and Safety in Construction: Construction: (Design and Management) Regulations 2015. Guidance on Regulations; HSE Books: London, UK, 2015. [Google Scholar]
- Benjaoran, V.; Bhokha, S. An integrated safety management with construction management using 4D CAD model. J. Saf. Sci. 2010, 48, 395–403. [Google Scholar] [CrossRef]
- Larsson, T.J.; Almen, L. Health and safety coordinators in building projects. Built Environ. Proj. Asset Manag. 2014, 4, 251–263. [Google Scholar]
- Erickson, A.J. Interdisciplinary: Increasing safety performance. Prof. Safety. Peer-Rev. 2016, 61, 26–32. [Google Scholar]
- Qi, J. Integration of Construction Worker Fall Safety in Design through the Use of Building Information Modelling. Unpublished. Ph.D. Thesis, University of Florida, Gainsville, FL, USA, 2011. [Google Scholar]
- Atkinson, A.; Westall, R. The relationship between integrated design and construction and safety on construction projects. Constr. Manag. Econ. 2010, 28, 1007–1017. [Google Scholar] [CrossRef]
- Emuze, F.; Smallwood, J.J. Collaborative working in South African construction: Contractors’ perspectives. J. Eng. Des. Technol. 2014, 12, 294–306. [Google Scholar] [CrossRef]
- SACPCMP (South African Council for Project and Construction Management Professions). Registration Rules for Construction Health and Safety Agents in Terms of Section 18 (1) c of the Project and Construction Management Professions Act, Act No. 48 of 2000; SACPCMP: Midrand, South Africa, 2013. [Google Scholar]
- Manu, P.; Emuze, F.; Saurin, T.A.; Hadikusumo, B. Construction Health and Safety in Developing Countries, 1st ed.; Routledge Taylor & Francis Group: New York, NY, USA, 2020; ISBN 978-1-138-31707-9. [Google Scholar]
- Department of Public Works. Construction Regulations Launch: Address by the Minister of Public Works; Department of Public Works: Boksburg, South Africa, 2014.
- Rantsatsi, N.; Musonda, I.; Agumba, J. Factors that determine construction health and safety agent collaboration on construction projects: A Delphi study. Acta Structilia 2021, 28, 53–77. [Google Scholar] [CrossRef]
- Khoza, D.J. Development of a Client-Driven Health and Safety Model for Measuring Health and Safety Performance of Construction Projects in South Africa. Ph.D. Thesis, Unversity of KwaZulu-Natal, Durban, South Africa, 2020. [Google Scholar]
- Smallwood, J.J.; Deacon, C. The performance of construction health and safety agents. In Proceedings of the Ninth International Structural Engineering and Construction Conference (ISEC9), Valencia, Spain, 24–28 July 2017. [Google Scholar]
- Badri, A.; Gbodossou, A.; Nadeau, S. Occupational health and safety risks: Towards the integration into project management. J. Saf. Sci. 2012, 50, 190–198. [Google Scholar] [CrossRef]
- Chunxiang, W. Safety Responsibilities for Owner and Example in Public Works. In Procedia Engineering International Symposium on Safety Science and Engineering in China, 2012 (ISSSE-2012); Elsevier: Amsterdam, The Netherlands, 2012; Volume 43, pp. 523–527. [Google Scholar]
- Rantsatsi, N.; Musonda, I.; Agumba, J. Identifying factors of collaboration critical for improving health and safety performance in construction projects: A systematic literature review. Acta Structilia 2020, 27, 120–150. [Google Scholar]
- Sinelnikov, S.; Inouye, J.; Kerper, S. Using leading indicators to measure occupational health and safety performance. Saf. Sci. J. 2015, 72, 240–248. [Google Scholar] [CrossRef]
- Rajendran, S. Sustainable construction safety and health rating system. Civil construction and environmental engineering. Ph.D. Thesis, Oregon State University, Corvallis, OR, USA, 2006. [Google Scholar]
- Aulin, R.; Capone, P. The role of health and safety coordinator in Sweden and Italy construction industry. In Proceedings of the W099—Special Track 18th CIB World Building Congress, Salford, UK, 10–13 May 2010; pp. 93–106, CIB Publication 357. [Google Scholar]
- Lingard, H.; Cooke, T.; Blismas, N.N. Who is ‘The Designer’ in Construction Occupational Health and Safety?, Proceedings of the 27th Annual ARCOM Conference, Bristol, UK, 5–7 September 2011; Egbu, C., Lou, E.C.W., Eds.; Association of Researchers in Construction Management: Reading, UK, 2011; pp. 299–308. [Google Scholar]
- Skeepers, N. Safety Leadership and Management in the Construction Industry in Gauteng Province, South Africa. Ph.D. Thesis, University of Johannesburg, Johannesburg, South Africa, 2016. [Google Scholar]
- Kukoyi, P.O. A Framework for Improving Construction Workers’ Health and Safety Practices in Lagos, Nigeria. Ph.D. Thesis, Nelson Mandela University, Gqeberha, South Africa, 2018. [Google Scholar]
- Samuel, L. Labour on Injuries and Fatalities in SA Construction Sector. 2017. Available online: https://www.gov.za/speeches/sa-construction-sector-9-mar-2017-0000 (accessed on 31 October 2018).
- Smith, A.P.; Wadsworth, E.J. Safety Culture, Advice and Performance: The Associations Between Safety Culture and Safety Performance, Health and Wellbeing at an Individual Level, and Safety Culture, Competent Occupational Safety and Health Advice, and Safety Performance at a Corporate Level; Cardiff University: Cardiff, UK, 2009. [Google Scholar]
- Rebbitt, D. The Value Proposition of Safety Professional: Do Safety Professionals Actually Reduce Fatalities? Master’s Thesis, Athabasca University, Athabasca, AB, Canada, 2012. [Google Scholar]
- Cameron, I.; Hare, B.; Duff, R. An analysis of safety advisors roles and site safety performance. Eng. Constr. Archit. Manag. 2013, 20, 505–521. [Google Scholar] [CrossRef]
- Borys, D. The Value Proposition for the Occupational Health and Safety Professional: Literature Review; International Network of Safety & Health Practitioner Organisations (INSHPO): Park Ridge, IL, USA, 2014. [Google Scholar]
- Provan, D.J.; Dekker, S.W.A.; Rae, A.J. Bureaucracy, influence and beliefs: A literature review of the factors shaping the role of a safety professional. J. Saf. Sci. 2017, 98, 98–112. [Google Scholar] [CrossRef]
- Bemelmans, J.; Voordijk, H.; Vos, B. Supplier-contractor collaboration in the construction industry: A taxonomic approach to the literature of 2000–2009. Eng. Constr. Archit. Manag. 2012, 19, 342–368. [Google Scholar] [CrossRef]
- Deep, S.; Gajendran, T.; Jefferies, M. A systematic review of ‘enablers of collaboration’ among the participants in construction projects. Int. J. Constr. Manag. 2019, 21, 919–931. [Google Scholar] [CrossRef]
- Faris, H.; Gaterell, M.; Hutchinson, D. Investigating underlying factors of collaboration for construction projects in emerging economies using exploratory factor analysis. Int. J. Constr. Manag. 2019, 22, 514–526. [Google Scholar] [CrossRef]
- Thomson, A.M.; Perry, J.; Miller, T. Conceptualizing and measuring collaboration. J. Public Adm. Res. Theory 2009, 19, 23–56. [Google Scholar] [CrossRef]
- Amabile, T.M.; Patterson, C.; Mueller, J.; Wojcik, T.; Kramer, S.J.; Odomirok, P.W.; Marsh, M. Academic-practitioner collaboration in management research: A case of cross-profession collaboration. Acad. Manag. J. 2001, 44, 418–431. [Google Scholar] [CrossRef]
- Lu, W.; Zhang, D.; Rowlinson, S. BIM Collaboration: A Conceptual Model and Its Characteristics, Proceedings of the 29th Annual Association of Researchers in Construction Management (ARCOM) Conference, Reading, UK, 2–4 September 2013; Smith, S.D., Ahiaga-Dagbui, D.D., Eds.; Association of Researchers in Construction Management: Reading, UK, 2013; pp. 25–34. [Google Scholar]
- Bronstein, R.L. A Model for Interdisciplinary Collaboration Author(s): Laura, R. Bronstein Source. Soc. Work. 2003, 48, 297–306. [Google Scholar] [CrossRef]
- Patel, H.; Pettitt, M.; Wilson, J. Factors of collaborative working: A framework for a collaboration model. J. Appl. Ergon. 2012, 43, 1–26. [Google Scholar] [CrossRef]
- Torneman, C. Collaboration in Construction Project Delivery: Strategic Implications Technical Consultancy Firms. Unpublished. Master’s Thesis, Chalmers University of Technology, Gothenburg, Sweden, 2015. [Google Scholar]
- Roberts, D.; Van Wyk, R.; Dhanpat, N. Exploring Practices for Effective Collaboration. In Proceedings of the 28th Annual Conference of the Southern African Institute of Management Scientists, Johannesburg, South Africa, 26–28 September 2016; pp. 1–13, ISBN 978-0-620-71797-7. [Google Scholar]
- Ylitalo, J.; Eerikki, M.; Ziegler, K. Evolvement of trust and mutuality in early stages of interorganisational collaboration. Front. E-Bus. Res. 2004, 9, 546–560. [Google Scholar]
- Liu, Y.; Van Nederveen, S.; Hertogh, M. Understanding effects of BIM on collaborative design and construction. An empirical study in China. Int. J. Proj. Manag. 2017, 35, 686–698. [Google Scholar] [CrossRef]
- Khalfan, M.M.A.; McDermott, P.; Swan, W. Building trust in construction projects. J. Supply Chain. Manag. 2007, 12, 385–391. [Google Scholar] [CrossRef]
- D’Amour, D.; Ferrada-Videla, M.; Rodriquez, L.; Beaulieu, M. The conceptual basis for interprofessional collaboration: Core concepts and theoretical frameworks. J. Interprofessional Care 2005, 19, 118–206. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, P.; Eskerod, P.; Dalcher, D.; Sandhawalia, B. The dynamics of collaboration in multi-partner projects. Proj. Manag. J. 2010, 41, 59–78. [Google Scholar] [CrossRef]
- Hasanzadeha, M.S.; Hosseinalipourb, M.; Hafezi, M. Collaborative procurement in construction Coordinating collaboration in contractually different complex construction projects. Procedia Soc. Behav. Sci. 2014, 20, 811–818. [Google Scholar]
- Hughes, D. Development of an Effective Model for Collaboration within the UK Construction Industry. Unpublished. Ph.D. Thesis, University of South Wales, Cardiff, UK, 2018. [Google Scholar]
- Akintan, O.; Morledge, R. Improving the collaboration between main contractors and subcontractors within traditional construction procurement. J. Constr. Eng. 2013, 2013, 281236. [Google Scholar] [CrossRef]
- Masemeni, N.M.; Aigbavboa, C.O.; Thwala, D.W. Evaluating Barriers of Collaboration in South Africa Construction Supply Chain; SACQSP2015-20; University of Johannesburg: Johannesburg, South Africa, 2015. [Google Scholar]
- Fulford, R.; Standing, C. Construction industry productivity and the potential for collaborative practice. Int. J. Proj. Manag. 2014, 32, 315–326. [Google Scholar] [CrossRef]
- Greenwood, D.; Wu, S. Establishing the association between collaborative working and construction project performance based on client and contractor perceptions. Constr. Manag. Econ. 2012, 30, 299–308. [Google Scholar] [CrossRef]
- Pal, R.; Wang, P.; Liang, X. The critical factors in managing relationships in international engineering, procurement and construction (IEPC) projects of Chinese organisations. Int. J. Proj. Manag. 2017, 35, 1225–1237. [Google Scholar] [CrossRef]
- Saifullah, N.M.; Ismail, F. Integration of occupational safety and health during preconstruction stage in Malaysia. Procedia Soc. Behav. Sci. 2012, 35, 603–610. [Google Scholar] [CrossRef]
- Mroszczyk, J.W. Improving construction safety: A Team Effort. Prof. Saf. 2015, 60, 55–68. Available online: www.asse.org (accessed on 27 August 2019).
- El-Sheikh, A.A.; Abonazel, M.R.; Gamil, N. A review of software packages for structural equation modeling: A comparative study. Appl. Math. Phys. 2017, 5, 85–94. [Google Scholar]
- Ozturk, G.; Arditi, D.; Yitmen, I.; Yalcinkaya, M. The factors affecting collaborative building design. World multidisciplinary civil engineering-architecture-urban planning symposium 2016 (WMCAUS 2016). Procedia Eng. 2016, 161, 797–803. [Google Scholar] [CrossRef]
- Welman, C.; Kruger, F.; Mitchell, B. Research Methodology, 3rd ed.; Oxford University Press: Cape Town, South Africa, 2005. [Google Scholar]
- Changi, H.K.; Karen, Y. Beyond consensus: A review of Delphi research published in Malaysian social science journals. Int. J. Bus. Soc. 2018, 19, 312–323. [Google Scholar]
- Von der Gracht, H. Consensus measurement in Delphi studies Re-opinion and implications for future quality assurance. Technol. Forecast. Soc. Change 2012, 79, 1525–1536. [Google Scholar] [CrossRef]
- Habibi, A.; Sarafrazi, A.; Izadyar, S. Delphi technique theoretical framework in qualitative research. Int. J. Eng. Sci. 2014, 3, 8–13. [Google Scholar]
- Costello, A.; Osborne, J. Best practices in exploratory factor analysis: Four recommendations for getting the most from your analysis. Pract. Assess. Res. Eval. 2005, 10, 7. [Google Scholar]
- Pallant, J. Survival Manual. A Step by Step Guide to Data Analysis Using SPSS for Windows, 3rd ed.; McGraw-Hill Companies, Inc.: New York, NY, USA, 2007; ISBN lO:0-335-22366-4. [Google Scholar]
- Farrington, M.F. Sibling Partnerships in South African Small and Medium-Size Family Businesses. Ph.D. Thesis, Nelson Mandela Metropolitan University, Gqeberha, South Africa, 2009. [Google Scholar]
- Brown, A.T. Confirmatory Factor Analysis for Applied Research; The Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Afthanorhan, W.A. A comparison of partial least square structural equation modeling and covariance based structural equation modeling for confirmatory factor analysis. Int. J. Eng. Sci. Innov. Eng. 2013, 2, 198–205. [Google Scholar]
- Kline, R.B. Principles and Practices of Structural Equation Modeling, 2nd ed.; The Guilford Press: New York, NY, USA, 2005. [Google Scholar]
- Lingard, H.; Pirzadeh, P.; Blismas, N.; Wakefied, R.; Kleiner, B. Exploring the link between early constructor involvement in project decision-making and the efficacy of health and safety risk control. Constr. Manag. Econ. 2014, 32, 918–931. [Google Scholar] [CrossRef]
- Hoque, M.; Awang, Z.; Siddiqui, A. Technopreneurial intention among university students of business courses in Malaysia: A structural equation modelling. Int. J. Entrep. Small Medium Enterp. 2017, 4, 1–16. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria Versus New Alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Schreiber, J.B.; Nora, A.; Stage, F.K.; Barlow, E.A.; King, J. Reporting structural equation modeling and and confirmatory factor analysis results: A Review. J. Educ. Res. 2006, 99, 323–337. [Google Scholar] [CrossRef]
- Awang, Z. Validating the Measurement Model: CFA. SEM Made Simple; MPWS Publisher: Bangi, Selangor, Malaysia, 2015; pp. 54–74. [Google Scholar]
- Bentler, P.M. EQS 6 Structural Equations Program Manual; Multivariate Software, Inc.: Encino, CA, USA, 2006; ISBN 1-885898-03-7. [Google Scholar]
- Stage, K.F.; Carter, C.H.; Nora, A. Path Analysis: An Introduction and Analysis of a Decade of Research. J. Educ. Res. 2004, 98, 5–13. [Google Scholar] [CrossRef]
- Raykov, T.; Marcoulides, G. A First Course in Structural Equation Modeling; Lawrence Erlbaum Associates: London, UK, 1991. [Google Scholar]
- Byrne, M.B. Structural Equation Modeling with AMOS: Basic Concepts, Applications and Programming, 2nd ed.; Routledge Taylor and Francis Group: London, UK, 2006. [Google Scholar]
- Born-Barnard, T.; Fletcher, L.; Steyn, H. Link trust and collaboration in project teams to project management success. Int. J. Manag. Proj. Bus. 2018, 11, 432–457. [Google Scholar] [CrossRef]
- Iyer, R.V. Engaging a Multi-Disciplinary Literature Review in the Development of a Framework to Assess Construction Collaboration. Master’s Thesis, Texas A&M University, College Station, TX, USA, 2015. [Google Scholar]
- Tau, S.; Seoke, S.Y. An assessment of the implemented occupational health and safety practices in Botswana construction industry. Afr. Newsl. Occup. Health Saf. 2013, 23, 55–58. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic | Characteristic | Frequency | Percentage |
|---|---|---|---|
| Country | South Africa | 9 | 64.28% |
| United Kingdom | 1 | 7.14% | |
| Nigeria | 2 | 14.28% | |
| Malaysia | 1 | 7.14% | |
| United States of America | 1 | 7.14% | |
| Total | 14 | 100.00% | |
| Qualification | PhD | 6 | 42.85% |
| Master of Science Degree | 2 | 14.28% | |
| Bachelor’s Degree | 4 | 28.57% | |
| National Diploma | 2 | 14.28% | |
| Total | 14 | 100.00% | |
| Professional registration | Construction project managers | 2 | 14.28% |
| CHSAs | 7 | 50% | |
| Construction managers | 2 | 14.28% | |
| Engineer | 1 | 7.14% | |
| Construction health and safety manager | 1 | 7.14% | |
| Certified safety professional | 1 | 7.14% | |
| Total | 14 | 100.00% | |
| Years of experience | 1–5 | 3 | 21.42% |
| 6–10 | 3 | 21.42% | |
| 11–15 | 1 | 7.14% | |
| 16–20 | 1 | 7.14% | |
| 21–25 | 2 | 14.28 | |
| 26–30 | 2 | 14.28 | |
| 31–40 | 2 | 14.28 | |
| Total | 14 | 100.00% |
| Expert Publication | Number of Publications |
|---|---|
| Peer-reviewed journals | 353 |
| Peer-reviewed conference papers | 201 |
| Editor or author of book | 10 |
| Author of a book chapter | 8 |
| Position | Frequency | Percentage |
|---|---|---|
| Construction project manager | 50 | 23.5 |
| CHSA | 61 | 28.6 |
| Construction manager | 37 | 17.4 |
| Construction H&S manager | 61 | 28.6 |
| Other | 4 | 1.9 |
| Total | 213 | 100 |
| Professions | ||
| Construction project management | 51 | 23.9 |
| Construction H&S management | 121 | 56.8 |
| Construction management | 40 | 18.8 |
| Other | 1 | 0.5 |
| Total | 213 | 100 |
| Professional registration | ||
| Construction project manager | 55 | 25.8 |
| CHSA | 116 | 54.5 |
| Construction manager | 39 | 18.3 |
| Other | 3 | 1.4 |
| 213 | 100 | |
| Highest qualification | ||
| Doctorate Degree | 2 | 0.9 |
| Master’s Degree | 22 | 10.3 |
| Honors Degree | 19 | 8.9 |
| B-Tech Degree/BSc | 56 | 26.3 |
| National Diploma | 90 | 42.3 |
| Certificate | 13 | 6.1 |
| Matric | 10 | 4.7 |
| Less than matric | 1 | 0.5 |
| Total | 213 | 100 |
| Years of experience | ||
| 0–2 | 0 | 0.0 |
| 2–5 | 8 | 3.8 |
| 6–10 | 52 | 24.4 |
| 11–15 | 68 | 31.9 |
| 16–20 | 31 | 14.6 |
| 20 years and over | 54 | 25.3 |
| Organization type | ||
| Client | 61 | 28.6 |
| Construction health and safety consulting | 53 | 24.9 |
| Designer | 20 | 9.4 |
| Contractor | 79 | 37.1 |
| Total | 213 | 100 |
| Method | ||
| Design-bid-build | 37 | 17.4 |
| Design and build | 80 | 37.6 |
| Integrated project delivery | 83 | 39.0 |
| Other | 13 | 6.1 |
| Total | 213 | 100 |
| Province | ||
| Eastern Cape | 19 | 8.9 |
| Free State | 17 | 8.0 |
| Gauteng | 75 | 35.2 |
| KwaZulu Natal | 19 | 8.9 |
| Limpopo | 21 | 9.9 |
| Mpumalanga | 27 | 12.7 |
| North West | 8 | 3.8 |
| Northern Cape | 10 | 4.7 |
| Western Cape | 17 | 8.0 |
| Total | 213 | 100 |
| Department responsible for health and safety | ||
| Engineering department | 13 | 6.1 |
| H&S department | 171 | 80.3 |
| Construction department | 25 | 11.7 |
| Other | 4 | 1.9 |
| Total | 213 | 100 |
| Kaiser–Meyer–Olkin Measure of Sampling Adequacy. | 0.954 | |
|---|---|---|
| Bartlett’s Test of Sphericity | Approx. Chi-Square | 13,285.276 |
| df | 990 | |
| Sig. | 0.000 | |
| Factor | |
|---|---|
| 1 | |
| M5 Project knowledge that benefit other members was shared with the CHSA | 0.785 |
| M4 Responsibilities for project activities were shared with the CHSA | 0.754 |
| M2 The CHSA was involved in decision making with other project team members | 0.711 |
| EE3 Leadership was shared between the CHSA and project team members | 0.690 |
| M1 Project Information was shared with the CHSA | 0.681 |
| EE2 Project team members communicated frequently with the CHSA | 0.543 |
| Factor | |
| 2 | |
| T2 I trusted that the CHSA would fulfil their obligations | 0.799 |
| T3 I trusted the CHSA based on previous interactions and experience | 0.794 |
| T6 I trusted the role of CHSA | 0.785 |
| PCS2 The CHSA respected the inputs of other project team members | 0.778 |
| PCS1 The CHSA was willing to work with other project team members | 0.753 |
| T5 I trusted the CHSA based on their professional registration | 0.692 |
| T4 I trusted the CHSA based on their education background | 0.670 |
| PCS3 The CHSA placed project interests above individual interests | 0.610 |
| PCS8 The CHSA had knowledge of the health and safety management | 0.552 |
| Factor | |
| 3 | |
| IS4 Professional bodies ensured the implementation of health and safety by communicating good health and safety practices to the CHSA | 0.819 |
| IS3 Health and safety legislation requirements were adhered to because of the professional bodies | 0.808 |
| IS2 Health and safety legislation requirements were adhered to because of the department of labor | 0.728 |
| IS5 Professional bodies communicated new construction practices to the CHSA | 0.656 |
| IS1 The involvement of the CHSA was ensured because of health and safety legislation requirements | 0.620 |
| Factor | |
| 4 | |
| PC6 We used a project structure that promoted good relationships between the CHSA and project team members | 0.707 |
| PC3 There was two-way communication | 0.684 |
| PC2 Project objectives were defined clearly | 0.675 |
| CP6 The CHSA worked with project team members to achieve a goal of zero accidents | 0.670 |
| PC7 Project knowledge was shared with the CHSA | 0.665 |
| PC5 Project team members worked with the CHSA to deal with the complexity of the project | 0.659 |
| PC1 Project roles were clear | 0.658 |
| CP1 Project team members were committed to the project vision | 0.642 |
| Factor | |
| 5 | |
| PCS7 The CHSA had knowledge of the financials and costs | 0.711 |
| Extraction method: principal axis factoring. Rotation method: varimax with Kaiser normalization. | |
| Rotation converged in 7 iterations. | |
| Factor | Initial Eigenvalues | Extraction Sums of Squared Loadings | ||||
|---|---|---|---|---|---|---|
| Total | % of Variance | Cumulative % | Total | % of Variance | Cumulative % | |
| 1 | 27.553 | 61.230 | 61.230 | 27.320 | 60.712 | 60.712 |
| 2 | 2.976 | 6.614 | 67.843 | 2.751 | 6.113 | 66.825 |
| 3 | 2.166 | 4.814 | 72.658 | 1.923 | 4.274 | 71.098 |
| 4 | 1.446 | 3.212 | 75.870 | 1.233 | 2.741 | 73.839 |
| 5 | 1.257 | 2.794 | 78.664 | 1.028 | 2.285 | 76.124 |
| 6 | 0.941 | 2.091 | 80.755 | |||
| 7 | 0.822 | 1.827 | 82.582 | |||
| 8 | 0.701 | 1.557 | 84.139 | |||
| 9 | 0.650 | 1.445 | 85.584 | |||
| 10 | 0.557 | 1.238 | 86.822 | |||
| 11 | 0.471 | 1.047 | 87.869 | |||
| 12 | 0.455 | 1.010 | 88.880 | |||
| 13 | 0.422 | 0.939 | 89.819 | |||
| 14 | 0.369 | 0.821 | 90.639 | |||
| 15 | 0.323 | 0.717 | 91.356 | |||
| 16 | 0.288 | 0,639 | 91.996 | |||
| 17 | 0.277 | 0.615 | 92.610 | |||
| 18 | 0.258 | 0.573 | 93.183 | |||
| 19 | 0.236 | 0.525 | 93.708 | |||
| 20 | 0.226 | 0.503 | 94.211 | |||
| 21 | 0.220 | 0.488 | 94.699 | |||
| 22 | 0.206 | 0.458 | 95.157 | |||
| 23 | 0.203 | 0.451 | 95.608 | |||
| 24 | 0.188 | 0.419 | 96.027 | |||
| 25 | 0,165 | 0.367 | 96.394 | |||
| 26 | 0,156 | 0.346 | 96.740 | |||
| 27 | 0,146 | 0.325 | 97.066 | |||
| 28 | 0,132 | 0.294 | 97.360 | |||
| 29 | 0,124 | 0.276 | 97.636 | |||
| 30 | 0,112 | 0.250 | 97.886 | |||
| 31 | 0,106 | 0.235 | 98.121 | |||
| 32 | 0.095 | 0.211 | 98.332 | |||
| 33 | 0.088 | 0.196 | 98.528 | |||
| 34 | 0.082 | 0.181 | 98.709 | |||
| 35 | 0.074 | 0.165 | 98.874 | |||
| 36 | 0.073 | 0.163 | 99.037 | |||
| 37 | 0.065 | 0.145 | 99.182 | |||
| 38 | 0,061 | 0.135 | 99.317 | |||
| 39 | 0.056 | 0.124 | 99.441 | |||
| 40 | 0.054 | 0.119 | 99.560 | |||
| 41 | 0.047 | 0.104 | 99.664 | |||
| 42 | 0.045 | 0.100 | 99.763 | |||
| 43 | 0.041 | 0.092 | 99.855 | |||
| 44 | 0.034 | 0.075 | 99.930 | |||
| 45 | 0.031 | 0.070 | 100.000 | |||
| Kaiser–Meyer–Olkin Measure of Sampling Adequacy. | 0.958 | |
|---|---|---|
| Bartlett’s Test of Sphericity | Approx. Chi-Square | 4886.122 |
| df | 120 | |
| Sig. | 0.000 | |
| Factor | |
|---|---|
| 1 | |
| HSP8 The way CHSA collaborated with project team members reduced the number of workers affected by work related injuries | 0.862 |
| HSP6 The way CHSA collaborated with project team members promoted Health and safety awareness on the project | 0.857 |
| HSP5 The way CHSA collaborated with project team members promoted safe work behavior | 0.827 |
| HSP4 The way CHSA collaborated with project team members led to the Integration of H&S aspects on project | 0.810 |
| HSP1 The way CHSA collaborated with project team members reduced work related injuries and accidents | 0.786 |
| HSP7 The way CHSA collaborated with project team members led to the elimination of construction hazards | 0.774 |
| HSP2 The way CHSA collaborated with project team members reduced work related illnesses and diseases | 0.768 |
| HSP3 The way CHSA collaborated with project team members led to the reduction of total cost related to accidents and injuries | 0.709 |
| Factor | |
| 2 | |
| CC6 There was integration of skills and knowledge | 0.876 |
| CC2 There was a fair distribution of roles between the CHSA and project team members | 0.841 |
| CC1 Participative decision making was encouraged between the CHSA and project team members | 0.839 |
| CC4 Collaborative spirit existed between the CHSA and project team members | 0.804 |
| CC5 There was alignment of contributions provided by the CHSA and project team members | 0.779 |
| CC7 Conflict resolution mechanism was established | 0.725 |
| CC3 The CHSA held regular meetings with project team members | 0.703 |
| CC8 Top management provided support to the CHSA and project team members | 0.664 |
| Extraction method: principal axis factoring. Rotation method: varimax with Kaiser normalization | |
| a. Rotation converged in 3 iterations. |
| Factor | Initial Eigenvalues | Extraction Sums of Squared Loadings | ||||
|---|---|---|---|---|---|---|
| Total | % of Variance | Cumulative % | Total | % of Variance | Cumulative % | |
| 1 | 12.211 | 76.319 | 76.319 | 12.036 | 75.226 | 75.226 |
| 2 | 1.259 | 7.869 | 84.187 | 1.096 | 6.853 | 82.078 |
| 3 | 0.400 | 2.499 | 86.687 | |||
| 4 | 0.348 | 2.176 | 88.863 | |||
| 5 | 0.305 | 1.908 | 90.770 | |||
| 6 | 0.281 | 1.756 | 92.527 | |||
| 7 | 0.201 | 1.256 | 93.783 | |||
| 8 | 0.177 | 1.106 | 94.889 | |||
| 9 | 0.157 | 0.980 | 95.868 | |||
| 10 | 0.133 | 0.829 | 96.697 | |||
| 11 | 0.123 | 0.769 | 97.467 | |||
| 12 | 0.112 | 0.699 | 98.166 | |||
| 13 | 0.097 | 0.604 | 98.770 | |||
| 14 | 0.077 | 0.479 | 99.249 | |||
| 15 | 0.068 | 0.427 | 99.676 | |||
| 16 | 0.052 | 0.324 | 100.000 | |||
| Construct | Mardia’s Coefficient | (S − Bχ2) | Df | Chiq/Df | CFI | SRMR | RMSEA | MFI |
|---|---|---|---|---|---|---|---|---|
| Mutuality | 50.5462 | 21.5289 | 9 | 2.392 | 0.971 | 0.033 | 0.081 | 0.971 |
| Trust and | 89.7255 | 52.1693 | 14 | 3.726 | 0.850 | 0.048 | 0.113 | 0.914 |
| Institutional support (IS) | 38.3234 | 18.9481 | 5 | 3.789 | 0.959 | 0.035 | 0.115 | 0.968 |
| Project context and common purpose (PCP) | 70.6309 | 60.5622 | 20 | 3.028 | 0.890 | 0.041 | 0.098 | 0.909 |
| CHSA collaboration (CC) | 54.3420 | 35.8348 | 20 | 1.791 | 0.974 | 0.019 | 0.061 | 0.964 |
| H&S performance (HSP) | 65.9500 | 56.8808 | 20 | 2.844 | 0.906 | 0.019 | 0.093 | 0.917 |
| Construct | Number of Indicator Variables | Cronbach’s Alpha | Rho Coefficient |
|---|---|---|---|
| Mutuality | 6 | 0.951 | 0.951 |
| Trust | 7 | 0.954 | 0.954 |
| Institutional support | 5 | 0.927 | 0.933 |
| Project context and common purpose | 8 | 0.957 | 0.958 |
| CHSA collaboration | 8 | 0.977 | 0.977 |
| H&S performance | 8 | 0.974 | 0.974 |
| Fit Index | Cut-Off Value | Estimate | Comment | Sources |
|---|---|---|---|---|
| Df | 0≥ | 4 | Acceptable | [65,72] |
| Chiq/Df | Values between 2.0 and 5.0 indicate good fit | 4.405 | Good fit | [66,72]. |
| CFI | Values equal or greater to 0.90 (acceptable fit) or equal or greater than 0.95 (good fit) | 0.953 | Good fit | [70,71] |
| SRMR | Values equal or less than 0.50 (good fit) and equal or less than 0.80 (acceptable fit) | 0.048 | Good fit | [70,71] |
| RMSEA | Values equal to 0.08 (acceptable fit) and values less than 0.05 (good fit) 90% confidence interval | 0.113 0.070–0.189 | In acceptable range | [66,70,71,72] |
| MFI | Values greater than 0.90 (good fit) and more than 1.0 (perfect fit) | 0.969 | Good fit | [65,70,73]. |
| Parameter | Variable | Estimate | Standard Error | T-Statistic |
|---|---|---|---|---|
| P5p1 | Mutuality (M) influence CHSA collaboration | 0.104 | 0.046 (0.60) | 2.169 (1.648) |
| P5p2 | Trust (T) influence CHSA collaboration | 0.107 | 0.047 (104) | 2.769 (1.265) |
| P5p3 | Institutional support (IS) influence CHSA collaboration | 0.088 | 0.036 (0.48) | 2.254 (1.707) |
| P5p4 | Project context and common purpose (PCP) influence CHSA collaboration | 0.689 | 0.061 (0.71) | 12.729 (10.93) |
| P6p5 | CHSA collaboration (CC) influences H&S performance (HSP) | 0.882 | 0.35 (0.62) | 21.000 (11.89) |
| Factor | Unstandardized Coefficient | Standardized Coefficient | Z-Statistics | Significant at 5% Level? |
|---|---|---|---|---|
| MEE | 0.099 | 0.104 | 2.169 (1.648) | No |
| TPC | 0.132 | 0.107 | 2.769 (1.265) | No |
| IS | 0.082 | 0.088 | 2.254 (1.707) | No |
| PCP | 0.781 | 0.689 | 12.729 (10.93) | Yes |
| CC | 0.738 | 0.882 | 21.000 (11.89) | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rantsatsi, N.P.; Musonda, I.; Agumba, J. Construction Health and Safety Agent Collaboration and Its Influence on Health and Safety Performance in the South African Construction Industry. Safety 2023, 9, 8. https://doi.org/10.3390/safety9010008
Rantsatsi NP, Musonda I, Agumba J. Construction Health and Safety Agent Collaboration and Its Influence on Health and Safety Performance in the South African Construction Industry. Safety. 2023; 9(1):8. https://doi.org/10.3390/safety9010008
Chicago/Turabian StyleRantsatsi, Ndaleni Phinias, Innocent Musonda, and Justus Agumba. 2023. "Construction Health and Safety Agent Collaboration and Its Influence on Health and Safety Performance in the South African Construction Industry" Safety 9, no. 1: 8. https://doi.org/10.3390/safety9010008