
Clinical Utility of 18Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography (18F-FDG PET/CT) in Multivisceral Transplant Patients
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Imaging
2.4. 18F-FDG PET/CT Interpretation
2.5. Clinical Assessment of Examination Results and Utility
3. Results
3.1. General
3.2. Sepsis
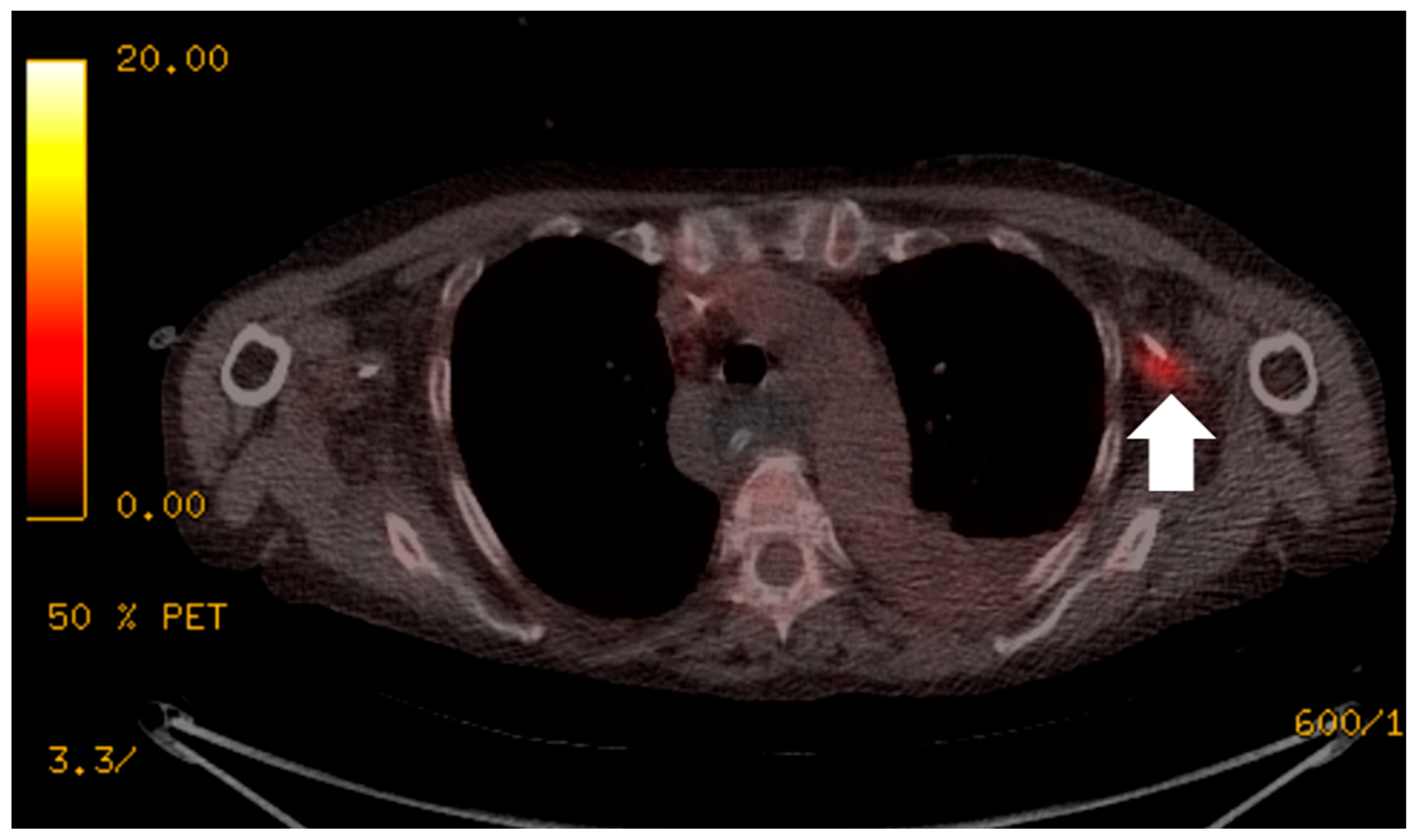
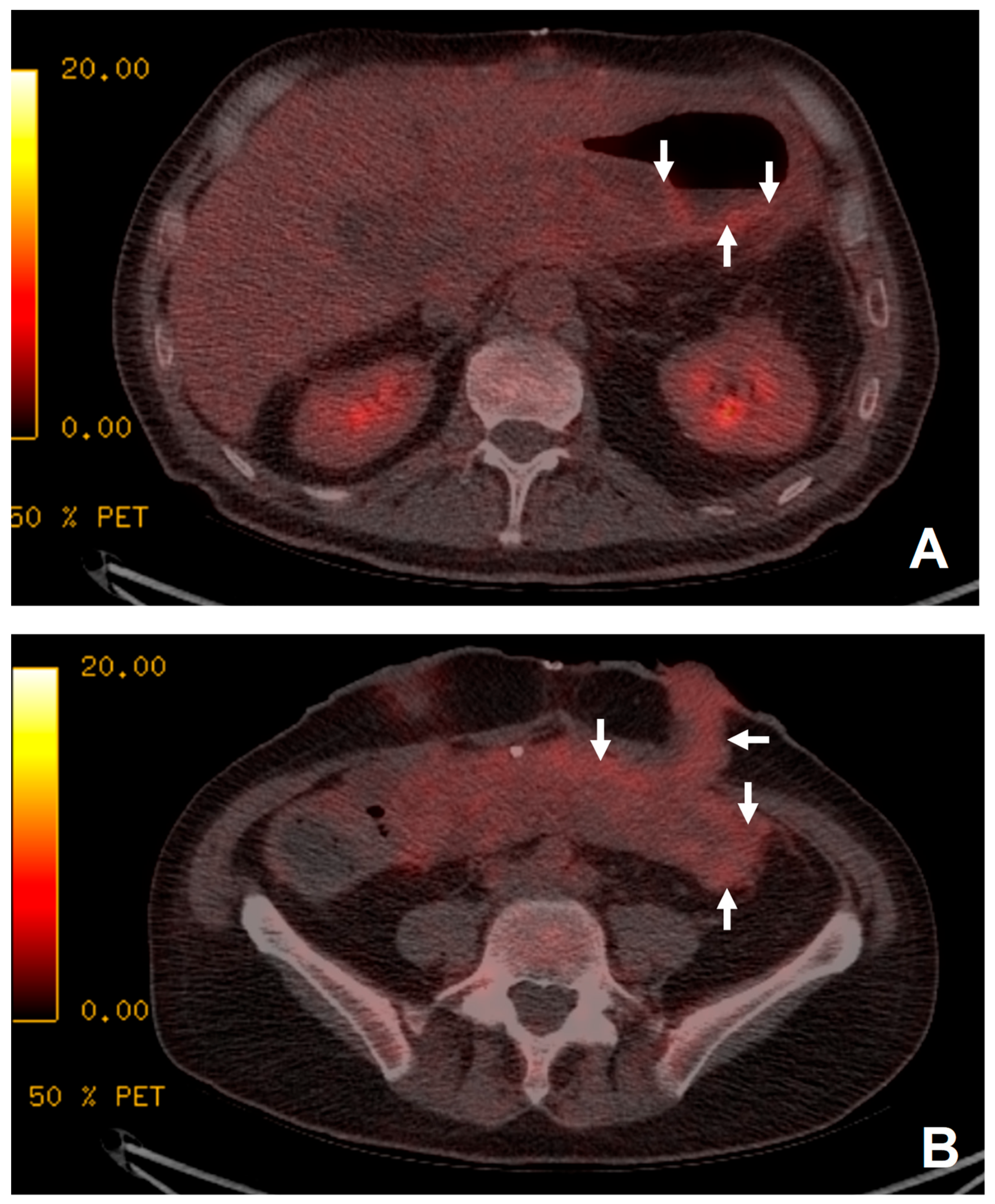
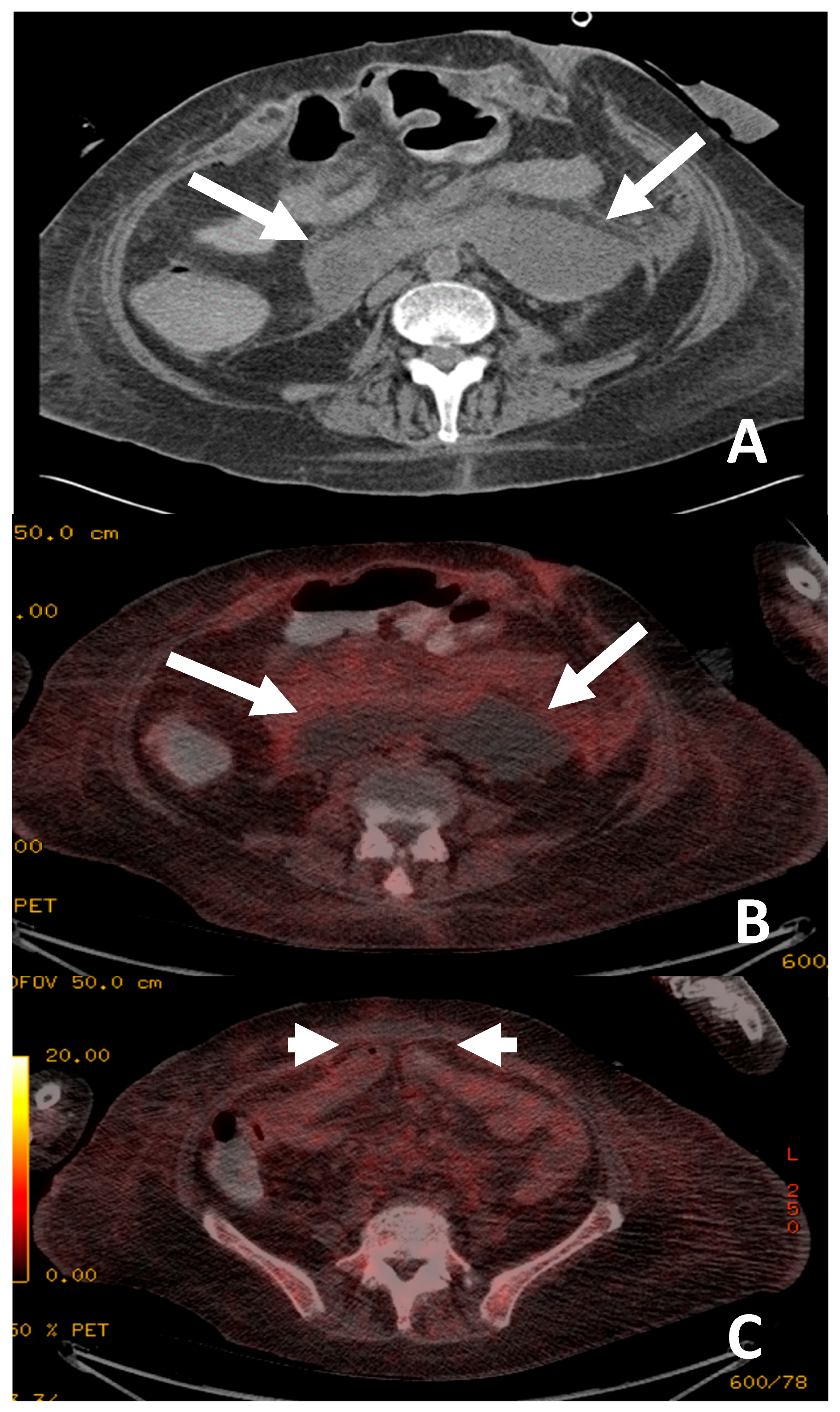
3.3. Specific Sites for Infection
3.4. Post-Transplant Lymphoproliferative Disorder
3.5. Rejection
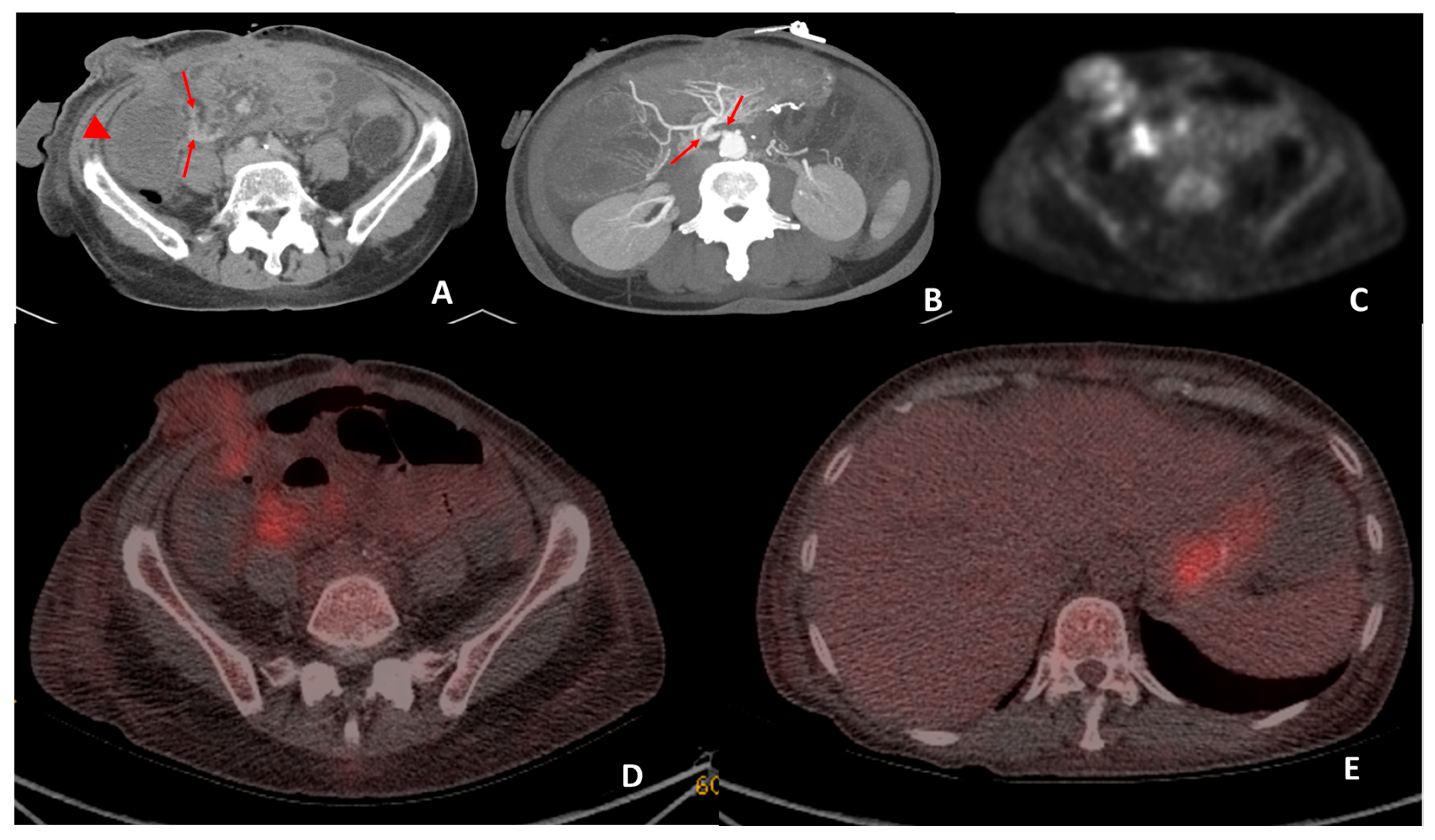
3.6. Malignancy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yildiz, B.D. Where are we at with short bowel syndrome and small bowel transplant. World J. Transplant. 2012, 2, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, E.; Upponi, S.; See, T.; Cheow, H.; Sivaprakasam, R.; Butler, A.; Whitley, S. A radiologist’s guide to small bowel and multivisceral transplantation. Clin. Radiol. 2013, 68, 983–991. [Google Scholar] [CrossRef]
- Nightingale, J.; Woodward, J.M.; Small Bowel and Nutrition Committee of the British Society of Gastroenterology. Guidelines for management of patients with a short bowel. Gut 2006, 55, iv1–iv12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangus, R.S.; Tector, A.J.; Kubal, C.A.; Fridell, J.A.; Vianna, R.M. Multivisceral Transplantation: Expanding Indications and Improving Outcomes. J. Gastrointest. Surg. 2013, 17, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Tzakis, A.G.; Kato, T.; Levi, D.M.; DeFaria, W.; Selvaggi, G.; Weppler, D.; Nishida, S.; Moon, J.; Madariaga, J.R.; David, A.I.; et al. 100 Multivisceral Transplants at a Single Center. Ann. Surg. 2005, 242, 480–493. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.G.; Nakamura, K.; Tsamandas, A.C.; Abu-Elmagd, K.; Furukawa, H.; Hutson, W.R.; Reyes, J.; Tabasco-Minguillan, J.S.; Todo, S.; Demetris, A.J. Pathology of human intestinal transplantation. Gastroenterology 1996, 110, 1820–1834. [Google Scholar] [CrossRef]
- Alsina, A.E.; Krisiunas, L.; Rosenberg, R.J.; Sziklas, J.J.; Schweizer, R.T. Value of 111indium leukocyte scanning in febrile organ transplant patients. Clin. Transplant. 1991, 5, 368–375. [Google Scholar]
- Alavi, J.B.; Alavi, A.; Staum, M. Evaluation of Infection in Neutropenic Patients with lndium-111-Labeled Donor Granulocytes. Clin. Nucl. Med. 1980, 5, 397–400. [Google Scholar] [CrossRef]
- Lin, S.; Marcus, C.S. Augmentation of Leukocyte Count With G-CSF in a Patient With Neutropenia Before In-111 WBC Scintigraphy. Clin. Nucl. Med. 1996, 21, 544–546. [Google Scholar] [CrossRef]
- Noraini, A.R.; Gay, E.; Ferrara, C.; Ravelli, E.; Mancini, V.; Morra, E.; Muti, P.; Tahir, A.; Jalil, N.A.; Rossetti, C. PET-CT as an effective imaging modality in the staging and follow-up of post-transplant lymphoproliferative disorder following solid organ transplantation. Singap. Med. J. 2009, 50, 1189–1195. [Google Scholar]
- Bodet-Milin, C.; Lacombe, M.; Malard, F.; Lestang, E.; Cahu, X.; Chevallier, P.; Guillaume, T.; Delaunay, J.; Brissot, E.; Moreau, P.; et al. 18F-FDG PET/CT for the assessment of gastrointestinal GVHD: Results of a pilot study. Bone Marrow Transplant. 2014, 49, 131–137. [Google Scholar] [CrossRef]
- Graute, V.; Jansen, N.; Sohn, H.-Y.; Becker, A.; Klein, B.; Schmid, I.; Greil, S.; Lehner, S.; Bartenstein, P.; Pfluger, T.; et al. Diagnostic role of whole-body [18F]-FDG positron emission tomography in patients with symptoms suspicious for malignancy after heart transplantation. J. Heart Lung Transplant. 2012, 31, 958–966. [Google Scholar] [CrossRef]
- Primeggia, J.; Matsumoto, C.; Fishbein, T.; Karacki, P.; Fredette, T.; Timpone, J. Infection among adult small bowel and multivisceral transplant recipients in the 30-day postoperative period. Transpl. Infect. Dis. 2013, 15, 441–448. [Google Scholar] [CrossRef]
- Meller, J.; Koster, G.; Liersch, T.; Siefker, U.; Lehmann, K.; Meyer, I.; Schreiber, K.; Altenvoerde, G.; Becker, W. Chronic bacterial osteomyelitis: Prospective comparison of 18F-FDG imaging with a dual-head coincidence camera and 111In-labelled autologous leucocyte scintigraphy. Eur. J. Nucl. Med. 2002, 29, 53–60. [Google Scholar] [CrossRef]
- Al-Mansour, Z.; Nelson, B.P.; Evens, A.M. Post-Transplant Lymphoproliferative Disease (PTLD): Risk Factors, Diagnosis, and Current Treatment Strategies. Curr. Hematol. Malign Rep. 2013, 8, 173–183. [Google Scholar] [CrossRef] [Green Version]
- Parker, A.; Bowles, K.; Bradley, J.A.; Emery, V.; Featherstone, C.; Gupte, G.; Marcus, R.; Parameshwar, J.; Ramsay, A.; Newstead, C.; et al. Management of post-transplant lymphoproliferative disorder in adult solid organ transplant recipients—BCSH and BTS Guidelines. Br. J. Haematol. 2010, 149, 693–705. [Google Scholar] [CrossRef]
- McCormack, L.; Hany, T.I.; Hübner, M.; Petrowsky, H.; Mullhaupt, B.; Knuth, A.; Stenner, F.; Clavien, P.-A. How Useful is PET/CT Imaging in the Management of Post-Transplant Lymphoproliferative Disease After Liver Transplantation? Am. J. Transplant. 2006, 6, 1731–1736. [Google Scholar] [CrossRef]
- Jerusalem, G.; Hustinx, R.; Beguin, Y.; Fillet, G. Evaluation of Therapy for Lymphoma. Semin. Nucl. Med. 2005, 35, 186–196. [Google Scholar] [CrossRef]
- Cremerius, U.; Fabry, U.; Wildberger, J.; Zimny, M.; Reinartz, P.; Nowak, B.; Schaefer, W.; Buell, U.; Osieka, R. Pre-transplant positron emission tomography (PET) using fluorine-18-fluoro-deoxyglucose (FDG) predicts outcome in patients treated with high-dose chemotherapy and autologous stem cell transplantation for non-Hodgkin’s lymphoma. Bone Marrow Transplant. 2002, 30, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Dierickx, D.; Tousseyn, T.; Requilé, A.; Verscuren, R.; Sagaert, X.; Morscio, J.; Wlodarska, I.; Herreman, A.; Kuypers, D.; Van Cleemput, J.; et al. The accuracy of positron emission tomography in the detection of posttransplant lymphoproliferative disorder. Haematologica 2013, 98, 771–775. [Google Scholar] [CrossRef]
- Timpone, J.G.; Girlanda, R.; Rudolph, L.; Fishbein, T.M. Infections in Intestinal and Multivisceral Transplant Recipients. Infect. Dis. Clin. N. Am. 2013, 27, 359–377. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, P. Updates on acute and chronic rejection in small bowel and multivisceral allografts. Curr. Opin. Organ Transplant. 2014, 19, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Wareham, N.E.; Lundgren, J.D.; Da Cunha-Bang, C.; Gustafsson, F.; Iversen, M.; Johannesen, H.H.; Kjær, A.; Rasmussen, A.; Sengeløv, H.; Sørensen, S.S.; et al. The clinical utility of FDG PET/CT among solid organ transplant recipients suspected of malignancy or infection. Eur. J. Nucl. Med. 2016, 44, 421–431. [Google Scholar] [CrossRef] [Green Version]
- Wareham, N.E.; Nielsen, S.D.; Sørensen, S.S.; Fischer, B.M. FDG PET/CT for Detection of Infectious Complications Following Solid Organ Transplantation. Semin. Nucl. Med. 2021, 51, 321–334. [Google Scholar] [CrossRef] [PubMed]
- Ouvrard, E.; De Mestier, L.; Boursier, C.; Lachachi, B.; Sahakian, N.; Chevalier, E.; Mikail, N.; Carullo, J.; Bando-Delaunay, A.; Walter, T.; et al. 18F-DOPA PET/CT at the Forefront of Initial or Presurgical Evaluation of Small-Intestine Neuroendocrine Tumors. J. Nucl. Med. 2022, 63, 1865–1870. [Google Scholar] [CrossRef]
- Addeo, P.; Poncet, G.; Goichot, B.; Leclerc, L.; Brigand, C.; Mutter, D.; Romain, B.; Namer, I.-J.; Bachellier, P.; Imperiale, A. The Added Diagnostic Value of 18F-Fluorodihydroxyphenylalanine PET/CT in the Preoperative Work-Up of Small Bowel Neuroendocrine Tumors. J. Gastrointest. Surg. 2017, 22, 722–730. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (at Examination) | Average 45.7 Years; Range, 22.9–61.9 Years | |
|---|---|---|
| Sex | Male | 10 |
| Female | 10 | |
| Indication for Multivisceral transplant | Primary cause | Numbers |
| Thromboembolic disease | 10 | |
| Complication of Crohn’s disease | 3 | |
| Intra-abdominal Malignancy | 1 (post Whipple’s procedure) 1 (small bowel resected with desmoid tumour) 1 (post-radiotherapy strictures) | |
| Visceral myopathy | 2 | |
| Volvolus | 1 | |
| Intussusception | 1 | |
| Small bowel obstruction secondary to adhesions | 1 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ong, S.J.; Sharkey, L.M.; Low, K.E.; Cheow, H.K.; Butler, A.J.; Buscombe, J.R. Clinical Utility of 18Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography (18F-FDG PET/CT) in Multivisceral Transplant Patients. J. Imaging 2023, 9, 114. https://doi.org/10.3390/jimaging9060114
Ong SJ, Sharkey LM, Low KE, Cheow HK, Butler AJ, Buscombe JR. Clinical Utility of 18Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography (18F-FDG PET/CT) in Multivisceral Transplant Patients. Journal of Imaging. 2023; 9(6):114. https://doi.org/10.3390/jimaging9060114
Chicago/Turabian StyleOng, Shao Jin, Lisa M. Sharkey, Kai En Low, Heok K. Cheow, Andrew J. Butler, and John R. Buscombe. 2023. "Clinical Utility of 18Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography (18F-FDG PET/CT) in Multivisceral Transplant Patients" Journal of Imaging 9, no. 6: 114. https://doi.org/10.3390/jimaging9060114