
Vasari Scoring System in Discerning between Different Degrees of Glioma and IDH Status Prediction: A Possible Machine Learning Application?
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statements
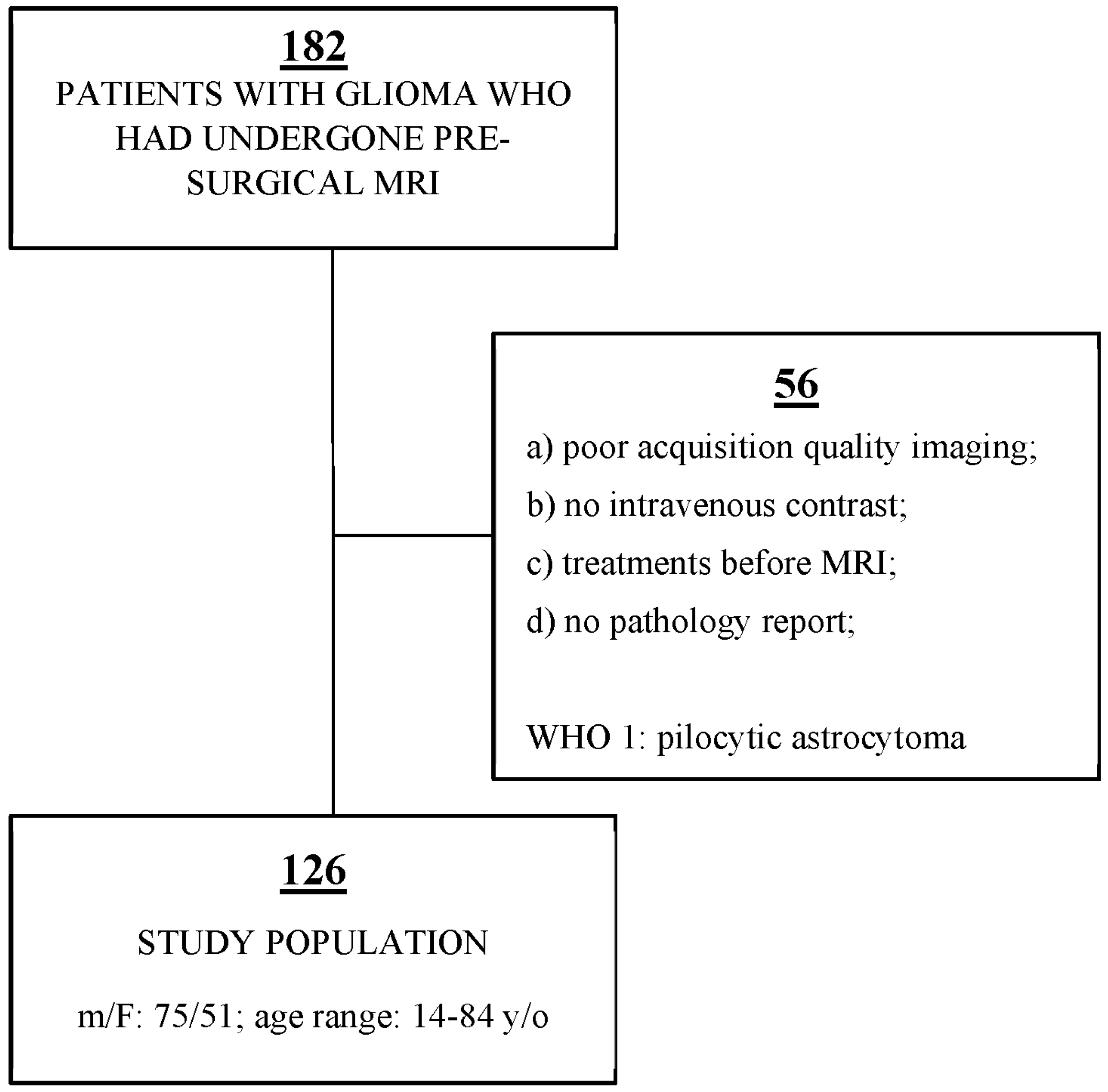
2.2. Patients
2.3. Magnetic Resonance Imaging Technique
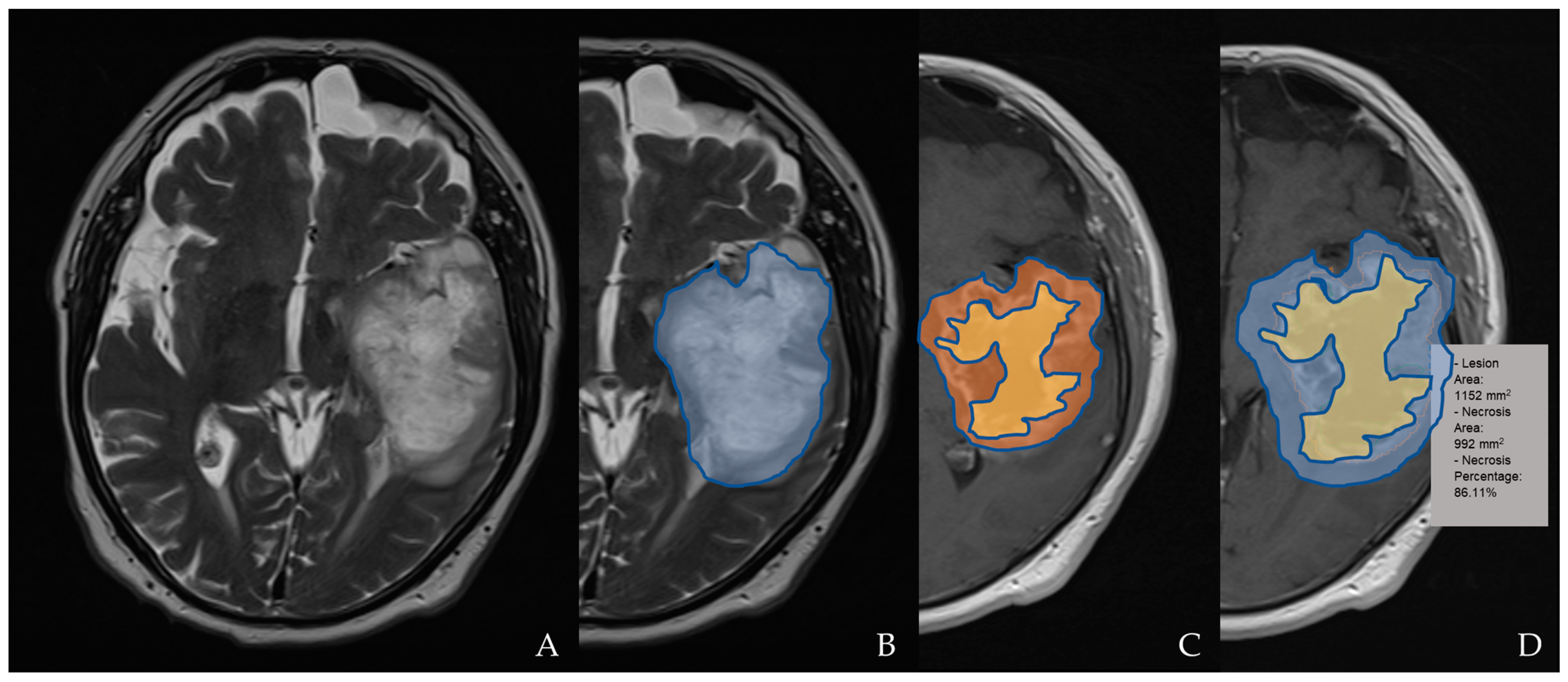
2.4. Magnetic Resonance Imaging Assessment and Analysis
2.5. Statistical Analysis
3. Results
3.1. Inter-Reader Agreement
3.2. Grade Prediction
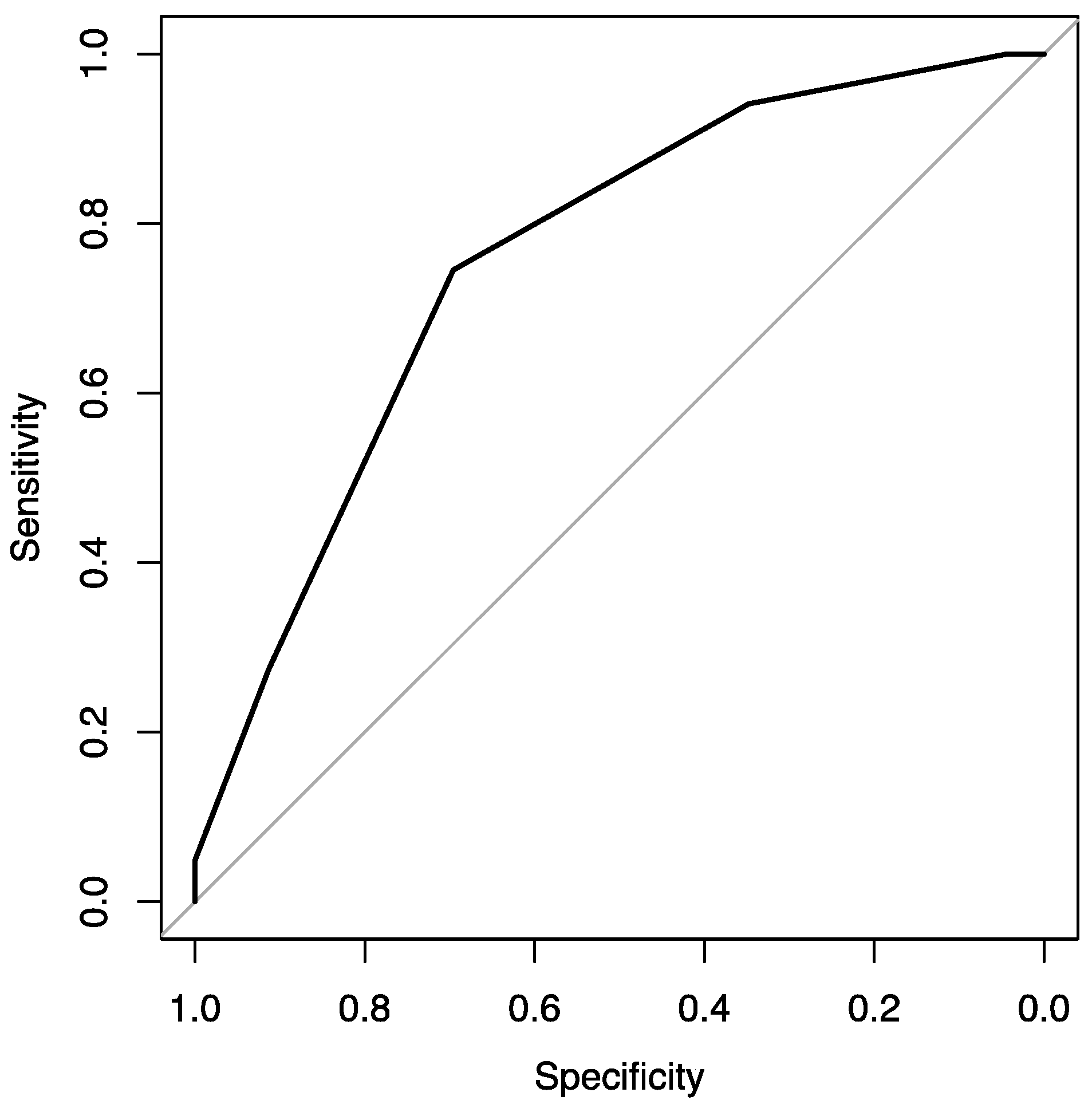
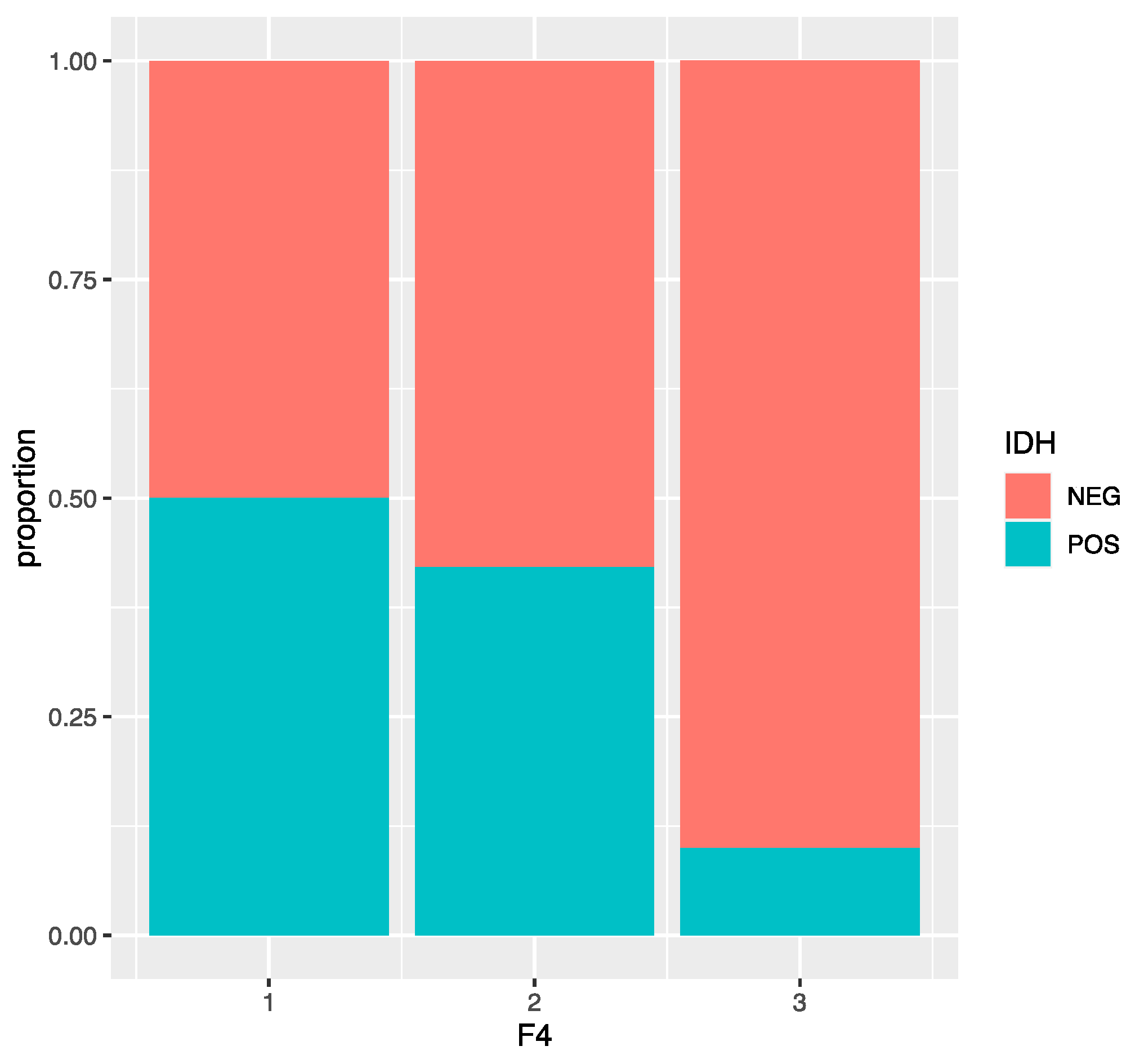
3.3. IDH Analysis
4. Discussion
- -
- The classes (low level/high level) are quite unbalanced (23 observations in the low level and 102 in the high level); we are planning to apply a balancing method, such as oversampling or undersampling, to improve the performance of the model.
- -
- The recent study showed that glioblastoma patients with a combination of deep white matter tracts and ependymal invasions on the imaging had a significant decrease in their overall survival compared with patients with an absence of such invasive imaging features. In this study, pial and ependymal invasions had a significantly increased risk of high-grade gliomas on the univariate analysis but not on the multivariate regression analysis.
- -
- Correlations between the patients’ outcomes and survival times and the VASARI scores were not identified in this study.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Omuro, A.; DeAngelis, L.M. Glioblastoma and other malignant gliomas: A clinical review. JAMA 2013, 310, 1842–1850. [Google Scholar] [CrossRef] [PubMed]
- Parsons, D.W.; Jones, S.; Zhang, X.; Lin, J.C.-H.; Leary, R.J.; Angenendt, P.; Mankoo, P.; Carter, H.; Siu, I.-M.; Gallia, G.L.; et al. An integrated genomic analysis of human glioblastoma multiforme. Science 2008, 321, 1807–1812. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Parsons, D.W.; Jin, G.; McLendon, R.; Rasheed, B.A.; Yuan, W.; Kos, I.; Batinic-Haberle, I.; Jones, S.; Riggins, G.J.; et al. IDH1 and IDH2 mutations in gliomas. N. Engl. J. Med. 2009, 360, 765–773. [Google Scholar] [CrossRef]
- Hartmann, C.; Meyer, J.; Balss, J.; Capper, D.; Mueller, W.; Christians, A.; Felsberg, J.; Wolter, M.; Mawrin, C.; Wick, W.; et al. Type and frequency of IDH1 and IDH2 mutations are related to astrocytic and oligodendroglial differentiation and age: A study of 1010 diffuse gliomas. Acta Neuropathol. 2009, 118, 469–474. [Google Scholar] [CrossRef]
- Houillier, C.; Wang, X.; Kaloshi, G.; Mokhtari, K.; Guillevin, R.; Laffaire, J.; Paris, S.; Boisselier, B.; Idbaih, A.; Laigle-Donadey, F.; et al. IDH1 or IDH2 mutations predict longer survival and response to temozolomide in low-grade gliomas. Neurology 2010, 75, 1560–1566. [Google Scholar] [CrossRef] [PubMed]
- König, I.R.; Fuchs, O.; Hansen, G.; Von Mutius, E.; Kopp, M.V. What is precision medicine? Eur. Respir. J. 2017, 50, 1700391. [Google Scholar] [CrossRef]
- Yang, K.; Wu, Z.; Zhang, H.; Zhang, N.; Wu, W.; Wang, Z.; Dai, Z.; Zhang, X.; Zhang, L.; Peng, Y.; et al. Glioma targeted therapy: Insight into future of molecular approaches. Mol. Cancer 2022, 21, 39. [Google Scholar] [CrossRef]
- Leibetseder, A.; Preusser, M.; Berghoff, A.S. New Approaches with Precision Medicine in Adult Brain Tumors. Cancers 2022, 14, 712. [Google Scholar] [CrossRef]
- Dunbar, E.; Yachnis, A.T. Glioma diagnosis: Immunohistochemistry and beyond. Adv. Anat. Pathol. 2010, 17, 187–201. [Google Scholar] [CrossRef]
- Nicholson, J.G.; Fine, H.A. Diffuse Glioma Heterogeneity and Its Therapeutic Implications. Cancer Discov. 2021, 11, 575–590. [Google Scholar] [CrossRef] [PubMed]
- Weller, M.; van den Bent, M.; Preusser, M.; Le Rhun, E.; Tonn, J.C.; Minniti, G.; Bendszus, M.; Balana, C.; Chinot, O.; Dirven, L.; et al. EANO guidelines on the diagnosis and treatment of diffuse gliomas of adulthood. Nat. Rev. Clin. Oncol. 2021, 18, 170–186, Erratum in Nat. Rev. Clin. Oncol. 2022, 19, 357–358. [Google Scholar] [CrossRef]
- VASARI—Cancer Imaging Program. Available online: https://wiki.nci.nih.gov/display/CIP/VASARI (accessed on 21 March 2020).
- Merkaj, S.; Bahar, R.C.; Zeevi, T.; Lin, M.; Ikuta, I.; Bousabarah, K.; Petersen, G.I.C.; Staib, L.; Payabvash, S.; Mongan, J.T.; et al. Machine Learning Tools for Image-Based Glioma Grading and the Quality of Their Reporting: Challenges and Opportunities. Cancers 2022, 14, 2623. [Google Scholar] [CrossRef]
- Rapisarda, A.; Melillo, G. Overcoming disappointing results with antiangiogenic therapy by targeting hypoxia. Nat. Rev. Clin. Oncol. 2012, 9, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Beig, N.; Patel, J.; Prasanna, P.; Hill, V.; Gupta, A.; Correa, R.; Bera, K.; Singh, S.; Partovi, S.; Varadan, V.; et al. Radiogenomic analysis of hypoxia pathway is predictive of overall survival in Glioblastoma. Sci. Rep. 2018, 8, 7. [Google Scholar] [CrossRef]
- Kickingereder, P.; Burth, S.; Wick, A.; Götz, M.; Eidel, O.; Schlemmer, H.-P.; Maier-Hein, K.H.; Wick, W.; Bendszus, M.; Radbruch, A.; et al. Radiomic Profiling of Glioblastoma: Identifying an Imaging Predictor of Patient Survival with Improved Performance over Established Clinical and Radiologic Risk Models. Radiology 2016, 280, 880–889. [Google Scholar] [CrossRef]
- McGarry, S.D.; Hurrell, S.L.; Kaczmarowski, A.L.; Cochran, E.J.; Connelly, J.; Rand, S.D.; Schmainda, K.M.; LaViolette, P.S. Magnetic Resonance Imaging-Based Radiomic Profiles Predict Patient Prognosis in Newly Diagnosed Glioblastoma Before Therapy. Tomography 2016, 2, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Li, Y.; Qian, Z.; Sun, Z.; Xu, K.; Wang, K.; Liu, S.; Fan, X.; Li, S.; Zhang, Z.; et al. A radiomic signature as a non-invasive predictor of progression-free survival in patients with lower-grade gliomas. Neuroimage Clin. 2018, 20, 1070–1077. [Google Scholar] [CrossRef]
- Zhou, H.; Vallières, M.; Bai, H.X.; Su, C.; Tang, H.; Oldridge, D.; Zhang, Z.; Xiao, B.; Liao, W.; Tao, Y.; et al. MRI features predict survival and molecular markers in diffuse lower-grade gliomas. Neuro Oncol. 2017, 19, 862–870, Erratum in Neuro Oncol. 2017, 19, 1701. [Google Scholar] [CrossRef]
- Kickingereder, P.; Götz, M.; Muschelli, J.; Wick, A.; Neuberger, U.; Shinohara, R.T.; Sill, M.; Nowosielski, M.; Schlemmer, H.-P.; Radbruch, A.; et al. Large-scale Radiomic Profiling of Recurrent Glioblastoma Identifies an Imaging Predictor for Stratifying Anti-Angiogenic Treatment Response. Clin. Cancer Res. 2016, 22, 5765–5771. [Google Scholar] [CrossRef]
- Grossmann, P.; Narayan, V.; Chang, K.; Rahman, R.; Abrey, L.; Reardon, D.A.; Schwartz, L.H.; Wen, P.Y.; Alexander, B.M.; Huang, R.; et al. Quantitative imaging biomarkers for risk stratification of patients with recurrent glioblastoma treated with bevacizumab. Neuro Oncol. 2017, 19, 1688–1697. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Zaccagna, F.; Rundo, L.; Testa, C.; Agati, R.; Lodi, R.; Manners, D.N.; Tonon, C. Convolutional Neural Network Techniques for Brain Tumor Classification (from 2015 to 2022): Review, Challenges, and Future Perspectives. Diagnostics 2022, 12, 1850. [Google Scholar] [CrossRef]
- Jaju, A.; Yeom, K.W.; Ryan, M.E. MR Imaging of Pediatric Brain Tumors. Diagnostics 2022, 12, 961. [Google Scholar] [CrossRef]
- Singh, G.; Manjila, S.; Sakla, N.; True, A.; Wardeh, A.H.; Beig, N.; Vaysberg, A.; Matthews, J.; Prasanna, P.; Spektor, V. Radiomics and radiogenomics in gliomas: A contemporary update. Br. J. Cancer 2021, 125, 641–657. [Google Scholar] [CrossRef]
- Tortora, M.; Gemini, L.; Scaravilli, A.; Ugga, L.; Ponsiglione, A.; Stanzione, A.; D’Arco, F.; D’Anna, G.; Cuocolo, R. Radiomics Applications in Head and Neck Tumor Imaging: A Narrative Review. Cancers 2023, 15, 1174. [Google Scholar] [CrossRef]
- Sacli-Bilmez, B.; Firat, Z.; Topcuoglu, O.M.; Yaltirik, K.; Ture, U.; Ozturk-Isik, E. Identifying overall survival in 98 glioblastomas using VASARI features at 3T. Clin. Imaging 2023, 93, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Yi, X.; Fu, Y.; Pang, P.; Deng, H.; Tang, H.; Han, Z.; Li, H.; Nie, J.; Gong, G.; et al. Preoperative Magnetic Resonance Imaging Radiomics for Predicting Early Recurrence of Glioblastoma. Front. Oncol. 2021, 11, 769188. [Google Scholar] [CrossRef] [PubMed]
- Lacroix, M.; Abi-Said, D.; Fourney, D.R.; Gokaslan, Z.L.; Shi, W.; DeMonte, F.; Lang, F.F.; McCutcheon, I.E.; Hassenbusch, S.J.; Holland, E.; et al. A multivariate analysis of 416 patients with glioblastoma multiforme: Prognosis, extent of resection, and survival. J. Neurosurg. 2001, 95, 190–198. [Google Scholar] [CrossRef]
- Yu, J.; Wang, M.; Song, J.; Huang, D.; Hong, X. Potential Utility of Visually AcceSAble Rembrandt Images Assessment in Brain Astrocytoma Grading. J. Comput. Assist. Tomogr. 2016, 40, 301–306. [Google Scholar] [CrossRef]
- Zhang, B.; Chang, K.; Ramkissoon, S.; Tanguturi, S.; Bi, W.L.; Reardon, D.A.; Ligon, K.L.; Alexander, B.M.; Wen, P.Y.; Huang, R.Y. Multimodal MRI features predict isocitrate dehydrogenase genotype in high-grade gliomas. Neuro Oncol. 2017, 19, 109–117. [Google Scholar] [CrossRef]
- Park, C.; Han, K.; Kim, H.; Ahn, S.; Choi, D.; Park, Y.; Chang, J.; Kim, S.; Cha, S.; Lee, S.-K. MRI Features May Predict Molecular Features of Glioblastoma in Isocitrate Dehydrogenase Wild-Type Lower-Grade Gliomas. AJNR Am. J. Neuroradiol. 2021, 42, 448–456. [Google Scholar] [CrossRef]
- Sun, C.; Fan, L.; Wang, W.; Wang, W.; Liu, L.; Duan, W.; Pei, D.; Zhan, Y.; Zhao, H.; Sun, T.; et al. Radiomics and Qualitative Features From Multiparametric MRI Predict Molecular Subtypes in Patients With Lower-Grade Glioma. Front. Oncol. 2022, 11, 756828. [Google Scholar] [CrossRef] [PubMed]
- Messina, C.; Bignone, R.; Bruno, A.; Bruno, A.; Bruno, F.; Calandri, M.; Caruso, D.; Coppolino, P.; De Robertis, R.; Gentili, F.; et al. Diffusion-Weighted Imaging in Oncology: An Update. Cancers 2020, 12, 1493. [Google Scholar] [CrossRef]
- Wu, C.-C.; Jain, R.; Radmanesh, A.; Poisson, L.; Guo, W.-Y.; Zagzag, D.; Snuderl, M.; Placantonakis, D.; Golfinos, J.; Chi, A. Predicting Genotype and Survival in Glioma Using Standard Clinical MR Imaging Apparent Diffusion Coefficient Images: A Pilot Study from The Cancer Genome Atlas. AJNR Am. J. Neuroradiol. 2018, 39, 1814–1820. [Google Scholar] [CrossRef]
- Su, C.-Q.; Lu, S.-S.; Zhou, M.-D.; Shen, H.; Shi, H.-B.; Hong, X.-N. Combined texture analysis of diffusion-weighted imaging with conventional MRI for non-invasive assessment of IDH1 mutation in anaplastic gliomas. Clin. Radiol. 2019, 74, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Durmo, F.; Rydelius, A.; Baena, S.C.; Askaner, K.; Lätt, J.; Bengzon, J.; Englund, E.; Chenevert, T.L.; Björkman-Burtscher, I.M.; Sundgren, P. Multivoxel 1H-MR Spectroscopy Biometrics for Preoprerative Differentiation Between Brain Tumors. Tomography 2018, 4, 172–181. [Google Scholar] [CrossRef]
- Farche, M.K.; Fachinetti, N.O.; da Silva, L.R.; Matos, L.A.; Appenzeller, S.; Cendes, F.; Reis, F. Revisiting the use of proton magnetic resonance spectroscopy in distinguishing between primary and secondary malignant tumors of the central nervous system. Neuroradiol. J. 2022, 35, 619–626. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Glioma Grade | ||||||
|---|---|---|---|---|---|---|
| Other Data | 1 (n = 3) | 2 (n = 21) | 3 (n = 18) | 4 (n = 84) | ||
| Age (year) | <50 | 3 | 10 | 8 | 18 | 39 |
| >50 | 0 | 11 | 10 | 66 | 87 | |
| Sex | Male | 2 | 8 | 11 | 54 | 75 |
| Female | 1 | 13 | 7 | 30 | 51 | |
| Location | Frontal | 0 | 12 | 9 | 28 | 49 |
| Temporal | 0 | 7 | 4 | 17 | 28 | |
| Insular | 2 | 2 | 1 | 6 | 11 | |
| Parietal | 0 | 0 | 1 | 22 | 23 | |
| Occipital | 0 | 0 | 2 | 2 | 4 | |
| Brain steam | 1 | 0 | 1 | 5 | 7 | |
| Other (cerebellum) | 0 | 0 | 0 | 4 | 4 | |
| Side | Right | 0 | 11 | 5 | 47 | 63 |
| Left | 2 | 0 | 2 | 5 | 9 | |
| Central/Bilateral | 1 | 10 | 11 | 32 | 54 | |
| Eloquent area | No | 2 | 15 | 13 | 45 | 75 |
| Motor speech | 1 | 2 | 1 | 7 | 11 | |
| Receptive speech | 0 | 4 | 2 | 16 | 22 | |
| Motor area | 0 | 0 | 1 | 15 | 16 | |
| Visual area | 0 | 0 | 1 | 1 | 2 | |
| IDH status | Positive | 2 | 13 | 3 | 4 | 22 |
| Negative | 1 | 8 | 15 | 80 | 104 | |
| F4 | OR | 2.5% | 97.5% | Level 1 Probability |
|---|---|---|---|---|
| as.factor(F4)1 | 1.285714 | 0.4790464 | 3.59729 | 0.5625000 |
| as.factor(F4)2 | 1.069444 | 0.2748978 | 4.15047 | 0.5789474 |
| as.factor(F4)3 | 7.972222 | 2.3284132 | 27.90801 | 0.9111111 |
| IDH Status | GRADE | ||||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | ||
| Negative | 0.8 | 3.2 | 10.4 | 65.6 | 80.0 |
| Positive | 0.8 | 13.6 | 4.0 | 1.6 | 20.0 |
| 1.6 | 16.8 | 14.4 | 67.2 | 100 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gemini, L.; Tortora, M.; Giordano, P.; Prudente, M.E.; Villa, A.; Vargas, O.; Giugliano, M.F.; Somma, F.; Marchello, G.; Chiaramonte, C.; et al. Vasari Scoring System in Discerning between Different Degrees of Glioma and IDH Status Prediction: A Possible Machine Learning Application? J. Imaging 2023, 9, 75. https://doi.org/10.3390/jimaging9040075
Gemini L, Tortora M, Giordano P, Prudente ME, Villa A, Vargas O, Giugliano MF, Somma F, Marchello G, Chiaramonte C, et al. Vasari Scoring System in Discerning between Different Degrees of Glioma and IDH Status Prediction: A Possible Machine Learning Application? Journal of Imaging. 2023; 9(4):75. https://doi.org/10.3390/jimaging9040075
Chicago/Turabian StyleGemini, Laura, Mario Tortora, Pasqualina Giordano, Maria Evelina Prudente, Alessandro Villa, Ottavia Vargas, Maria Francesca Giugliano, Francesco Somma, Giulia Marchello, Carmela Chiaramonte, and et al. 2023. "Vasari Scoring System in Discerning between Different Degrees of Glioma and IDH Status Prediction: A Possible Machine Learning Application?" Journal of Imaging 9, no. 4: 75. https://doi.org/10.3390/jimaging9040075