
Advances in Hydrogel Adhesives for Gastrointestinal Wound Closure and Repair

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
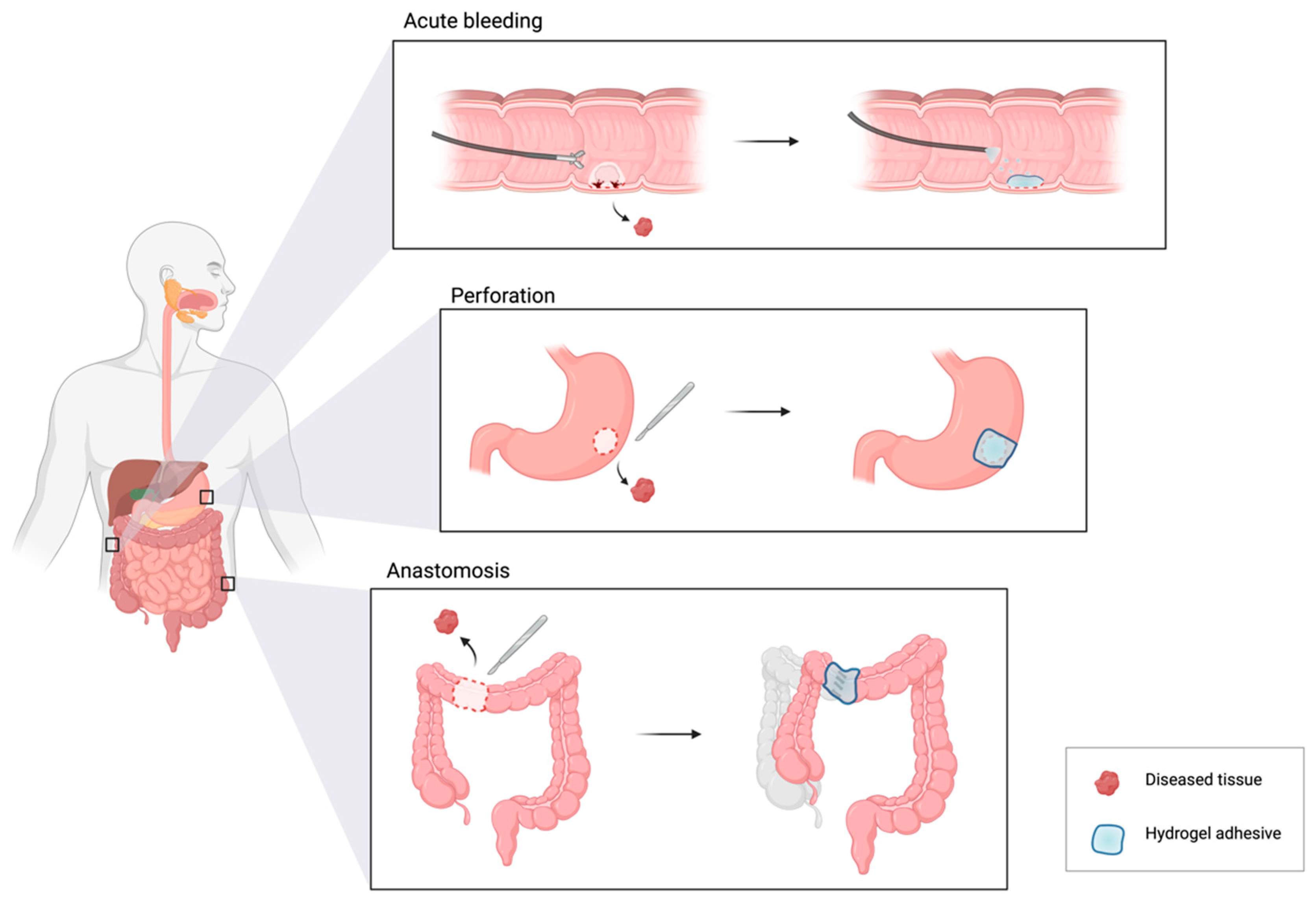
2. Acute GI Bleeding
2.1. Disease Condition and Current Standards
2.2. Hydrogel Requirements
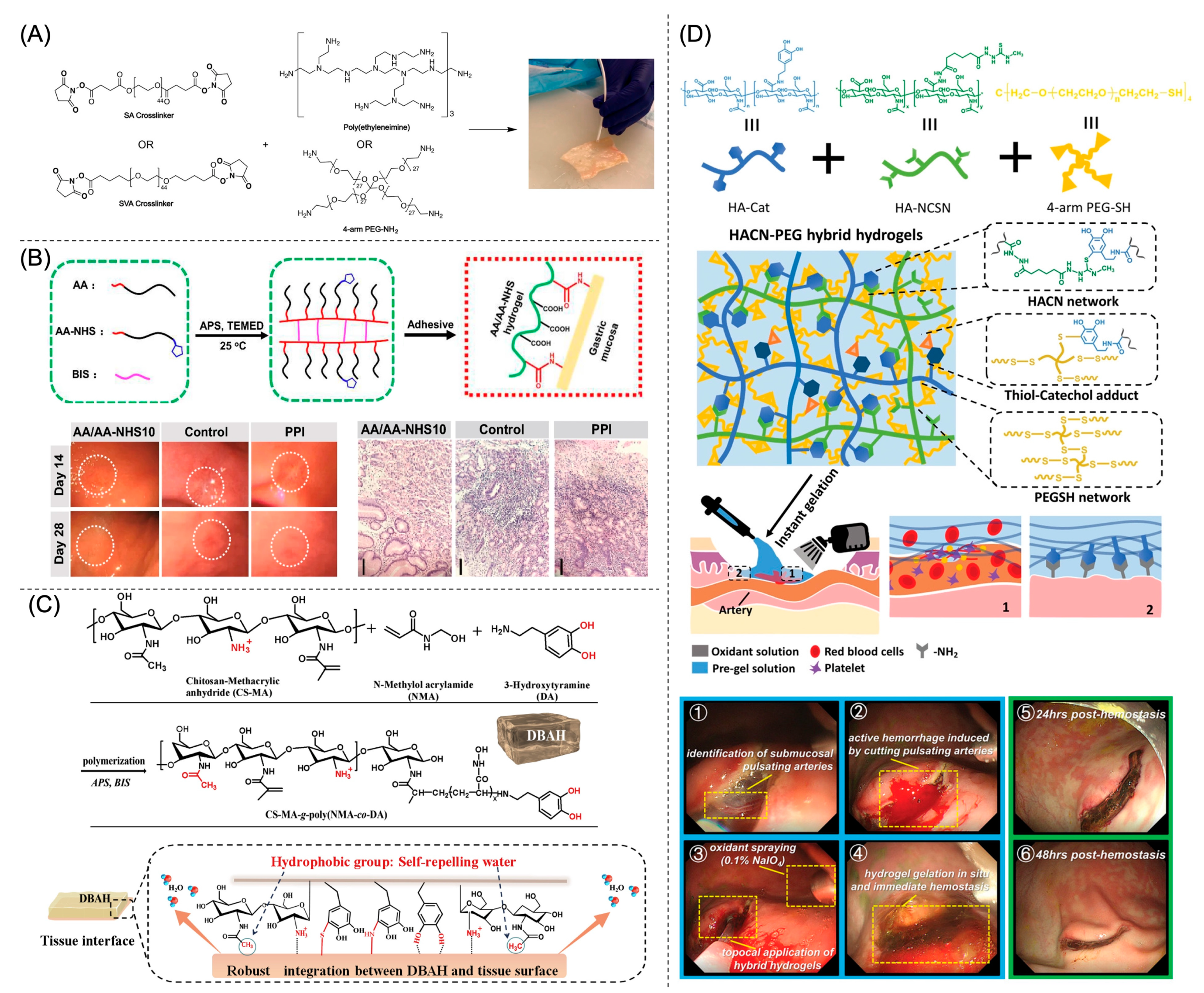
2.3. Crosslinking and Adhesion Mechanisms
2.4. Enhancing Wet Adhesion
2.5. Antibacterial Properties and Wound Healing
2.6. Summary
3. GI Perforation
3.1. Disease Condition and Current Standards
3.2. Hydrogel Requirements
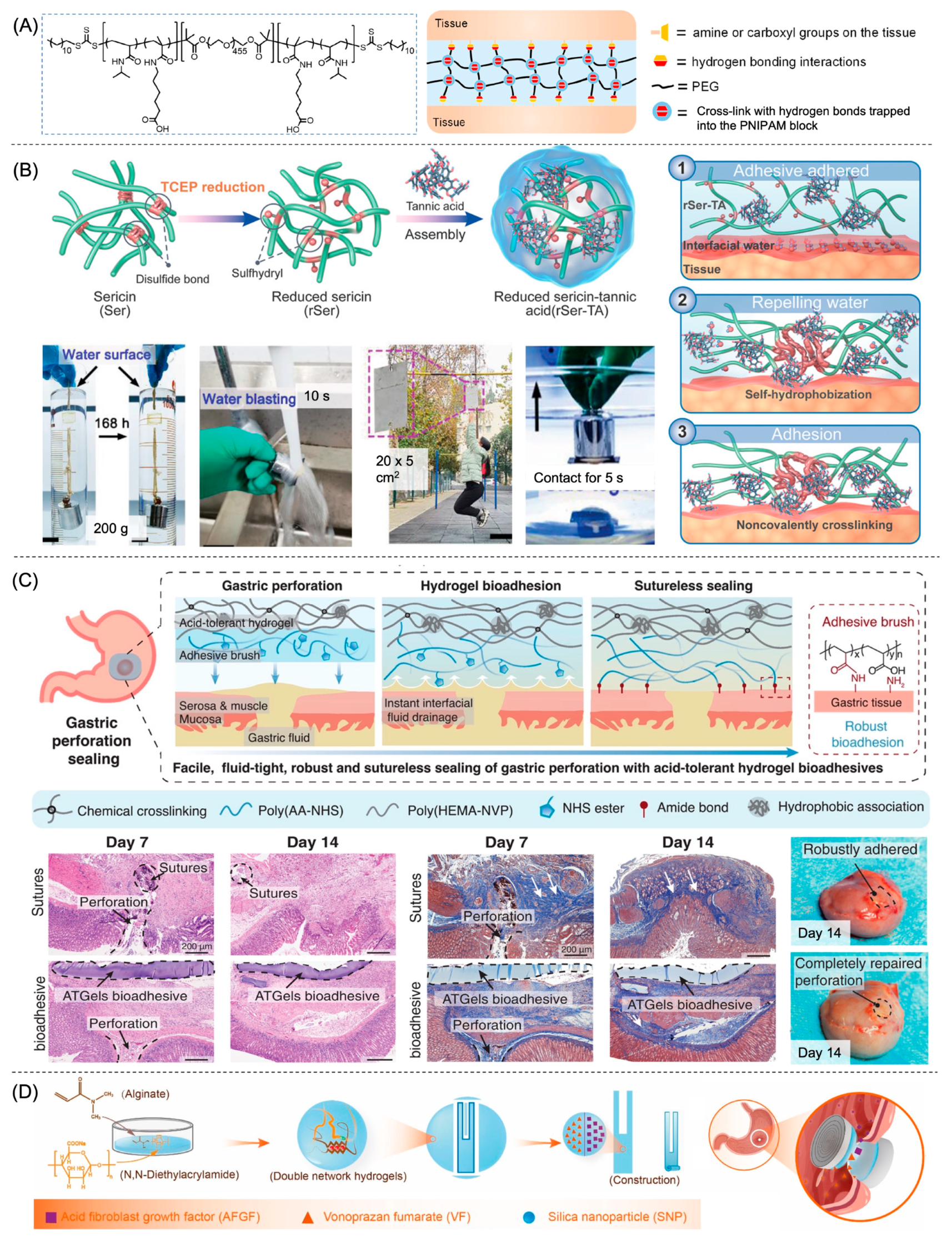
3.3. Crosslinking and Adhesion Mechanisms
3.4. Enhancing Wet Adhesion
3.5. Multifunctionality through Interpenetrating Polymer Networks
3.6. Hydrogel in Different Forms
3.7. Wound Healing
3.8. Summary
4. Anastomotic Leak
4.1. Disease Condition and Current Standards
4.2. Hydrogel Requirements
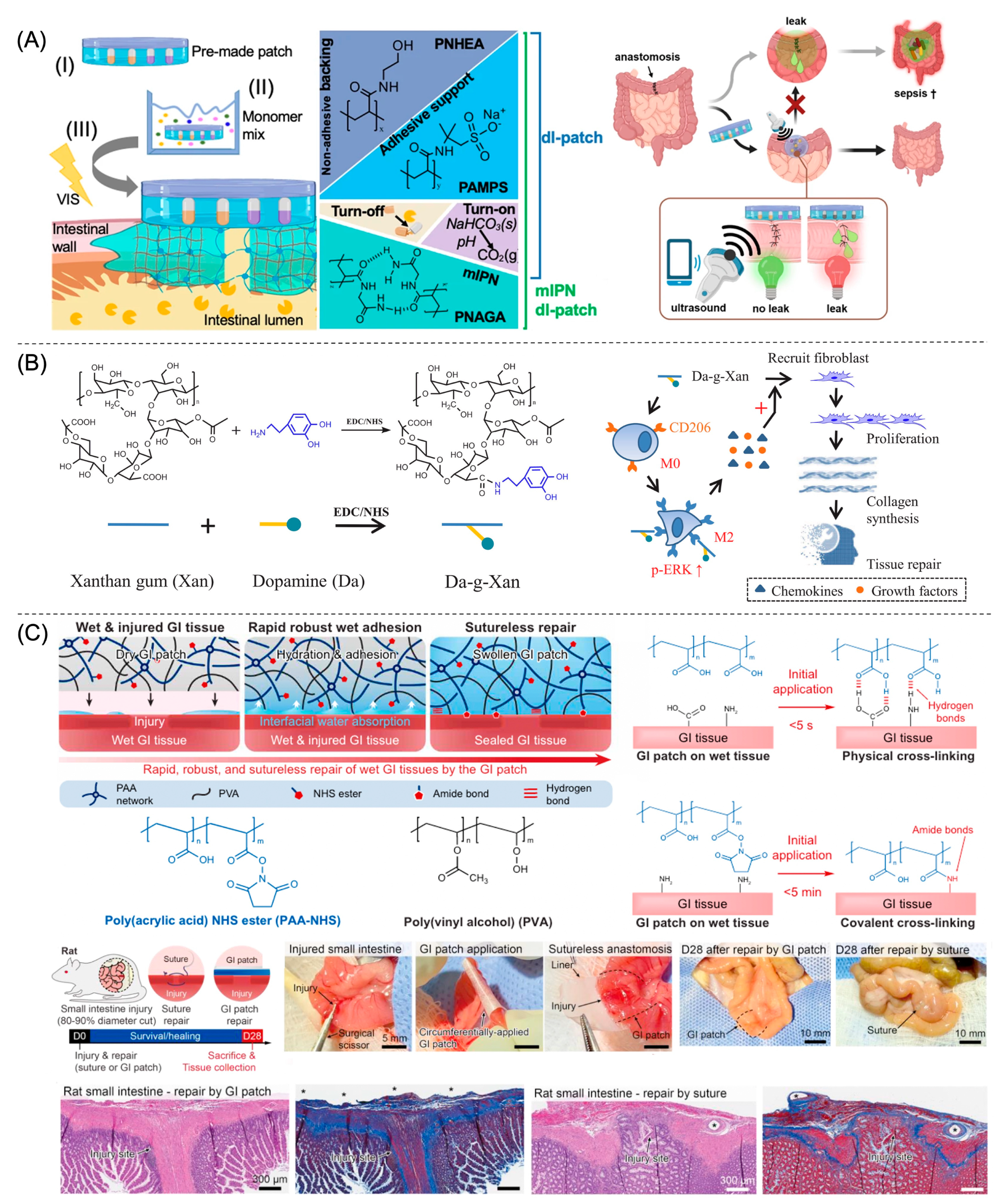
4.3. Hydrogels for Suture/Staple Reinforcement
4.4. Wound Healing
4.5. Anti-Adhesion
4.6. Sutureless Anastomosis
4.7. Leak Detection
4.8. Summary
5. Concluding Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Picut, C.A.; Coleman, G.D. Gastrointestinal Tract. In Atlas of Histology of the Juvenile Rat; Elsevier: Amsterdam, The Netherlands, 2016; pp. 127–171. ISBN 978-0-12-802682-3. [Google Scholar]
- Common Types of Gastrointestinal Surgical Procedures. Available online: https://www.farnorthsurgery.com/blog/common-types-of-gastrointestinal-surgical-procedures (accessed on 13 February 2023).
- Gastrointestinal Surgery. Available online: https://intermountainhealthcare.org/services/gastroenterology/treatment-and-detection-methods/gastrointestinal-surgery/ (accessed on 13 February 2023).
- Ye, S.-P.; Zhu, W.-Q.; Huang, Z.-X.; Liu, D.-N.; Wen, X.-Q.; Li, T.-Y. Role of Minimally Invasive Techniques in Gastrointestinal Surgery: Current Status and Future Perspectives. World J. Gastrointest. Surg. 2021, 13, 941–952. [Google Scholar] [CrossRef] [PubMed]
- Rudiman, R. Minimally Invasive Gastrointestinal Surgery: From Past to the Future. Ann. Med. Surg. 2021, 71, 102922. [Google Scholar] [CrossRef] [PubMed]
- Nam, S.; Mooney, D. Polymeric Tissue Adhesives. Chem. Rev. 2021, 121, 11336–11384. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.M.; Auyeung, K.K.Y.; Lam, S.F.; Chiu, P.W.Y.; Teoh, A.Y.B. Current Status in Endoscopic Management of Upper Gastrointestinal Perforations, Leaks and Fistulas. Dig. Endosc. 2022, 34, 43–62. [Google Scholar] [CrossRef]
- Li, M.; Pan, G.; Zhang, H.; Guo, B. Hydrogel Adhesives for Generalized Wound Treatment: Design and Applications. J. Polym. Sci. 2022, 60, 1328–1359. [Google Scholar] [CrossRef]
- Staudenmann, D.; Choi, K.K.H.; Kaffes, A.J.; Saxena, P. Current Endoscopic Closure Techniques for the Management of Gastrointestinal Perforations. Clin. Med. Insights Gastroenterol. 2022, 15, 263177452210767. [Google Scholar] [CrossRef]
- Wu, J.; Yuk, H.; Sarrafian, T.L.; Guo, C.F.; Griffiths, L.G.; Nabzdyk, C.S.; Zhao, X. An Off-the-Shelf Bioadhesive Patch for Sutureless Repair of Gastrointestinal Defects. Sci. Transl. Med. 2022, 14, eabh2857. [Google Scholar] [CrossRef]
- Ghobril, C.; Grinstaff, M.W. The Chemistry and Engineering of Polymeric Hydrogel Adhesives for Wound Closure: A Tutorial. Chem. Soc. Rev. 2015, 44, 1820–1835. [Google Scholar] [CrossRef]
- Bashir, S.; Hina, M.; Iqbal, J.; Rajpar, A.H.; Mujtaba, M.A.; Alghamdi, N.A.; Wageh, S.; Ramesh, K.; Ramesh, S. Fundamental Concepts of Hydrogels: Synthesis, Properties, and Their Applications. Polymers 2020, 12, 2702. [Google Scholar] [CrossRef]
- Zhang, L.; Liu, M.; Zhang, Y.; Pei, R. Recent Progress of Highly Adhesive Hydrogels as Wound Dressings. Biomacromolecules 2020, 21, 3966–3983. [Google Scholar] [CrossRef]
- Bovone, G.; Dudaryeva, O.Y.; Marco-Dufort, B.; Tibbitt, M.W. Engineering Hydrogel Adhesion for Biomedical Applications via Chemical Design of the Junction. ACS Biomater. Sci. Eng. 2021, 7, 4048–4076. [Google Scholar] [CrossRef]
- Shi, K.; Xue, B.; Liao, J.; Qu, Y.; Qian, Z. Polymeric Hydrogels for Post-Operative Adhesion Prevention: A Review. Mater. Express 2017, 7, 417–438. [Google Scholar] [CrossRef]
- Caló, E.; Khutoryanskiy, V.V. Biomedical Applications of Hydrogels: A Review of Patents and Commercial Products. Eur. Polym. J. 2015, 65, 252–267. [Google Scholar] [CrossRef] [Green Version]
- Pan, Z.; Ye, H.; Wu, D. Recent Advances on Polymeric Hydrogels as Wound Dressings. APL Bioeng. 2021, 5, 011504. [Google Scholar] [CrossRef]
- Anthis, A.H.C.; Hu, X.; Matter, M.T.; Neuer, A.L.; Wei, K.; Schlegel, A.A.; Starsich, F.H.L.; Herrmann, I.K. Chemically Stable, Strongly Adhesive Sealant Patch for Intestinal Anastomotic Leakage Prevention. Adv. Funct. Mater. 2021, 31, 2007099. [Google Scholar] [CrossRef]
- Evans, D.F.; Pye, G.; Bramley, R.; Clark, A.G.; Dyson, T.J.; Hardcastle, J.D. Measurement of Gastrointestinal PH Profiles in Normal Ambulant Human Subjects. Gut 1988, 29, 1035–1041. [Google Scholar] [CrossRef] [Green Version]
- Anthis, A.H.C.; Schlegel, A.A.; Hartel, M.; Herrmann, I.K. Sutureless Gastrointestinal Anastomoses. Nat. Biomed. Eng. 2022, 6, 1089–1091. [Google Scholar] [CrossRef]
- Johansson, M.E.V.; Sjövall, H.; Hansson, G.C. The Gastrointestinal Mucus System in Health and Disease. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 352–361. [Google Scholar] [CrossRef] [Green Version]
- Cheng, H.M.; Mah, K.K.; Seluakumaran, K. Motility: Peristalsis, Segmentation, Haustration and Mass Movement. In Defining Physiology: Principles, Themes, Concepts; Springer International Publishing: Cham, Switzerland, 2020; Volume 2, pp. 35–37. ISBN 978-3-030-62284-8. [Google Scholar]
- Antunes, C.; Copelin, E.L., II. Upper Gastrointestinal Bleeding. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Gastrointestinal Bleeding. Available online: https://medlineplus.gov/gastrointestinalbleeding.html (accessed on 14 February 2023).
- Lorenzo-Zúñiga, V.; Bustamante-Balén, M.; Pons-Beltrán, V. Prevention of Late Complications with Coverage Agents in Endoscopic Resection of Colorectal Lesions: Current Landscape in Gastrointestinal Endoscopy. World J. Gastroenterol. 2021, 27, 1563–1568. [Google Scholar] [CrossRef]
- Mangira, D.; Ket, S.N.; Majeed, A.; Gibson, P.R.; Brown, G. Postpolypectomy Prophylactic Clip Closure for the Prevention of Delayed Postpolypectomy Bleeding: A Systematic Review. JGH Open 2018, 2, 105–110. [Google Scholar] [CrossRef]
- Cook, K.; Naguib, N.; Price, C.E.; Katharios, S.; Kirsch, J.; Cortes, K.; Hohl, K.; O’Toole, G.A.; Grinstaff, M.W. Temporary In Situ Hydrogel Dressings for Colon Polypectomies. ACS Biomater. Sci. Eng. 2021, 7, 4362–4370. [Google Scholar] [CrossRef] [PubMed]
- Ito, S.; Nishiguchi, A.; Sasaki, F.; Maeda, H.; Kabayama, M.; Ido, A.; Taguchi, T. Robust Closure of Post-Endoscopic Submucosal Dissection Perforation by Microparticle-Based Wound Dressing. Mater. Sci. Eng. C 2021, 123, 111993. [Google Scholar] [CrossRef] [PubMed]
- Bon, I.; Bartolí, R.; Lorenzo-Zúñiga, V. Endoscopic Shielding Technique, a New Method in Therapeutic Endoscopy. World J. Gastroenterol. 2017, 23, 3761. [Google Scholar] [CrossRef] [PubMed]
- Xia, X.; Xu, X.; Wang, B.; Zhou, D.; Zhang, W.; Xie, X.; Lai, H.; Xue, J.; Rai, A.; Li, Z.; et al. Adhesive Hemostatic Hydrogel with Ultrafast Gelation Arrests Acute Upper Gastrointestinal Hemorrhage in Pigs. Adv. Funct. Mater. 2022, 32, 2109332. [Google Scholar] [CrossRef]
- Sankar, S.; O’Neill, K.; Bagot D’Arc, M.; Rebeca, F.; Buffier, M.; Aleksi, E.; Fan, M.; Matsuda, N.; Gil, E.S.; Spirio, L. Clinical Use of the Self-Assembling Peptide RADA16: A Review of Current and Future Trends in Biomedicine. Front. Bioeng. Biotechnol. 2021, 9, 679525. [Google Scholar] [CrossRef]
- Achneck, H.E.; Sileshi, B.; Jamiolkowski, R.M.; Albala, D.M.; Shapiro, M.L.; Lawson, J.H. A Comprehensive Review of Topical Hemostatic Agents: Efficacy and Recommendations for Use. Ann. Surg. 2010, 251, 217–228. [Google Scholar] [CrossRef]
- Mourad, F.H.; Leong, R.W. Role of Hemostatic Powders in the Management of Lower Gastrointestinal Bleeding: A Review: Hemostatic Agents Lower Intestinal Bleed. J. Gastroenterol. Hepatol. 2018, 33, 1445–1453. [Google Scholar] [CrossRef] [Green Version]
- Barmpatsalou, V.; Dubbelboer, I.R.; Rodler, A.; Jacobson, M.; Karlsson, E.; Pedersen, B.L.; Bergström, C.A.S. Physiological Properties, Composition and Structural Profiling of Porcine Gastrointestinal Mucus. Eur. J. Pharm. Biopharm. 2021, 169, 156–167. [Google Scholar] [CrossRef]
- Sakai, T.; Matsunaga, T.; Yamamoto, Y.; Ito, C.; Yoshida, R.; Suzuki, S.; Sasaki, N.; Shibayama, M.; Chung, U. Design and Fabrication of a High-Strength Hydrogel with Ideally Homogeneous Network Structure from Tetrahedron-like Macromonomers. Macromolecules 2008, 41, 5379–5384. [Google Scholar] [CrossRef]
- Miura, Y.; Tsuji, Y.; Cho, R.; Fujisawa, A.; Fujisawa, M.; Kamata, H.; Yoshikawa, Y.; Yamamichi, N.; Sakai, T.; Koike, K. The Feasibility of a Novel Injectable Hydrogel for Protecting Artificial Gastrointestinal Ulcers after Endoscopic Resection: An Animal Pilot Study. Sci. Rep. 2021, 11, 18508. [Google Scholar] [CrossRef]
- Bu, Y.; Zhang, L.; Liu, J.; Zhang, L.; Li, T.; Shen, H.; Wang, X.; Yang, F.; Tang, P.; Wu, D. Synthesis and Properties of Hemostatic and Bacteria-Responsive in Situ Hydrogels for Emergency Treatment in Critical Situations. ACS Appl. Mater. Interfaces 2016, 8, 12674–12683. [Google Scholar] [CrossRef]
- Yin, X.; Hao, Y.; Lu, Y.; Zhang, D.; Zhao, Y.; Mei, L.; Sui, K.; Zhou, Q.; Hu, J. Bio-Multifunctional Hydrogel Patches for Repairing Full-Thickness Abdominal Wall Defects. Adv. Funct. Mater. 2021, 31, 2105614. [Google Scholar] [CrossRef]
- Wang, W.; Zeng, Z.; Xiang, L.; Liu, C.; Diaz-Dussan, D.; Du, Z.; Asha, A.B.; Yang, W.; Peng, Y.-Y.; Pan, M.; et al. Injectable Self-Healing Hydrogel via Biological Environment-Adaptive Supramolecular Assembly for Gastric Perforation Healing. ACS Nano 2021, 15, 9913–9923. [Google Scholar] [CrossRef]
- Yuk, H.; Varela, C.E.; Nabzdyk, C.S.; Mao, X.; Padera, R.F.; Roche, E.T.; Zhao, X. Dry Double-Sided Tape for Adhesion of Wet Tissues and Devices. Nature 2019, 575, 169–174. [Google Scholar] [CrossRef]
- Nugent, S.G. Intestinal Luminal PH in Inflammatory Bowel Disease: Possible Determinants and Implications for Therapy with Aminosalicylates and Other Drugs. Gut 2001, 48, 571–577. [Google Scholar] [CrossRef] [Green Version]
- He, J.; Zhang, Z.; Yang, Y.; Ren, F.; Li, J.; Zhu, S.; Ma, F.; Wu, R.; Lv, Y.; He, G.; et al. Injectable Self-Healing Adhesive PH-Responsive Hydrogels Accelerate Gastric Hemostasis and Wound Healing. Nano-Micro Lett. 2021, 13, 80. [Google Scholar] [CrossRef]
- Han, W.; Zhou, B.; Yang, K.; Xiong, X.; Luan, S.; Wang, Y.; Xu, Z.; Lei, P.; Luo, Z.; Gao, J.; et al. Biofilm-Inspired Adhesive and Antibacterial Hydrogel with Tough Tissue Integration Performance for Sealing Hemostasis and Wound Healing. Bioact. Mater. 2020, 5, 768–778. [Google Scholar] [CrossRef]
- Nishiguchi, A.; Kurihara, Y.; Taguchi, T. Underwater-Adhesive Microparticle Dressing Composed of Hydrophobically-Modified Alaska Pollock Gelatin for Gastrointestinal Tract Wound Healing. Acta Biomater. 2019, 99, 387–396. [Google Scholar] [CrossRef]
- Liu, H.; Qin, S.; Liu, J.; Zhou, C.; Zhu, Y.; Yuan, Y.; Fu, D.; Lv, Q.; Song, Y.; Zou, M.; et al. Bio-Inspired Self-Hydrophobized Sericin Adhesive with Tough Underwater Adhesion Enables Wound Healing and Fluid Leakage Sealing. Adv. Funct. Mater. 2022, 32, 2201108. [Google Scholar] [CrossRef]
- Shanmugapriya, K.; Kim, H.; Kang, H.W. EGFR-Conjugated Hydrogel Accelerates Wound Healing on Ulcer-Induced Burn Wounds by Targeting Collagen and Inflammatory Cells Using Photoimmunomodulatory Inhibition. Mater. Sci. Eng. C 2021, 118, 111541. [Google Scholar] [CrossRef]
- Araki, T.; Mitsuyama, K.; Yamasaki, H.; Morita, M.; Tsuruta, K.; Mori, A.; Yoshimura, T.; Fukunaga, S.; Kuwaki, K.; Yoshioka, S.; et al. Therapeutic Potential of a Self-Assembling Peptide Hydrogel to Treat Colonic Injuries Associated with Inflammatory Bowel Disease. J. Crohn’s Colitis 2021, 15, 1517–1527. [Google Scholar] [CrossRef] [PubMed]
- Uraoka, T.; Ochiai, Y.; Fujimoto, A.; Goto, O.; Kawahara, Y.; Kobayashi, N.; Kanai, T.; Matsuda, S.; Kitagawa, Y.; Yahagi, N. A Novel Fully Synthetic and Self-Assembled Peptide Solution for Endoscopic Submucosal Dissection-Induced Ulcer in the Stomach. Gastrointest. Endosc. 2016, 83, 1259–1264. [Google Scholar] [CrossRef] [PubMed]
- Parsa, P.; Paydayesh, A.; Davachi, S.M. Investigating the Effect of Tetracycline Addition on Nanocomposite Hydrogels Based on Polyvinyl Alcohol and Chitosan Nanoparticles for Specific Medical Applications. Int. J. Biol. Macromol. 2019, 121, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Yan, D.; Li, Y.; Liu, Y.; Li, N.; Zhang, X.; Yan, C. Antimicrobial Properties of Chitosan and Chitosan Derivatives in the Treatment of Enteric Infections. Molecules 2021, 26, 7136. [Google Scholar] [CrossRef] [PubMed]
- Sigmon, D.F.; Tuma, F.; Kamel, B.G.; Cassaro, S. Gastric Perforation. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Liu, S.; Luan, Z.; Wang, T.; Xu, K.; Luo, Q.; Ye, S.; Wang, W.; Dan, R.; Shu, Z.; Huang, Y.; et al. Endoscopy Deliverable and Mushroom-Cap-Inspired Hyperboloid-Shaped Drug-Laden Bioadhesive Hydrogel for Stomach Perforation Repair. ACS Nano 2022, 17, 111–126. [Google Scholar] [CrossRef]
- Chen, X.; Zhang, J.; Chen, G.; Xue, Y.; Zhang, J.; Liang, X.; Lei, I.M.; Lin, J.; Xu, B.B.; Liu, J. Hydrogel Bioadhesives with Extreme Acid-Tolerance for Gastric Perforation Repairing. Adv. Funct. Mater. 2022, 32, 2202285. [Google Scholar] [CrossRef]
- Chen, J.; Caserto, J.S.; Ang, I.; Shariati, K.; Webb, J.; Wang, B.; Wang, X.; Bouklas, N.; Ma, M. An Adhesive and Resilient Hydrogel for the Sealing and Treatment of Gastric Perforation. Bioact. Mater. 2022, 14, 52–60. [Google Scholar] [CrossRef]
- Coco, D.; Leanza, S. A Review on Treatment of Perforated Peptic Ulcer by Minimally Invasive Techniques. Maedica 2022, 17, 692–698. [Google Scholar] [CrossRef]
- Hafner, J.; Tuma, F.; Hoilat, G.J.; Marar, O. Intestinal Perforation. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Liu, X.; Yang, Y.; Yu, H.; Wang, L.; Sheng, Y.; Huang, Z.; Yang, J.; Ni, Z.; Shen, D. Instant and Tough Adhesives for Rapid Gastric Perforation and Traumatic Pneumothorax Sealing. Adv. Healthc. Mater. 2022, 11, 2201798. [Google Scholar] [CrossRef]
- Yu, J.; Qin, Y.; Yang, Y.; Zhao, X.; Zhang, Z.; Zhang, Q.; Su, Y.; Zhang, Y.; Cheng, Y. Robust Hydrogel Adhesives for Emergency Rescue and Gastric Perforation Repair. Bioact. Mater. 2023, 19, 703–716. [Google Scholar] [CrossRef]
- Peng, X.; Xia, X.; Xu, X.; Yang, X.; Yang, B.; Zhao, P.; Yuan, W.; Chiu, P.W.Y.; Bian, L. Ultrafast Self-Gelling Powder Mediates Robust Wet Adhesion to Promote Healing of Gastrointestinal Perforations. Sci. Adv. 2021, 7, eabe8739. [Google Scholar] [CrossRef]
- Xue, W.; Yang, R.; Liu, S.; Pu, Y.; Wang, P.; Zhang, W.; Tan, X.; Chi, B. Ascidian-Inspired Aciduric Hydrogels with High Stretchability and Adhesiveness Promote Gastric Hemostasis and Wound Healing. Biomater. Sci. 2022, 10, 2417–2427. [Google Scholar] [CrossRef]
- Fan, H.; Wang, J.; Zhang, Q.; Jin, Z. Tannic Acid-Based Multifunctional Hydrogels with Facile Adjustable Adhesion and Cohesion Contributed by Polyphenol Supramolecular Chemistry. ACS Omega 2017, 2, 6668–6676. [Google Scholar] [CrossRef]
- Liu, B.; Wang, Y.; Miao, Y.; Zhang, X.; Fan, Z.; Singh, G.; Zhang, X.; Xu, K.; Li, B.; Hu, Z.; et al. Hydrogen Bonds Autonomously Powered Gelatin Methacrylate Hydrogels with Super-Elasticity, Self-Heal and Underwater Self-Adhesion for Sutureless Skin and Stomach Surgery and E-Skin. Biomaterials 2018, 171, 83–96. [Google Scholar] [CrossRef]
- Fan, H.; Gong, J.P. Bioinspired Underwater Adhesives. Adv. Mater. 2021, 33, 2102983. [Google Scholar] [CrossRef]
- Crosby, C.O.; Stern, B.; Kalkunte, N.; Pedahzur, S.; Ramesh, S.; Zoldan, J. Interpenetrating Polymer Network Hydrogels as Bioactive Scaffolds for Tissue Engineering. Rev. Chem. Eng. 2022, 38, 347–361. [Google Scholar] [CrossRef]
- Dragan, E.S. Advances in Interpenetrating Polymer Network Hydrogels and Their Applications. Pure Appl. Chem. 2014, 86, 1707–1721. [Google Scholar] [CrossRef]
- Bian, S.; Zheng, Z.; Liu, Y.; Ruan, C.; Pan, H.; Zhao, X. A Shear-Thinning Adhesive Hydrogel Reinforced by Photo-Initiated Crosslinking as a Fit-to-Shape Tissue Sealant. J. Mater. Chem. B 2019, 7, 6488–6499. [Google Scholar] [CrossRef]
- Yuan, Y.; Wu, H.; Ren, X.; Wang, J.; Liu, R.; Hu, B.; Gu, N. Dual-Network Hydrogel Based on Ionic Nano-Reservoir for Gastric Perforation Sealing. Sci. China Mater. 2022, 65, 827–835. [Google Scholar] [CrossRef]
- Cheng, Y.; Koh, L.-D.; Li, D.; Ji, B.; Han, M.-Y.; Zhang, Y.-W. On the Strength of β-Sheet Crystallites of Bombyx mori Silk Fibroin. J. R. Soc. Interface 2014, 11, 20140305. [Google Scholar] [CrossRef] [Green Version]
- Cui, C.; Wu, T.; Chen, X.; Liu, Y.; Li, Y.; Xu, Z.; Fan, C.; Liu, W. A Janus Hydrogel Wet Adhesive for Internal Tissue Repair and Anti-Postoperative Adhesion. Adv. Funct. Mater. 2020, 30, 2005689. [Google Scholar] [CrossRef]
- Zhao, T.; Zhao, W.; Chen, Y.; Ahokas, R.A.; Sun, Y. Acidic and Basic Fibroblast Growth Factors Involved in Cardiac Angiogenesis Following Infarction. Int. J. Cardiol. 2011, 152, 307–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, A.H.; Chao, W.; Ecker, M. Review of Colonic Anastomotic Leakage and Prevention Methods. J. Clin. Med. 2020, 9, 4061. [Google Scholar] [CrossRef] [PubMed]
- Guida, A.M.; Leonetti, G.; Finizio, R.; Montagnese, F.; Efrati, C.; Sena, G.; Divizia, A.; Benavoli, D. Endoscopic Solutions for Colorectal Anastomotic Leaks. Tech. Innov. Gastrointest. Endosc. 2022, 24, 57–65. [Google Scholar] [CrossRef]
- Vakalopoulos, K.A.; Daams, F.; Wu, Z.; Timmermans, L.; Jeekel, J.J.; Kleinrensink, G.-J.; van der Ham, A.; Lange, J.F. Tissue Adhesives in Gastrointestinal Anastomosis: A Systematic Review. J. Surg. Res. 2013, 180, 290–300. [Google Scholar] [CrossRef]
- DeStigter, K.; Keating, D. Imaging Update: Acute Colonic Diverticulitis. Clin. Colon Rectal Surg. 2009, 22, 147–155. [Google Scholar] [CrossRef] [Green Version]
- Blumetti, J. Management of Low Colorectal Anastomotic Leak: Preserving the Anastomosis. World J. Gastrointest. Surg. 2015, 7, 378. [Google Scholar] [CrossRef]
- Kern, N.G.; Behrens, A.M.; Srinivasan, P.; Rossi, C.T.; Daristotle, J.L.; Kofinas, P.; Sandler, A.D. Solution Blow Spun Polymer: A Novel Preclinical Surgical Sealant for Bowel Anastomoses. J. Pediatr. Surg. 2017, 52, 1308–1312. [Google Scholar] [CrossRef]
- Hirai, K.; Tabata, Y.; Hasegawa, S.; Sakai, Y. Enhanced Intestinal Anastomotic Healing with Gelatin Hydrogel Incorporating Basic Fibroblast Growth Factor: Enhanced Intestinal Anastomotic Healing with BFGF Release. J. Tissue Eng. Regen. Med. 2016, 10, E433–E442. [Google Scholar] [CrossRef] [Green Version]
- Joo, G.; Sultana, T.; Rahaman, S.; Bae, S.H.; Jung, H.I.; Lee, B.-T. Polycaprolactone-Gelatin Membrane as a Sealant Biomaterial Efficiently Prevents Postoperative Anastomotic Leakage with Promoting Tissue Repair. J. Biomater. Sci. Polym. Ed. 2021, 32, 1530–1547. [Google Scholar] [CrossRef]
- Rosendorf, J.; Klicova, M.; Cervenkova, L.; Palek, R.; Horakova, J.; Klapstova, A.; Hosek, P.; Moulisova, V.; Bednar, L.; Tegl, V.; et al. Double-Layered Nanofibrous Patch for Prevention of Anastomotic Leakage and Peritoneal Adhesions, Experimental Study. In Vivo 2021, 35, 731–741. [Google Scholar] [CrossRef]
- Mizuno, Y.; Watanabe, S.; Taguchi, T. Tissue-Sealing and Anti-Adhesion Properties of an in Situ Hydrogel of Hydrophobically-Modified Alaska Pollock-Derived Gelatin. Int. J. Biol. Macromol. 2020, 163, 2365–2373. [Google Scholar] [CrossRef]
- Qin, J.; Chen, F.; Wu, P.; Sun, G. Recent Advances in Bioengineered Scaffolds for Cutaneous Wound Healing. Front. Bioeng. Biotechnol. 2022, 10, 841583. [Google Scholar] [CrossRef]
- Nosrati, H.; Aramideh Khouy, R.; Nosrati, A.; Khodaei, M.; Banitalebi-Dehkordi, M.; Ashrafi-Dehkordi, K.; Sanami, S.; Alizadeh, Z. Nanocomposite Scaffolds for Accelerating Chronic Wound Healing by Enhancing Angiogenesis. J. Nanobiotechnol. 2021, 19, 1. [Google Scholar] [CrossRef]
- Negut, I.; Dorcioman, G.; Grumezescu, V. Scaffolds for Wound Healing Applications. Polymers 2020, 12, 2010. [Google Scholar] [CrossRef]
- Liu, X.; Xu, H.; Zhang, M.; Yu, D.-G. Electrospun Medicated Nanofibers for Wound Healing: Review. Membranes 2021, 11, 770. [Google Scholar] [CrossRef]
- Dorkhani, E.; Noorafkan, Y.; Asbagh, R.A.; Okhovat, M.; Heirani-Tabasi, A.; Ahmadi Tafti, S.M. Design and Fabrication of Modified Bi-Layer Poly Vinyl Alcohol Adhesive Sealant Film for Preventing Gastrointestinal Leakage. Front. Surg. 2022, 9, 1018590. [Google Scholar] [CrossRef]
- Paonessa, S.; Barbani, N.; Rocchietti, E.C.; Giachino, C.; Cristallini, C. Design and Development of a Hybrid Bioartificial Water-Induced Shape Memory Polymeric Material as an Integral Component for the Anastomosis of Human Hollow Organs. Mater. Sci. Eng. C 2017, 75, 1427–1434. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Jiang, Y.; Liu, Y.; Ren, Y.; Xu, Z.; Li, Z.; Zhao, Y.; Wu, X.; Ren, J. Marine-Inspired Molecular Mimicry Generates a Drug-Free, but Immunogenic Hydrogel Adhesive Protecting Surgical Anastomosis. Bioact. Mater. 2021, 6, 770–782. [Google Scholar] [CrossRef]
- Anthis, A.H.C.; Abundo, M.P.; Neuer, A.L.; Tsolaki, E.; Rosendorf, J.; Rduch, T.; Starsich, F.H.L.; Weisse, B.; Liska, V.; Schlegel, A.A.; et al. Modular Stimuli-Responsive Hydrogel Sealants for Early Gastrointestinal Leak Detection and Containment. Nat. Commun. 2022, 13, 7311. [Google Scholar] [CrossRef]
- Meyer, G.; Lang, R.; Prodinger, P.; Stier, C. Grundlagen und Biologie der Anastomosenheilung. Viszeralchirurgie 2007, 42, 134–144. [Google Scholar] [CrossRef]
- Ustek, S.; Kismet, K.; Akkus, M.A.; Ozcan, A.H.; Aydogan, A.; Renda, N. Effect of Povidone-Iodine Liposome Hydrogel on Colonic Anastomosis. Eur. Surg. Res. 2005, 37, 242–245. [Google Scholar] [CrossRef] [PubMed]
- Thornton, F.J.; Barbul, A. Healing in the Gastrointestinal Tract. Surg. Clin. N. Am. 1997, 77, 549–573. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Guan, P.; Wen, C.; Lu, M.; Li, T.; Fan, L.; Yang, Q.; Guan, Y.; Kang, X.; Jiang, Y.; et al. Strong Biopolymer-Based Nanocomposite Hydrogel Adhesives with Removability and Reusability for Damaged Tissue Closure and Healing. ACS Appl. Mater. Interfaces 2022, 14, 54488–54499. [Google Scholar] [CrossRef] [PubMed]
- Liakakos, T.; Thomakos, N.; Fine, P.M.; Dervenis, C.; Young, R.L. Peritoneal Adhesions: Etiology, Pathophysiology, and Clinical Significance. Dig. Surg. 2001, 18, 260–273. [Google Scholar] [CrossRef]
- Tang, J.; Xiang, Z.; Bernards, M.T.; Chen, S. Peritoneal Adhesions: Occurrence, Prevention and Experimental Models. Acta Biomater. 2020, 116, 84–104. [Google Scholar] [CrossRef]
- Jeon, E.Y.; Lee, J.; Kim, B.J.; Joo, K.I.; Kim, K.H.; Lim, G.; Cha, H.J. Bio-Inspired Swellable Hydrogel-Forming Double-Layered Adhesive Microneedle Protein Patch for Regenerative Internal/External Surgical Closure. Biomaterials 2019, 222, 119439. [Google Scholar] [CrossRef]
- Bosmans, J.W.A.M.; Moossdorff, M.; Al-Taher, M.; van Beek, L.; Derikx, J.P.M.; Bouvy, N.D. International Consensus Statement Regarding the Use of Animal Models for Research on Anastomoses in the Lower Gastrointestinal Tract. Int. J. Color. Dis. 2016, 31, 1021–1030. [Google Scholar] [CrossRef] [Green Version]
- Marland, J.; Gray, M.; Argyle, D.; Underwood, I.; Murray, A.; Potter, M. Post-Operative Monitoring of Intestinal Tissue Oxygenation Using an Implantable Microfabricated Oxygen Sensor. Micromachines 2021, 12, 810. [Google Scholar] [CrossRef]
- Bosmans, J.W.A.M.; Jongen, A.C.H.M.; Bouvy, N.D.; Derikx, J.P.M. Colorectal Anastomotic Healing: Why the Biological Processes That Lead to Anastomotic Leakage Should Be Revealed Prior to Conducting Intervention Studies. BMC Gastroenterol. 2015, 15, 180. [Google Scholar] [CrossRef] [Green Version]
- Digestive Diseases Statistics for the United States. Available online: https://www.niddk.nih.gov/health-information/health-statistics/digestive-diseases (accessed on 15 February 2023).





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, X.; Grinstaff, M.W. Advances in Hydrogel Adhesives for Gastrointestinal Wound Closure and Repair. Gels 2023, 9, 282. https://doi.org/10.3390/gels9040282
Hu X, Grinstaff MW. Advances in Hydrogel Adhesives for Gastrointestinal Wound Closure and Repair. Gels. 2023; 9(4):282. https://doi.org/10.3390/gels9040282
Chicago/Turabian StyleHu, Xingyu, and Mark W. Grinstaff. 2023. "Advances in Hydrogel Adhesives for Gastrointestinal Wound Closure and Repair" Gels 9, no. 4: 282. https://doi.org/10.3390/gels9040282