
Diagnosis and Treatment of Invasive Aspergillosis Caused by Non-fumigatus Aspergillus spp.
 , , , and
, , , and
Abstract
:1. Introduction
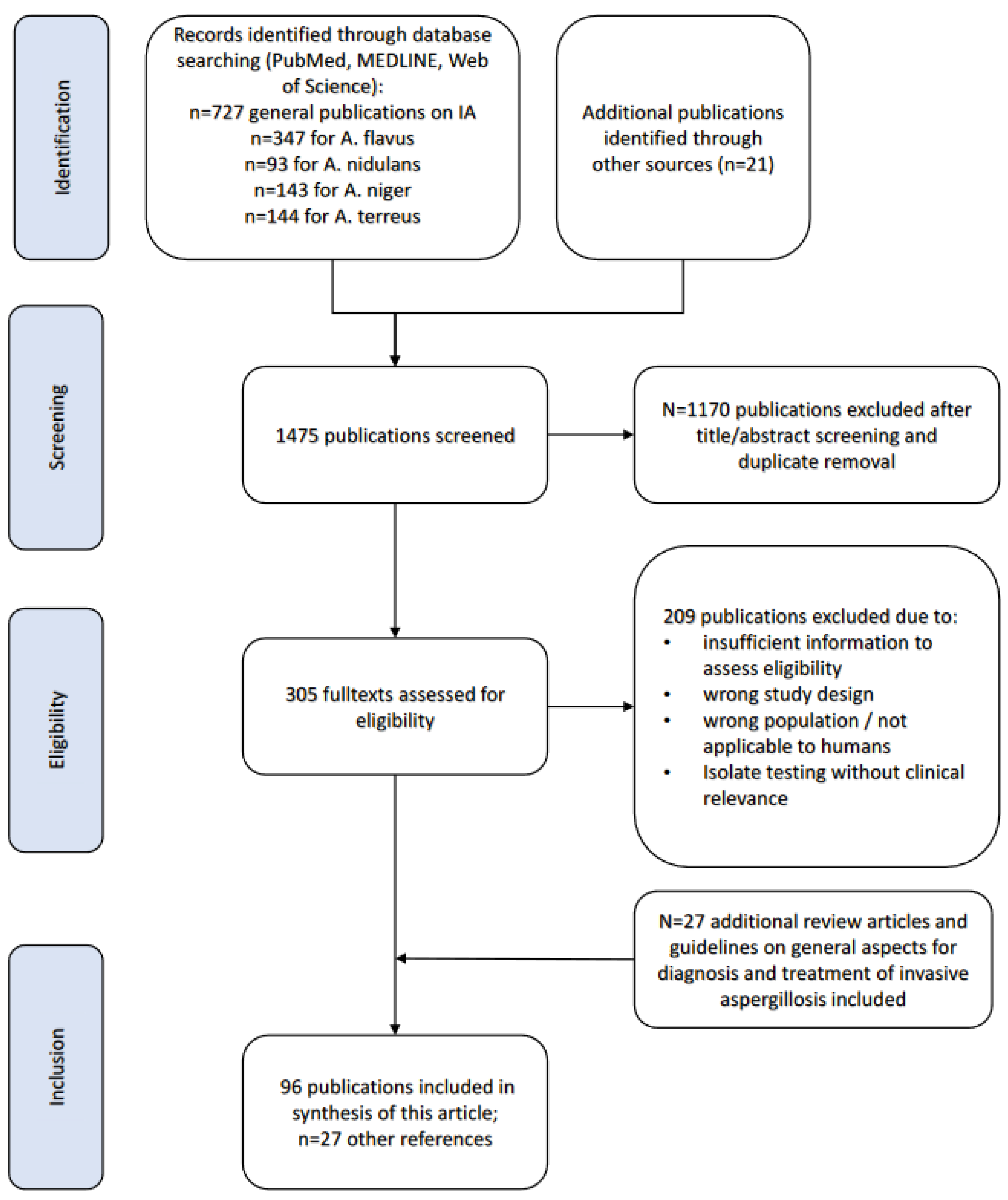
2. Methods
3. Results
General Aspects

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A. fumigatus | A. flavus | A. nidulans | A. niger | A. terreus | |
|---|---|---|---|---|---|
| Phylogeny—Subgenus and Section | Fumigati Fumigati | Circumdati Flavi | Nidulantes Nidulantes | Circumdati Nigri | Circumdati Terrei |
| Environmental sources | Ubiquitous in the environment, construction work, dust, soil, compost | Ubiquitous in the environment; also identified in compost | Ubiquitous in the environment | Ubiquitous in the environment | Ubiquitous in the environment; compost, soil, construction work, dust |
| Epidemiology | Worldwide identification | Higher incidence in warm, arid climate zones (tropical and subtropical climate zones) | Worldwide identification | Worldwide identification | More often identified in Austria, Israel, Spain and Texas, USA |
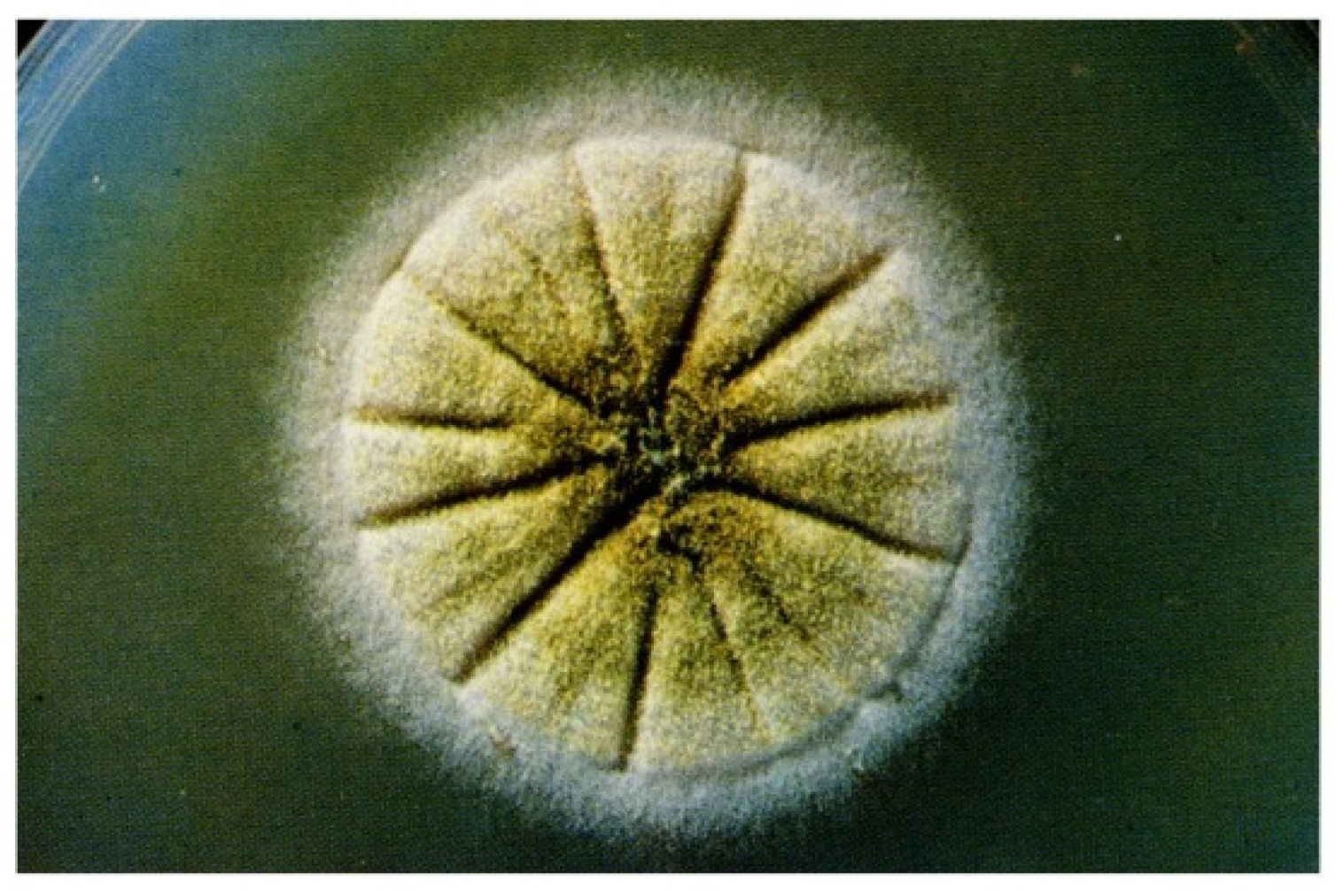
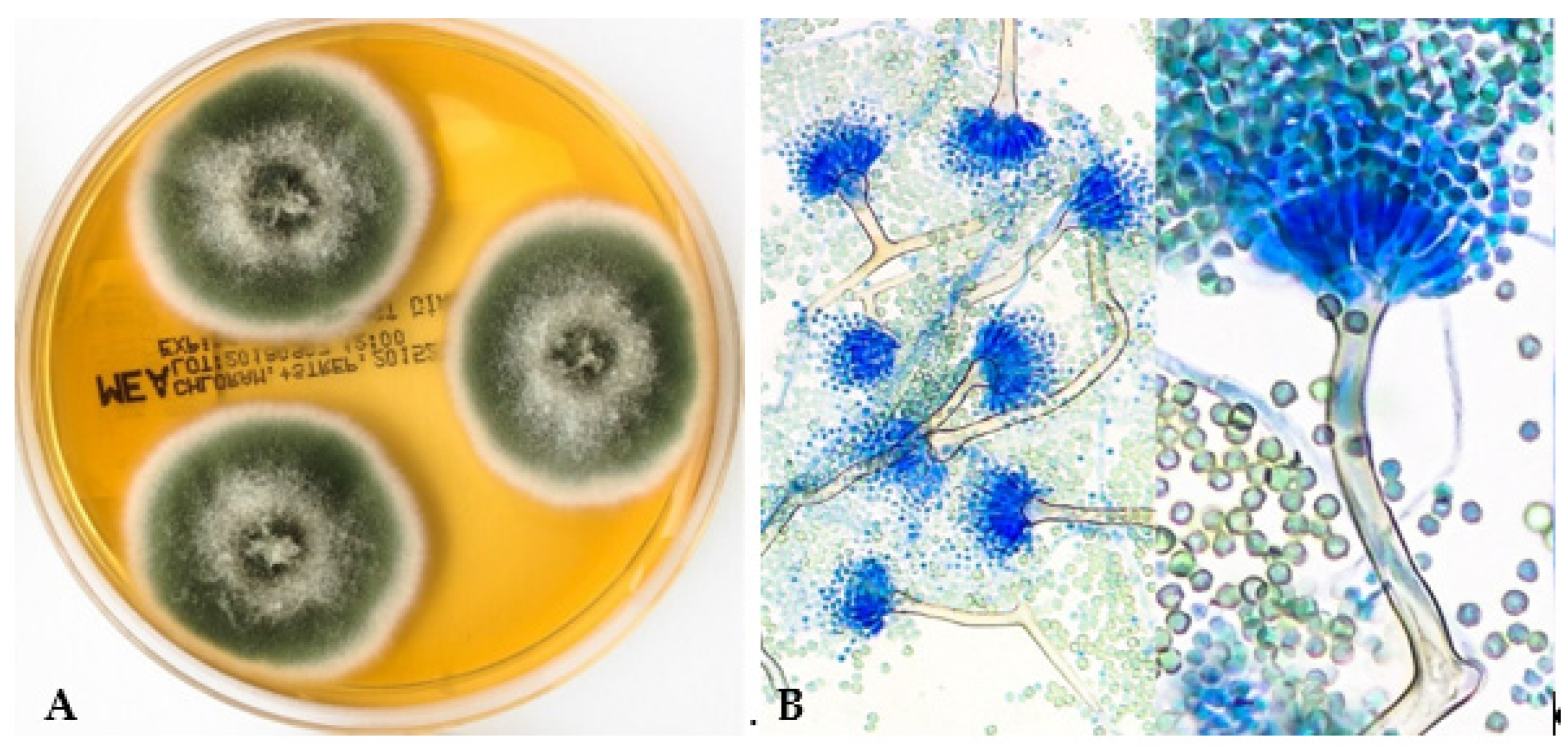
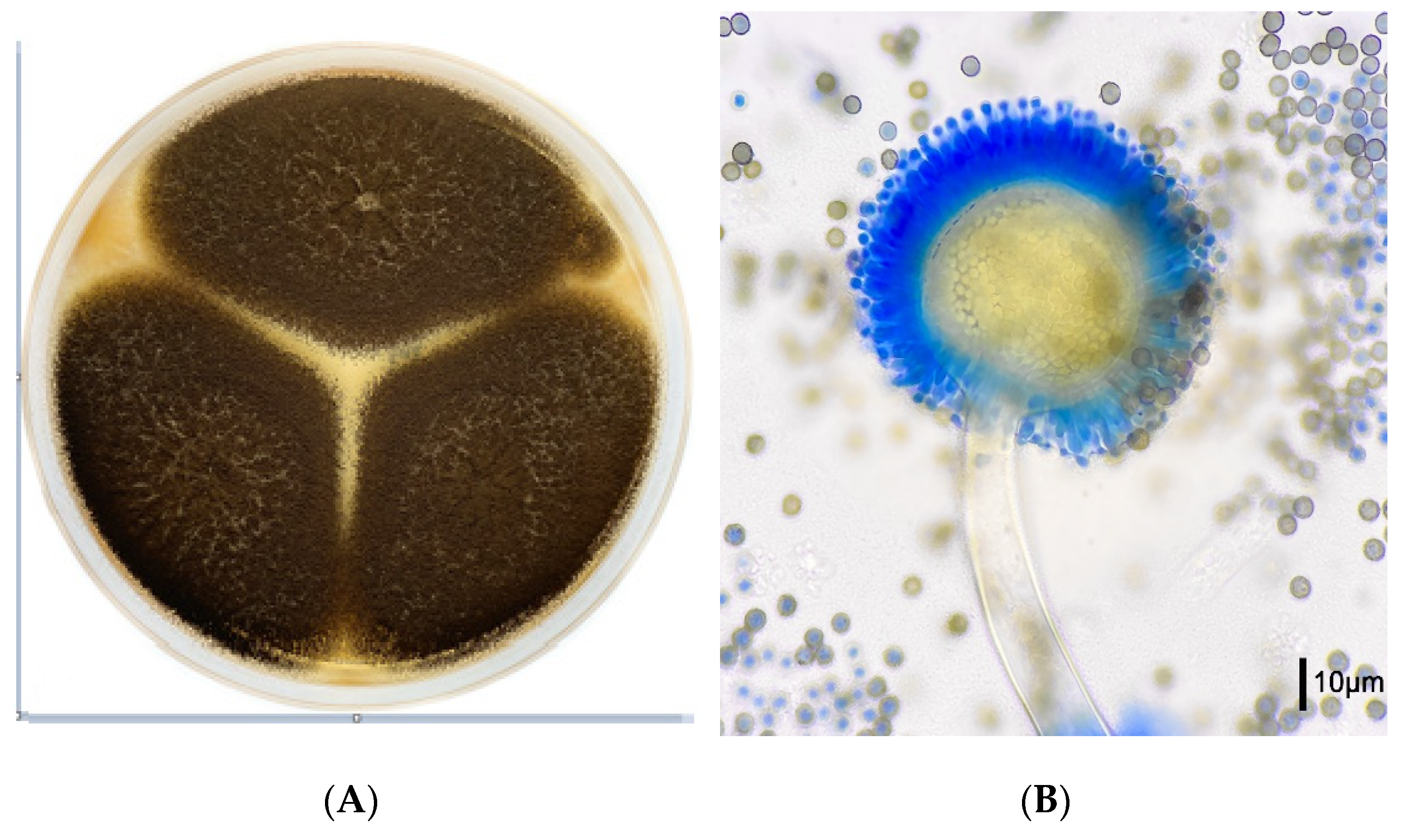
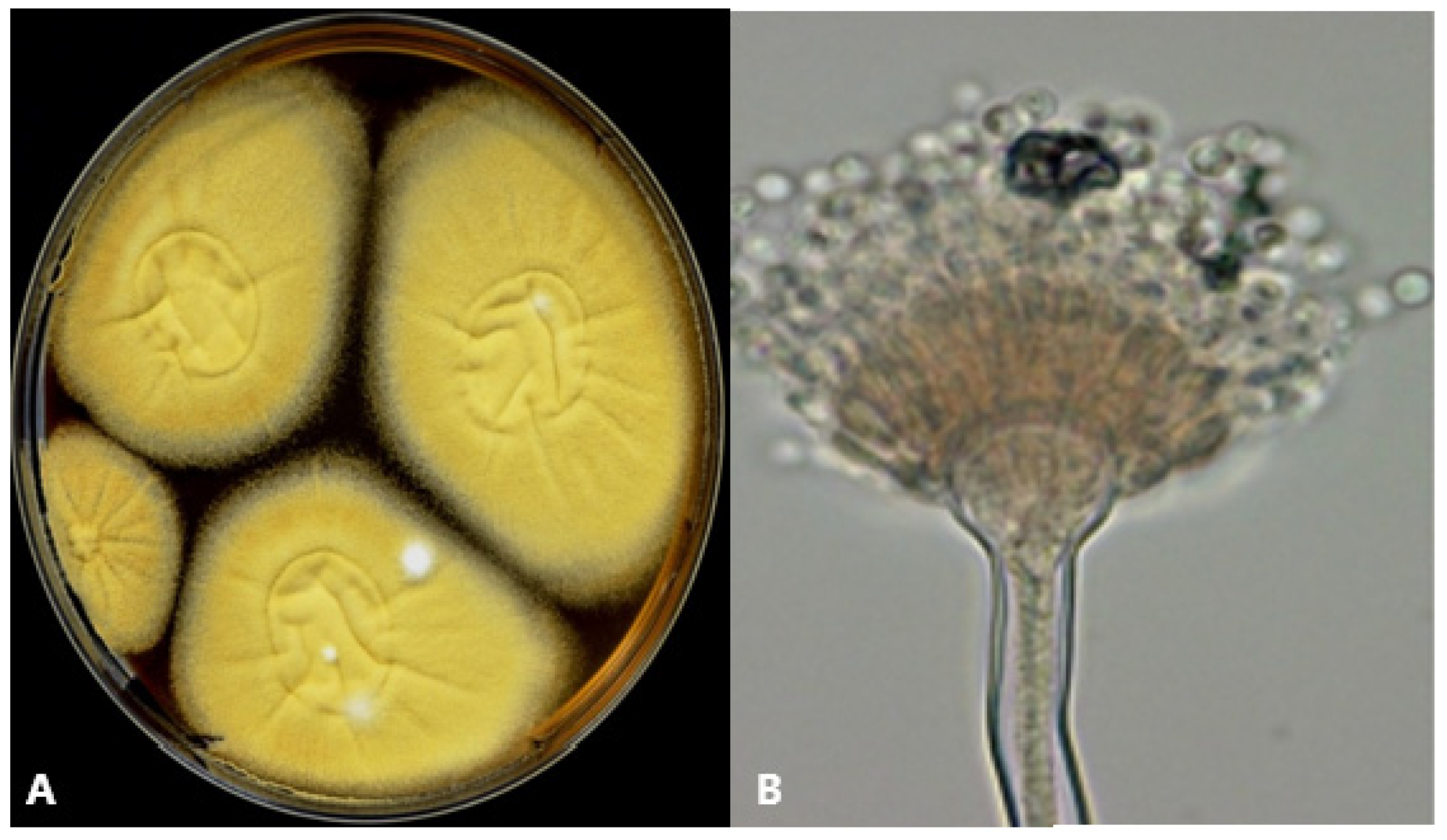
| Morphology | |||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Microbiological test peculiarities | Microscopy, culture, PCR, Galactomannan in BAL or serum; Hypersensitivity tests for ABPA | Microscopy, culture, PCR, Galactomannan in BAL or serum (reduced sensitivity) | Microscopy, culture, PCR, Galactomannan in serum or BAL; | Microscopy, culture, PCR, Galactomannan in serum or BAL; | Microscopy, culture, PCR, Galactomannan in serum or BAL; |
| Disease entities | IPA, sinusitis and cerebral IA; chronic aspergillosis including aspergilloma; allergic bronchopulmonary aspergillosis | IPA, sinusitis, otomycosis, cutaneous IA; osteomyelitis; rarely aflatoxin-induced diseases | IPA, osteomyelitis | IPA, superficial infections in chronically ill patients: otomycosis, sinusitis | IPA, Higher rate of disseminated disease reported |
| Main risk factors for IFI | Long-term neutropenia (acute leukemias, HSCT), GvHD, SOT, ICU patients with viral pneumonia (CAPA, IAPA) | Long-term neutropenia (acute leukemias, HSCT), SOT, Trauma, diabetes | Neutropenia, CGD | Long-term neutropenia (acute leukemias, HSCT), SOT; frequently identified colonizer in immunocompetent individuals | Neutropenia, HSCT, liver transplant |
| Treatment until susceptibility test results available | Triazoles (isavuconazole, posaconazole, voriconazole), (liposomal) AmB | Triazoles (isavuconazole, posaconazole, voriconazole), consider combination therapy | Voriconazole | Avoid azole monotherapy; consider combination with (liposomal) AmB | Triazoles (isavuconazole, posaconazole, voriconazole) |
| Peculiarities in treatment (according to MIC) | Azole resistance in Europe increasing | Sometimes reduced susceptibility for AmB (≥4 mg/L); if MIC ≥2 mg/L combination treatment with echinocandins suggested | Reduced susceptibility for AmB (published MICs between ≥1 mg and 4 mg/mL), innate resistance to AmB suggested | Commonly reported elevated MICs of azoles compared to A. fumigatus (2 µg/mL, 1 µg/mL, 4 µg/mL, and 1 µg/mL for AmB, isavuconazole, itraconazole, and voriconazole, respectively), lower MIC for posaconazole (0.5 µg/mL) and caspofungin (0.25 µg/mL) (CLSI) [57]; if available use other azoles than itraconazole or isavuconazole | Avoid AmB (most species with intrinsic resistance and MIC >2 mg/L) |
4. A. flavus
4.1. General Characteristics and Epidemiology
4.2. Diagnosis and Microbiology
4.3. Clinical Management and Treatment
5. A. nidulans
5.1. General Characteristics and Epidemiology
5.2. Diagnosis and Microbiology
5.3. Clinical Management and Treatment
6. A. niger
6.1. General Characteristics and Epidemiology
6.2. Diagnosis and Microbiology
6.3. Clinical Management and Treatment
7. A. terreus
7.1. General Characteristics and Epidemiology
7.2. Diagnosis and Microbiology
7.3. Clinical Management and Treatment
8. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Buil, J.B.; Snelders, E.; Denardi, L.B.; Melchers, W.J.G.; Verweij, P.E. Trends in Azole Resistance in Aspergillus fumigatus, the Netherlands, 1994–2016. Emerg. Infect. Dis. 2019, 25, 176–178. [Google Scholar] [CrossRef] [PubMed]
- Friedman, D.Z.P.; Schwartz, I.S. Emerging Fungal Infections: New Patients, New Patterns, and New Pathogens. J. Fungi 2019, 5, 67. [Google Scholar] [CrossRef] [PubMed]
- Koehler, P.; Stecher, M.; Cornely, O.A.; Koehler, D.; Vehreschild, M.; Bohlius, J.; Wisplinghoff, H.; Vehreschild, J.J. Morbidity and mortality of candidaemia in Europe: An epidemiologic meta-analysis. Clin. Microbiol. Infect. 2019, 25, 1200–1212. [Google Scholar] [CrossRef] [PubMed]
- Kohlenberg, A.; Struelens, M.J.; Monnet, D.L.; Plachouras, D. Candida auris: Epidemiological situation, laboratory capacity and preparedness in European Union and European Economic Area countries, 2013 to 2017. Eur. Surveill. 2018, 23. [Google Scholar] [CrossRef] [PubMed]
- Kontoyiannis, D.P.; Marr, K.A.; Park, B.J.; Alexander, B.D.; Anaissie, E.J.; Walsh, T.J.; Ito, J.; Andes, D.R.; Baddley, J.W.; Brown, J.M.; et al. Prospective surveillance for invasive fungal infections in hematopoietic stem cell transplant recipients, 2001–2006: Overview of the Transplant-Associated Infection Surveillance Network (TRANSNET) Database. Clin. Infect. Dis. 2010, 50, 1091–1100. [Google Scholar] [CrossRef]
- Latgé, J.P.; Chamilos, G. Aspergillus fumigatus and Aspergillosis in 2019. Clin. Microbiol. Rev. 2019, 33, e00140-18. [Google Scholar] [CrossRef]
- Pappas, P.G.; Alexander, B.D.; Andes, D.R.; Hadley, S.; Kauffman, C.A.; Freifeld, A.; Anaissie, E.J.; Brumble, L.M.; Herwaldt, L.; Ito, J.; et al. Invasive fungal infections among organ transplant recipients: Results of the Transplant-Associated Infection Surveillance Network (TRANSNET). Clin. Infect. Dis. 2010, 50, 1101–1111. [Google Scholar] [CrossRef]
- Steinbach, W.J.; Marr, K.A.; Anaissie, E.J.; Azie, N.; Quan, S.P.; Meier-Kriesche, H.U.; Apewokin, S.; Horn, D.L. Clinical epidemiology of 960 patients with invasive aspergillosis from the PATH Alliance registry. J. Infect. 2012, 65, 453–464. [Google Scholar] [CrossRef]
- Sacks, D.; Baxter, B.; Campbell, B.C.V.; Carpenter, J.S.; Cognard, C.; Dippel, D.; Eesa, M.; Fischer, U.; Hausegger, K.; Hirsch, J.A.; et al. Multisociety Consensus Quality Improvement Revised Consensus Statement for Endovascular Therapy of Acute Ischemic Stroke. Int. J. Stroke 2018, 13, 612–632. [Google Scholar] [CrossRef]
- Ragozzino, S.; Goldenberger, D.; Wright, P.R.; Zimmerli, S.; Mühlethaler, K.; Neofytos, D.; Riat, A.; Boggian, K.; Nolte, O.; Conen, A.; et al. Distribution of Aspergillus Species and Prevalence of Azole Resistance in Respiratory Samples From Swiss Tertiary Care Hospitals. Open Forum Infect. Dis. 2022, 9, ofab638. [Google Scholar] [CrossRef]
- Lamoth, F.; Chung, S.J.; Damonti, L.; Alexander, B.D. Changing Epidemiology of Invasive Mold Infections in Patients Receiving Azole Prophylaxis. Clin. Infect. Dis. 2017, 64, 1619–1621. [Google Scholar] [CrossRef] [PubMed]
- Zanganeh, E.; Zarrinfar, H.; Rezaeetalab, F.; Fata, A.; Tohidi, M.; Najafzadeh, M.J.; Alizadeh, M.; Seyedmousavi, S. Predominance of non-fumigatus Aspergillus species among patients suspected to pulmonary aspergillosis in a tropical and subtropical region of the Middle East. Microb. Pathog. 2018, 116, 296–300. [Google Scholar] [CrossRef] [PubMed]
- Thompson, G.R., 3rd; Young, J.H. Aspergillus Infections. N. Engl. J. Med. 2021, 385, 1496–1509. [Google Scholar] [CrossRef] [PubMed]
- Koehler, P.; Bassetti, M.; Chakrabarti, A.; Chen, S.C.A.; Colombo, A.L.; Hoenigl, M.; Klimko, N.; Lass-Flörl, C.; Oladele, R.O.; Vinh, D.C.; et al. Defining and managing COVID-19-associated pulmonary aspergillosis: The 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect. Dis. 2021, 21, e149–e162. [Google Scholar] [CrossRef] [PubMed]
- Cornely, O.A.; Maertens, J.; Winston, D.J.; Perfect, J.; Ullmann, A.J.; Walsh, T.J.; Helfgott, D.; Holowiecki, J.; Stockelberg, D.; Goh, Y.T.; et al. Posaconazole vs. fluconazole or itraconazole prophylaxis in patients with neutropenia. N. Engl. J. Med. 2007, 356, 348–359. [Google Scholar] [CrossRef]
- Mellinghoff, S.C.; Panse, J.; Alakel, N.; Behre, G.; Buchheidt, D.; Christopeit, M.; Hasenkamp, J.; Kiehl, M.; Koldehoff, M.; Krause, S.W.; et al. Primary prophylaxis of invasive fungal infections in patients with haematological malignancies: 2017 update of the recommendations of the Infectious Diseases Working Party (AGIHO) of the German Society for Haematology and Medical Oncology (DGHO). Ann. Hematol. 2018, 97, 197–207. [Google Scholar] [CrossRef]
- Lass-Flörl, C. How to make a fast diagnosis in invasive aspergillosis. Med. Mycol. 2019, 57, S155–S160. [Google Scholar] [CrossRef]
- Park, S.Y.; Kim, S.H.; Choi, S.H.; Sung, H.; Kim, M.N.; Woo, J.H.; Kim, Y.S.; Park, S.K.; Lee, J.H.; Lee, K.H.; et al. Clinical and radiological features of invasive pulmonary aspergillosis in transplant recipients and neutropenic patients. Transpl. Infect. Dis. 2010, 12, 309–315. [Google Scholar] [CrossRef]
- Bitterman, R.; Hardak, E.; Raines, M.; Stern, A.; Zuckerman, T.; Ofran, Y.; Lavi, N.; Guralnik, L.; Frisch, A.; Nudelman, O.; et al. Baseline Chest Computed Tomography for Early Diagnosis of Invasive Pulmonary Aspergillosis in Hemato-oncological Patients: A Prospective Cohort Study. Clin. Infect. Dis. 2019, 69, 1805–1808. [Google Scholar] [CrossRef]
- Ceesay, M.M.; Desai, S.R.; Berry, L.; Cleverley, J.; Kibbler, C.C.; Pomplun, S.; Nicholson, A.G.; Douiri, A.; Wade, J.; Smith, M.; et al. A comprehensive diagnostic approach using galactomannan, targeted β-d-glucan, baseline computerized tomography and biopsy yields a significant burden of invasive fungal disease in at risk haematology patients. Br. J. Haematol. 2015, 168, 219–229. [Google Scholar] [CrossRef]
- Stemler, J.; Bruns, C.; Mellinghoff, S.C.; Alakel, N.; Akan, H.; Ananda-Rajah, M.; Auberger, J.; Bojko, P.; Chandrasekar, P.H.; Chayakulkeeree, M.; et al. Baseline Chest Computed Tomography as Standard of Care in High-Risk Hematology Patients. J. Fungi 2020, 6. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.Y.; Sheng, W.H.; Cheng, A.; Chen, Y.C.; Tsay, W.; Tang, J.L.; Huang, S.Y.; Chang, S.C.; Tien, H.F. Invasive fungal sinusitis in patients with hematological malignancy: 15 years experience in a single university hospital in Taiwan. BMC Infect. Dis. 2011, 11, 250. [Google Scholar] [CrossRef] [PubMed]
- Lass-Flörl, C.; Samardzic, E.; Knoll, M. Serology anno 2021-fungal infections: From invasive to chronic. Clin. Microbiol. Infect. 2021, 27, 1230–1241. [Google Scholar] [CrossRef] [PubMed]
- Springer, J.; Lackner, M.; Nachbaur, D.; Girschikofsky, M.; Risslegger, B.; Mutschlechner, W.; Fritz, J.; Heinz, W.J.; Einsele, H.; Ullmann, A.J.; et al. Prospective multicentre PCR-based Aspergillus DNA screening in high-risk patients with and without primary antifungal mould prophylaxis. Clin. Microbiol. Infect. 2016, 22, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Woo, P.C.; Chan, C.M.; Leung, A.S.; Lau, S.K.; Che, X.Y.; Wong, S.S.; Cao, L.; Yuen, K.Y. Detection of cell wall galactomannoprotein Afmp1p in culture supernatants of Aspergillus fumigatus and in sera of aspergillosis patients. J. Clin. Microbiol. 2002, 40, 4382–4387. [Google Scholar] [CrossRef] [PubMed]
- Pazos, C.; Pontón, J.; Del Palacio, A. Contribution of (1->3)-beta-D-glucan chromogenic assay to diagnosis and therapeutic monitoring of invasive aspergillosis in neutropenic adult patients: A comparison with serial screening for circulating galactomannan. J. Clin. Microbiol. 2005, 43, 299–305. [Google Scholar] [CrossRef]
- Boch, T.; Spiess, B.; Cornely, O.A.; Vehreschild, J.J.; Rath, P.M.; Steinmann, J.; Heinz, W.J.; Hahn, J.; Krause, S.W.; Kiehl, M.G.; et al. Diagnosis of invasive fungal infections in haematological patients by combined use of galactomannan, 1,3-β-D-glucan, Aspergillus PCR, multifungal DNA-microarray, and Aspergillus azole resistance PCRs in blood and bronchoalveolar lavage samples: Results of a prospective multicentre study. Clin. Microbiol. Infect. 2016, 22, 862–868. [Google Scholar] [CrossRef]
- Hoog, J.G.; Guarro, J.; Gené, J.; Ahmed, S.; Al-Hatmi, A.M.S.; Figueras, M.J.; Vitale, R.G. Atlas of Clinical Fungi 2019, 3rd ed.; Reus: Utrecht, The Netherlands, 2019. [Google Scholar]
- McClenny, N. Laboratory detection and identification of Aspergillus species by microscopic observation and culture: The traditional approach. Med. Mycol. 2005, 43, S125–S128. [Google Scholar] [CrossRef]
- Buess, M.; Cathomas, G.; Halter, J.; Junker, L.; Grendelmeier, P.; Tamm, M.; Stolz, D. Aspergillus-PCR in bronchoalveolar lavage for detection of invasive pulmonary aspergillosis in immunocompromised patients. BMC Infect. Dis. 2012, 12, 237. [Google Scholar] [CrossRef]
- Howard, S.J. Multi-resistant aspergillosis due to cryptic species. Mycopathologia 2014, 178, 435–439. [Google Scholar] [CrossRef]
- Florent, M.; Katsahian, S.; Vekhoff, A.; Levy, V.; Rio, B.; Marie, J.P.; Bouvet, A.; Cornet, M. Prospective evaluation of a polymerase chain reaction-ELISA targeted to Aspergillus fumigatus and Aspergillus flavus for the early diagnosis of invasive aspergillosis in patients with hematological malignancies. J. Infect. Dis. 2006, 193, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Alanio, A.; Beretti, J.L.; Dauphin, B.; Mellado, E.; Quesne, G.; Lacroix, C.; Amara, A.; Berche, P.; Nassif, X.; Bougnoux, M.E. Matrix-assisted laser desorption ionization time-of-flight mass spectrometry for fast and accurate identification of clinically relevant Aspergillus species. Clin. Microbiol. Infect. 2011, 17, 750–755. [Google Scholar] [CrossRef] [PubMed]
- Cassagne, C.; Normand, A.C.; L’Ollivier, C.; Ranque, S.; Piarroux, R. Performance of MALDI-TOF MS platforms for fungal identification. Mycoses 2016, 59, 678–690. [Google Scholar] [CrossRef] [PubMed]
- Espinel-Ingroff, A.; Cuenca-Estrella, M.; Cantón, E. EUCAST and CLSI: Working Together Towards a Harmonized Method for Antifungal Susceptibility Testing. Curr. Fungal Infect. Rep. 2013, 7, 59–67. [Google Scholar] [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs for Antifungal Agents. 2020. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/AFST/Clinical_breakpoints/AFST_BP_v10.0_200204_updatd_links_200924.pdf. (accessed on 4 March 2023).
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef]
- Krishnan, S.; Manavathu, E.K.; Chandrasekar, P.H. Aspergillus flavus: An emerging non-fumigatus Aspergillus species of significance. Mycoses 2009, 52, 206–222. [Google Scholar] [CrossRef]
- Patterson, T.F.; Thompson, G.R., III; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, e1–e60. [Google Scholar] [CrossRef]
- Ruhnke, M.; Cornely, O.A.; Schmidt-Hieber, M.; Alakel, N.; Boell, B.; Buchheidt, D.; Christopeit, M.; Hasenkamp, J.; Heinz, W.J.; Hentrich, M.; et al. Treatment of invasive fungal diseases in cancer patients-Revised 2019 Recommendations of the Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Oncology (DGHO). Mycoses 2020, 63, 653–682. [Google Scholar] [CrossRef]
- Tissot, F.; Agrawal, S.; Pagano, L.; Petrikkos, G.; Groll, A.H.; Skiada, A.; Lass-Flörl, C.; Calandra, T.; Viscoli, C.; Herbrecht, R. ECIL-6 guidelines for the treatment of invasive candidiasis, aspergillosis and mucormycosis in leukemia and hematopoietic stem cell transplant patients. Haematologica 2017, 102, 433–444. [Google Scholar] [CrossRef]
- Ullmann, A.J.; Aguado, J.M.; Arikan-Akdagli, S.; Denning, D.W.; Groll, A.H.; Lagrou, K.; Lass-Flörl, C.; Lewis, R.E.; Munoz, P.; Verweij, P.E.; et al. Diagnosis and management of Aspergillus diseases: Executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin. Microbiol. Infect. 2018, 24 (Suppl. S1), e1–e38. [Google Scholar] [CrossRef]
- Herbrecht, R.; Denning, D.W.; Patterson, T.F.; Bennett, J.E.; Greene, R.E.; Oestmann, J.W.; Kern, W.V.; Marr, K.A.; Ribaud, P.; Lortholary, O.; et al. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N. Engl. J. Med. 2002, 347, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Maertens, J.A.; Raad, I.I.; Marr, K.A.; Patterson, T.F.; Kontoyiannis, D.P.; Cornely, O.A.; Bow, E.J.; Rahav, G.; Neofytos, D.; Aoun, M.; et al. Isavuconazole versus voriconazole for primary treatment of invasive mould disease caused by Aspergillus and other filamentous fungi (SECURE): A phase 3, randomised-controlled, non-inferiority trial. Lancet 2016, 387, 760–769. [Google Scholar] [CrossRef] [PubMed]
- Maertens, J.A.; Rahav, G.; Lee, D.G.; Ponce-de-León, A.; Ramírez Sánchez, I.C.; Klimko, N.; Sonet, A.; Haider, S.; Diego Vélez, J.; Raad, I.; et al. Posaconazole versus voriconazole for primary treatment of invasive aspergillosis: A phase 3, randomised, controlled, non-inferiority trial. Lancet 2021, 397, 499–509. [Google Scholar] [CrossRef] [PubMed]
- Ellis, M.; Spence, D.; de Pauw, B.; Meunier, F.; Marinus, A.; Collette, L.; Sylvester, R.; Meis, J.; Boogaerts, M.; Selleslag, D.; et al. An EORTC international multicenter randomized trial (EORTC number 19923) comparing two dosages of liposomal amphotericin B for treatment of invasive aspergillosis. Clin. Infect. Dis. 1998, 27, 1406–1412. [Google Scholar] [CrossRef]
- Walsh, T.J.; Pappas, P.; Winston, D.J.; Lazarus, H.M.; Petersen, F.; Raffalli, J.; Yanovich, S.; Stiff, P.; Greenberg, R.; Donowitz, G.; et al. Voriconazole compared with liposomal amphotericin B for empirical antifungal therapy in patients with neutropenia and persistent fever. N. Engl. J. Med. 2002, 346, 225–234. [Google Scholar] [CrossRef]
- Maertens, J.; Raad, I.; Petrikkos, G.; Boogaerts, M.; Selleslag, D.; Petersen, F.B.; Sable, C.A.; Kartsonis, N.A.; Ngai, A.; Taylor, A.; et al. Efficacy and Safety of Caspofungin for Treatment of Invasive Aspergillosis in Patients Refractory to or Intolerant of Conventional Antifungal Therapy. Clin. Infect. Dis. 2004, 39, 1563–1571. [Google Scholar] [CrossRef]
- Marr, K.A.; Schlamm, H.T.; Herbrecht, R.; Rottinghaus, S.T.; Bow, E.J.; Cornely, O.A.; Heinz, W.J.; Jagannatha, S.; Koh, L.P.; Kontoyiannis, D.P.; et al. Combination Antifungal Therapy for Invasive Aspergillosis. Ann. Intern. Med. 2015, 162, 81–89. [Google Scholar] [CrossRef]
- Singh, N.; Limaye, A.P.; Forrest, G.; Safdar, N.; Muñoz, P.; Pursell, K.; Houston, S.; Rosso, F.; Montoya, J.G.; Patton, P.; et al. Combination of voriconazole and caspofungin as primary therapy for invasive aspergillosis in solid organ transplant recipients: A prospective, multicenter, observational study. Transplantation 2006, 81, 320–326. [Google Scholar] [CrossRef]
- Barchiesi, F.; Spreghini, E.; Sanguinetti, M.; Giannini, D.; Manso, E.; Castelli, P.; Girmenia, C. Effects of amphotericin B on Aspergillus flavus clinical isolates with variable susceptibilities to the polyene in an experimental model of systemic aspergillosis. J. Antimicrob. Chemother. 2013, 68, 2587–2591. [Google Scholar] [CrossRef]
- Hadrich, I.; Makni, F.; Neji, S.; Cheikhrouhou, F.; Bellaaj, H.; Elloumi, M.; Ayadi, A.; Ranque, S. Amphotericin B in vitro resistance is associated with fatal Aspergillus flavus infection. Med. Mycol. 2012, 50, 829–834. [Google Scholar] [CrossRef]
- Lionakis, M.S.; Lewis, R.E.; Chamilos, G.; Kontoyiannis, D.P. Aspergillus susceptibility testing in patients with cancer and invasive aspergillosis: Difficulties in establishing correlation between in vitro susceptibility data and the outcome of initial amphotericin B therapy. Pharmacotherapy 2005, 25, 1174–1180. [Google Scholar] [CrossRef] [PubMed]
- Mosquera, J.; Warn, P.A.; Morrissey, J.; Moore, C.B.; Gil-Lamaignere, C.; Denning, D.W. Susceptibility testing of Aspergillus flavus: Inoculum dependence with itraconazole and lack of correlation between susceptibility to amphotericin B in vitro and outcome in vivo. Antimicrob. Agents Chemother. 2001, 45, 1456–1462. [Google Scholar] [CrossRef]
- Paterson, P.J.; Seaton, S.; Prentice, H.G.; Kibbler, C.C. Treatment failure in invasive aspergillosis: Susceptibility of deep tissue isolates following treatment with amphotericin B. J. Antimicrob. Chemother. 2003, 52, 873–876. [Google Scholar] [CrossRef]
- Hoenigl, M.; Sprute, R.; Egger, M.; Arastehfar, A.; Cornely, O.A.; Krause, R.; Lass-Flörl, C.; Prattes, J.; Spec, A.; Thompson, G.R., 3rd; et al. The Antifungal Pipeline: Fosmanogepix, Ibrexafungerp, Olorofim, Opelconazole, and Rezafungin. Drugs 2021, 81, 1703–1729. [Google Scholar] [CrossRef] [PubMed]
- The European Committee on Antimicrobial Susceptibility Testing. Overview of Antifungal ECOFFs and Clinical Breakpoints for Yeasts, Moulds and Dermatophytes Using the EUCAST E.Def 7.3, E.Def 9.4 and E.Def 11.0 Procedures, Version 3. 2022. Available online: http://www.eucast.org (accessed on 4 March 2023).
- Rudramurthy, S.M.; Paul, R.A.; Chakrabarti, A.; Mouton, J.W.; Meis, J.F. Invasive Aspergillosis by Aspergillus flavus: Epidemiology, Diagnosis, Antifungal Resistance, and Management. J. Fungi 2019, 5, 55. [Google Scholar] [CrossRef] [PubMed]
- Saghrouni, F.; Ben Youssef, Y.; Gheith, S.; Bouabid, Z.; Ben Abdeljelil, J.; Khammari, I.; Fathallah, A.; Khlif, A.; Ben Saïd, M. Twenty-nine cases of invasive aspergillosis in neutropenic patients. Med. Mal. Infect. 2011, 41, 657–662. [Google Scholar] [CrossRef]
- Tarrand, J.J.; Lichterfeld, M.; Warraich, I.; Luna, M.; Han, X.Y.; May, G.S.; Kontoyiannis, D.P. Diagnosis of Invasive Septate Mold Infections: A Correlation of Microbiological Culture and Histologic or Cytologic Examination. Am. J. Clin. Pathol. 2003, 119, 854–858. [Google Scholar] [CrossRef] [PubMed]
- Al-Hatmi, A.M.S.; Castro, M.A.; de Hoog, G.S.; Badali, H.; Alvarado, V.F.; Verweij, P.E.; Meis, J.F.; Zago, V.V. Epidemiology of Aspergillus species causing keratitis in Mexico. Mycoses 2019, 62, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Chakrabarti, A.; Kaur, H.; Savio, J.; Rudramurthy, S.M.; Patel, A.; Shastri, P.; Pamidimukkala, U.; Karthik, R.; Bhattacharya, S.; Kindo, A.J.; et al. Epidemiology and clinical outcomes of invasive mould infections in Indian intensive care units (FISF study). J. Crit. Care 2019, 51, 64–70. [Google Scholar] [CrossRef]
- Chakrabarti, A.; Chatterjee, S.S.; Das, A.; Shivaprakash, M.R. Invasive aspergillosis in developing countries. Med. Mycol. 2011, 49 (Suppl. S1), S35–S47. [Google Scholar] [CrossRef]
- Gabrielli, E.; Fothergill, A.W.; Brescini, L.; Sutton, D.A.; Marchionni, E.; Orsetti, E.; Staffolani, S.; Castelli, P.; Gesuita, R.; Barchiesi, F. Osteomyelitis caused by Aspergillus species: A review of 310 reported cases. Clin. Microbiol. Infect. 2014, 20, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Koehler, P.; Tacke, D.; Cornely, O.A. Aspergillosis of bones and joints—A review from 2002 until today. Mycoses 2014, 57, 323–335. [Google Scholar] [CrossRef] [PubMed]
- Villate, J.I.; Aldamiz-Echevarria, G.; Gaztelurrutia, L.; Barrenechea, J.I.; González de Zárate, P. Cardiac aspergillosis. J. Thorac. Cardiovasc. Surg. 2000, 119, 403–404. [Google Scholar] [CrossRef] [PubMed]
- Pasqualotto, A.C.; Denning, D.W. Post-operative aspergillosis. Clin. Microbiol. Infect. 2006, 12, 1060–1076. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.K.; Mauger, J.; McGowan, K.L. Immunohistochemical Detection of Aspergillus Species in Pediatric Tissue Samples. Am. J. Clin. Pathol. 2004, 121, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, L.; Standard, P.G.; Jalbert, M.; Kraft, D.E. Immunohistologic identification of Aspergillus spp. and other hyaline fungi by using polyclonal fluorescent antibodies. J. Clin. Microbiol. 1997, 35, 2206–2209. [Google Scholar] [CrossRef] [PubMed]
- Taghizadeh-Armaki, M.; Hedayati, M.T.; Moqarabzadeh, V.; Ansari, S.; Mahdavi Omran, S.; Zarrinfar, H.; Saber, S.; Verweij, P.E.; Denning, D.W.; Seyedmousavi, S. Effect of involved Aspergillus species on galactomannan in bronchoalveolar lavage of patients with invasive aspergillosis. J. Med. Microbiol. 2017, 66, 898–904. [Google Scholar] [CrossRef] [PubMed]
- Lass-Flörl, C.; Kofler, G.; Kropshofer, G.; Hermans, J.; Kreczy, A.; Dierich, M.P.; Niederwieser, D. In-vitro testing of susceptibility to amphotericin B is a reliable predictor of clinical outcome in invasive aspergillosis. J. Antimicrob. Chemother. 1998, 42, 497–502. [Google Scholar] [CrossRef]
- Rudramurthy, S.M.; Chakrabarti, A.; Geertsen, E.; Mouton, J.W.; Meis, J.F. In vitro activity of isavuconazole against 208 Aspergillus flavus isolates in comparison with 7 other antifungal agents: Assessment according to the methodology of the European Committee on Antimicrobial Susceptibility Testing. Diagn Microbiol. Infect. Dis. 2011, 71, 370–377. [Google Scholar] [CrossRef]
- Paul, R.A.; Rudramurthy, S.M.; Dhaliwal, M.; Singh, P.; Ghosh, A.K.; Kaur, H.; Varma, S.; Agarwal, R.; Chakrabarti, A. Magnitude of Voriconazole Resistance in Clinical and Environmental Isolates of Aspergillus flavus and Investigation into the Role of Multidrug Efflux Pumps. Antimicrob. Agents Chemother. 2018, 62, e01022-18. [Google Scholar] [CrossRef]
- Sharma, C.; Kumar, R.; Kumar, N.; Masih, A.; Gupta, D.; Chowdhary, A. Investigation of Multiple Resistance Mechanisms in Voriconazole-Resistant Aspergillus flavus Clinical Isolates from a Chest Hospital Surveillance in Delhi, India. Antimicrob. Agents Chemother. 2018, 62, e01928-17. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Sun, Y.; Chen, W.; Liu, W.; Wan, Z.; Bu, D.; Li, R. The T788G mutation in the cyp51C gene confers voriconazole resistance in Aspergillus flavus causing aspergillosis. Antimicrob. Agents Chemother. 2012, 56, 2598–2603. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Su, X.; Sun, W.-K.; Chen, F.; Xu, X.-Y.; Shi, Y. Efficacy of the Combination of Voriconazole and Caspofungin in Experimental Pulmonary Aspergillosis by Different Aspergillus Species. Mycopathologia 2014, 177, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Kaushik, S.; Ram, J.; Brar, G.S.; Jain, A.K.; Chakraborti, A.; Gupta, A. Intracameral amphotericin B: Initial experience in severe keratomycosis. Cornea 2001, 20, 715–719. [Google Scholar] [CrossRef]
- Seyedmousavi, S.; Lionakis, M.S.; Parta, M.; Peterson, S.W.; Kwon-Chung, K.J. Emerging Aspergillus Species Almost Exclusively Associated With Primary Immunodeficiencies. Open Forum Infect. Dis. 2018, 5, ofy213. [Google Scholar] [CrossRef]
- Falcone, E.L.; Holland, S.M. Invasive fungal infection in chronic granulomatous disease: Insights into pathogenesis and management. Curr. Opin. Infect. Dis. 2012, 25, 658–669. [Google Scholar] [CrossRef]
- Winkelstein, J.A.; Marino, M.C.; Johnston, R.B., Jr.; Boyle, J.; Curnutte, J.; Gallin, J.I.; Malech, H.L.; Holland, S.M.; Ochs, H.; Quie, P.; et al. Chronic granulomatous disease. Report on a national registry of 368 patients. Medicine 2000, 79, 155–169. [Google Scholar] [CrossRef]
- Dotis, J.; Roilides, E. Osteomyelitis due to Aspergillus spp. in patients with chronic granulomatous disease: Comparison of Aspergillus nidulans and Aspergillus fumigatus. Int. J. Infect. Dis. 2004, 8, 103–110. [Google Scholar] [CrossRef]
- Segal, B.H.; DeCarlo, E.S.; Kwon-Chung, K.J.; Malech, H.L.; Gallin, J.I.; Holland, S.M. Aspergillus nidulans infection in chronic granulomatous disease. Medicine 1998, 77, 345–354. [Google Scholar] [CrossRef]
- Blumental, S.; Mouy, R.; Mahlaoui, N.; Bougnoux, M.E.; Debré, M.; Beauté, J.; Lortholary, O.; Blanche, S.; Fischer, A. Invasive mold infections in chronic granulomatous disease: A 25-year retrospective survey. Clin. Infect. Dis. 2011, 53, e159–e169. [Google Scholar] [CrossRef]
- Stemler, J.; Salmanton-García, J.; Seidel, D.; Alexander, B.D.; Bertz, H.; Hoenigl, M.; Herbrecht, R.; Meintker, L.; Meißner, A.; Mellinghoff, S.C.; et al. Risk factors and mortality in invasive Rasamsonia spp. infection: Analysis of cases in the FungiScope(®) registry and from the literature. Mycoses 2020, 63, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Gallin, J.I.; Alling, D.W.; Malech, H.L.; Wesley, R.; Koziol, D.; Marciano, B.; Eisenstein, E.M.; Turner, M.L.; DeCarlo, E.S.; Starling, J.M.; et al. Itraconazole to prevent fungal infections in chronic granulomatous disease. N. Engl. J. Med. 2003, 348, 2416–2422. [Google Scholar] [CrossRef] [PubMed]
- Sprute, R.; Nacov, J.A.; Neofytos, D.; Oliverio, M.; Prattes, J.; Reinhold, I.; Cornely, O.A.; Stemler, J. Antifungal prophylaxis and pre-emptive therapy: When and how? Mol. Asp. Med. 2023; Accepted for publication. [Google Scholar]
- Henriet, S.; Verweij, P.E.; Holland, S.M.; Warris, A. Invasive fungal infections in patients with chronic granulomatous disease. Adv. Exp. Med. Biol. 2013, 764, 27–55. [Google Scholar] [CrossRef] [PubMed]
- Honsig, C.; Selitsch, B.; Hollenstein, M.; Vossen, M.G.; Spettel, K.; Willinger, B. Identification of Filamentous Fungi by MALDI-TOF Mass Spectrometry: Evaluation of Three Different Sample Preparation Methods and Validation of an In-House Species Cutoff. J. Fungi 2022, 8, 383. [Google Scholar] [CrossRef]
- García-Rodríguez, J.; García-Guereta, L.; De Pablos, M.; Burgueros, M.; Borches, D. Galactomannan detection as a tool for the diagnosis and management of cardiac aspergillosis in 2 immunocompetent patients. Clin. Infect. Dis. 2008, 47, e90–e92. [Google Scholar] [CrossRef] [PubMed]
- Tavakoli, M.; Rivero-Menendez, O.; Abastabar, M.; Hedayati, M.T.; Sabino, R.; Siopi, M.; Zarrinfar, H.; Nouripour-Sisakht, S.; van der Lee, H.; Valadan, R.; et al. Genetic diversity and antifungal susceptibility patterns of Aspergillus nidulans complex obtained from clinical and environmental sources. Mycoses 2020, 63, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Espinel-Ingroff, A.; Chowdhary, A.; Gonzalez, G.M.; Lass-Flörl, C.; Martin-Mazuelos, E.; Meis, J.; Peláez, T.; Pfaller, M.A.; Turnidge, J. Multicenter study of isavuconazole MIC distributions and epidemiological cutoff values for Aspergillus spp. for the CLSI M38-A2 broth microdilution method. Antimicrob. Agents Chemother. 2013, 57, 3823–3828. [Google Scholar] [CrossRef]
- Kontoyiannis, D.P.; Lewis, R.E.; May, G.S.; Osherov, N.; Rinaldi, M.G. Aspergillus nidulans is frequently resistant to amphotericin B. Mycoses 2002, 45, 406–407. [Google Scholar] [CrossRef]
- Seyedmousavi, S.; Chang, Y.C.; Law, D.; Birch, M.; Rex, J.H.; Kwon-Chung, K.J. Efficacy of Olorofim (F901318) against Aspergillus fumigatus, A. nidulans, and A. tanneri in Murine Models of Profound Neutropenia and Chronic Granulomatous Disease. Antimicrob. Agents Chemother. 2019, 63, e00129-19. [Google Scholar] [CrossRef]
- Singh, N.; Paterson, D.L. Aspergillus infections in transplant recipients. Clin. Microbiol. Rev. 2005, 18, 44–69. [Google Scholar] [CrossRef]
- Vermeulen, E.; Maertens, J.; Meersseman, P.; Saegeman, V.; Dupont, L.; Lagrou, K. Invasive Aspergillus niger complex infections in a Belgian tertiary care hospital. Clin. Microbiol. Infect. 2014, 20, O333–O335. [Google Scholar] [CrossRef] [PubMed]
- Verweij, P.E.; Snelders, E.; Kema, G.H.; Mellado, E.; Melchers, W.J. Azole resistance in Aspergillus fumigatus: A side-effect of environmental fungicide use? Lancet Infect. Dis. 2009, 9, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Montazeri, A.; Zandi, H.; Teymouri, F.; Soltanianzadeh, Z.; Jambarsang, S.; Mokhtari, M. Microbiological analysis of bacterial and fungal bioaerosols from burn hospital of Yazd (Iran) in 2019. J. Environ. Health Sci. Eng. 2020, 18, 1121–1130. [Google Scholar] [CrossRef] [PubMed]
- Gautier, M.; Normand, A.C.; L’Ollivier, C.; Cassagne, C.; Reynaud-Gaubert, M.; Dubus, J.C.; Brégeon, F.; Hendrickx, M.; Gomez, C.; Ranque, S.; et al. Aspergillus tubingensis: A major filamentous fungus found in the airways of patients with lung disease. Med. Mycol. 2016, 54, 459–470. [Google Scholar] [CrossRef] [PubMed]
- Aneja, K.R.; Sharma, C.; Joshi, R. Fungal infection of the ear: A common problem in the north eastern part of Haryana. Int. J. Pediatr. Otorhinolaryngol. 2010, 74, 604–607. [Google Scholar] [CrossRef] [PubMed]
- Fianchi, L.; Picardi, M.; Cudillo, L.; Corvatta, L.; Mele, L.; Trapè, G.; Girmenia, C.; Pagano, L. Aspergillus niger infection in patients with haematological diseases: A report of eight cases. Mycoses 2004, 47, 163–167. [Google Scholar] [CrossRef]
- Dotis, J.; Kondou, A.; Koukloumperi, E.; Karava, V.; Papadopoulou, A.; Gkogka, C.; Printza, N. Aspergillus peritonitis in peritoneal dialysis patients: A systematic review. J. Mycol. Med. 2020, 30, 101037. [Google Scholar] [CrossRef]
- D’Hooge, E.; Becker, P.; Stubbe, D.; Normand, A.C.; Piarroux, R.; Hendrickx, M. Black aspergilli: A remaining challenge in fungal taxonomy? Med. Mycol. 2019, 57, 773–780. [Google Scholar] [CrossRef]
- Chen, S.C.-A.; Meyer, W.; Sorrell, T.C.; Halliday, C.L. Aspergillus, Talaromyces, and Penicillium. In Manual of Clinical Microbiology; John and Wiley and Sons: Hoboken, NJ, USA, 2016; p. 2116. [Google Scholar]
- Arendrup, M.C.; Meletiadis, J.; Mouton, J.W.; Guinea, J.; Cuenca-Estrella, M.; Lagrou, K.; Howard, S.J. EUCAST technical note on isavuconazole breakpoints for Aspergillus, itraconazole breakpoints for Candida and updates for the antifungal susceptibility testing method documents. Clin. Microbiol. Infect. 2016, 22, 571.e1–571.e4. [Google Scholar] [CrossRef]
- Espinel-Ingroff, A.; Arendrup, M.; Cantón, E.; Cordoba, S.; Dannaoui, E.; García-Rodríguez, J.; Gonzalez, G.M.; Govender, N.P.; Martin-Mazuelos, E.; Lackner, M.; et al. Multicenter Study of Method-Dependent Epidemiological Cutoff Values for Detection of Resistance in Candida spp. and Aspergillus spp. to Amphotericin B and Echinocandins for the Etest Agar Diffusion Method. Antimicrob. Agents Chemother. 2017, 61, e01792-16. [Google Scholar] [CrossRef]
- Hashimoto, A.; Hagiwara, D.; Watanabe, A.; Yahiro, M.; Yikelamu, A.; Yaguchi, T.; Kamei, K. Drug Sensitivity and Resistance Mechanism in Aspergillus Section Nigri Strains from Japan. Antimicrob. Agents Chemother. 2017, 61, e02583-16. [Google Scholar] [CrossRef] [PubMed]
- Espinel-Ingroff, A.; Turnidge, J. The role of epidemiological cutoff values (ECVs/ECOFFs) in antifungal susceptibility testing and interpretation for uncommon yeasts and moulds. Rev. Iberoam. Micol. 2016, 33, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Roohani, A.H.; Fatima, N.; Shameem, M.; Khan, H.M.; Khan, P.A.; Akhtar, A. Comparing the profile of respiratory fungal pathogens amongst immunocompetent and immunocompromised hosts, their susceptibility pattern and correlation of various opportunistic respiratory fungal infections and their progression in relation to the CD4+T-cell counts. Indian J. Med. Microbiol. 2018, 36, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Torres, H.A.; Rivero, G.A.; Lewis, R.E.; Hachem, R.; Raad, I.I.; Kontoyiannis, D.P. Aspergillosis caused by non-fumigatus Aspergillus species: Risk factors and in vitro susceptibility compared with Aspergillus fumigatus. Diagn. Microbiol. Infect. Dis. 2003, 46, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Wald, A.; Leisenring, W.; van Burik, J.-A.; Bowden, R.A. Epidemiology of Aspergillus Infections in a Large Cohort of Patients Undergoing Bone Marrow Transplantation. J. Infect. Dis. 1997, 175, 1459–1466. [Google Scholar] [CrossRef]
- Howard, S.J.; Harrison, E.; Bowyer, P.; Varga, J.; Denning, D.W. Cryptic species and azole resistance in the Aspergillus niger complex. Antimicrob. Agents Chemother. 2011, 55, 4802–4809. [Google Scholar] [CrossRef]
- Lass-Flörl, C.; Dietl, A.-M.; Kontoyiannis, D.P.; Brock, M. Aspergillus terreus Species Complex. Clin. Microbiol. Rev. 2021, 34, e00311–e00320. [Google Scholar] [CrossRef]
- Baddley, J.W.; Pappas, P.G.; Smith, A.C.; Moser, S.A. Epidemiology of Aspergillus terreus at a University Hospital. J. Clin. Microbiol. 2003, 41, 5525–5529. [Google Scholar] [CrossRef]
- Risslegger, B.; Zoran, T.; Lackner, M.; Aigner, M.; Sánchez-Reus, F.; Rezusta, A.; Chowdhary, A.; Taj-Aldeen, S.J.; Arendrup, M.C.; Oliveri, S.; et al. A prospective international Aspergillus terreus survey: An EFISG, ISHAM and ECMM joint study. Clin. Microbiol. Infect. 2017, 23, 776.e1–776.e5. [Google Scholar] [CrossRef]
- Arabatzis, M.; Velegraki, A. Sexual reproduction in the opportunistic human pathogen Aspergillus terreus. Mycologia 2013, 105, 71–79. [Google Scholar] [CrossRef]
- Lass-Flörl, C.; Griff, K.; Mayr, A.; Petzer, A.; Gastl, G.; Bonatti, H.; Freund, M.; Kropshofer, G.; Dierich, M.P.; Nachbaur, D. Epidemiology and outcome of infections due to Aspergillus terreus: 10-year single centre experience. Br. J. Haematol. 2005, 131, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Malani, A.N.; Kauffman, C.A. Changing Epidemiology of Rare Mould Infections. Drugs 2007, 67, 1803–1812. [Google Scholar] [CrossRef] [PubMed]
- Blum, G.; Perkhofer, S.; Grif, K.; Mayr, A.; Kropshofer, G.; Nachbaur, D.; Kafka-Ritsch, R.; Dierich, M.P.; Lass-Flörl, C. A 1-year Aspergillus terreus surveillance study at the University Hospital of Innsbruck: Molecular typing of environmental and clinical isolates. Clin. Microbiol. Infect. 2008, 14, 1146–1151. [Google Scholar] [CrossRef] [PubMed]
- Rüping, M.J.; Gerlach, S.; Fischer, G.; Lass-Flörl, C.; Hellmich, M.; Vehreschild, J.J.; Cornely, O.A. Environmental and clinical epidemiology of Aspergillus terreus: Data from a prospective surveillance study. J. Hosp. Infect. 2011, 78, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Driemeyer, C.; Falci, D.R.; Oladele, R.O.; Bongomin, F.; Ocansey, B.K.; Govender, N.P.; Hoenigl, M.; Gangneux, J.P.; Lass-Flörl, C.; Cornely, O.A.; et al. The current state of clinical mycology in Africa: A European Confederation of Medical Mycology and International Society for Human and Animal Mycology survey. Lancet Microbe 2022, 3, e464–e470. [Google Scholar] [CrossRef]
- Salmanton-García, J.; Au, W.Y.; Hoenigl, M.; Chai, L.Y.A.; Badali, H.; Basher, A.; Brockhoff, R.A.; Chen, S.C.; Chindamporn, A.; Chowdhary, A.; et al. The current state of laboratory mycology in Asia/Pacific: A survey from the European Confederation of Medical Mycology (ECMM) and International Society for Human and Animal Mycology (ISHAM). Int. J. Antimicrob. Agents 2023, 106718. [Google Scholar] [CrossRef]
- Salmanton-García, J.; Hoenigl, M.; Gangneux, J.-P.; Segal, E.; Alastruey-Izquierdo, A.; Arikan Akdagli, S.; Lagrou, K.; Özenci, V.; Vena, A.; Cornely, O.A. The current state of laboratory mycology and access to antifungal treatment in Europe: A European Confederation of Medical Mycology survey. Lancet Microbe 2023, 4, e47–e56. [Google Scholar] [CrossRef]
- Van Der Linden, J.W.; Warris, A.; Verweij, P.E. Aspergillus species intrinsically resistant to antifungal agents. Med. Mycol. 2011, 49 (Suppl. S1), S82–S89. [Google Scholar] [CrossRef]
- Glampedakis, E.; Cassaing, S.; Fekkar, A.; Dannaoui, E.; Bougnoux, M.-E.; Bretagne, S.; Neofytos, D.; Schreiber, P.W.; Hennequin, C.; Morio, F.; et al. Invasive Aspergillosis Due to Aspergillus Section Usti: A Multicenter Retrospective Study. Clin. Infect. Dis. 2021, 72, 1379–1385. [Google Scholar] [CrossRef]
- Seidel, D.; Durán Graeff, L.A.; Vehreschild, M.; Wisplinghoff, H.; Ziegler, M.; Vehreschild, J.J.; Liss, B.; Hamprecht, A.; Köhler, P.; Racil, Z.; et al. FungiScope(™) -Global Emerging Fungal Infection Registry. Mycoses 2017, 60, 508–516. [Google Scholar] [CrossRef]
- Hoenigl, M.; Gangneux, J.-P.; Segal, E.; Alanio, A.; Chakrabarti, A.; Chen, S.C.A.; Govender, N.; Hagen, F.; Klimko, N.; Meis, J.F.; et al. Global guidelines and initiatives from the European Confederation of Medical Mycology to improve patient care and research worldwide: New leadership is about working together. Mycoses 2018, 61, 885–894. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stemler, J.; Többen, C.; Lass-Flörl, C.; Steinmann, J.; Ackermann, K.; Rath, P.-M.; Simon, M.; Cornely, O.A.; Koehler, P. Diagnosis and Treatment of Invasive Aspergillosis Caused by Non-fumigatus Aspergillus spp. J. Fungi 2023, 9, 500. https://doi.org/10.3390/jof9040500
Stemler J, Többen C, Lass-Flörl C, Steinmann J, Ackermann K, Rath P-M, Simon M, Cornely OA, Koehler P. Diagnosis and Treatment of Invasive Aspergillosis Caused by Non-fumigatus Aspergillus spp. Journal of Fungi. 2023; 9(4):500. https://doi.org/10.3390/jof9040500
Chicago/Turabian StyleStemler, Jannik, Christina Többen, Cornelia Lass-Flörl, Jörg Steinmann, Katharina Ackermann, Peter-Michael Rath, Michaela Simon, Oliver Andreas Cornely, and Philipp Koehler. 2023. "Diagnosis and Treatment of Invasive Aspergillosis Caused by Non-fumigatus Aspergillus spp." Journal of Fungi 9, no. 4: 500. https://doi.org/10.3390/jof9040500