
Pneumocystis jirovecii Pneumonia Diagnostic Approach: Real-Life Experience in a Tertiary Centre
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Hospital Setting, Patients and Study Population
2.2. Microbiological Diagnosis
2.3. Data Collection
2.4. PJP Definition
2.5. Statistical Analyses
2.6. Ethics
3. Results
3.1. Microbiological Diagnosis for Pneumocystis jirovecii Pneumonia
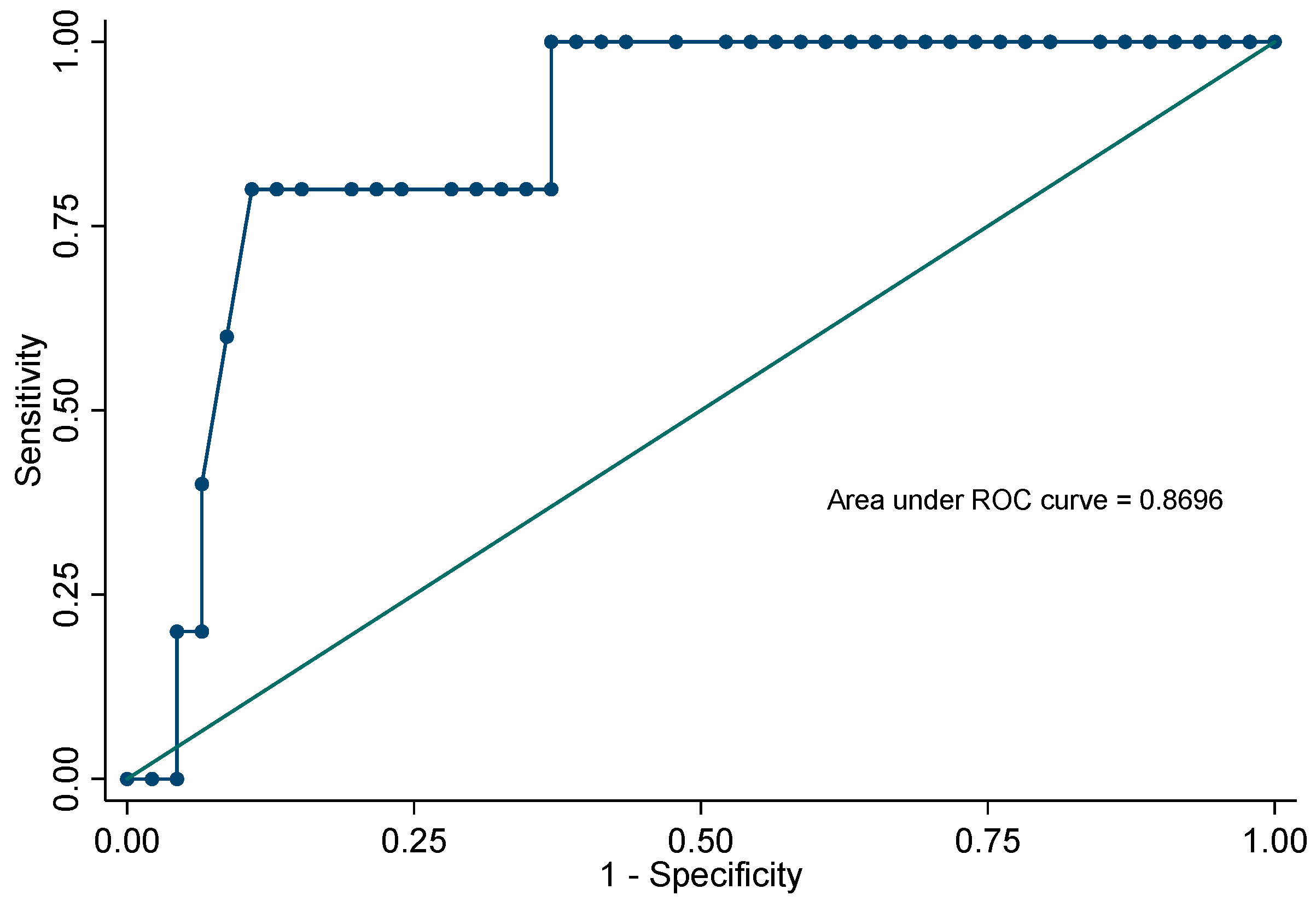
3.2. Cycle Threshold PCR Stratification
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sepkowitz, K.A. Opportunistic infections in patients with and patients without Acquired Immunodeficiency Syndrome. Clin Infect. Dis. 2002, 34, 1098–1107, published correction appears in Clin. Infect. Dis. 2002, 34, 1293. [Google Scholar] [CrossRef]
- Williams, K.M.; Ahn, K.W.; Chen, M.; Aljurf, M.D.; Agwu, A.L.; Chen, A.R.; Walsh, T.J.; Szabolcs, P.; Boeckh, M.J.; Auletta, J.J.; et al. The incidence, mortality and timing of Pneumocystis jiroveci pneumonia after hematopoietic cell transplantation: A CIBMTR analysis. Bone Marrow Transpl. 2016, 51, 573–580. [Google Scholar] [CrossRef] [Green Version]
- Thomas, C.F., Jr.; Limper, A.H. Pneumocystis pneumonia. N. Engl. J. Med. 2004, 350, 2487–2498. [Google Scholar] [CrossRef]
- Bateman, M.; Oladele, R.; Kolls, J.K. Diagnosing Pneumocystis jirovecii pneumonia: A review of current methods and novel approaches. Med. Mycol. 2020, 58, 1015–1028. [Google Scholar] [CrossRef]
- Robert-Gangneux, F.; Belaz, S.; Revest, M.; Tattevin, P.; Jouneau, S.; Decaux, O.; Chevrier, S.; Le Tulzo, Y.; Gangneux, J.-P. Diagnosis of Pneumocystis jirovecii pneumonia in immunocompromised patients by real-time PCR: A 4-year prospective study. J. Clin. Microbiol. 2014, 52, 3370–3376. [Google Scholar] [CrossRef] [Green Version]
- Doyle, L.; Vogel, S.; Procop, G.W. Pneumocystis PCR: It Is Time to Make PCR the Test of Choice. Open Forum. Infect. Dis. 2017, 4, ofx193. [Google Scholar] [CrossRef] [Green Version]
- Morjaria, S.; Frame, J.; Franco-Garcia, A.; Geyer, A.; Kamboj, M.; Babady, N.E. Clinical Performance of (1,3) Beta-D Glucan for the Diagnosis of Pneumocystis Pneumonia (PCP) in Cancer Patients Tested with PCP Polymerase Chain Reaction. Clin. Infect. Dis. 2019, 69, 1303–1309. [Google Scholar] [CrossRef]
- Goterris, L.; Mancebo Fernández, M.A.; Aguilar-Company, J.; Falcó, V.; Ruiz-Camps, I.; Martín-Gómez, M.T. Molecular Diagnosis of Pneumocystis jirovecii Pneumonia by Use of Oral Wash Samples in Immunocompromised Patients: Usefulness and Importance of the DNA Target. J. Clin Microbiol. 2019, 57, e01287-19. [Google Scholar] [CrossRef]
- Limper, A.H.; Offord, K.P.; Smith, T.F.; Martin, W.J., 2nd. Pneumocystis carinii pneumonia. Differences in lung parasite number and inflammation in patients with and without AIDS. Am. Rev. Respir. Dis. 1989, 140, 1204–1209. [Google Scholar] [CrossRef]
- Maillet, M.; Maubon, D.; Brion, J.P.; François, P.; Molina, L.; Stahl, J.P.; Epaulard, O.; Bosseray, A.; Pavese, P. Pneumocystis jirovecii (Pj) quantitative PCR to differentiate Pj pneumonia from Pj colonization in immunocompromised patients. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 331–336. [Google Scholar] [CrossRef]
- Larsen, H.H.; Masur, H.; Kovacs, J.A.; Gill, V.J.; Silcott, V.A.; Kogulan, P.; Maenza, J.; Smith, M.; Lucey, D.R.; Fischer, S.H. Development and evaluation of a quantitative, touch-down, real-time PCR assay for diagnosing Pneumocystis carinii pneumonia. J. Clin. Microbiol. 2002, 40, 490–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fauchier, T.; Hasseine, L.; Gari-Toussaint, M.; Casanova, V.; Marty, P.M.; Pomares, C. Detection of Pneumocystis jirovecii by Quantitative PCR To Differentiate Colonization and Pneumonia in Immunocompromised HIV-Positive and HIV-Negative Patients. J. Clin. Microbiol. 2016, 54, 1487–1495. [Google Scholar] [CrossRef] [Green Version]
- Mühlethaler, K.; Bögli-Stuber, K.; Wasmer, S.; von Garnier, C.; Dumont, P.; Rauch, A.; Mühlemann, K.; Garzoni, C. Quantitative PCR to diagnose Pneumocystis pneumonia in immunocompromised non-HIV patients. Eur. Respir. J. 2012, 39, 971–978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, J.W.; Limper, A.H.; Grys, T.E.; Karre, T.; Wengenack, N.L.; Binnicker, M.J. Pneumocystis jirovecii testing by real-time polymerase chain reaction and direct examination among immunocompetent and immunosuppressed patient groups and correlation to disease specificity. Diagn Microbiol. Infect. Dis. 2011, 69, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Alanio, A.; Desoubeaux, G.; Sarfati, C.; Hamane, S.; Bergeron, A.; Azoulay, E.; Molina, J.M.; Derouin, F.; Menotti, J. Real-time PCR assay-based strategy for differentiation between active Pneumocystis jirovecii pneumonia and colonization in immunocompromised patients. Clin. Microbiol. Infect. 2011, 17, 1531–1537. [Google Scholar] [CrossRef] [PubMed]
- Tia, T.; Putaporntip, C.; Kosuwin, R.; Kongpolprom, N.; Kawkitinarong, K.; Jongwutiwes, S. A highly sensitive novel PCR assay for detection of Pneumocystis jirovecii DNA in bronchoalveloar lavage specimens from immunocompromised patients. Clin. Microbiol. Infect. 2012, 18, 598–603. [Google Scholar] [CrossRef] [Green Version]
- Walzer, P.D.; Evans, H.E.; Copas, A.J.; Edwards, S.G.; Grant, A.D.; Miller, R.F. Early predictors of mortality from Pneumocystis jirovecii pneumonia in HIV-infected patients: 1985–2006. Clin. Infect. Dis. 2008, 46, 625–633. [Google Scholar] [CrossRef]
- Gaborit, B.J.; Tessoulin, B.; Lavergne, R.-A.; Morio, F.; Sagan, C.; Canet, E.; LeComte, R.; Leturnier, P.; Deschanvres, C.; Khatchatourian, L.; et al. Outcome and prognostic factors of Pneumocystis jirovecii pneumonia in immunocompromised adults: A prospective observational study. Ann. Intensive Care. 2019, 9, 131. [Google Scholar] [CrossRef]
- Roblot, F.; Godet, C.; Le Moal, G.; Garo, B.; Faouzi Souala, M.; Dary, M.; de Gentile, L.; Gandji, J.; Guimard, Y.; Lacroix, C.; et al. Analysis of underlying diseases and prognosis factors associated with Pneumocystis carinii pneumonia in immunocompromised HIV-negative patients. Eur. J. Clin. Microbiol. Infect. Dis. 2002, 21, 523–531. [Google Scholar] [CrossRef]
- Pulvirenti, J.; Herrera, P.; Venkataraman, P.; Ahmed, N. Pneumocystis carinii pneumonia in HIV-infected patients in the HAART era. AIDS Patient Care STDS 2003, 17, 261–265. [Google Scholar] [CrossRef]
- Procop, G.W.; Haddad, S.; Quinn, J.; Wilson, M.L.; Henshaw, N.G.; Reller, L.B.; Artymyshyn, R.L.; Katanik, M.T.; Weinstein, M.P. Detection of Pneumocystis jiroveci in respiratory specimens by four staining methods. J. Clin. Microbiol. 2004, 42, 3333–3335. [Google Scholar] [CrossRef] [Green Version]
- Moodley, B.; Tempia, S.; Frean, J.A. Comparison of quantitative real-time PCR and direct immunofluorescence for the detection of Pneumocystis jirovecii. PLoS ONE 2017, 12, e0180589. [Google Scholar] [CrossRef]
- Peterson, J.C.; Cushion, M.T. Pneumocystis: Not just pneumonia. Curr. Opin. Microbiol. 2005, 8, 393–398. [Google Scholar] [CrossRef]
- Durand-Joly, I.; Chabé, M.; Soula, F.; Delhaes, L.; Camus, D.; Dei-Cas, E. Molecular diagnosis of Pneumocystis pneumonia. FEMS Immunol. Med. Microbiol. 2005, 45, 405–410. [Google Scholar] [CrossRef] [Green Version]
- Lagrou, K.; Chen, S.; Masur, H.; Viscoli, C.; Decker, C.F.; Pagano, L.; Groll, A.H. Pneumocystis jirovecii Disease: Basis for the Revised EORTC/MSGERC Invasive Fungal Disease Definitions in Individuals Without Human Immunodeficiency Virus. Clin. Infect. Dis. 2021, 72 (Suppl. S2), S114–S120. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [Green Version]
- Alvarez-Martínez, M.J.; Miró, J.M.; Valls, M.E.; Moreno, A.; Rivas, P.V.; Solé, M.; Benito, N.; Domingo, P.; Muñoz-Batet, C.; Rivera, E.; et al. Sensitivity and specificity of nested and real-time PCR for the detection of Pneumocystis jiroveci in clinical specimens. Diagn Microbiol. Infect. Dis. 2006, 56, 153–160. [Google Scholar] [CrossRef]
- Fan, L.C.; Lu, H.W.; Cheng, K.B.; Li, H.P.; Xu, J.F. Evaluation of PCR in bronchoalveolar lavage fluid for diagnosis of Pneumocystis jirovecii pneumonia: A bivariate meta-analysis and systematic review. PLoS ONE 2013, 8, e73099. [Google Scholar] [CrossRef] [Green Version]
- Alanio, A.; Hauser, P.M.; Lagrou, K.; Melchers, W.J.G.; Helweg-Larsen, J.; Matos, O.; Cesaro, S.; Maschmeyer, G.; Einsele, H.; Donnelly, J.P.; et al. ECIL guidelines for the diagnosis of Pneumocystis jirovecii pneumonia in patients with haematological malignancies and stem cell transplant recipients. J. Antimicrob. Chemother. 2016, 71, 2386–2396. [Google Scholar] [CrossRef] [Green Version]
- Juliano, J.J.; Barnett, E.; Parobek, C.M.; Taylor, S.M.; Meshnick, S.R.; Stone, S.; Chang, E.; Fong, S.; Huang, L. Use of Oropharyngeal Washes to Diagnose and Genotype Pneumocystis jirovecii. Open Forum. Infect. Dis. 2015, 2, ofv080. [Google Scholar] [CrossRef] [Green Version]
- To, K.K.W.; Wong, S.C.Y.; Xu, T.; Poon, R.W.S.; Mok, K.-Y.; Chan, J.F.W.; Cheng, V.C.C.; Chan, K.-H.; Hung, I.F.N.; Yuen, K.-Y. Use of nasopharyngeal aspirate for diagnosis of pneumocystis pneumonia. J. Clin. Microbiol. 2013, 51, 1570–1574. [Google Scholar] [CrossRef] [Green Version]
- Guigue, N.; Alanio, A.; Menotti, J.; De Castro, N.; Hamane, S.; Peyrony, O.; LeGoff, J.; Bretagne, S. Utility of adding Pneumocystis jirovecii DNA detection in nasopharyngeal aspirates in immunocompromised adult patients with febrile pneumonia. Med. Mycol. 2015, 53, 241–247. [Google Scholar] [CrossRef] [Green Version]
- Onishi, A.; Sugiyama, D.; Kogata, Y.; Saegusa, J.; Sugimoto, T.; Kawano, S.; Morinobu, A.; Nishimura, K.; Kumagai, S. Diagnostic accuracy of serum 1,3-β-D-glucan for pneumocystis jiroveci pneumonia, invasive candidiasis, and invasive aspergillosis: Systematic review and meta-analysis. J. Clin. Microbiol. 2012, 50, 7–15. [Google Scholar] [CrossRef] [Green Version]
- Matsumura, Y.; Ito, Y.; Iinuma, Y.; Yasuma, K.; Yamamoto, M.; Matsushima, A.; Nagao, M.; Takakura, S.; Ichiyama, S. Quantitative real-time PCR and the (1→3)-β-D-glucan assay for differentiation between Pneumocystis jirovecii pneumonia and colonization. Clin. Microbiol. Infect. 2012, 18, 591–597. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| With PJP n (%) | Without PJP n (%) | p Value | |
|---|---|---|---|
| Patients | 48 | 251 | |
| Median age (years, IQR) | 57 (49–69) | 58 (45–69) | 0.83 |
| Sex (male) | 31 (65) | 163 (65) | 0.96 |
| Underlying disease | |||
| Hematologic malignancy | 10 (21) | 53 (21) | 0.965 |
| HIV infection | 12 (25) | 41 (16) | 0.150 |
| Solid tumor | 16 (33) | 36 (14) | <0.01 |
| Solid organ transplantation | 1 (2) | 24 (10) | 0.09 |
| Autoimmune disease | 3 (6) | 16 (6) | 0.97 |
| Steroid exposure | 3 (6) | 9 (4) | 0.39 |
| Other a | 0 | 1 (0.4) | 0.66 |
| No immunosuppression | 3 (6) | 71 (28) | <0.01 |
| Previous PJP prophylaxis | 2 (4) | 59 (24) | <0.01 |
| Main clinical manifestation | |||
| Dyspnea | 29 (60) | 132 (53) | 0.47 |
| Fever | 12 (25) | 59 (24) | 0.82 |
| Cough | 7 (15) | 22 (9) | 0.21 |
| No suggestive symptoms | 0 | 38 (15) | <0.01 |
| Radiological findings | |||
| Interstitial | 21 (44) | 46 (18) | <0.01 |
| Ground glass pattern | 15 (31) | 21 (8) | <0.01 |
| Reticular | 1 (2) | 21 (8) | 0.13 |
| Consolidation | 10 (21) | 120 (48) | <0.01 |
| Other b | 1 (2) | 43(17) | 0.02 |
| Median ALC (cell/µL) (IQR) | 600 (300–1100) | 700 (300–1400) | 0.29 |
| Median LDH (U/L) (IQR) | 381 (2–527) | 273 (188–401) | <0.01 |
| BDG (pg/mL) performed | 28(58) | 75 (30) | <0.01 |
| <80 | 6 (21) | 39 (52) | <0.01 |
| ≥80 | 22 (79) | 36 (48) | <0.01 |
| Microbiological diagnosis | |||
| IFA positive | 13 (27) | 0 | <0.01 |
| PCR positive | 46 (96) | 5 (2) | <0.01 |
| Median Ct (range) | 30.3 (18.2–38.5) | 36.6 (32.4–37.6) | <0.01 |
| Sample collected | |||
| BALF | 25 (52) | 156 (62) | 0.19 |
| Tracheal aspirate | 6 (13) | 47 (19) | 0.30 |
| Sputum | 17 (35) | 48 (19) | <0.01 |
| Mortality | 12(25) | 2 (2) | <0.01 |
| IFA 95% CI | PCR 95% CI | |
|---|---|---|
| Sensitivity | 27.1% (16.6–41) | 95.8% (86–98.8) |
| Specificity | 100% (98.5–100) | 98% (95.4–99.1) |
| PPV | 100% (77.2–100) | 90.2% (79.0–95.7) |
| NPV | 87.2% (83.5–91.1) | 99.2% (97.1–99.8) |
| BALF % (95% CI) | Tracheal Aspirate % (95% CI) | Sputum % (95% CI) | ||||
|---|---|---|---|---|---|---|
| IFA | PCR | IFA | PCR | IFA | PCR | |
| Sensitivity | 24 (11.5–43.4) | 100 (86.7–100) | 33.3 (9.7–70) | 100 (61–100) | 29.4 (13.3–53.1) | 83.2 (65.7–96.7) |
| Specificity | 100 (97.6–100) | 99.4 (96.5–100) | 100 (92.4–100) | 100 (92.4–100) | 100 (92.6–100) | 91.7 (80.4–97) |
| PPV | 100 (61–100) | 96.2 (81.1–99.3) | 100 (34.2–100) | 100 (61–100) | 100 (56.6–100) | 78.9 (56.7–91.5) |
| NPV | 89.1 (83.7–92.9) | 100 (96.9–100) | 92.2 (81.5–97) | 100 (92.4–100) | 80 (68.2–88.2) | 95.7 (85.5–98.8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veintimilla, C.; Álvarez-Uría, A.; Martín-Rabadán, P.; Valerio, M.; Machado, M.; Padilla, B.; Alonso, R.; Diez, C.; Muñoz, P.; Marín, M. Pneumocystis jirovecii Pneumonia Diagnostic Approach: Real-Life Experience in a Tertiary Centre. J. Fungi 2023, 9, 414. https://doi.org/10.3390/jof9040414
Veintimilla C, Álvarez-Uría A, Martín-Rabadán P, Valerio M, Machado M, Padilla B, Alonso R, Diez C, Muñoz P, Marín M. Pneumocystis jirovecii Pneumonia Diagnostic Approach: Real-Life Experience in a Tertiary Centre. Journal of Fungi. 2023; 9(4):414. https://doi.org/10.3390/jof9040414
Chicago/Turabian StyleVeintimilla, Cristina, Ana Álvarez-Uría, Pablo Martín-Rabadán, Maricela Valerio, Marina Machado, Belén Padilla, Roberto Alonso, Cristina Diez, Patricia Muñoz, and Mercedes Marín. 2023. "Pneumocystis jirovecii Pneumonia Diagnostic Approach: Real-Life Experience in a Tertiary Centre" Journal of Fungi 9, no. 4: 414. https://doi.org/10.3390/jof9040414