
Clinical Manifestations of Human Exposure to Fungi

 , , and
, , and 
Abstract
:1. Introduction
2. Allergic Fungal Diseases
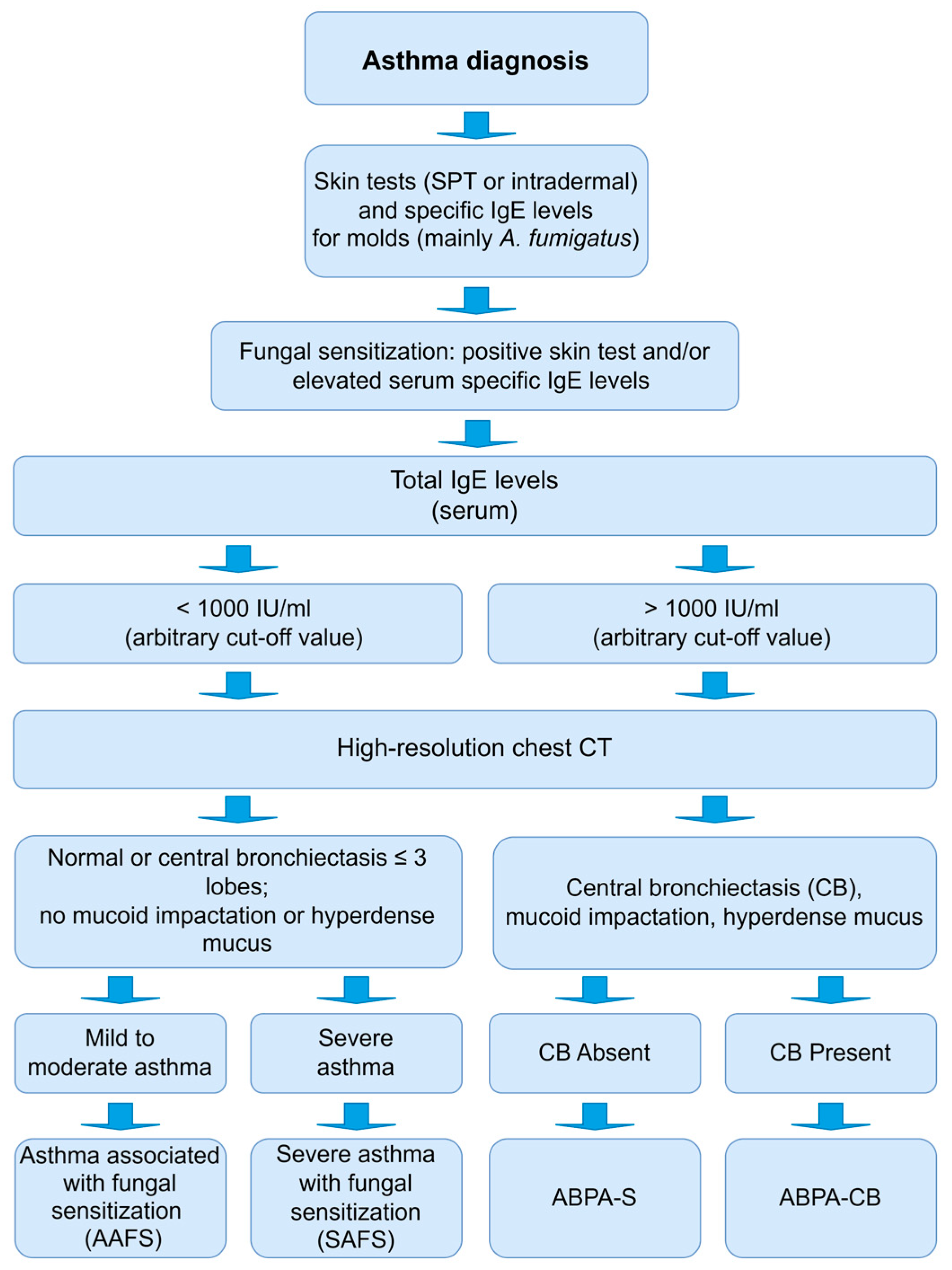
2.1. Allergic Bronchopulmonary Aspergillosis (ABPA)
2.2. Severe Asthma with Fungal Sensitization (SAFS)
2.3. Thunderstorm Asthma (TA)
2.4. Allergic Fungal Rhinosinusitis (AFRS)
2.5. Occupational Lung Diseases
3. Association of Immunodeficiencies and Fungal Diseases
4. Fungal Infections
4.1. Superficial Infections
4.1.1. Dermatophytosis
4.1.2. Candidiasis
4.1.3. Pityriasis Versicolor
4.2. Subcutaneous Infections
4.2.1. Eumycetoma
4.2.2. Chromoblastomycosis
4.3. Systemic Infections
4.3.1. Aspergilloma and Aspergillosis
4.3.2. Candidemia and Invasive Candidiasis
4.3.3. Cryptococcosis
4.3.4. Blastomycosis
4.3.5. Coccidioidomycosis
4.3.6. Histoplasmosis
4.3.7. Emergomycosis
4.3.8. Paracoccidioidomycosis
4.3.9. Talaromycosis
4.3.10. Fusariosis
4.3.11. Hyalohyphomycosis
4.3.12. Lomentosporiosis
4.3.13. Mucormycosis
4.3.14. Phaeohyphomycosis
4.3.15. Pneumocystis Jirovecii Pneumonia
4.3.16. Sporotrichosis
4.3.17. Treatment of Systemic Mycoses
5. Prospects
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oliveira, M.; Amorim, M.; Ferreira, E.; Delgado, L.; Abreu, I. Main airborne Ascomycota spores: Characterization by culture, spore morphology, ribosomal DNA sequences and enzymatic analysis. Appl. Microbiol. Biotechnol. 2010, 86, 1171–1181. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, M.; Ribeiro, H.; Delgado, L.; Fonseca, J.; Castel-Branco, M.G.; Abreu, I. Outdoor allergenic fungal spores: Comparison between an urban and a rural area in northern Portugal. J. Investig. Allergol. Clin. Immunol. 2010, 20, 117. [Google Scholar] [PubMed]
- Adnan, M.; Islam, W.; Gang, L.; Chen, H. Advanced research tools for fungal diversity and its impact on forest ecosystem. Environ. Sci. Pollut. Res. 2022, 29, 45044–45062. [Google Scholar] [CrossRef] [PubMed]
- Barros, J.; Seena, S. Fungi in Freshwaters: Prioritising Aquatic Hyphomycetes in Conservation Goals. Water 2022, 14, 605. [Google Scholar] [CrossRef]
- Gonçalves, M.; Esteves, A.; Alves, A. Marine fungi: Opportunities and challenges. Encyclopedia 2022, 2, 559–577. [Google Scholar] [CrossRef]
- Perez, J. Fungi of the human gut microbiota: Roles and significance. Int. J. Med. Microbiol. 2021, 311, 151490. [Google Scholar] [CrossRef]
- Kim, H.; Oh, H.N.; Park, T.; Kim, H.; Lee, H.G.; An, S.; Sul, W.J. Aged related human skin microbiome and mycobiome in Korean women. Sci. Rep. 2022, 12, 2351. [Google Scholar] [CrossRef]
- Park, J.; Schwardt, N.H.; Jo, J.-H.; Zhang, Z.; Pillai, V.; Phang, S.; Brady, S.M.; Portillo, J.A.; MacGibeny, M.A.; Liang, H.; et al. Shifts in the skin bacterial and fungal communities of healthy children transitioning through puberty. J. Investig. Dermatol. 2022, 142, 212–219. [Google Scholar] [CrossRef]
- Oliveira, M.; Azevedo, L. Molecular markers: An overview of data published for fungi over the last ten years. J. Fungi 2022, 8803, 2022. [Google Scholar] [CrossRef]
- Priyamvada, H.; Singh, R.K.; Akila, M.; Ravikrishna, R.; Verma, R.S.; Gunthe, S.S. Seasonal variation of the dominant allergenic fungal aerosols—One year study from southern Indian Region. Sci. Rep. 2017, 7, 11171. [Google Scholar] [CrossRef] [Green Version]
- Norros, V.; Rannik, Ü.; Hussein, T.; Petäjä, T.; Vesala, T.; Ovaskainen, O. Do small spores disperse further than large spores? Ecology 2014, 95, 1612–1621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winck, J.; Delgado, L.; Murta, R.; Lopez, M.; Marques, J. Antigen characterization of major cork molds in Suberosis (cork worker’s pneumonitis) by immunoblotting. Allergy 2004, 59, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Suphioglu, C.; Singh, M.B.; Taylor, P.; Knox, R.B.; Bellomo, R.; Holmes, P.; Puy, R. Mechanism of grass-pollen-induced asthma. Lancet 1992, 339, 569–572. [Google Scholar] [CrossRef] [PubMed]
- Bongomin, F.; Gago, S.; Oladele, R.O.; Denning, D.W. Global and multi-national prevalence of fungal diseases-estimate precision. J. Fungi 2017, 3, 57. [Google Scholar] [CrossRef] [PubMed]
- Wardlaw, A. Allergic fungal airway disease is a distinct endotype of difficult-to-treat asthma. J. Allergy Clin. Immunol. Pract. 2021, 9, 4268–4269. [Google Scholar] [CrossRef] [PubMed]
- Wardlaw, A.J.; Rick, E.M.; Pur Ozyigit, L.; Scadding, A.; Gaillard, E.A.; Pashley, C.H. New perspectives in the diagnosis and management of allergic fungal airway disease. J. Asthma Allergy 2021, 14, 557–573. [Google Scholar] [CrossRef]
- Arbes, S.; Gergen, P.; Elliott, L.; Zeldin, D. Prevalence of positive skin test responses to 10 common allergens in the US population: Results from the third National Health and Nutrition Examination Survey. J. Allergy Clin. Immunol. 2005, 116, 377–383. [Google Scholar] [CrossRef]
- Pongracic, J.A.; O’Connor, G.T.; Muilenberg, M.L.; Vaughn, B.; Gold, D.R.; Kattan, M.; Morgan, W.J.; Gruchalla, R.S.; Smartt, E.; Mitchell, H.E. Differential effects of outdoor versus indoor fungal spores on asthma morbidity in inner-city children. J. Allergy Clin. Immunol. 2010, 125, 593–599. [Google Scholar] [CrossRef] [Green Version]
- Roy, S.; Chakraborty, A.; Maitra, S.; Bhattacharya, K. Monitoring of airborne fungal spore load in relation to meteorological factors, air pollutants and allergic symptoms in Farakka, an unexplored biozone of eastern India. Environ. Monit. Assess. 2017, 189, 1–14. [Google Scholar] [CrossRef]
- Simon-Nobbe, B.; Denk, U.; Pöll, V.; Rid, R.; Breitenbach, M. The spectrum of fungal allergy. Int. Arch. Allergy Immunol. 2008, 145, 58–86. [Google Scholar] [CrossRef] [Green Version]
- Zeng, Y.; Xue, X.; Cai, H.; Zhu, G.; Zhu, M.; Wang, J.; Song, X.; Mo, Y.; Gao, X.; Zhou, J.; et al. Clinical Characteristics and Prognosis of Allergic Bronchopulmonary Aspergillosis: A Retrospective Cohort Study. J. Asthma Allergy 2022, 15, 53. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.R.; Patel, A.R.; Singh, S.; Singh, S.; Khawaja, I. Diagnosing allergic bronchopulmonary aspergillosis: A review. Cureus 2019, 11, e4550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beltrão, M.; Ferreira, A.R.; Pereira, A.M.; Sokhatska, O.; Amorim, A.; Delgado, L. Specific IgE and IgG to Aspergillus fumigatus antigens in the diagnosis of allergic bronchopulmonary aspergillosis. Rev. Port. Imunoalergol. 2021, 29, 243–252. [Google Scholar]
- Hew, M.; Douglass, J.; Tay, T.; Hehir, R. Allergic bronchopulmonary aspergillosis, hypersensitivity pneumonitis, and epidemic thunderstorm asthma. In Middleton’s Allergy E-Book: Principles and Practice; Elsevier Health Sciences: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Patel, A.R.; Patel, A.R.; Singh, S.; Singh, S.; Khawaja, I. Treating allergic bronchopulmonary aspergillosis: A review. Cureus 2019, 11, e4538. [Google Scholar] [CrossRef] [Green Version]
- Jack, J.; Bajaj, T. Allergic Bronchopulmonary Aspergillosis, StatPearls Publishing. 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK542329/ (accessed on 14 January 2023).
- Baluku, J.; Nuwagira, E.; Bongomin, F.; Denning, D. Pulmonary TB and chronic pulmonary aspergillosis: Clinical differences and similarities. Int. J. Tuberc. Lung Dis. 2021, 25, 537–546. [Google Scholar] [CrossRef]
- Iqbal, N.; Sheikh, M.; Jabeen, K.; Awan, S.; Irfan, M. Allergic bronchopulmonary aspergillosis misdiagnosed as smear negative pulmonary tuberculosis; a retrospective study from Pakistan. Ann. Med. Surg. 2021, 72, 10304. [Google Scholar] [CrossRef]
- Ekeng, B.E.; Davies, A.A.; Osaigbovo, I.I.; Warris, A.; Oladele, R.O.; Denning, D.W. Pulmonary and extrapulmonary manifestations of fungal infections misdiagnosed as tuberculosis: The need for prompt diagnosis and management. J. Fungi 2022, 8, 460. [Google Scholar] [CrossRef]
- Rosenberg, M.; Patterson, R.; Mintzer, R.; Cooper, B.J.; Roberts, M.; Harris, K.E. Clinical and immunologic criteria for the diagnosis of allergic bronchopulmonary aspergillosis. Ann. Intern. Med. 1977, 86, 405–414. [Google Scholar] [CrossRef]
- Schwartz, H.; Greenberger, P. The prevalence of allergic bronchopulmonary aspergillosis in patients with asthma, determined by serologic and radiologic criteria in patients at risk. J. Lab. Clin. Med. 1991, 117, 138–142. [Google Scholar]
- Agarwal, R.; Chakrabarti, A.; Shah, A.; Gupta, D.; Meis, J.F.; Guleria, R.; Moss, R.; Denning, D.W. Allergic bronchopulmonary aspergillosis: Review of literature and proposal of new diagnostic and classification criteria. Clin. Exp. Allergy 2013, 43, 850–873. [Google Scholar] [CrossRef]
- Agarwal, R.; Muthu, V.; Sehgal, I.S.; Dhooria, S.; Prasad, K.T.; Aggarwal, A.N. Allergic bronchopulmonary aspergillosis. Clin. Chest. Med. 2022, 43, 99–125. [Google Scholar] [CrossRef]
- Eraso, I.; Sangiovanni, S.; Morales, E.; Fernández-Trujillo, L. Use of monoclonal antibodies for allergic bronchopulmonary aspergillosis in patients with asthma and cystic fibrosis: Literature review. Ther. Adv. Respir. Dis. 2020, 14, 1753466620961648. [Google Scholar] [CrossRef] [PubMed]
- Moreira, A.; Silva, D.; Ferreira, A.; Delgado, L. Antifungal treatment in allergic bronchopulmonary aspergillosis with and without cystic fibrosis: A systematic review. Clin. Exp. Allergy 2014, 44, 1210–1227. [Google Scholar] [CrossRef] [PubMed]
- Periselneris, J.; Nwankwo, L.; Schelenz, S.; Shah, A.; Armstrong-James, D. Posaconazole for the treatment of allergic bronchopulmonary aspergillosis in patients with cystic fibrosis. Antimicrob. Chemother. 2019, 74, 1701–1703. [Google Scholar] [CrossRef] [PubMed]
- Terashima, T.; Shinozaki, T.; Iwami, E.; Nakajima, T.; Matsuzaki, T. A case of allergic bronchopulmonary aspergillosis successfully treated with mepolizumab. BMC Pulm. Med. 2018, 18, 53. [Google Scholar] [CrossRef]
- Parisi, G.F.; Portale, A.; Papale, M.; Tardino, L.; Rotolo, N.; Licari, A.; Leonardi, S. Successful treatment with omalizumab of allergic bronchopulmonary aspergillosis in patients with cystic fibrosis: Case reports and literature review. J. Allergy Clin. Immunol. Pract. 2019, 7, 1636–1638. [Google Scholar] [CrossRef]
- Soeda, S.; Kono, Y.; Tsuzuki, R.; Yamawaki, S.; Katsube, O.; To, M.; To, Y. Allergic bronchopulmonary aspergillosis successfully treated with benralizumab. J. Allergy Clin. Immunol. Pract. 2019, 7, 1633–1635. [Google Scholar] [CrossRef]
- Ramonell, R.; Lee, F.; Swenson, C.; Kuruvilla, M. Dupilumab treatment for allergic bronchopulmonary aspergillosis: A case series. J. Allergy Clin. Immunol. Pract. 2020, 8, 742–743. [Google Scholar] [CrossRef]
- Calhoun, W. Effect of omalizumab on exacerbations and glucocorticoid use in patients with allergic bronchopulmonary aspergillosis: A systematic review and meta-analysis. Am. J. Respir. Crit. Care Med. 2022, 205, A1235. [Google Scholar]
- Manti, S.; Giallongo, A.; Parisi, G.F.; Papale, M.; Mulè, E.; Aloisio, D.; Rotolo, N.; Leonardi, S. Biologic drugs in treating allergic bronchopulmonary aspergillosis in patients with cystic fibrosis: A systematic review. Eur. Resp. Rev. 2022, 31, 220011. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, A.; Agarwal, K.; Kathuria, S.; Gaur, S.N.; Randhawa, H.S.; Meis, J.F. Allergic bronchopulmonary mycosis due to fungi other than Aspergillus: A global overview. Crit. Rev. Microbiol. 2014, 40, 30–48. [Google Scholar] [CrossRef] [PubMed]
- Sehgal, I.S.; Choudhary, H.; Dhooria, S.; Aggarwal, A.N.; Bansal, S.; Garg, M.; Behera, D.; Chakrabarti, A.; Agarwal, R. Prevalence of sensitization to Aspergillus flavus in patients with allergic bronchopulmonary aspergillosis. Med. Mycol. 2019, 57, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Masaki, K.; Fukunaga, K.; Matsusaka, M.; Kabata, H.; Tanosaki, T.; Mochimaru, T.; Kamatani, T.; Ohtsuka, K.; Baba, R.; Ueda, S.; et al. Characteristics of severe asthma with fungal sensitization. Ann. Allergy Asthma Immunol. 2017, 119, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Tiwary, M.; Samarasinghe, A. Initiation and pathogenesis of severe asthma with fungal sensitisation. Cells 2021, 10, 913. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R. Severe asthma with fungal sensitisation. Curr. Allergy Asthma Rep. 2011, 11, 403. [Google Scholar] [CrossRef] [PubMed]
- Rapeport, W.; Ito, K.; Denning, D. The role of antifungals in the management of patients with severe asthma. Clin. Transl. Allergy 2020, 10, 46. [Google Scholar] [CrossRef]
- Chung, K.F.; Wenzel, S.E.; Brozek, J.L.; Bush, A.; Castro, M.; Sterk, P.J.; Adcock, I.M.; Bateman, E.D.; Bel, E.H.; Bleecker, E.R.; et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur. Resp. J. 2014, 43, 343–373. [Google Scholar] [CrossRef] [Green Version]
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. 2022. Available online: https://ginasthma.org/ (accessed on 14 January 2023).
- Denning, D.W.; O’Driscoll, B.R.; Powell, G.; Chew, F.; Atherton, G.T.; Vyas, A.; Miles, J.; Morris, J.; Niven, R.M. Randomized controlled trial of oral antifungal treatment for severe asthma with fungal sensitization: The Fungal Asthma Sensitization Trial (FAST) study. Am. J. Resp. Crit. Care Med. 2009, 179, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Wark, P.; Hussaini, S.; Holder, C.; Powell, H.; Gibson, P.; Oldmeadow, C. Omalizumab is an effective intervention in severe asthma with fungal sensitization. J. Allergy Clin. Immunol. Pract. 2020, 8, 3428–3433. [Google Scholar] [CrossRef]
- Dhariwal, J.; Hearn, A.P.; Kavanagh, J.E.; d’Ancona, G.; Green, L.; Fernandes, M.; Thomson, L.; Roxas, C.; Kent, B.D.; Nanzer, A.M.; et al. Real-world effectiveness of anti–IL-5/5R therapy in severe atopic eosinophilic asthma with fungal sensitization. J. Allergy Clin. Immunol. Pract. 2021, 9, 2315–2320. [Google Scholar] [CrossRef]
- Moss, R. Severe fungal asthma: A role for biologics and inhaled antifungals. J. Fungi 2023, 9, 85. [Google Scholar] [CrossRef]
- Kevat, A. Thunderstorm asthma: Looking back and looking forward. J. Asthma Allergy 2020, 13, 293. [Google Scholar] [CrossRef] [PubMed]
- Idrose, N.S.; Dharmage, S.C.; Lowe, A.J.; Lambert, K.A.; Lodge, C.J.; Abramson, M.J.; Douglass, J.A.; Newbigin, E.J.; Erbas, B. A systematic review of the role of grass pollen and fungi in thunderstorm asthma. Environ. Res. 2020, 181, 108911. [Google Scholar] [CrossRef] [PubMed]
- Price, D.; Hughes, K.; Thien, F.; Suphioglu, C. Epidemic thunderstorm asthma: Lessons learned from the storm down-under. J. Allergy Clin. Immunol. 2021, 9, 1510–1515. [Google Scholar] [CrossRef] [PubMed]
- Hughes, K.; Price, D.; Suphioglu, C. Importance of allergen–environment interactions in epidemic thunderstorm asthma. Ther. Adv. Respir. Dis. 2022, 16, 17534666221099733. [Google Scholar] [CrossRef] [PubMed]
- Harun, N.; Lachapelle, P.; Douglass, J. Thunderstorm-triggered asthma: What we know so far. J. Asthma Allergy 2019, 12, 101–108. [Google Scholar] [CrossRef] [Green Version]
- Australian Institute of Health and Welfare. Allergic Rhinitis (‘Hay Fever’). 2020. Available online: https://www.aihw.gov.au/reports/chronic-respiratory-conditions/allergic-rhinitis-hay-fever/contents/allergic-rhinitis (accessed on 14 January 2023).
- Xu, Y.; Xue, T.; Li, H.; Guan, K. Retrospective analysis of epidemic thunderstorm asthma in children in Yulin, Northwest China. Pediatr. Res. 2021, 4, 958–961. [Google Scholar] [CrossRef]
- Thien, F.; Beggs, P.J.; Csutoros, D.; Darvall, J.; Hew, M.; Davies, J.M.; Bardin, P.G.; Bannister, T.; Barnes, S.; Bellomo, R.; et al. The Melbourne epidemic thunderstorm asthma event 2016: An investigation of environmental triggers, effect on health services, and patient risk factors. Lancet Planet. Health 2018, 2, e255–e263. [Google Scholar] [CrossRef]
- Saini, R.; Singh, V.; Saroj, S.K.; Chaudhary, A.K.; Kumar, R.; Siva, S.; Yadav, R.R.; Yadav, S.; Silky, S.; Gupta, D.K.; et al. Fungal rhinosinusitis: An overview. J. Natl. Med. Assoc. 2022, 16, 5–18. [Google Scholar] [CrossRef]
- Luong, A.U.; Chua, A.; Alim, B.M.; Olsson, P.; Javer, A. Allergic fungal rhinosinusitis: The role and expectations of biologics. J. Allergy Clin. Immunol. Pract. 2022, 10, 3156–3162. [Google Scholar] [CrossRef]
- Dolen, W. Risk factors for allergic Aspergillus sinusitis. Med. Mycol. 2006, 44 (Suppl. S1), S273–S275. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Kim, H.J.; Lee, J.W.; Yoon, Y.H.; Kim, Y.M.; Rha, K.S. Categorization and clinicopathological features of chronic rhinosinusitis with eosinophilic mucin in a Korean population. Clin. Exp. Otorhinolaryngol. 2015, 8, 39–45. [Google Scholar] [CrossRef]
- Hoyt, A.; Borish, L.; Gurrola, J.; Payne, S. Allergic fungal rhinosinusitis. J. Allergy Clin. Immunol. Pract. 2016, 4, 599–604. [Google Scholar] [CrossRef] [PubMed]
- Dutre, T.; Dousary, S.A.; Zhang, N.; Bachert, C. Allergic fungal rhinosinusitis—More than a fungal disease? J. Allergy Clin. Immunol. 2013, 132, 487–489. [Google Scholar] [CrossRef] [PubMed]
- Bent, J.; Kuhn, F. Diagnosis of allergic fungal sinusitis. Otolaryngol. Head Neck Surg. 1994, 111, 580–588. [Google Scholar] [CrossRef]
- Schubert, M. Fungal rhinosinusitis: Diagnosis and therapy. Curr. Allergy Asthma Rep. 2001, 1, 268–276. [Google Scholar] [CrossRef]
- Schubert, M. Allergic fungal sinusitis: Pathophysiology, diagnosis and management. Med. Mycol. 2009, 47 (Suppl. S1), S324–S330. [Google Scholar] [CrossRef] [Green Version]
- Orlandi, R.R.; Kingdom, T.T.; Smith, T.L.; Bleier, B.; DeConde, A.; Luong, A.U.; Poetker, D.M.; Soler, Z.; Welch, K.C.; Wise, S.K.; et al. International consensus statement on allergy and rhinology: Rhinosinusitis 2021. Int. Forum Allergy Rhinol. 2021, 11, 213–739. [Google Scholar] [CrossRef]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European position paper on rhinosinusitis and nasal polyps 2020. Rhinology 2020, 58 (Suppl. S29), 1–464. [Google Scholar] [CrossRef]
- Head, K.; Sharp, S.; Chong, L.Y.; Hopkins, C.; Philpott, C. Topical and systemic antifungal therapy for chronic rhinosinusitis. Cochrane Database Syst. Rev. 2018, 9, Cd012453. [Google Scholar] [CrossRef] [Green Version]
- Gan, E.C.; Thamboo, A.; Rudmik, L.; Hwang, P.H.; Ferguson, B.J.; Javer, A.R. Medical management of allergic fungal rhinosinusitis following endoscopic sinus surgery: An evidence-based review and recommendations. Int. Forum Allergy Rhinol. 2014, 4, 702–715. [Google Scholar] [CrossRef]
- Mabry, R.; Marple, B.; Folker, R.; Mabry, C. Immunotherapy for allergic fungal sinusitis: Three years’ experience. Otolaryngol. Head Neck Surg. 1998, 119, 648–651. [Google Scholar] [CrossRef]
- Mabry, R.; Mabry, C. Allergic fungal sinusitis: The role of immunotherapy. Otoloryngol. Clin. N. Am. 2000, 33, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Bachert, C.; Han, J.K.; Desrosiers, M.; Hellings, P.W.; Amin, N.; Lee, S.E.; Mullol, J.; Greos, L.S.; Bosso, J.V.; Laidlaw, T.M.; et al. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): Results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group phase 3 trials. Lancet 2019, 394, 1638–1650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gevaert, P.; Omachi, T.A.; Corren, J.; Mullol, J.; Han, J.; Lee, S.E.; Kaufman, D.; Ligueros-Saylan, M.; Howard, M.; Zhu, R.; et al. Efficacy and safety of omalizumab in nasal polyposis: 2 randomized phase 3 trials. J. Allergy Clin. Immunol. 2020, 146, 595–605. [Google Scholar] [CrossRef] [PubMed]
- Han, J.K.; Bachert, C.; Fokkens, W.; Desrosiers, M.; Wagenmann, M.; Lee, S.E.; Smith, S.G.; Martin, N.; Mayer, B.; Yancey, S.W.; et al. Mepolizumab for chronic rhinosinusitis with nasal polyps (SYNAPSE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Resp. Med. 2021, 9, 1141–1153. [Google Scholar] [CrossRef]
- Dalphin, J.; Gondouin, A. Rare causes and the spectrum of hypersensitivity pneumonitis. In Orphan Lung Diseases; Springer: Berlin/Heidelberg, Germany, 2015; pp. 457–472. [Google Scholar]
- Hirschmann, J.; Pipavath, S.; Godwin, J. Hypersensitivity pneumonitis: A historical, clinical, and radiologic review. Radiographics 2009, 29, 1921–1938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nogueira, R.; Melo, N.; Bastos, H.N.; Martins, N.; Delgado, L.; Morais, A.; Mota, P.C. Hypersensitivity pneumonitis: Antigen diversity and disease implications. Pulmonology 2019, 25, 97–108. [Google Scholar] [CrossRef]
- Freitas, C.; Lima, B.; Melo, N.; Mota, P.; Novais-Bastos, H.; Alves, H.; Sokhatska, O.; Delgado, L.; Morais, A. Distinct TNF-alpha and HLA polymorphisms associate with fibrotic and non-fibrotic subtypes of hypersensitivity pneumonitis. Pulmonology 2021. [Google Scholar] [CrossRef]
- Raghu, G.; Remy-Jardin, M.; Ryerson, C.J.; Myers, J.L.; Kreuter, M.; Vasakova, M.; Bargagli, E.; Chung, J.H.; Collins, B.F.; Bendstrup, E.; et al. Diagnosis of hypersensitivity pneumonitis in adults. An official ATS/JRS/ALAT clinical practice guideline. Am. J. Resp. Crit. Care Med. 2020, 202, e36–e69. [Google Scholar] [CrossRef]
- Fernández Pérez, E.R.; Travis, W.D.; Lynch, D.A.; Brown, K.K.; Johannson, K.A.; Selman, M.; Ryu, J.H.; Wells, A.U.; Tony Huang, Y.C.; Pereira, C.A.C.; et al. Executive Summary: Diagnosis and Evaluation of Hypersensitivity Pneumonitis: CHEST Guideline and Expert Panel Report. Chest 2021, 160, 595–615. [Google Scholar] [CrossRef] [PubMed]
- Buendia-Roldan, I.; Aguilar-Duran, H.; Johannson, K.; Selman, M. Comparing the performance of two recommended criteria for establishing a diagnosis for hypersensitivity pneumonitis. Am. J. Resp. Crit. Care Med. 2021, 204, 865–868. [Google Scholar] [CrossRef] [PubMed]
- Walsh, S.L.; Wells, A.U.; Poletti, V.; Dubini, A.; Piciucchi, S.; Bendstrup, E.; Madsen, L.B.; Rasmussen, F.; Grutters, J.C.; Seldenrijk, K.; et al. A multicentre evaluation of inter-multidisciplinary team agreement for diagnosis in diffuse lung disease, In C102. Stategies to understand ild: Registries, prognostic indicators and more. Am. J. Respir. Crit. Care Med. 2016, 193, A6211. [Google Scholar]
- Cano-Jiménez, E.; Acuña, A.; Botana, M.I.; Hermida, T.; González, M.G.; Leiro, V.; Martín, I.; Paredes, S.; Sanjuán, P. Farmer’s lung disease. A review. Arch. Bronconeumol. 2016, 52, 321–328. [Google Scholar] [CrossRef]
- Cano-Jiménez, E.; Rubal, D.; Pérez de Llano, L.A.; Mengual, N.; Castro-Añón, O.; Méndez, L.; Golpe, R.; Sanjuán, P.; Martín, I.; Veres, A. Farmer’s lung disease: Analysis of 75 cases. Med. Clin. 2017, 149, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Hayes, J.; Rooney, J. The prevalence of respiratory symptoms among mushroom workers in Ireland. Occup. Med. 2014, 64, 533–538. [Google Scholar] [CrossRef] [Green Version]
- Tsushima, K.; Fujimoto, K.; Yoshikawa, S.; Kawakami, S.; Koizumi, T.; Kubo, K. Hypersensitivity pneumonitis due to Bunashimeji mushrooms in the mushroom industry. Int. Arch. Allergy Immunol. 2005, 137, 241–248. [Google Scholar] [CrossRef]
- Ampere, A.; Delhaes, L.; Soots, J.; Bart, F.; Wallaert, B. Hypersensitivity pneumonitis induced by Shiitake mushroom spores. Med. Mycol. 2012, 50, 654–657. [Google Scholar] [CrossRef]
- Bekci, T.; Calik, M.; Calik, S.; Esme, H. Oyster mushrooms (Pleurotus ostreatus) caused hypersensitivity pneumonitis: Mushroom worker’s lung. Eur. Resp. J. 2014, 44 (Suppl. S58), P4023. [Google Scholar]
- Ficociello, B.; Masciarelli, E.; Casorri, L.; Cichelli, A.; Pacioni, G. The onset of occupational diseases in mushroom cultivation and handling operators: A review. Ital. J. Mycol. 2019, 48, 26–38. [Google Scholar]
- Morais, A.; Winck, J.C.; Delgado, I.; Palmares, M.C.; Fonseca, J.; e Sá, J.M.; Marques, J.A. Suberosis and bird fancier’s disease: A comparative study of radiological, functional and bronchoalveolar lavage profiles. J. Allergy Clin. Immunol. Pract. 2004, 14, 26–33. [Google Scholar]
- Morell, F.; Roger, A.; Cruz, M.; Munoz, X.; Rodrigo, M. Suberosis: Clinical study and new etiologic agents in a series of eight patients. Chest 2003, 124, 1145–1152. [Google Scholar] [CrossRef] [Green Version]
- Ávila, R.; Lucas, J.M.G.; Araújo, A.T.; Lacey, J.; Heitor, M.C.; Mendes, E.M. Estudo epidemiológico da doença respiratória dos operários da indústria da cortiça. O Médico 1973, 1146, 257. [Google Scholar]
- Emanuel, D.; Lawton, B.; Wenzel, F. Maple-bark disease: Pneumonitis due to Coniosporium corticale. N. Engl. J. Med. 1962, 266, 333–337. [Google Scholar] [CrossRef]
- Emanuel, D.; Wenzel, F.; Lawton, B. Pneumonitis due to Cryptostroma corticale (maple-bark disease). N. Engl. J. Med. 1966, 274, 1413–1418. [Google Scholar] [CrossRef] [PubMed]
- Cohen, H.; Merigan, T.; Kosek, J.; Eldridge, F. Sequoiosis: A granulomatous pneumonitis associated with redwood sawdust inhalation. Am. J. Med. 1967, 43, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Chan-Yeung, M.; Abboud, R. Occupational asthma due to California redwood (Sequoia sempervirens) dusts. Am. Rev. Respir. Dis. 1976, 114, 1027–1031. [Google Scholar]
- Schlueter, D.; Fink, J.; Hensley, G. Wood-pulp workers’ disease: A hypersensitivity pneumonitis caused by Alternaria. Ann. Intern. Med. 1972, 77, 907–914. [Google Scholar] [CrossRef] [Green Version]
- Popp, W.; Ritschka, L.; Zwick, H.; Rauscher, H. Berry sorter’s lung or wine grower’s lung--an exogenous allergic alveolitis caused by Botrytis cinerea spores. Prax. Und Klin. Der Pneumol. 1987, 41, 165–169. [Google Scholar]
- Riddle, H.F.V.; Channell, S.; Blyth, W.; Weir, D.M.; Lloyd, M.; Amos, W.M.G.; Grant, I.W.B. Allergic alveolitis in a maltworker. Thorax 1968, 23, 271–280. [Google Scholar] [CrossRef] [Green Version]
- Channell, S.; Blyth, W.; Lloyd, M.; Weir, D.M.; Amos, W.M.G.; Littlewood, A.P.H.; Riddle, F.V.; Grant, I.W.B. Allergic alveolitis in maltworkers: A clinical, mycological, and immunological study. QJM 1969, 38, 351–353. [Google Scholar]
- Riddle, H. Prevalence of respiratory symptoms and sensitisation by mold antigens among a group of maltworkers. Occup. Environ. Med. 1974, 31, 31–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammar, S. Extrinsic allergic alveolitis. In Pulmonary Pathology; Springer: Berlin/Heidelberg, Germany, 1994; pp. 597–614. [Google Scholar]
- Walusiak, J.; Palczynski, C.; Hanke, W.; Wittczak, T.; Krakowiak, A.; Górski, P. The risk factors of occupational hypersensitivity in apprentice bakers–the predictive value of atopy markers. Int. Arch. Occup. Environ. Health 2002, 75, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.; Kryda, M.; Treuhaft, M.; Marx, L.; Roberts, R. Cheese worker’s hypersensitivity pneumonitis. Am. Rev. Respir. Dis. 1983, 127, 495–496. [Google Scholar] [CrossRef] [PubMed]
- Guglielminetti, M.; Valoti, E.; Cassini, P.; Taino, G.; Caretta, G. Respiratory syndrome very similar to extrinsic allergic alveolitis due to Penicillium verrucosum in workers in a cheese factory. Mycopathol 2001, 149, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Bringgold, W.; Halliday, S. The cheese whiz lung: Hypersensitivity pneumonitis in an imitation cheese factory worker. Chest 2020, 158, A1821. [Google Scholar] [CrossRef]
- Rouzaud, P.; Soulat, J.M.; Trela, C.; Fraysse, P.; Recco, P.; Carles, P.; Lauque, D. Symptoms and serum precipitins in workers exposed to dry sausage mould: Consequences of exposure to sausage mould. Int. Arch. Occup. Environ. Health. 2001, 74, 371–374. [Google Scholar] [CrossRef] [Green Version]
- Moise, L.; Barbu, B.; Rașcu, A. Extrinsic allergic alveolitis induced by spores of Penicillium in a salami factory worker. Rom. J. Intern. Med. 2018, 69, 22–26. [Google Scholar] [CrossRef] [Green Version]
- Zagà, V.; Dell’Omo, M.; Murgia, N.; Mura, M. Tobacco worker’s lung: A neglected subtype of hypersensitivity pneumonitis. Lung 2021, 199, 13–19. [Google Scholar] [CrossRef]
- Cormier, Y.; Israël-Assayag, E.; Bédard, G.; Duchaine, C. Hypersensitivity pneumonitis in peat moss processing plant workers. Am. J. Resp. Crit. Care Med. 1998, 158, 412–417. [Google Scholar] [CrossRef]
- Patterson, R.; Mazur, N.; Roberts, M.; Scarpelli, D.; Semerdjian, R.; Harris, K.E. Hypersensitivity pneumonitis due to humidifier disease: Seek and ye shall find. Chest 1998, 114, 931–933. [Google Scholar] [CrossRef] [PubMed]
- Caillaud, D.; Raobison, R.; Evrard, B.; Montcouquiol, S.; Horo, K. Domestic hypersensitivity pneumoniti. Rev. Mal. Respir. 2012, 29, 971–977. [Google Scholar] [CrossRef] [PubMed]
- Ando, M.; Suga, M.; Nishiura, Y.; Miyajima, M. Summer-type hypersensitivity pneumonitis. Intern. Med. 1995, 34, 707–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakajima, A.; Saraya, T.; Mori, T.; Ikeda, R.; Sugita, T.; Watanabe, T.; Fujiwara, M.; Takizawa, H.; Goto, H. Familial summer-type hypersensitivity pneumonitis in Japan: Two case reports and review of the literature. BMC Res. Notes 2013, 6, 371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lodha, S.; Maria, S.; Sharma, O. Hypersensitivity pneumonitis in a saxophone player. Chest 1988, 93, 1322. [Google Scholar] [CrossRef] [PubMed]
- Metersky, M.L.; Bean, S.B.; Meyer, J.D.; Mutambudzi, M.; Brown-Elliott, B.A.; Wechsler, M.E.; Wallace, R.J. Trombone player’s lung: A probable new cause of hypersensitivity pneumonitis. Chest 2010, 138, 754–756. [Google Scholar] [CrossRef]
- Metzger, F.; Haccuria, A.; Reboux, G.; Nolard, N.; Dalphin, J.C.; De Vuyst, P. Hypersensitivity pneumonitis due to molds in a saxophone player. Chest 2010, 138, 724–726. [Google Scholar] [CrossRef]
- King, J.; Richardson, M.; Quinn, A.; Holme, J.; Chaudhuri, N. Bagpipe lung; a new type of interstitial lung disease? Thorax 2017, 72, 380–382. [Google Scholar] [CrossRef] [Green Version]
- Pana, Z.; Roilides, E.; Warris, A.; Groll, A.; Zaoutis, T. Epidemiology of invasive fungal disease in children. JPIDS 2017, 6 (Suppl. S1), S3–S11. [Google Scholar] [CrossRef] [Green Version]
- Lionakis, M. Primary immunodeficiencies and invasive fungal infection: When to suspect and how to diagnose and manage. Curr. Opin. Infect. Dis. 2019, 32, 531–537. [Google Scholar] [CrossRef]
- Elaziz, D.A.; El-Ghany, M.A.; Meshaal, S.; Hawary, R.E.; Lotfy, S.; Galal, N.; Ouf, S.A.; Elmarsafy, A. Fungal infections in primary immunodeficiency diseases. Clin. Immunol. 2020, 219, 108553. [Google Scholar] [CrossRef] [PubMed]
- Cifaldi, C.; Ursu, G.M.; D’Alba, I.; Paccoud, O.; Danion, F.; Lanternier, F.; Chiriaco, M. Main human inborn errors of immunity leading to fungal infections. Clin. Microbiol. Infect. 2022, 28, 1435–1440. [Google Scholar] [CrossRef] [PubMed]
- Schmiedel, Y.; Zimmerli, S. Common invasive fungal diseases: An overview of invasive candidiasis, aspergillosis, cryptococcosis, and Pneumocystis pneumonia. Swiss Med. Wkly. 2016, 146, w14281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ochoa, S.; Constantine, G.; Lionakis, M. Genetic susceptibility to fungal infection in children. Curr. Opin. Pediat. 2020, 32, 780–789. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.D.; Denning, D.W.; Gow, N.A.; Levitz, S.M.; Netea, M.G.; White, T.C. Hidden killers: Human fungal infections. Sci. Transl. Med. 2012, 4, 165rv13. [Google Scholar] [CrossRef] [Green Version]
- Morris, A.; Norris, K. Colonization by Pneumocystis jirovecii and its role in disease. Clin. Microbiol. Rev. 2012, 25, 297–317. [Google Scholar] [CrossRef] [Green Version]
- Lehman, H.; Gordon, C. The skin as a window into primary immune deficiency diseases: Atopic dermatitis and chronic mucocutaneous candidiasis. J. Allergy Clin. Immunol. Pract. 2019, 7, 788–798. [Google Scholar] [CrossRef]
- McCusker, C.; Upton, J.; Warrington, R. Primary immunodeficiency. Allergy Asthma Clin. Immunol. 2018, 14, 1–12. [Google Scholar] [CrossRef]
- Guarner, J. Human immunodeficiency virus and fungal infections. Sem. Diagn. Pathol. 2017, 34, 325–331. [Google Scholar] [CrossRef]
- Tangye, S.G.; Al-Herz, W.; Bousfiha, A.; Cunningham-Rundles, C.; Franco, J.L.; Holland, S.M.; Klein, C.; Morio, T.; Oksenhendler, E.; Picard, C.; et al. Human inborn errors of immunity: 2022 update on the classification from the international union of immunological societies expert committee. J. Clin. Immunol. 2022, 42, 1473–1507. [Google Scholar] [CrossRef]
- Bousfiha, A.; Moundir, A.; Tangye, S.G.; Picard, C.; Jeddane, L.; Al-Herz, W.; Rundles, C.C.; Franco, J.L.; Holland, S.M.; Klein, C.; et al. The 2022 update of IUIS phenotypical classification for human inborn errors of immunity. J. Clin. Immunol. 2022, 42, 1508–1520. [Google Scholar] [CrossRef] [PubMed]
- Redmond, M.; Scherzer, R.; Prince, B. Novel genetic discoveries in primary immunodeficiency disorders. Clin. Rev. Allergy Immunol. 2022, 2022, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Lanternier, F.; Cypowyj, S.; Picard, C.; Bustamante, J.; Lortholary, O.; Casanova, J.L.; Puel, A. Primary immunodeficiencies underlying fungal infections. Curr. Opin. Pediatr. 2013, 25, 736. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, M.L.; Albuquerque, P.C. Searching for a change: The need for increased support for public health and research on fungal diseases. PLoS Negl. Trop. Dis. 2018, 12, e0006479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burki, T. WHO publish fungal priority pathogens list. Lancet Microbe 2023, 4, E74. [Google Scholar] [CrossRef] [PubMed]
- Rokas, A. Evolution of the human pathogenic lifestyle in fungi. Nat. Microbiol. 2022, 7, 607–619. [Google Scholar] [CrossRef]
- Kaeuffer, C.; Baldacini, M.; Ruge, T.; Ruch, Y.; Zhu, Y.-J.; De Cian, M.; Philouze, G.; Bachellier, P.; Denis, J.; Lefebvre, N.; et al. Fungal Infections Caused by Kazachstania spp., Strasbourg, France, 2007–2020. Emerg. Infect. Dis. 2022, 28, 30. [Google Scholar] [CrossRef]
- Alagha, R.; Tham, S.M.; Chew, K.L.; Cheng, J.W.S.; Lian, D.W.; Vathsala, A.; Lum, L.H.W. Volvariella volvacea brain abscess in an immunocompromised host—An emerging fungal pathogen in Asia. J. Med. Mycol. 2022, 32, 101272. [Google Scholar] [CrossRef]
- Laga, A.; Crothers, J.; Cañete-Gibas, C.; Wiederhold, N.; Solomon, I. Rigidoporus corticola colonization and invasive fungal disease in immunocompromised patients, United States. Emerg. Infect. Dis. 2022, 28, 856. [Google Scholar] [CrossRef]
- Petrucelli, M.F.; de Abreu, M.H.; Cantelli, B.A.M.; Segura, G.G.; Nishimura, F.G.; Bitencourt, T.A.; Marins, M.; Fachin, A.L. Epidemiology and diagnostic perspectives of dermatophytoses. J. Fungi 2020, 6, 310. [Google Scholar] [CrossRef]
- Urban, K.; Chu, S.; Scheufele, C.; Giesey, R.L.; Mehrmal, S.; Uppal, P.; Delost, G.R. The global, regional, and national burden of fungal skin diseases in 195 countries and territories: A cross-sectional analysis from the Global Burden of Disease Study 2017. JAAD Int. 2021, 2, 22–27. [Google Scholar] [CrossRef]
- Havlickova, B.; Czaika, V.; Friedrich, M. Epidemiological trends in skin mycoses worldwide. Mycoses 2008, 51, 2–15. [Google Scholar] [CrossRef] [PubMed]
- Seth, D.; Cheldize, K.; Brown, D.; Freeman, E. Global burden of skin disease: Inequities and innovations. Curr. Dermatol. Rep. 2017, 6, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Al-Khikani, F.; Ayit, A. Major challenges in dermatophytosis treatment: Current options and future visions. Egypt J. Dermatol. Venerol. 2021, 41, 1. [Google Scholar] [CrossRef]
- Moskaluk, A.; VandeWoude, S. Current topics in Dermatophyte classification and clinical diagnosis. Pathogens 2022, 11, 957. [Google Scholar] [CrossRef]
- Oke, O.; Onayemi, O.; Olasode, O.; Omisore, A.; Oninla, O. The prevalence and pattern of superficial fungal infections among school children in Ile-Ife, South-Western Nigeria. Dermatol. Res. Pract. 2014, 2014, 842917. [Google Scholar] [CrossRef] [Green Version]
- Cornet, L.; D’hooge, E.; Magain, N.; Stubbe, D.; Packeu, A.; Baurain, D.; Becker, P. The taxonomy of the Trichophyton rubrum complex: A phylogenomic approach. Microb. Genom. 2021, 7, 000707. [Google Scholar] [CrossRef]
- Rashidian, S.; Falahati, M.; Kordbacheh, P.; Mahmoudi, M.; Safara, M.; Tafti, H.S.; Mahmoudi, S.; Zaini, F. A study on etiologic agents and clinical manifestations of dermatophytosis in Yazd, Iran. Curr. Med. Mycol. 2015, 1, 20. [Google Scholar] [CrossRef] [Green Version]
- Son, J.H.; Doh, J.Y.; Han, K.; Kim, Y.H.; Han, J.H.; Bang, C.H.; Park, Y.M.; Lee, J.H. Risk factors of dermatophytosis among Korean adults. Sci. Rep. 2022, 12, 13444. [Google Scholar]
- Jazdarehee, A.; Malekafzali, L.; Lee, J.; Lewis, R.; Mukovozov, I. Transmission of onychomycosis and dermatophytosis between household members: A scoping review. J. Fungi 2022, 8, 60. [Google Scholar] [CrossRef]
- Hayette, M.; Sacheli, R. Dermatophytosis, Trends in Epidemiology and Diagnostic Approach. Curr. Fungal. Infect. Rep. 2015, 9, 164–179. [Google Scholar] [CrossRef]
- Rinaldi, M. Dermatophytosis: Epidemiological and microbiological update. J. Am. Acad. Dermatol. 2000, 43, S120–S124. [Google Scholar] [CrossRef] [PubMed]
- Park, B.J.; Taguchi, H.; Kamei, K.; Matsuzawa, T.; Hyon, S.H.; Park, J.C. In vitro antifungal activity of epigallocatechin 3-O-gallate against clinical isolates of dermatophytes. Yonsei Med. J. 2011, 52, 535–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponte, T. Epigallocatechin-3-Gallate Antimycotic and Azole Resistant Modulator Potential against Resistant Fungi. Ph.D. Thesis, Instituto Politécnico de Lisboa, Escola Superior de Tecnologia da Saúde de Lisboa, Lisboa, Portugal, 2021. [Google Scholar]
- Khosravi, R.A.; Shokri, H.; Farahnejat, Z.; Chalangari, R.; Katalin, M. Antimycotic efficacy of Iranian medicinal plants towards dermatophyte obtained from patients with dermatophytosis. Chin. J. Nat. Med. 2013, 11, 43–48. [Google Scholar] [CrossRef]
- Mousavi, S.; Kazemi, A. In vitro and in vivo antidermatophytic activities of some Iranian medicinal plants. Med. Mycol. 2015, 53, 852–859. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez, J.; Pico, A.; Álvarez, E.; Acevedo, R. Meta-analysis of the antifungal activities of three essential oils as alternative therapies in dermatophytosis infections. J. App. Microbiol. 2022, 133, 241–253. [Google Scholar] [CrossRef]
- Puel, A. Human inborn errors of immunity underlying superficial or invasive candidiasis. Hum. Genet. 2020, 139, 1011–1022. [Google Scholar] [CrossRef]
- Vila, T.; Sultan, A.; Montelongo-Jauregui, D.; Jabra-Rizk, M. Oral candidiasis: A disease of opportunity. J. Fungi 2020, 6, 15. [Google Scholar] [CrossRef] [Green Version]
- Richardson, J.; Naglik, J. Special issue: Mucosal fungal infections. J. Fungi 2018, 4, 43. [Google Scholar] [CrossRef] [Green Version]
- Hu, L.; He, C.; Zhao, C.; Chen, X.; Hua, H.; Yan, Z. Characterization of oral candidiasis and the Candida species profile in patients with oral mucosal disease. Microb. Pathog. 2019, 134, 103575. [Google Scholar] [CrossRef]
- Quindós, G.; Gil-Alonso, S.; Marcos-Arias, C.; Sevillano, E.; Mateo, E.; Jauregizar, N.; Eraso, E. Therapeutic tools for oral candidiasis: Current and new antifungal drugs. Med. Oral. Patol. Oral. Cir. Bucal. 2019, 24, e172. [Google Scholar] [CrossRef]
- Lu, S. Oral candidiasis: Pathophysiology and best practice for diagnosis, classification, and successful management. J. Fungi 2021, 7, 555. [Google Scholar] [CrossRef] [PubMed]
- Sardi, J.C.O.; Silva, D.R.; Anibal, P.C.; de Campos Baldin, J.J.C.M.; Ramalho, S.R.; Rosalen, P.L.; Macedo, M.L.R.; Hofling, J.F. Vulvovaginal candidiasis: Epidemiology and risk factors, pathogenesis, resistance, and new therapeutic options. Curr. Fungal. Infect. Rep. 2021, 15, 32–40. [Google Scholar] [CrossRef]
- Nama, Z.; AL-Janabi, A.; AbdulWahid, H.; AL-Janabi, A. Vulvovaginal candidiasis: The infection should explain itself. Int. J. 2021, 4, 261. [Google Scholar]
- Talapko, J.; Juzbašić, M.; Matijević, T.; Pustijanac, E.; Bekić, S.; Kotris, I.; Škrlec, I. Candida albicans—The virulence factors and clinical manifestations of infection. J. Fungi 2021, 7, 79. [Google Scholar] [CrossRef]
- Jafarzadeh, L.; Ranjbar, M.; Nazari, T.; Naeimi Eshkaleti, M.; Aghaei Gharehbolagh, S.; Sobel, J.D.; Mahmoudi, S. Vulvovaginal candidiasis: An overview of mycological, clinical, and immunological aspects. J. Obstet. Gynaecol. Res. 2022, 48, 1546–1560. [Google Scholar] [CrossRef]
- Wray, A.A.; Velasquez, J.; Khetarpal, S. Balanitis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Errichetti, E.; Lallas, A.; Di Stefani, A.; Apalla, Z.; Kyrgidis, A.; Lacarrubba, F.; Micali, G.; Galvan, A.; Piaserico, S.; Stinco, G. Accuracy of dermoscopy in distinguishing erythroplasia of Queyrat from common forms of chronic balanitis: Results from a multicentric observational study. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 966–972. [Google Scholar] [CrossRef]
- Rodrigues, C.; Rodrigues, M.; Henriques, M. Promising alternative therapeutics for oral candidiasis. Curr. Med. Chem. 2019, 24, 2515–2528. [Google Scholar] [CrossRef]
- Ferreira, E.S.; Rosalen, P.L.; Benso, B.; Sardi, J.C.O.; Denny, C.; de Sousa, S.A.; Guerra, F.Q.S.; Lima, E.O.; Freires, I.A.; de Castro, R.D. The use of essential oils and their isolated compounds for the treatment of oral candidiasis: A literature review. Evid. -Based Complement. Altern. Med. 2021, 2021, 1059274. [Google Scholar] [CrossRef]
- Ferreira, P.S.; Victorelli, F.D.; Rodero, C.F.; Fortunato, G.C.; Araújo, V.H.S.; Fonseca-Santos, B.; Bauab, T.M.; Van Dijck, P.; Chorilli, M. p-Coumaric acid loaded into liquid crystalline systems as a novel strategy to the treatment of vulvovaginal candidiasis. Int. J. Pharm. 2021, 603, 120658. [Google Scholar] [CrossRef]
- Anwar, S.; Elmonaem, S.; Moussa, E.; Aboulela, A.; Essawy, M. Curcumin nanoparticles: The topical antimycotic suspension treating oral candidiasis. Odontology 2022, 603, 120658. [Google Scholar] [CrossRef]
- Sobel, J.; Nyirjesy, P. Oteseconazole: An advance in treatment of recurrent vulvovaginal candidiasis. Future Microbiol. 2012, 16, 1453–1461. [Google Scholar] [CrossRef] [PubMed]
- Barnes, K.; Yancey, A. Ibrexafungerp in the treatment of vulvovaginal candidiasis. Ann. Pharmacother. 2022, 57, 10600280221091301. [Google Scholar] [CrossRef] [PubMed]
- Fabri, R.L.; Freitas, J.C.O.; Lemos, A.S.O.; Campos, L.M.; Diniz, I.O.M.; Pinto, N.C.C.; Silva, T.P.; Palazzi, C.; Marchesini, P.; Monteiro, C.; et al. Spilanthol as a promising antifungal alkylamide for the treatment of vulvovaginal candidiasis. Med. Mycol. 2021, 59, 1210–1224. [Google Scholar] [CrossRef] [PubMed]
- Neto, A.S.O.; Souza, I.L.A.; Amorim, M.E.S.; Souza, T.F.; Rocha, V.N.; do Couto, R.O.; Fabri, R.L.; Araújo, M.G.F. Antifungal efficacy of atorvastatin-containing emulgel in the treatment of oral and vulvovaginal candidiasis. Med. Mycol. 2021, 59, 476–485. [Google Scholar] [CrossRef] [PubMed]
- Vahedpoor, Z.; Abastabar, M.; Sehat, M.; Talebian, P.; Fini, T.F.; Dastanpour, Z.; Haghani, I.; Chelongarian, R.; Nazeri, M. Vaginal and oral use of probiotics as adjunctive therapy to fluconazole in patients with vulvovaginal candidiasis: A clinical trial on iranian women. Curr. Med. Mycol. 2021, 7, 36. [Google Scholar] [CrossRef]
- Bonifaz, A.; Tirado-Sánchez, A.; Jaramillo-Manzur CAraiza, J.; Fierro-Arias, L. Candida balanitis. Clinical and mycological study about the efficacy of a single-day oral treatment with itraconazole (400 mg). Nasza Dermatol. Online 2020, 11, 1–5. [Google Scholar] [CrossRef]
- Chin, L.; Parvinnejad, N.; Haber, R. Pityriasis in dermatology: An updated review. Int. J. Dermatol. 2021, 60, 141–158. [Google Scholar] [CrossRef]
- Karray, M.; McKinney, W. Tinea Versicolor. 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK482500/ (accessed on 14 January 2023).
- Bansal, L.; Dhiman, A. A brief review of fungal infection-pityriasis versicolor. EAS J. Med. Surg. 2022, 4, 19–23. [Google Scholar] [CrossRef]
- Emery, D.; Denning, D. The global distribution of actinomycetoma and eumycetoma. PLOS Negl. Trop Dis. 2020, 14, e0008397. [Google Scholar] [CrossRef]
- Méndez-Tovar, F. Eumycetoma and Global Warming. In The Impact of Climate Change on Fungal Disease; Springer: Berlin/Heidelberg, Germany, 2022; pp. 99–113. [Google Scholar]
- Siddig, E.E.; Ahmed, A.; Ali, Y.; Bakhiet, S.M.; Mohamed, N.S.; Ahmed, E.S.; Fahal, A.H. Eumycetoma medical treatment: Past, current practice, latest advances and perspectives. Microbiol. Res. 2021, 12, 899–906. [Google Scholar] [CrossRef]
- Hao, X.; Cognetti, M.; Burch-Smith, R.; Mejia, E.; Mirkin, G. Mycetoma: Development of diagnosis and treatment. J. Fungi 2022, 8, 743. [Google Scholar] [CrossRef] [PubMed]
- Nyuykonge, B.; Lim, W.; van Amelsvoort, L.; Bonifaz, A.; Fahal, A.; Badali, H.; Abastabar, M.; Verbon, A.; van de Sande, W. Eumycetoma causative agents are inhibited in vitro by luliconazole, lanoconazole and ravuconazole. Mycoses 2022, 65, 650–655. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.; Chandra, S.; Jayanthi, M.; Shirahatti, P.; Ramu, R. Role of medicinal plants in the treatment of eumycetoma: A review. J. App. Biol. Biotechnol. 2021, 9, 1–8. [Google Scholar]
- Brito, A.; Bittencourt, M. Chromoblastomycosis: An etiological, epidemiological, clinical, diagnostic, and treatment update. An. Bras. De Dermatol. 2018, 93, 495–506. [Google Scholar] [CrossRef] [PubMed]
- Santos, D.W.C.L.; Azevedo, C.M.P.S.; Vicente, V.A.; Queiroz-Telles, F.; Rodrigues, A.M.; de Hoog, G.S.; Denning, D.W.; Colombo, A.L. The global burden of chromoblastomycosis. PLoS Negl. Trop. Dis. 2021, 15, e0009611. [Google Scholar] [CrossRef] [PubMed]
- Damayanti, N.; Noor, L.; Purwanto, H.; Siswati, A. Diagnosis and therapy of chromoblastomycosis. J. Pak. Assoc. Dermatol. 2022, 32, 443–448. [Google Scholar]
- Lian, X.; Scott-Thomas, A.; Lewis, J.G.; Bhatia, M.; MacPherson, S.A.; Zeng, Y.; Chambers, S.T. Monoclonal antibodies and invasive aspergillosis: Diagnostic and therapeutic perspectives. Int. J. Mol. Sci. 2022, 23, 55. [Google Scholar] [CrossRef]
- Chakraborty, R.; Baradhi, K. Aspergilloma. 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK546668/ (accessed on 14 January 2023).
- Jenks, J.; Nam, H.; Hoenigl, M. Invasive aspergillosis in critically ill patients: Review of definitions and diagnostic approaches. Mycoses 2021, 64, 1002–1014. [Google Scholar] [CrossRef]
- Kluge, S.; Strauß, R.; Kochanek, M.; Weigand, M.A.; Rohde, H.; Lahmer, T. Aspergillosis: Emerging risk groups in critically ill patients. Med. Mycol. 2022, 60, myab064. [Google Scholar] [CrossRef]
- Vuong, M.; Waymack, J. Aspergillosis. 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK482241/ (accessed on 14 January 2023).
- Chamilos, G.; Kontoyiannis, D. Defining the diagnosis of invasive aspergillosis. Med. Mycol. 2006, 44 (Suppl. S1), S163–S173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vrinceanu, D.; Dumitru, M.; Patrascu, O.M.; Costache, A.; Papacocea, T.; Cergan, R. Current diagnosis and treatment of rhinosinusal aspergilloma. Exp. Ther. Med. 2021, 22, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Pappas, P.; Lionakis, M.; Arendrup, M.; Ostrosky-Zeichner, L.; Kullberg, B. Invasive candidiasis. Nat. Ver. Dis. Primers 2018, 4, 1–20. [Google Scholar] [CrossRef] [PubMed]
- McCarty, T.; White, C.; Pappas, P. Candidemia and invasive candidiasis. Infect. Dis. Clin. 2021, 35, 389–413. [Google Scholar] [CrossRef]
- Ben-Ami, R. Treatment of invasive candidiasis: A narrative review. J. Fungi 2018, 4, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clancy, C.; Nguyen, M. Diagnosing invasive candidiasis. J. Clin. Microbiol. 2018, 56, e01909–e01917. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Lara, M.; Ostrosky-Zeichner, L. Invasive candidiasis. Semin. Respir. Crit. Care Med. 2020, 41, 3–12. [Google Scholar] [CrossRef]
- Camp, I.; Spettel, K.; Willinger, B. Molecular methods for the diagnosis of invasive candidiasis. J. Fungi 2020, 6, 101. [Google Scholar] [CrossRef]
- Zavala, S.; Baddley, J. Cryptococcosis. Semin Respir. Crit. Care Med. 2020, 41, 69–79. [Google Scholar] [CrossRef]
- Sousa, H.; Frazão, S.; Júnior, G.; Albuquerque, P.; Nicola, A. Cryptococcal virulence in humans: Learning from translational studies with clinical isolates. Front. Cel. Infect. Microbiol. 2021, 11, 657502. [Google Scholar] [CrossRef]
- Francisco, E.; Jong, A.; Hagen, F. Cryptococcosis and Cryptococcus. Mycopathol 2021, 186, 729–731. [Google Scholar] [CrossRef]
- Bandalizadeh, Z.; Javidnia, J.; Hossein, S.A.; Moosazadeh, M.; Amouei, A.; Kermani, F.; Seyedmousavi, S.; Shokohi, T. Cryptococcus and cryptococcosis in Iran during 1969–2019: A systematic review and meta-analysis. J. Mycol. Med. 2020, 30, 100917. [Google Scholar] [CrossRef] [PubMed]
- Giro, A. Review on Cryptococcus disease. J. Trop Dis. 2021, 9, 288. [Google Scholar]
- Maziarz, E.; Perfect, J. Cryptococcosis. Infect. Dis. Clin. 2016, 30, 179–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kashef Hamadani, B.H.; Franco-Paredes, C.; McCollister, B.; Shapiro, L.; Beckham, J.D.; Henao-Martínez, A.F. Cryptococcosis and cryptococcal meningitis: New predictors and clinical outcomes at a United States academic medical centre. Mycoses 2018, 61, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Gushiken, A.; Saharia, K.; Baddley, J. Cryptococcosis. Infect. Dis. Clin. 2021, 35, 493–514. [Google Scholar] [CrossRef]
- Mazi, P.; Rauseo, A.; Spec, A. Blastomycosis. Infect. Dis. Clin. 2021, 35, 515–530. [Google Scholar] [CrossRef]
- Miceli, A.; Krishnamurthy, K. Blastomycosis. 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK441987/ (accessed on 14 January 2023).
- Lee, P.P.; Lau, Y.L. Cellular and molecular defects underlying invasive fungal infections-revelations from endemic mycoses. Front. Immunol. 2017, 8, 735. [Google Scholar] [CrossRef] [Green Version]
- Murray, P.R.; Rosenthal, K.S.; Pfaller, M.A. Systemic Mycoses Caused by Dimorphic Fungi-Blastomycosis. In Medical Microbiology; Elsevier: Amsterdam, The Netherlands, 2020; pp. 634–636. [Google Scholar]
- Pullen, M.; Alpern, J.; Bahr, N. Blastomycosis—Some progress but still much to learn. J. Fungi 2022, 8, 824. [Google Scholar] [CrossRef]
- Leedy, N.; Ribes, J.; Soria, J.; Myint, T. Risk factors of severe blastomycosis and comparison of diagnosis and outcomes between immunocompetent and immunocompromised patients. Mycoses 2021, 65, 239–246. [Google Scholar]
- Linder, K.; Kauffman, C. Current and new perspectives in the diagnosis of blastomycosis and histoplasmosis. J. Fungi 2020, 7, 12. [Google Scholar] [CrossRef]
- Brineman, R.; Nichols, L. Educational case: Coccidioidomycosis. Acad. Pathol. 2022, 9, 100042. [Google Scholar] [CrossRef] [PubMed]
- Crum, N. Coccidioidomycosis: A contemporary review. Infect. Dis. Ther. 2022, 11, 713–742. [Google Scholar] [CrossRef]
- Williams, S.; Chiller, T. Update on the epidemiology, diagnosis, and treatment of Coccidioidomycosis. J. Fungi 2022, 8, 666. [Google Scholar] [CrossRef] [PubMed]
- Nemade, S.; Shinde, K. Coccidioidomycosis. In Granulomatous Diseases in Otorhinolaryngology, Head and Neck; Springer: Berlin/Heidelberg, Germany, 2021; pp. 165–171. [Google Scholar]
- Azar, M.; Loyd, J.; Relich, R.; Wheat, L.; Hage, C. Current concepts in the epidemiology, diagnosis, and management of histoplasmosis syndromes. Semin. Respir. Crit. Care Med. 2020, 41, 13–30. [Google Scholar] [CrossRef]
- Toscanini, M.; Nusblat, A.; Cuestas, M. Diagnosis of histoplasmosis: Current status and perspectives. App. Microbiol. Biotechnol. 2021, 105, 1837–1859. [Google Scholar] [CrossRef] [PubMed]
- Roy, M.; Park, B.; Chiller, T. Donor-derived fungal infections in transplant patients. Curr. Fungal. Infect. Rep. 2010, 4, 219–228. [Google Scholar] [CrossRef]
- Azar, M.; Hage, C. Clinical perspectives in the diagnosis and management of histoplasmosis. Clin. Chest. Med. 2017, 38, 403–415. [Google Scholar] [CrossRef]
- Wheat, L.; Conces, D.; Allen, S.; Blue-Hnidy, D.; Loyd, J. Pulmonary histoplasmosis syndromes: Recognition, diagnosis, and management. Sem. Resp. Crit. Care Med. 2004, 25, 129–144. [Google Scholar] [CrossRef]
- Samaddar, A.; Sharma, A. Emergomycosis, an emerging systemic mycosis in immunocompromised patients: Current trends and future prospects. Front. Med. 2021, 8, 670731. [Google Scholar] [CrossRef]
- Gnat, S.; Łagowski, D.; Nowakiewicz, A.; Dyląg, M. A global view on fungal infections in humans and animals: Infections caused by dimorphic fungi and dermatophytoses. J. App. Microbiol. 2021, 131, 2688–2704. [Google Scholar] [CrossRef] [PubMed]
- Reddy, D.; Nel, J.; Govender, N. Emergomycosis. J. Med. Mycol. 2022, 33, 101313. [Google Scholar] [CrossRef] [PubMed]
- Martinez, R. Epidemiology of paracoccidioidomycosis. Rev. Inst. Med. Trop. Sao Paulo 2015, 57, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Wagner, G.; Moertl, D.; Glechner, A.; Mayr, V.; Klerings, I.; Zachariah, C.; Van den Nest, M.; Gartlehner, G.; Willinger, B. Paracoccidioidomycosis diagnosed in Europe—A systematic literature review. J. Fungi 2021, 7, 157. [Google Scholar] [CrossRef] [PubMed]
- Queiroz-Telles, F.; Pietrobom, P.; Júnior, M.; Baptista, R.; Peçanha, P. New insights on pulmonary paracoccidioidomycosis. Semin. Respir. Crit. Care Med. 2020, 41, 53–68. [Google Scholar] [CrossRef]
- Hahn, R.C.; Hagen, F.; Mendes, R.P.; Burger, E.; Nery, A.F.; Siqueira, N.P.; Guevara, A.; Rodrigues, A.M.; de Camargo, Z.P. Paracoccidioidomycosis: Current status and future trends. Clin. Microbiol. Rev. 2022, 35, e00233. [Google Scholar] [CrossRef] [PubMed]
- Shikanai-Yasuda, M. Paracoccidioidomycosis treatment. Rev. Inst. Med. Trop. Sao Paulo 2015, 57, 31–37. [Google Scholar] [CrossRef] [Green Version]
- Savarese, L.; Monsignore, L.; Hernandes, M.; Martinez, R.; Nogueira-Barbosa, M. Magnetic resonance imaging findings of paracoccidioidomycosis in the musculoskeletal system. Trop. Med. Int. Health 2015, 20, 1346–1354. [Google Scholar] [CrossRef] [Green Version]
- Cao, C.; Xi, L.; Chaturvedi, V. Talaromycosis (penicilliosis) due to Talaromyces (Penicillium) marneffei: Insights into the clinical trends of a major fungal disease 60 years after the discovery of the pathogen. Mycopathologia 2019, 184, 709–720. [Google Scholar] [CrossRef]
- Le, T.; Thanh, N.; Thwaites, G. Talaromycosis (Penicilliosis). In Hunter’s Tropical Medicine and Emerging Infectious Diseases; Elsevier: Amsterdam, The Netherlands, 2020; pp. 682–685. [Google Scholar]
- Narayanasamy, S.; Dat, V.Q.; Thanh, N.T.; Ly, V.T.; Chan, J.F.-W.; Yuen, K.-Y.; Ning, C.; Liang, H.; Li, L.; Chowdhary, A.; et al. A global call for talaromycosis to be recognised as a neglected tropical disease. Lancet Glob. Health 2021, 9, e1618–e1622. [Google Scholar] [CrossRef]
- Narayanasamy, S.; Dougherty, J.; Doorn, H.; Le, T. Pulmonary talaromycosis: A window into the immunopathogenesis of an endemic mycosis. Mycopathologia 2021, 186, 707–715. [Google Scholar] [CrossRef] [PubMed]
- Moretti, M.L.; Busso-Lopes, A.F.; Tararam, C.A.; Moraes, R.; Muraosa, Y.; Mikami, Y.; Gonoi, T.; Taguchi, H.; Lyra, L.; Reichert-Lima, F.; et al. Airborne transmission of invasive fusariosis in patients with hematologic malignancies. PLoS ONE 2018, 13, e0196426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batista, B.; Chaves, M.; Reginatto, P.; Saraiva, O.; Fuentefria, A. Human fusariosis: An emerging infection that is difficult to treat. Rev. Soc. Bras. Med. Trop. 2020, 53, e20200013. [Google Scholar] [CrossRef]
- Vadhan, J.; Melo, A.; Shogan, J.; Singh, V.; Carrillo, M. Fast and Fusariosis: A systematic review and case report of a rapidly fatal central nervous system infection. J. Emerg. Crit. Care Med. 2022, 2022, 1–7. [Google Scholar] [CrossRef]
- Nucci, M.; Barreiros, G.; Akiti, T.; Anaissie, E.; Nouér, S. Invasive fusariosis in patients with hematologic diseases. J. Fungi 2021, 7, 815. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, M.W.; Katragkou, A.; Iosifidis, E.; Roilides, E.; Walsh, T.J. Recent advances in the treatment of scedosporiosis and fusariosis. J. Fungi 2018, 4, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hospenthal, D. Hyalohyphomycosis: Infection Due to Hyaline Molds. In Diagnosis and Treatment of Fungal Infections; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Hasan, N. Human hyalohyphomycoses: A review of human infections due to Acremonium spp., Paecilomyces spp., Penicillium spp., Talaromyces spp., and Scopulariopsis spp. In Antifungal Therapy; CRC Press: Boca Raton, FL, USA, 2019; pp. 325–335. [Google Scholar]
- Jenks, J.D.; Seidel, D.; Cornely, O.A.; Chen, S.; van Hal, S.; Kauffman, C.; Miceli, M.H.; Heinemann, M.; Christner, M.; Jover Sáenz, A.; et al. Clinical characteristics and outcomes of invasive Lomentospora prolificans infections: Snalysis of patients in the FungiScope® registry. Mycoses 2020, 63, 437–442. [Google Scholar] [CrossRef]
- Konsoula, A.; Tsioutis, C.; Markaki, I.; Papadakis, M.; Agouridis, A.P.; Spernovasilis, N. Lomentospora prolificans: An emerging opportunistic fungal pathogen. Microorganisms 2022, 10, 1317. [Google Scholar] [CrossRef]
- Chen, S.; Halliday, C.; Hoenigl, M.; Cornely, O.; Meyer, W. Scedosporium and Lomentospora infections: Contemporary microbiological tools for the diagnosis of invasive disease. J. Fungi 2021, 7, 23. [Google Scholar] [CrossRef]
- Prakash, H.; Chakrabarti, A. Global epidemiology of mucormycosis. J. Fungi 2019, 5, 26. [Google Scholar] [CrossRef] [Green Version]
- Troiano, G.; Nante, N. Mucormycosis—Emerging fungal threats. Encyclopedia 2022, 2, 247–255. [Google Scholar] [CrossRef]
- Skiada, A.; Pavleas, I.; Drogari-Apiranthitou, M. Epidemiology and diagnosis of mucormycosis: An update. J. Fungi 2020, 6, 265. [Google Scholar] [CrossRef] [PubMed]
- Arcobello, J.; Revankar, S. Phaeohyphomycosis. Semin. Respir. Crit. Care Med. 2020, 41, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Kieselová, K.; Gomes, T.; Santiago, F.; Martinha, H. Emerging cutaneous phaeohyphomycosis caused by Alternaria infectoria. Acta. Med. Port. 2021, 34, 774–778. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Cissé, O.; Kovacs, J. A molecular window into the biology and epidemiology of Pneumocystis spp. Clin. Microbiol. Rev. 2018, 13, e00009-18. [Google Scholar]
- Schmidt, J.J.; Lueck, C.; Ziesing, S.; Stoll, M.; Haller, H.; Gottlieb, J.; Eder, M.; Welte, T.; Hoeper, M.M.; Scherag, A.; et al. Clinical course, treatment and outcome of Pneumocystis pneumonia in immunocompromised adults: A retrospective analysis over 17 years. Crit. Care 2018, 22, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Bro, K. Is Pneumocystis Jirovecii Transmitted by the Airborne Route? Am. J. Infect. Control. 2022, 50, S18. [Google Scholar] [CrossRef]
- Gingerich, A.; Norris, K.; Mousa, J. Pneumocystis pneumonia: Immunity, vaccines, and treatments. Pathogens 2021, 10, 236. [Google Scholar] [CrossRef]
- Tasaka, S. Recent advances in the diagnosis and management of Pneumocystis pneumonia. Tuberc. Respir. Dis. 2020, 83, 132. [Google Scholar] [CrossRef] [Green Version]
- Ramírez-Soto, M.; Aguilar-Ancori, E.; Tirado-Sánchez, A.; Bonifaz, A. Ecological determinants of sporotrichosis etiological agents. J. Fungi 2018, 4, 95. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, A.; Hagen, F.; Camargo, Z. A spotlight on Sporothrix and sporotrichosis. Mycopathologia 2022, 187, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Nava-Pérez, N.; Neri-García, L.G.; Romero-González, O.E.; Terrones-Cruz, J.A.; García-Carnero, L.C.; Mora-Montes, H.M. Biological and clinical attributes of Sporothrix globosa, a causative agent of sporotrichosis. Infect. Drug. Res. 2022, 15, 2067–2090. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, A.M.; Gonçalves, S.S.; de Carvalho, J.A.; Borba-Santos, L.P.; Rozental, S.; Camargo, Z.P.D. Current progress on epidemiology, diagnosis, and treatment of sporotrichosis and their future trends. J. Fungi 2022, 8, 776. [Google Scholar] [CrossRef]
- Sizar, O.; Talati, R. Sporotrichosis. 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK532255/ (accessed on 16 January 2023).
- Gerfaud-Valentin, M.; Reboux, G.; Traclet, J.; Thivolet-Béjui, F.; Cordier, J.F.; Cottin, V. Occupational hypersensitivity pneumonitis in a baker: A new cause. Chest 2014, 145, 856–858. [Google Scholar] [CrossRef] [PubMed]
- Zingales, V.; Taroncher, M.; Martino, P.A.; Ruiz, M.J.; Caloni, F. Climate change and effects on molds and mycotoxins. Toxins 2022, 14, 445. [Google Scholar] [CrossRef]
- Siscar-Lewin, S.; Hube, B.; Brunke, S. Emergence and evolution of virulence in human pathogenic fungi. Trends Microbiol. 2022, 30, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Lakoh, S.; Kamudumuli, P.S.; Penney, R.O.S.; DLitt, S.M.H.; Jarvis, J.N.; Hassan, A.J.; Moudoute, N.L.E.; Ocansey, B.K.; Izco, S.; Kipkerich, S.; et al. Diagnostic capacity for invasive fungal infections in advanced HIV disease in Africa: A continent-wide survey. Lancet Infect. Dis. 2022. [Google Scholar] [CrossRef] [PubMed]
- Rayens, E.; Norris, K.A.; Cordero, J.F. Mortality trends in risk conditions and invasive mycotic disease in the United States, 1999–2018. Clin. Infect. Dis. 2022, 74, 309–318. [Google Scholar] [CrossRef]
- Bongomin, F.; Ekeng, B.E.; Kibone, W.; Nsenga, L.; Olum, R.; Itam-Eyo, A.; Kuate, M.P.N.; Pebolo, F.P.; Davies, A.A.; Manga, M. Invasive Fungal Diseases in Africa: A Critical Literature Review. J. Fungi 2022, 8, 1236. [Google Scholar] [CrossRef]
- Miller, S.A.; Ferreira, J.P.; LeJeune, J.T. Antimicrobial use and resistance in plant agriculture: A one health perspective. Agriculture 2022, 12, 289. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Disease | Etiological Agent | Risk Factors | Clinical Manifestations | Diagnosis | Treatment |
|---|---|---|---|---|---|
| Allergic Bronchopulmonary Aspergillosis | A. fumigatus A. terreus A. niger A. flavus | Asthma (2.5% asthmatic patients) Cystic fibrosis (1–15% of CF patients) | Worsening asthma Worsening cystic fibrosis Coughing paroxysms Mucoid impaction, with consolidation of the lung Recurrent ‘chest infections’ | Total IgE > 1000 KIU/L SPT or specific IgE positive for Af Fleeting or fixed pulmonary opacities on chest radiograph Continuing respiratory symptoms Af IgG antibodies Eosinophilia (>500 cells/μL in steroid naïve patients) Filamentous fungal growth in sputum cultures or bronchial lavage fluid Sputum or bronchoscopy samples with positive PCR for Af | Oral and inhaled corticosteroids Adjuntive oral antifungal medication (itraconazole, voriconazole) Biologicals (omalizumab, mepolizumab, benralizumab, dupilumab)—off label |
| Severe Asthma with Fungal Sensitization | A. fumigatus P. chrysogenum C. herbarum A. alternata C. albicans Trichophyton spp. | Rarely any underlying disease | Worsening asthma symptoms Need for a high dose of inhaled steroids and/or frequent courses of oral steroids | Low FEV1 or peak flow (usually persistently) Total IgE < 1000 KIU/L SPT or specific IgE test positive for any fungus High-resolution chest CT: normal or minor alterations | Similar to severe asthma Partial or absent treatment response: consider biologicals (omalizumab, mepolizumab, benralizumab) and antifungal drugs (itraconazol) |
| Thunderstorm asthma | Alternaria spp. Cladosporium spp. Diatrypaceae D. exitialis P. nigran Sporobolomyces spp. | Sensitization and exposure to aeroallergens (mainly pollen grains and fungal spores) Asthma Allergic rhinitis Age Gender Ethnicity | The same as asthma | The same as asthma | The same as asthma |
| Allergic fungal rhinosinusitis | A. fumigatus A. flavus B. spicifera C. lunata A. alternata Other dematiaceous fungi | Atopy | Nasal obstruction Loss of smell Nasal discharge Nasal crust Pressure sensation over the face sinus Double vision or visual loss (rare) Facial asymmetry and proptosis Sino–bronchial allergic mycosis syndrome | SPT or elevated fungal-specific IgE Imagological findings (CT or MRI of the sinuses): opacification with centrally hyperdense content, nasal polyposis Histopathology showing eosinophilic mucin without invasion into the sinus tissue Fungal hyphae in the mucus | Topical and oral corticosteroids Saline douching Sinus surgery Biologicals (dupilumab, omalizumab, mepolizumab) Allergen immunotherapy (?) Antifungal therapy (?) |
| Disease | Etiological Agents | Risk Factors |
|---|---|---|
| Farmer’s lung | Alternaria spp. A. fumigatus A. glaucus Botrytis spp. P. brevicompactum P. olivicolor | Handling damp hay Opening bales for feeding livestock Threshing moldy grain |
| Mushroom worker’s lung | A. bisporus H. tessellatus L. edodes P. ostreatus | Exposure in spawning sheds |
| Suberosis | P. glabrum C. sitophila | Handling of damp cork |
| Maple bark stripper’s lung | C. corticale | Stripping bark from logs |
| Sequoiosis | Graphium spp. Pullularia spp. A. pullulans | Breathing damp sawmill dust |
| Wood pulp worker’s lung | Alternaria spp. | Pulping contaminated wood |
| Malt worker’s lung | A. clavatus P. granulatum P. citrinum R. stolonifer | Handling moldy grain |
| Wine grower’s lung | B. cinerea | Mold contamination |
| Baker’s lung disease | A. fumigatus | Handling contaminated flour |
| Cheese worker’s lung | P. roqueforti P. casei P. notatum P. viridicutum A. fumigatus A. niger A. pullulans | Cleaning mold off cheese |
| Salami Brusher’s disease | P. glabrum P. camemberti P. nalgiovense A. fumigatus Cladosporium spp. | Cleaning the white mold growing on salami surface using a manual wire brush |
| Tobacco worker’s lung | A. fumigatus | Exposure to tobacco dust and molds dispersed in the air in cigarette production facilities |
| Peak moss worker’s lung | Monocillium spp. P. citreonigrum | Handling contaminated peat moss |
| Paprika slicer’s lung | M. stolonifer | Handling moldy paprika pods during slicing |
| Summer-type HP | T. cutaneum T. asahii T. mucoides | Exposure to damp housing and furniture materials |
| Humidifiers, heating, and ventilation systems | Aspergillus spp. Cladosporium spp. Penicillium spp. A. pullulans Cephalosporium spp. Mucor spp. Rhodoturula spp. | Humidifier ran continuously without cleaning and with water added periodically |
| PID | Inheritance | CMCC Incidence | Other Fungal Infections | Non-Fungal Infections | Noninfectious Complications | |
|---|---|---|---|---|---|---|
| Cellular and combined immunodeficiencies | SCID | X-linked or AR | 30–35% | Variable (e.g., PCP) | Bacteria, viruses and mycobacteria | |
| DOCK8 deficiency (AR-HIES) | AR | 53–64% | Histoplasmosis Cryptococcosis PCP | Staphylococcal infections, HSV, VZV, HPV, molluscum contagiosum virus | Eczema, food allergy and asthma, malignancies (lymphoma) | |
| PGM3 deficiency (AR-HIES) | AR | Variable | Variable | HSV, CMV | Eczema, asthma, neurologic impairment, leukocytoclastic vasculitis | |
| Defective Th17 immunity | STAT3 LOF mutation (AD-HIES) | AD | 80% | Aspergillosis Cryptococcosis Histoplasmosis | S. aureus | Eczema, pneumatoceles, coronary aneurisms, hyperextensible joints |
| STAT1 GOF mutation | AD | 100% | Histoplasmosis Coccidioidomycosis | HSV | Autoimmunity Cerebral and aortic aneurisms | |
| CARD9 deficiency | AR | Variable | Candida meningoencephalitis Deep dermatophytosis | None | None | |
| APECED | AD or AR | 90–100% | None | None | Hypoparathyroidism Adrenal insufficiency Vitiligo, alopecia, keratoconjunctivitis | |
| IL-17F mutation | AD | Variable | None | None | None | |
| IL-17RC mutation | AR | Variable | None | None | None | |
| IL-17RA and ACT1 mutations | AR | Variable | None | Staphylococcal infections (dermatitis and blepharitis) | None | |
| RORC mutation | AR | 90–100% | Disseminated mycobacterial infection | None | ||
| PID | Infections | ||||||
|---|---|---|---|---|---|---|---|
| Invasive Aspergillosis | Invasive Candidiasis | Dimorphic Fungi Infections | Cryptococcosis | Pneumocystis jirovecii Pneumonia | Deep Dermatophytosis | ||
| Phagocytic defects | CGD | High | Occasionally | - | - | - | - |
| LAD-1 | Occasionally | Occasionally | - | - | - | - | |
| Congenital neutropenia | Occasionally | Occasionally | - | - | - | - | |
| Cellular and combined deficiencies | SCID, CIDs (e.g., AR-HIES, X-linked HIGM, IPEX) | Occasionally | Variable susceptibility (e.g., IPEX) | Variable susceptibility to Histoplasmosis, mostly in AR-HIES (DOCK8 deficiency) and HIGM | Variable, mostly in AR-HIES (DOCK8 deficiency) and HIGM | High in patients with X-linked HIGM syndrome; variable in patients with SCID, AR-HIES, NEMO and MHC class II deficiency | - |
| Defective Th17 immunity | AD-HIES (STAT3) | High in patients with lung cavities | Occasionally | Histoplasmosis Coccidioidomycosis | Occasionally | - | - |
| STAT1 GOF mutation | . | - | Coccidioidomycosis Histoplasmosis | - | - | - | |
| CARD9 deficiency | . | Invasive CNS candidiasis | - | - | - | High | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliveira, M.; Oliveira, D.; Lisboa, C.; Boechat, J.L.; Delgado, L. Clinical Manifestations of Human Exposure to Fungi. J. Fungi 2023, 9, 381. https://doi.org/10.3390/jof9030381
Oliveira M, Oliveira D, Lisboa C, Boechat JL, Delgado L. Clinical Manifestations of Human Exposure to Fungi. Journal of Fungi. 2023; 9(3):381. https://doi.org/10.3390/jof9030381
Chicago/Turabian StyleOliveira, Manuela, Diana Oliveira, Carmen Lisboa, José Laerte Boechat, and Luís Delgado. 2023. "Clinical Manifestations of Human Exposure to Fungi" Journal of Fungi 9, no. 3: 381. https://doi.org/10.3390/jof9030381