1. Introduction
The term “phaeohyphomycosis” refers to subcutaneous, superficial, and systemic infections caused by pigmented (dematiaceous) fungi. There are over 100 species, and over 50 genera of these fungi, which have been associated with human disease [
1]. The presence of melanin in their cell walls is characteristic of the condition, and likely an important virulence factor, believed to be involved in evasion from the host immune response [
2]. Most human diseases caused by these fungi are noninvasive (e.g., onychomycosis, superficial cutaneous infection, chronic allergic fungal sinusitis) and associated with low mortality. However, rarely, phaeohyphomycosis can lead to invasive complications, including skin and subcutaneous disease, pneumonia, central nervous system (CNS) disease, fungemia, and multi-organ disseminated disease. Solid organ transplant (SOT) recipients are particularly at risk of invasive infections due to prolonged immunosuppression [
3,
4]. We describe three cases of phaeohyphomycosis caused by
Alternaria alternata,
Curvularia hawaiiensis, and
Alternaria infectoria in two heart recipients and one kidney recipient, respectively. Additionally, we provide a narrative review of the literature on phaeohyphomycosis infections occurring in SOT recipients over the last 10 years.
3. Results
3.1. Case 1
A 53-year-old male presented with a cutaneous lesion on the right leg 7 months after a heart transplant was performed for cardiac failure due to giant cell myocarditis. His clinical history was marked by acute cellular rejection at month 1 after the transplant, treated with steroid boluses. At the time of the skin lesion appearance, his immunosuppressive therapy was based on 15 mg of prednisone once daily, 750 mg of mycophenolate mofetil (MMF) twice daily, and tacrolimus (FK) with a trough level of around 14 ng/mL. The cutaneous lesion presented as a hard ulcerated nodule 1 cm in diameter draining purulent fluid (
Figure 1A). The lesion was scraped by the Infectious Disease and Dermatology team and was cultured. Two weeks after the mycelium was grown at 30 °C on a sabouraud chloramphenicol gentamicin agar plate, a scraping culture was made and after a microscopic examination, DNA extraction was performed. A polymerase chain reaction using 18S r-DNA revealed
Curvularia hawaiiensis and a topical therapy with bifonazole was started. The strain susceptibility assay was performed at the reference center (Università Cattolica-Policlinico Gemelli) with Sensititre™ YeastOne ITAMYUCC, (Thermo Fisher Scientific, Cleveland, OH, USA) broth micro-dilution, following CLSI methods for filamentous fungi [
5] (
Table 1). ESCMID and ECMM joint clinical guidelines were used for the results interpretation [
6].
After 4 weeks of topical therapy, there was no improvement in the cutaneous lesion, and the patient developed eyelid ptosis, so a total-body CT scan was performed over concern for cerebral dissemination. There was no evidence of cerebral involvement, but two undefined pulmonary nodules were noted in the right lung and one in the left. The cutaneous lesion was surgically removed, and a systemic therapy with 400 mg of itraconazole once daily commenced. The patient was informed to take itraconazole capsules with food and acid drinks to obtain adequate plasma concentrations. FK dosing was reduced by 60% with monitoring of the trough levels. The therapeutic drug monitoring of itraconazole, measured by HPLC, showed a trough level of 1.4 mg/L and a peak level of 1.9 mg/L; the administered dose was unchanged for the duration of the therapy. Two months later, there was no evidence of recurrence of the cutaneous lesions, and the pulmonary nodules at CT were unchanged. The therapy was administered for 4 months. At the 5-month follow-up the patient was stable, with no recurrence.
3.2. Case 2
A 63-year-old male, working as a tomato grower, presented with a cutaneous erythematous nodular lesion 8 months after a heart transplant. His immunosuppressive therapy consisted of 20 mg of prednisone daily, 500 mg of MMF twice daily, and tacrolimus with a trough level of around 8 ng/mL. His medical history included an acute cellular rejection, treated with steroid boluses at 2 months after the transplant.
The lesion, on his left thigh, was 1.5 cm in diameter with a crusty and ulcerated surface that had been growing in dimension over the previous 3 months, followed by 2 satellite lesions on the same limb (
Figure 1B). No pain or itching was present. The lesions were concerning for of a lymphoproliferative malignancy; as a result, an excisional biopsy was done. The histopathological examination showed no sign of malignancy, but a significant inflammatory pattern was found, with neutrophilic infiltrate and the presence of hyphae and yeast-like structures. Molecular biology (18s-rRNA) performed on the excisional biopsy from the lesions on the thigh identified
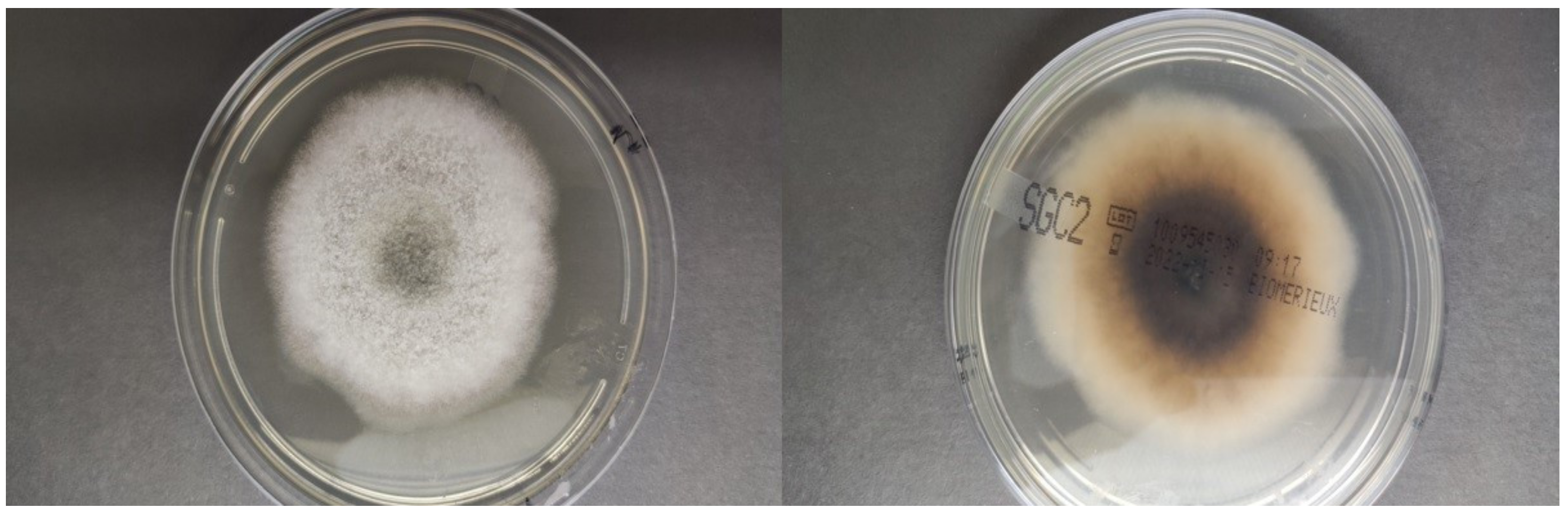
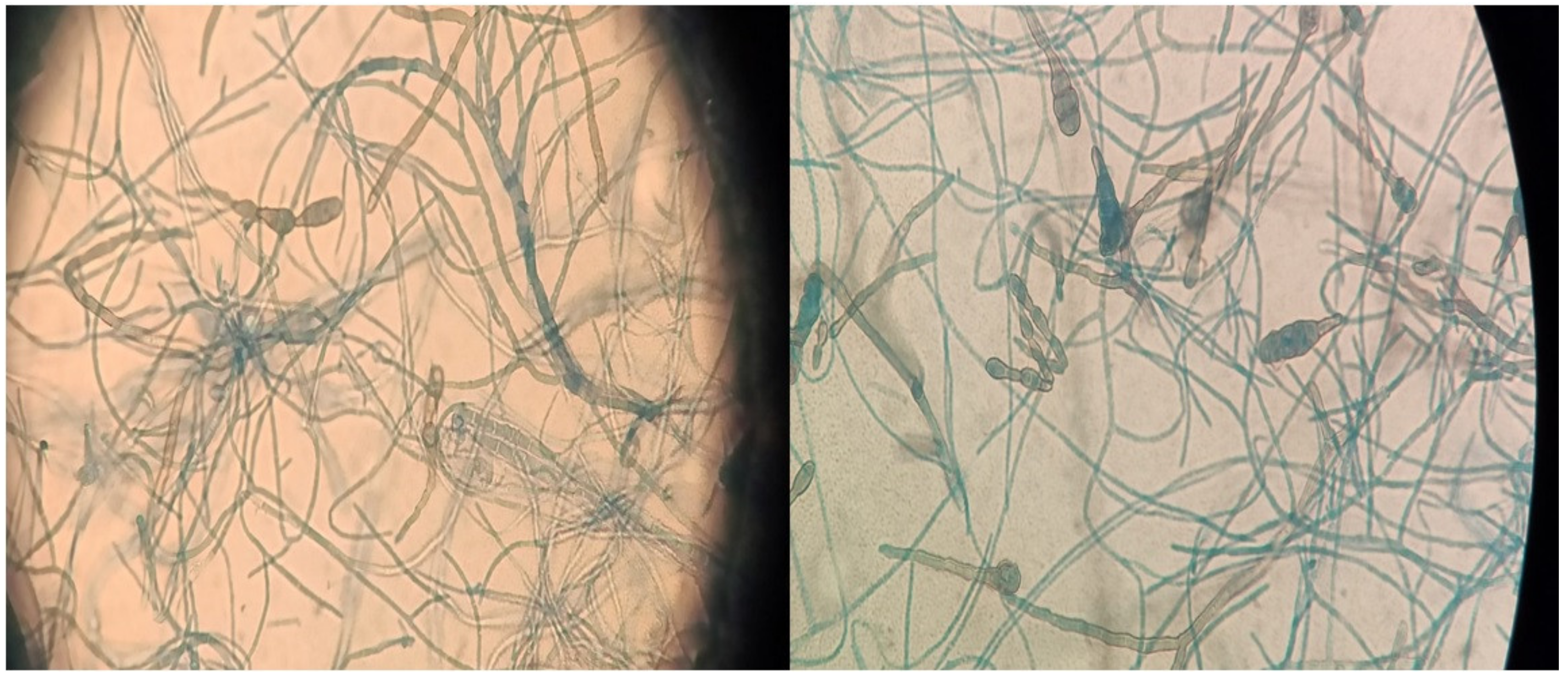
Alternaria alternata.A chest and brain CT scan was done, though no sign of dissemination was found. After the excisional biopsy, an oral therapy with isavuconazole was administered for 2 months, monitoring the FK trough levels. Four months after the cessation of therapy, the patient presented with two new cutaneous lesions on his forearms, which were surgically removed. A new histopathological examination found the same pattern as the first lesion, and
Alternaria alternata was identified again with molecular biology and culture (
Figure 2 and
Figure 3). The fungal isolate was sent for susceptibility testing to the reference center (Università Cattolica-Policlinico Gemelli). Based on the result of the susceptibility test [
5] (
Table 2), therapy with itraconazole commenced. Therapy was administered after meals, with lemon juice to improve the absorption. Monitoring of the trough level of itraconazole was done 7 days after starting the therapy, showing a trough level of 0.4 mg/L, which was under the therapeutic range (target range level between 0.5 and 1 mg/L), and the patient was told to take itraconazole 12 h apart from the therapy with the omeprazole he was taking simultaneously. The tacrolimus dose was reduced by 60%. Itraconazole was administered for 3 months. At the 6-month follow-up, there was no sign of new lesions or of dissemination.
3.3. Case 3
A 59-year-old male, working as a wheat farmer, with a history of kidney transplant for an IgA nephropathy performed 10 years prior, presented for a routine dermatological consult. His immunosuppressive therapy consisted of 500 mg of MMF twice daily, 2.5 mg of prednisone daily, and FK with a trough level of 6 ng/mL. A physical examination showed a lesion behind the ear and two other lesions, one on each knee (
Figure 1C). The lesions on the knees were two crusty painless nodules that had been growing for several months. The lesion behind the ears was surgically removed, and the histological examination showed pigmented basal cell carcinoma. Scraping was done from the knee lesions, which yielded
Alternaria infectoria as the species responsible for the infection. A total-body CT scan was done, and no other lesions were found. The lesions on the knees were surgically removed, and an inflammatory pattern was found at histological examination. No antifungal systemic therapy was administered, and no signs of relapse were found at the one-year follow-up.
3.4. Literature Review
A narrative review of the literature yielded a total of 66 published studies, with 94 cases from several countries (Argentina, Australia, Austria, Belgium, Brazil, China, Colombia, Czech Republic, France, French Antilles, Germany, Japan, India, Italy, Kuwait, Portugal, Singapore, Slovakia, Spain, Thailand, and the U.S.). We divided the cases into those reported from Europe (Eu
n = 36) and from other continents (Non-Eu
n = 58) (
Table 2). Among studies published outside Europe, 28 reports were from America, 26 were from Asia, and 4 were from Australia. Most of the cases (75%) were published between 2016 and 2022. A geographical distribution was noted, with 85% of the cases reported from countries with a mild or tropical climate. The majority of the cases in the EU were reported from Spain and France (
Table 2,
Table 3,
Table 4,
Table 5,
Table 6 and
Table 7).
3.5. Reported Cases from Europe vs. Outside Europe
Our literature review revealed a total of 94 cases, with 38% reported in the EU and 62% reported outside the EU. In total, 73% of the infections were reported in kidney transplants recipients, 14% were in lung transplants, 7.5% were in heart transplants, and 5.5% were in liver transplants. When comparing the EU and non-EU cases, lung transplant represented 36% and 0%, kidney transplant 45% and 91%, heart transplant 11% and 5%, and liver transplant 8% and 4%, respectively. Overall, the median age of patients at disease presentation was 56 years old (54 years old in EU vs. 58.5 in non-EU) and a male/female ratio of 3.5 in EU vs. 2.3 in other countries. The median time from transplant to diagnosis in months was 18, with no relevant differences all over the world. From all the reported cases, 70% were classified as “local,” 22% as “disseminated,” and 8% as “local deep”, with no differences between EU and non-EU countries.
We found approximately 40 different species of fungi causing phaeohyphomycosis in our review. Among cases with available pathogen identification, the most reported genus was Alternaria (19/81, 24%), followed by Exophiala (13/81, 16%) worldwide. In Europe, the causative microorganism was available in all of the cases; we found 16 different species of fungi, in most of the cases belonging to the genus Alternaria (44% of European cases), though Cladophialophora bantiana, Exophiala spp, and Medicopsis romeroi were commonly reported. Outside of Europe, in 52% of the reported cases, the identification of the pathogen was not available. In the remaining cases, over 30 different species of fungi were identified. Most cases involved the genus Exophiala (10/45, 22% of non-EU cases), though Alternaria spp. was also frequently reported. The identification of the pathogen was made using cultures in about 90% of the total cases (89% EU vs. 91% non-EU), while the use of molecular biology was reported in 58% of the cases (78% EU vs. 45% non-EU). In the remaining cases, an identification was made by direct microscopy or histological examination.
Susceptibility testing was done in 26.6% of the total cases. Susceptibilities to antifungal agents and treatment regimens were quite heterogeneous due to the variety of isolated species. Surgery was performed in 68% of total cases. In total, 10% of patients were treated with surgery alone, with no antifungal therapy, though this approach was more commonly reported in Europe (in 17% of EU cases vs. 5% of non-EU cases). The most used antifungal agents were voriconazole in Europe and itraconazole outside of Europe, followed by posaconazole and amphotericin B. The majority of patients (67%) were treated with a single antifungal agent (58% rate of monotherapy in EU vs. 72% in non-EU), and the rest with more than one agent, in sequential or combination therapy. The median length of antifungal therapy was 16 weeks, but in 41.5% of reports, the duration of therapy was not specified. Regarding the clinical outcome, recovery was reported in 81% of cases, with no relevant differences between EU (81%) and non-EU (85%). Five percent of patients died due to the fungal infection.
Table 3.
Reported cases in Europe.
Table 3.
Reported cases in Europe.
| Year | Ref | Country | Sex | Age | Dissemination | Location | Species | Method of Identification | Therapy | Duration of Therapy in Weeks | Surgery | Transplant | Outcome | Time Tx-Diagnosis in Months | Susceptibility
Test |
|---|
| 2019 | [7] | Spain | M | 58 | Local | Skin, foot | Alternaria alternata | Culture + molecular biology (18s-DNA, ITS 1 + ITS 4) | ITZ + VZL + TBF | 8 | No | Lung | FR | 42 | None |
| 2019 | [7] | Spain | M | 68 | Local deep | Foot tendon | Alternaria alternata | Culture + molecular biology (18s-DNA, ITS 1 + ITS 4) | Surgery | - | Yes | Lung | FR | 48 | None |
| 2019 | [7] | Spain | M | 32 | Local | Skin, legs, and wrist | Alternaria alternata | Culture + molecular biology (18s-DNA, ITS 1 + ITS 4) | ITZ | 24 | Yes | Lung | FR | 3 | None |
| 2015 | [8] | Portugal | M | 65 | Local | Skin, hand, and leg | Alternaria alternata | Culture + molecular biology (ITS 1 + ITS 4) | ITZ | 12 | Yes | Liver | FR | 6 | None |
| 2019 | [9] | Italy | M | 68 | Local | Skin, hand | Alternaria alternata | Culture + molecular biology | ISZ + PZL | - | No | Kidney | FR | 48 | Yes |
| 2020 | [10] | Italy | F | 56 | Local | Skin, limbs | Alternaria alternata | Culture | VZL | 24 | No | Liver | FR | 108 | Yes |
| 2019 | [7] | Spain | F | 53 | Local | Skin, leg | Alternaria infectoria | Culture + molecular biology (18s-DNA, ITS 1 + ITS 4) | ITZ | 28 | No | Lung | FR | 24 | None |
| 2019 | [7] | Spain | M | 64 | Local | Skin, legs | Alternaria infectoria | Culture + molecular biology (18s-DNA, ITS 1 + ITS 4) | ITZ + VZL | 72 | No | Lung | FR | 2 | None |
| 2019 | [7] | Spain | M | 51 | Local | Skin, leg | Alternaria infectoria | Culture + molecular biology (18s-DNA, ITS 1 + ITS 4) | Surgery | - | Yes | Kidney | FR | 24 | None |
| 2019 | [7] | Spain | M | 56 | Local | Skin, leg | Alternaria infectoria | Culture + molecular biology (18s-DNA, ITS 1 + ITS 4) | ITZ | 8 | Yes | Kidney | FR | 25 | None |
| 2019 | [7] | Spain | M | 46 | Local | Skin, leg | Alternaria infectoria | Culture + molecular biology (18s-DNA, ITS 1 + ITS 4) | Topic VZL | 8 | Yes | Lung | FR | 18 | None |
| 2017 | [11] | Spain | F | 72 | Local | Skin, leg | Alternaria infectoria | Culture + molecular biology (18s + 28s rRNA) | Surgery | - | Yes | Kidney | FR | 180 | None |
| 2012 | [12] | Portugal | M | 53 | Local | Skin, hands, and feet | Alternaria infectoria | Culture + molecular biology (ITS 1 + ITS 4) | ITZ | 40 | No | Kidney | FR | 16 | None |
| 2012 | [13] | Italy | F | 64 | Disseminated | Kidney | Alternaria infectoria | Undefined | TBF | - | Yes | Kidney | FR | - | Yes |
| 2016 | [14] | Czech Republic | M | 61 | Disseminated | Lungs | Alternaria infectoria | Culture + molecular biology (ITS) | VZL + PZL | 28 | No | Heart | FR | 12 | Yes |
| 2020 | [15] | Spain | M | 46 | Local | Skin, leg | Alternaria spp.
| Culture | VZL | 3 | Yes | Lung | FR | 24 | None |
| 2014 | [16] | Slovakia | M | 63 | Disseminated | Skin and brain | Cladophialophora bantiana | Culture + molecular biology (ITS 1 + ITS 4) | LAB | - | No | Heart | DFI | 9 | Yes |
| 2017 | [17] | France | F | 35 | Disseminated | CNS, spinal cord, and cerebellum | Cladophialophora bantiana | Culture + direct microscopy | LAB + PZL + FTS | 36 | No | Lung | DOR | 120 | None |
| 2016 | [18] | Belgium | F | 34 | Disseminated | Bone and brain | Cladophialophora bantiana | Culture + molecular biology | VZL + LAB, ISZ + LAB, PZL + LAB + FTS | - | Yes | Kidney | PR | 17 | Yes |
| 2019 | [7] | Spain | M | 70 | Local | Skin, knee | Cladosporium cladosporioides | Culture + molecular biology (18s-DNA, ITS 1 + ITS 4) | Surgery | - | Yes | Kidney | FR | 10 | None |
| 2013 | [19] | Spain | M | 25 | Local | Skin, leg | Curvularia lunata | Culture+ direct microscopy | ITZ | - | Yes | Kidney | FR | 18 | None |
| 2018 | [20] | France | M | 51 | Local deep | Foot tendon and skin | Diaporthe raonikayaporum | Culture + direct microscopy | Surgery | - | Yes | Kidney | FR | 84 | None |
| 2019 | [21] | Austria | M | 76 | Local deep | Sternal wound | Exophiala dermatitidis | Molecular biology (ITS sequence) | FZL + ADF, VZL | - | Yes | Lung | DFI | <1 | Yes |
| 2019 | [7] | Spain | M | 58 | Local | Skin, leg | Exophiala oligosperma | Culture + molecular biology (18s-DNA, ITS 1 + ITS 4) | VZL | 32 | Yes | Lung | DOR | 20 | None |
| 2015 | [22] | Italy | F | 65 | Local | Skin, hand | Exophiala xenobiotica | Culture + molecular biology (ITS) | VZL, LAB, PZL | 68 | Yes | Kidney | FR | 18 | None |
| 2019 | [23] | Spain | M | 65 | Local | Skin, foot | Medicopsis romeroi | Culture + direct microscopy + molecular biology (ITS1 + ITS4) | PZL | 4 | Yes | Liver | FR | 1 | Yes |
| 2019 | [23] | Spain | F | 56 | Local | Skin, hand | Medicopsis romeroi | Culture + direct microscopy + molecular biology (ITS1 + ITS4) | VZL | 10 | Yes | Kidney | FR | - | Yes |
| 2020 | [24] | France | M | 30 | Local | Skin, foot | Medicopsis romeroi | Culture + molecular biology (ITS 1 + ITS 4) | VZL | 8 | Yes | Kidney | FR | 18 | None |
| 2019 | [7] | Spain | M | 65 | Local | Skin, leg | Microsphaeropsis arundinis | Culture + molecular biology (18s-DNA, ITS 1 + ITS 4) | ITZ + TBF | 54 | Yes | Lung | FR | 60 | None |
| 2015 | [25] | France | M | 59 | Local | Skin, toes, and foot | Neoscytalidium dimidiatum | Culture + molecular biology (ITS 1 + ITS 4) | VZL | 12 | No | Kidney | FR | 8 | None |
| 2015 | [25] | France | M | 49 | Disseminated | Skin, bones, and lungs | Neoscytalidium dimidiatum | Culture + molecular biology (ITS 1 + ITS 4) | VZL | - | No | Kidney | FR | 13 | Yes |
| 2012 | [26] | Germany | M | 69 | Local | Skin, leg, and abdomen | Ochroconis Gallopavum | Culture | VZL | 12 | Yes | Lung | DOR | 72 | None |
| 2012 | [26] | Germany | M | 69 | Disseminated | Skin and lung | Ochroconis Gallopavum | Culture + direct microscopy | VZL | - | Yes | Lung | DOR | 72 | None |
| 2012 | [27] | France | M | 66 | Local | Skin, foot | Pyrenochaeta romeroi | Molecular biology | Surgery, immunosuppression reduction | - | Yes | Kidney | FR | 14 | None |
| 2020 | [28] | France | M | 49 | Local | Skin, hand | Trematosphaeria grisea | Culture + molecular biology (rDNA 28S D1-D2) | ISZ + TBF | 84 | No | Heart | FR | 3 | None |
| 2017 | [29] | France | M | 71 | Local | Skin, leg | Veronaea botryosa | Direct microscopy + molecular biology | PZL | 12 | Yes | Heart | DOR | 7 | None |
Table 4.
Reported cases in the U.S.A.
Table 4.
Reported cases in the U.S.A.
| Year | Ref | Country | Sex | Age | Dissemination | Localization | Species | Method of Identification | Therapy | Duration of Therapy in Weeks | Surgery | Transplant | Outcome | Time Tx-Diagnosis in Months | Susceptibility Test |
|---|
| 2020 | [30] | U.S.A. | F | 54 | Disseminated | Brain | Acrophialophora levis | Culture + molecular biology (ITS) | VZL | - | No | Kidney | FR | 9 | Yes |
| 2019 | [31] | U.S.A. | F | 64 | Local | Skin, limbs | Alternaria alternata | Culture | PZL | 24 | Yes | Heart | FR | 10 | None |
| 2016 | [32] | U.S.A. | F | 65 | Local | Skin, arm | Biatriospora mackinnonii | Culture + molecular biology (rDNA D1-D2) | ITZ | 24 | Yes | Kidney | FR | 2 | None |
| 2011 | [33] | U.S.A. | M | 55 | Disseminated | Brain | Bipolaris spicifera | Histopathology + direct microscopy | LAB + VZL | 48 | No | Heart | FR | 1.5 | Yes |
| 2021 | [34] | U.S.A. | M | 69 | Disseminated | Lung and brain | Cladophialophora bantiana | Culture | ISZ + LAB | - | No | Kidney | DFI | 36 | None |
| 2017 | [35] | U.S.A. | M | 77 | Local deep | Skin, leg, and feet | Exophiala oligosperma | Culture | ITZ | 20 | Yes | Kidney | FR | - | Yes |
| 2019 | [36] | U.S.A. | F | 65 | Local deep | Skin, foot | Medicopsis romeroi | Culture + molecular biology (ITS 1 + ITS 2) | PZL | 12 | Yes | Kidney | FR | 70 | Yes |
| 2020 | [37] | U.S.A. | M | 64 | Local | Skin, leg | Nigrograna mackinnonii | Culture + molecular biology (ITS2 + 28s-rRNA) | PZL | 3 | No | Kidney | FR | 7 | None |
| 2012 | [38] | U.S.A. | M | 49 | Local | Skin, leg | Paraconiothyrium cyclothyrioides | Culture + molecular biology | VZL, PZL | 12 | No | Kidney | FR | 18 | None |
| 2014 | [39] | U.S.A. | F | 49 | Disseminated | Lung | Phaeoacremonium parasiticum | Culture + direct microscopy | PZL | 16 | No | Kidney | FR | 72 | None |
| 2022 | [40] | U.S.A. | M | 71 | Local | Skin, hand | Phialophora spp.
| Culture + molecular biology (ITS) | ITZ | - | No | Kidney | FR | 16 | None |
| 2020 | [41] | U.S.A. | M | 40 | Local | Skin, hand | Rhytidhysteron rufulum | Culture + molecular biology | VZL | 12 | Yes | Kidney | FR | - | None |
Table 5.
Reported cases in South America.
Table 5.
Reported cases in South America.
| Year | Ref | Country | Sex | Age | Dissemination | Localization | Species | Method of Identification | Therapy | Duration of Therapy in Weeks | Surgery | Transplant | Outcome | Time Tx-Diagnosis in Months | Susceptibility |
|---|
| 2014 | [42] | Brazil | M | 68 | Local | Skin, hand | Alternaria infectoria, Colletotrichum gloeosporioides | Culture | Surgery | - | Yes | Kidney | FR | 35 | Yes |
| 2019 | [43] | Colombia | M | 66 | Disseminated | Brain and lung | Alternaria spp.
| Culture + direct microscopy | LAB + TBF | 16 | No | Kidney | DOR | 12 | None |
| 2021 | [44] | Brazil | F | 46 | Local | Skin, face | Biatriospora mackinnonii | Culture + molecular biology (ITS 4 + ITS 5) | ITZ | - | Yes | Kidney | FR | 96 | None |
| 2019 | [45] | Colombia | - | - | Disseminated | Brain | Cladophialophora bantiana | Culture+ direct microscopy | VZL | - | Yes | Kidney | FR | 60 | None |
| 2016 | [46] | Brazil | M | 53 | Local | Skin, leg | Exophiala spp.
| Culture | ITZ | 20 | Yes | Kidney | FR | 48 | None |
| 2016 | [46] | Brazil | M | 59 | Local | Skin, leg | Exophiala spp.
| Culture | ITZ | 16 | Yes | Kidney | FR | 16 | None |
| 2016 | [47] | Brazil | M | 54 | Local | Skin, leg | Exophiala bergeri | Culture + molecular biology | ITZ | - | No | Kidney | FR | 24 | None |
| 2019 | [48] | Brazil | M | 45 | Local | Skin, leg | Exophiala xenobiotica | Culture + molecular biology (ITS 1 + ITS 4) | ITZ | 12 | Yes | Kidney | FR | 21 | Yes |
| 2016 | [47] | Brazil | M | 75 | Local | Skin, limbs | Exophiala xenobiotica | Culture + molecular biology | ITZ | - | No | Kidney | Lost on follow-up | 12 | None |
| 2016 | [47] | Brazil | M | 43 | Local | Skin, hand | Fonsecaea monophora | Culture + molecular biology | Surgery | - | Yes | Kidney | FR | 24 | None |
| 2016 | [47] | Brazil | M | 60 | Local | Skin, arm | Fonsecaea pedrosoi | Culture + molecular biology | ITZ + surgery | - | Yes | Kidney | FR | 36 | None |
| 2016 | [47] | Brazil | M | 57 | Local | Skin, arm | Fonsecaea spp. | Culture + molecular biology | TBF | - | No | Kidney | FR | 1 | None |
| 2017 | [49] | Argentina | M | 48 | Local | Skin, hand | Graphium basitruncatum | Culture + molecular biology | VZL + surgery | - | Yes | Heart | FR | 48 | None |
| 2015 | [50] | French Antilles | M | 71 | Disseminated | Skin, lung, and brain | Phaeoacremonium parasiticum and Paraconiothyrium cyclothyrioides | Culture + molecular biology | VZL + LAB | - | Yes | Kidney | DOR | 12 | Yes |
| 2014 | [51] | French Antilles | F | 59 | Local | Skin, leg | Pleurostoma ootheca | Culture + direct microscopy | PZL | - | No | Kidney | FR | 168 | None |
| 2016 | [47] | Brazil | F | 59 | Local | Skin, foot | Undefined | Culture + molecular biology | ITZ + surgery | - | Yes | Kidney | FR | 14 | None |
Table 6.
Reported cases in Asia.
Table 6.
Reported cases in Asia.
| Year | Ref | Country | Sex | Age | Dissemination | Localization | Species | Method of Identification | Therapy | Duration of Therapy in Weeks | Surgery | Transplant | Outcome | Time Tx-Diagnosis in Months | Susceptibility Test |
|---|
| 2015 | [52] | China | M | 61 | Local | Skin, leg | Alternaria species | Culture + direct microscopy | ITZ + VZL | 7 | No | Kidney | DOR | 12 | None |
| 2020 | [53] | Japan | F | 40 | Local | Skin, leg | Exophiala jeanselmei | Culture + direct microscopy | ITZ | 92 | Yes | Kidney | FR | 72 | None |
| 2017 | [54] | India | - | 16 | Local | Skin, leg | Exophiala jeanselmei | Culture | ITZ | 12 | Yes | Kidney | FR | 11 | None |
| 2016 | [55] | India | F | 48 | Local | Skin, leg | Exophiala jeanselmei | Culture + direct microscopy | LAB + ITZ | 6 | Yes | Kidney | FR | 6 | None |
| 2012 | [56] | China | M | 66 | Local | Skin, arm | Exophiala jeanselmei | Molecular biology (ITS sequence) | Surgery + local injection and undefined systemic antifungal treatment | - | Yes | Kidney | FR | 67 | Yes |
| 2020 | [57] | China | F | 47 | Local | Skin, hand | Hongkongmyces snookiorum | Culture + molecular biology (ITS 1 + ITS 2) | VZL | 8 | Yes | Kidney | FR | 18 | Yes |
| 2017 | [54] | India | | 37 | Local | Skin, foot | Neoscytalidium species | Culture | ITZ | 24 | Yes | Kidney | FR | 1 | None |
| 2015 | [58] | Japan | F | 61 | Local | Skin, arm | Phaeoacremonium spp.
| Culture + direct microscopy | LAB | 2 | No | Kidney | DOR | 156 | None |
| 2021 | [59] | China | M | 65 | Disseminated | Liver | Pleurostoma hongkongense sp. nov. | Culture + molecular biology (ITS + 28s nr-DNA + 18s nr-DNA) | ADF, LAB, VZL | 14 | Yes | Liver | FR | 16 | Yes |
| 2019 | [60] | Thailand | M | 57 | Disseminated | Liver | Pleurostomophora richardsiae | Culture + molecular biology (ITS 1 + ITS 2) | LAB | 4 | Yes | Liver | FR | 1 | Yes |
| 2019 | [61] | Singapore | M | - | Local | Skin, leg | Pleurostomophora richardsiae | Culture + direct microscopy | ITZ | 40 | Yes | Kidney | FR | 276 | None |
| 2017 | [62] | India | F | 43 | Local | Skin, leg | Pyrenochaeta romeroi | Culture + direct microscopy | ITZ + TBF, VZL | 8 | Yes | Kidney | FR | 6 | None |
| 2021 | [63] | Kuwait | F | 50 | Disseminated | Liver, brain, and lung | Rhinocladiella mackenziei | Culture + molecular biology (ITS) | LAB + VZL | 6 | No | Kidney | DFI | 3 | None |
| 2013 | [64] | Thailand | 69 | Disseminated | Brain | Scedosporium apiospermum and Phaeoacremonium parasiticum | Culture + direct microscopy | VZL | 24 | No | Kidney | PR | 168 | None |
| 2017 | [54] | India | | 21 | Local | Skin, foot | Undefined | Culture | ITZ | 72 | Yes | Kidney | FR | 6 | None |
| 2017 | [54] | India | | 22 | Local | Skin, hand | Undefined | Culture | ITZ | 68 | Yes | Kidney | FR | 6 | None |
| 2017 | [54] | India | F | 49 | Local | Skin, arm | Undefined | Culture | ITZ | 48 | Yes | Kidney | DOR | 12 | None |
| 2017 | [54] | India | | 43 | Local | Skin, foot | Undefined | Culture | Surgery | - | Yes | Kidney | FR | 6 | None |
| 2017 | [54] | India | | 23 | Local | Skin, foot | Undefined | Culture | ITZ | 12 | Yes | Kidney | FR | 5 | None |
| 2022 | [65] | India | F | 36 | Disseminated | Skin and bone | Undefined | Direct microscopy | Undefined | - | Yes | Kidney | FR | 72 | None |
| 2021 | [66] | India | M | 50 | Local | Skin, foot, and leg | Undefined | Culture + direct microscopy | ITZ | - | Yes | Kidney | PR | 24 | None |
| 2021 | [66] | India | M | 55 | Local | Skin, hand, and foot | Undefined | Culture + direct microscopy | VZL + CSF | - | Yes | Kidney | DOR | 3 | None |
| 2021 | [66] | India | M | 35 | Disseminated | Skin, foot, and peri-renal abscess | Undefined | Culture + direct microscopy | LAB | - | Yes | Kidney | FR | 24 | None |
| 2021 | [66] | India | M | 52 | Local deep | Facial skin and bone | Undefined | Culture + direct microscopy | LAB | - | Yes | Kidney | FR | 17 | None |
| 2021 | [66] | India | M | 52 | Local | Skin, foot | Undefined | Culture + direct microscopy | LAB | - | Yes | Kidney | FR | 1 | None |
| 2016 | [67] | India | M | 37 | Local deep | Salivary gland | Undefined dematiaceous fungi | Direct microscopy | VZL | - | Yes | Kidney | FR | 39 | None |
| 2016 | [67] | India | M | 37 | Local deep | Salivary gland | Undefined dematiaceous fungi | Direct microscopy | VZL | - | Yes | Kidney | FR | 39 | None |
Table 7.
Reported cases in Australia.
Table 7.
Reported cases in Australia.
| Year | Ref | Country | Sex | Age | Dissemination | Localization | Species | Method of Identification | Therapy | Duration of Therapy in Weeks | Surgery | Transplant | Outcome | Time Tx-Diagnosis in Months | Susceptibility Test |
|---|
| 2015 | [68] | Australia | F | 49 | Local | Skin, leg | Microsphaeropsis arundinis | Culture + molecular biology | VZL | 24 | No | Kidney | FR | 84 | Yes |
| 2015 | [68] | Australia | F | 70 | Local | Skin, leg, and arm | Microsphaeropsis arundinis | Culture + molecular biology | LAB + PZL | 48 | Yes | Kidney | FR | 4 | Yes |
| 2015 | [68] | Australia | M | 55 | Local | Skin, arm | Microsphaeropsis arundinis | Culture + molecular biology | ITZ | 44 | Yes | Kidney | FR | 30 | Yes |
| 2016 | [69] | Australia | F | 67 | Disseminated | Heart and brain | Verruconis gallopava | Molecular biology | VZL + ADF | - | No | Kidney | DFI | 18 | Yes |
4. Discussion
Phaeohyphomycosis (from the Greek word “phaeo” meaning “dark”) is caused by pigmented dematiaceous fungi and can cause a wide spectrum of clinical diseases, ranging from superficial to disseminated infections [
6]. Immunocompromised hosts, including SOT recipients, are the most affected category of patients [
35]. It is difficult to accurately determine the incidence of phaeohyphomycosis in the SOT population because of the rarity of the disease, and previous studies are limited to case reports and retrospective studies [
3]. We report three cases of phaeohyphomycosis local infections in SOT recipients caused by
Alternaria alternata, Alternaria infectoria, and
Curvularia hawaiiensis. In our cases, the length of therapy and choice of intervention (surgery, antifungals, or both) for each clinical entity were based primarily on the clinical presentation, the underlying condition of the host, and the initial response. In the two heart recipients (case 1 and 2), because of a more intense immunosuppression and recent treatment of acute rejection, surgical excision with systemic antifungal therapy was chosen. The kidney transplant recipient (case 3) requiring a less intense immunosuppressive regimen, surgical excision, without antifungal treatment, and follow-up was considered to be sufficient. All three patients survived, with full recovery.
Though phaeohyphomycosis is a rare fungal infection, trends toward an increasing incidence have been noted. In our review, most of the cases (75%) were published in the last seven years, confirming the increasing trend observed in recent years and already described by Schieffelin et al. and by McCarthy [
3,
70]. This is likely a consequence of medical advancements allowing for increased transplantation rates, resulting in increasing numbers of immunosuppressed patients who are at risk for such opportunistic infections. Interestingly, we additionally found substantial differences in characteristics of affected patients and causative organisms between cases reported in the EU and the rest of the world. While kidney transplant recipients were most frequently reported to be diagnosed with phaeohyphomycosis in every country, surprisingly, lung transplant recipients were only reported in the EU. This is inconsistent with what was reported by the U.S.-based (Transplant-Associated Infection Surveillance Network) TRANSNET cohort and Schieffelin at al. cohort, where 53% and 11% of the SOT recipients with phaeohyphomycosis were lung recipients, respectively [
3,
70]. This finding can be partially explained by the different time periods of the cases collection. We reviewed cases published from 2011 to 2022, Schieffelin at al. reported cases from 1988 to 2009, while in the TRANSNET cohort, cases were reported from 2001 to 2006. Regarding the time of onset of the infection, we found a median time from transplant to infection of 18 months; a similar time range was observed in the 2 cohorts previously mentioned. In our review, most of the infections described were localized to the skin and soft tissue. In fact, only 22% of them were disseminated to other organs. This finding is discordant with what is described in the TRANSNET cohort, where 63.3% of the infections were disseminated [
3]. This can partly explain the higher mortality observed in the TRANSNET cohort since disseminated infections are more severe than local ones.
Our literature review revealed about 40 different species of fungi causing phaeohyphomycosis; Alternaria and Exophiala resulted to be the most reported genera. Previous studies have shown a similar distribution of genera, with Alternaria and Exophiala being the most common genera involved; however, fewer species were identified [
3,
70]. The increasing number of pathogens could be attributable to a wider use of molecular biology, which provides a more accurate species identification including unusual pathogens. In addition to species identification, antifungal susceptibility testing should be performed with a microscopic examination and culture. Despite the fact that the guidelines of the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines [
6] as well as the American Society of Transplantation Infectious Diseases Community of Practice (AST-IDCOP) [
71] suggest obtaining a susceptibility test, in our review, we found that it was carried out only in about a third of cases (28% of cases in the EU vs. 26% in non-EU). Antifungal susceptibility testing could be useful to guide antifungal therapy; however, a correlation between in vitro MICs and patient outcomes is still debated due to the scarcity of robust clinical data. This is especially the case for rare fungal pathogens [
72]. Therefore, the majority of therapies reported were empirical.
There are no standardized therapies for phaeohyphomycosis. ESCMID guidelines [
6] suggest voriconazole, posaconazole, and itraconazole as empirical therapy. These suggestions are reflected in the European cases of our review, in which voriconazole was widely used, followed by itraconazole and posaconazole. In the TRANSNET cohort, the most used antifungal agent was voriconazole (44%), while in Schieffelin et al.’s review, itraconazole was the most used agent for skin lesions, but a combination of voriconazole and amphotericin B was preferred for disseminated disease. Surgical resection was performed in 67% of the European patients, with 17% of them not receiving an antifungal therapy. Similarly, in non-EU countries, surgery was performed in 69% of cases, but only 5% did not receive antifungals. In Schieffelin et al.’s cohort, most of the patients received surgery (81%), not followed by antifungal therapy in 14% of the cases. Phaeohyphomycosis mortality is related to the dissemination of the disease. The mortality rate was 5% overall compared to 47% mortality in the TRANSNET cohort, probably due to the greater proportion of disseminated disease.
To the best of our knowledge, this is the largest review of the literature on phaeohyphomycosis in SOT recipients. These infections have not been studied in clinical trials and the available therapeutic data are primarily based on sporadic case reports. This review additionally highlights that a standardized approach to phaeohyphomycosis is difficult to determine due to the wide spectrum of dematiaceous fungi involved, different characteristics of the hosts, and the variety of clinical presentations. An early diagnosis and therapy are critical in preventing the dissemination of disease; therefore, in SOT recipients with atypical cutaneous lesions, a skin biopsy should always be performed. The diagnosis relies on a high index of clinical suspicion paired with an accurate mycological investigation. In addition to a histologic examination, culture and molecular biology identification are essential to establish an etiologic diagnosis in rare fungal diseases. As cases increase, further studies are becoming necessary to determine the optimal management strategy in this vulnerable immunosuppressed population.

 ,
, 

{kind=link}
{kind=link}
{kind=link}


