
Long-Term Kinetics of Serum Galactomannan during Treatment of Complicated Invasive Pulmonary Aspergillosis

 , and
, and 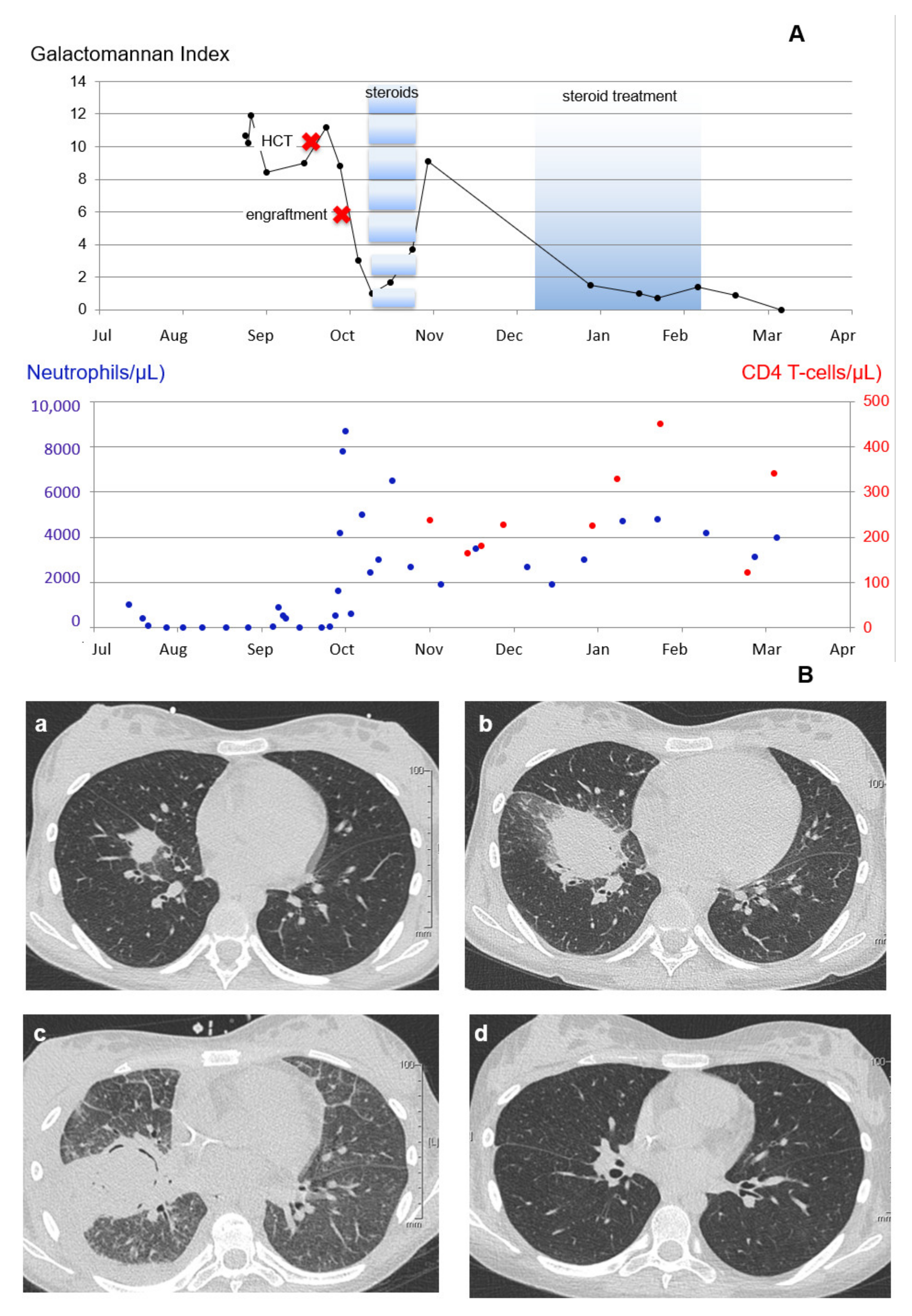{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Reports
2.1. Patient 1
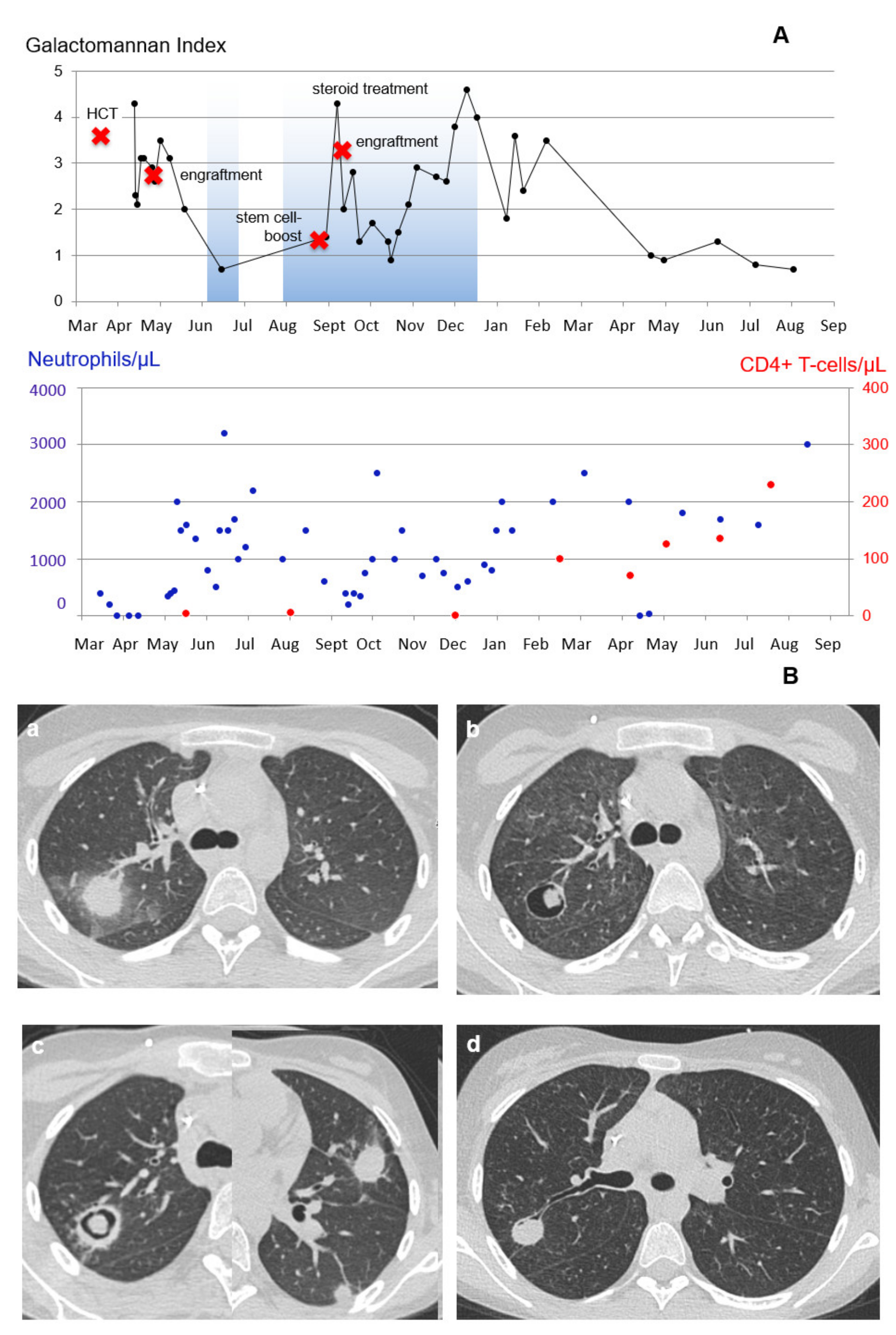
2.2. Patient 2
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Latgé, J.P.; Kobayashi, H.; Debeaupuis, J.P.; Diaquin, M.; Sarfati, J.; Wieruszeski, J.M.; Parra, E.; Bouchara, J.P.; Fournet, B. Chemical and immunological characterization of the extracellular galactomannan of Aspergillus fumigatus. Infect. Immun. 1994, 62, 5424–5433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mennink-Kersten, M.A.; Donnelly, J.P.; Verweij, P.E. Detection of circulating galactomannan for the diagnosis and management of invasive aspergillosis. Lancet Infect. Dis. 2004, 4, 349–357. [Google Scholar] [PubMed]
- Kovanda, L.L.; Desai, A.V.; Hope, W.W. Prognostic value of galactomannan: Current evidence for monitoring response to antifungal therapy in patients with invasive aspergillosis. J. Pharmacokinet. Pharmacodyn. 2017, 44, 143–151. [Google Scholar] [PubMed]
- Lehrnbecher, T.; Robinson, P.D.; Fisher, B.T.; Castagnola, E.; Groll, A.H.; Steinbach, W.J.; Zaoutis, T.E.; Negeri, Z.F.; Beyene, J.; Phillips, B.; et al. Galactomannan, β-D-Glucan, and Polymerase Chain Reaction-Based Assays for the Diagnosis of Invasive Fungal Disease in Pediatric Cancer and Hematopoietic Stem Cell Transplantation: A Systematic Review and Meta-Analysis. Clin. Infect. Dis. 2016, 63, 1340–1348. [Google Scholar] [PubMed] [Green Version]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 12, 1367–1376. [Google Scholar]
- Patterson, T.F.; Thompson, G.R., 3rd; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Executive Summary: Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, 433–442. [Google Scholar]
- Ullmann, A.J.; Aguado, J.M.; Arikan-Akdagli, S.; Denning, D.W.; Groll, A.H.; Lagrou, K.; Lass-Flörl, C.; Lewis, R.E.; Munoz, P.; Verweij, P.E.; et al. Diagnosis and management of Aspergillus diseases: Executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin. Microbiol Infect. 2018, 24, e1–e38. [Google Scholar] [CrossRef] [Green Version]
- Lehrnbecher, T.; Robinson, P.; Fisher, B.; Alexander, S.; Ammann, R.A.; Beauchemin, M.; Carlesse, F.; Groll, A.H.; Haeusler, G.M.; Santolaya, M.; et al. Guideline for the Management of Fever and Neutropenia in Children With Cancer and Hematopoietic Stem-Cell Transplantation Recipients: 2017 Update. J. Clin. Oncol. 2017, 35, 2082–2094. [Google Scholar] [CrossRef] [Green Version]
- Groll, A.H.; Pana, D.; Lanternier, F.; Mesini, A.; Ammann, R.A.; Averbuch, D.; Castagnola, E.; Cesaro, S.; Engelhard, D.; Garcia-Vidal, C.; et al. 8th European Conference on Infections in Leukaemia: 2020 guidelines for the diagnosis, prevention, and treatment of invasive fungal diseases in paediatric patients with cancer or post-haematopoietic cell transplantation. Lancet. Oncol. 2021, 22, e254–e269. [Google Scholar]
- Miceli, M.H.; Grazziutti, M.L.; Woods, G.; Zhao, W.; Kocoglu, M.H.; Barlogie, B.; Anaissie, E. Strong correlation between serum aspergillus galactomannan index and outcome of aspergillosis in patients with hematological cancer: Clinical and research implications. Clin. Infect. Dis. 2008, 46, 1412–1422. [Google Scholar]
- Mercier, T.; Guldentops, E.; Lagrou, K.; Maertens, J. Galactomannan, a Surrogate Marker for Outcome in Invasive Aspergillosis: Finally Coming of Age. Front. Microbiol. 2018, 9, 661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tragiannidis, A.; Roilides, E.; Walsh, T.J.; Groll, A.H. Invasive aspergillosis in children with acquired immunodeficiencies. Clin. Infect. Dis. 2012, 54, 258–267. [Google Scholar] [PubMed]
- Pana, Z.D.; Roilides, E.; Warris, A.; Groll, A.H.; Zaoutis, T. Epidemiology of Invasive Fungal Disease in Children. J. Pediatr. Infect. Dis Soc. 2017, 6, S3–S11. [Google Scholar]
- Linke, C.; Ehlert, K.; Ahlmann, M.; Fröhlich, B.; Mohring, D.; Burkhardt, B.; Rössig, C.; Groll, A.H. Epidemiology, utilisation of healthcare resources and outcome of invasive fungal diseases following paediatric allogeneic haematopoietic stem cell transplantation. Mycoses 2020, 63, 172–180. [Google Scholar]
- Leeflang, M.M.; Debets-Ossenkopp, Y.J.; Wang, J.; Visser, C.E.; Scholten, R.J.; Hooft, L.; Bijlmer, H.A.; Reitsma, J.B.; Zhang, M.; Bossuyt, P.M.; et al. Galactomannan detection for invasive aspergillosis in immunocompromised patients. Cochrane. Database Syst. Rev. 2015, 34, CD007394. [Google Scholar]
- Huppler, A.R.; Fisher, B.T.; Lehrnbecher, T.; Walsh, T.J.; Steinbach, W.J. Role of Molecular Biomarkers in the Diagnosis of Invasive Fungal Diseases in Children. J. Pediatric. Infect. Dis Soc. 2017, 6, S32–S44. [Google Scholar] [PubMed] [Green Version]
- Kovanda, L.L.; Kolamunnage-Dona, R.; Neely, M.; Maertens, J.; Lee, M.; Hope, W.W. Pharmacodynamics of Isavuconazole for Invasive Mold Disease: Role of Galactomannan for Real-Time Monitoring of Therapeutic Response. Clin. Infect. Dis. 2017, 64, 1557–1563. [Google Scholar] [CrossRef]
- McCarthy, M.W.; Walsh, T.J. Galactomannan antigenemia as a biomarker for therapeutic response of invasive aspergillosis: Implications for clinical trial design and patient care. Expert Rev. Mol. Diagn. 2018, 18, 601–604. [Google Scholar] [CrossRef]
- Slavin, M.A.; Chen, Y.C.; Cordonnier, C.; Cornely, O.A.; Cuenca-Estrella, M.; Donnelly, J.P.; Groll, A.H.; Lortholary, O.; Marty, F.M.; Nucci, M.; et al. When to change treatment of acute invasive aspergillosis: An expert viewpoint. J. Antimicrob. Chemother. 2021, 77, 16–23. [Google Scholar] [CrossRef]
- Petraitiene, R.; Petraitis, V.; Groll, A.H.; Sein, T.; Piscitelli, S.; Candelario, M.; Field-Ridley, A.; Avila, N.; Bacher, J.; Walsh, T.J. Antifungal activity and pharmacokinetics of posaconazole (SCH 56592) in treatment and prevention of experimental invasive pulmonary aspergillosis: Correlation with galactomannan antigenemia. Antimicrob. Agents Chemother. 2001, 45, 857–869. [Google Scholar]
- Petraitiene, R.; Petraitis, V.; Groll, A.H.; Sein, T.; Schaufele, R.L.; Francesconi, A.; Bacher, J.; Avila, N.A.; Walsh, T.J. Antifungal efficacy of caspofungin (MK-0991) in experimental pulmonary aspergillosis in persistently neutropenic rabbits: Pharmacokinetics, drug disposition, and relationship to galactomannan antigenemia. Antimicrob. Agents Chemother. 2002, 46, 12–23. [Google Scholar]
- Hope, W.W.; Petraitis, V.; Petraitiene, R.; Aghamolla, T.; Bacher, J.; Walsh, T.J. The initial 96 hours of invasive pulmonary aspergillosis: Histopathology, comparative kinetics of galactomannan and (1->3) β-d-glucan and consequences of delayed antifungal therapy. Antimicrob. Agents Chemother. 2010, 54, 4879–4886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Nakeeb, Z.; Petraitis, V.; Goodwin, J.; Petraitiene, R.; Walsh, T.J.; Hope, W.W. Pharmacodynamics of amphotericin B deoxycholate, amphotericin B lipid complex, and liposomal amphotericin B against Aspergillus fumigatus. Antimicrob. Agents Chemother. 2015, 59, 2735–2745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petraitiene, R.; Petraitis, V.; Bacher, J.D.; Finkelman, M.A.; Walsh, T.J. Effects of host response and antifungal therapy on serum and BAL levels of galactomannan and (1→3)-β-D-glucan in experimental invasive pulmonary aspergillosis. Med. Mycol. 2015, 53, 558–568. [Google Scholar] [PubMed] [Green Version]
- Kovanda, L.L.; Petraitiene, R.; Petraitis, V.; Walsh, T.J.; Desai, A.; Bonate, P.; Hope, W.W. Pharmacodynamics of isavuconazole in experimental invasive pulmonary aspergillosis: Implications for clinical breakpoints. J. Antimicrob. Chemother. 2016, 71, 1885–1891. [Google Scholar] [CrossRef] [Green Version]
- Gastine, S.; Hope, W.; Hempel, G.; Petraitiene, R.; Petraitis, V.; Mickiene, D.; Bacher, J.; Walsh, T.J.; Groll, A.H. Pharmacodynamics of Posaconazole in Experimental Invasive Pulmonary Aspergillosis: Utility of Serum Galactomannan as a Dynamic Endpoint of Antifungal Efficacy. Antimicrob. Agents Chemother. 2021, 65, e1574–e1620. [Google Scholar]
- Woods, G.; Miceli, M.H.; Grazziutti, M.L.; Zhao, W.; Barlogie, B.; Anaissie, E. Serum Aspergillus galactomannan antigen values strongly correlate with outcome of invasive aspergillosis: A study of 56 patients with hematologic cancer. Cancer 2007, 110, 830–834. [Google Scholar]
- Maertens, J.; Buvé, K.; Theunissen, K.; Meersseman, W.; Verbeken, E.; Verhoef, G.; Van Eldere, J.; Lagrou, K. Galactomannan serves as a surrogate endpoint for outcome of pulmonary invasive aspergillosis in neutropenic hematology patients. Cancer 2009, 115, 355–362. [Google Scholar] [CrossRef]
- Park, S.H.; Choi, S.M.; Lee, D.G.; Choi, J.H.; Kim, S.H.; Kwon, J.C.; Yoo, J.H.; Kim, H.J.; Lee, S.; Eom, K.S.; et al. Serum galactomannan strongly correlates with outcome of invasive aspergillosis in acute leukaemia patients. Mycoses 2011, 54, 523–530. [Google Scholar]
- Marr, K.A.; Schlamm, H.T.; Herbrecht, R.; Rottinghaus, S.T.; Bow, E.J.; Cornely, O.A.; Heinz, W.J.; Jagannatha, S.; Koh, L.P.; Kontoyiannis, D.P.; et al. Combination antifungal therapy for invasive aspergillosis: A randomized trial. Ann. Intern. Med. 2015, 162, 81–89. [Google Scholar]
- Boutboul, F.; Alberti, C.; Leblanc, T.; Sulahian, A.; Gluckman, E.; Derouin, F.; Ribaud, P. Invasive aspergillosis in allogeneic stem cell transplant recipients: Increasing antigenemia is associated with progressive disease. Clin. Infect. Dis. 2002, 34, 939–943. [Google Scholar] [PubMed] [Green Version]
- Koo, S.; Bryar, J.M.; Baden, L.R.; Marty, F.M. Prognostic features of galactomannan antigenemia in galactomannan-positive invasive aspergillosis. J. Clin. Microbiol. 2010, 48, 1255–1260. [Google Scholar] [CrossRef] [Green Version]
- Bergeron, A.; Porcher, R.; Menotti, J.; Poirot, J.L.; Chagnon, K.; Vekhoff, A.; Cornet, M.; Isnard, F.; Raffoux, E.; Brethon, B.; et al. Prospective evaluation of clinical and biological markers to predict the outcome of invasive pulmonary aspergillosis in hematological patients. J. Clin. Microbiol. 2012, 50, 823–830. [Google Scholar] [PubMed] [Green Version]
- Chai, L.Y.; Kullberg, B.J.; Johnson, E.M.; Teerenstra, S.; Khin, L.W.; Vonk, A.G.; Maertens, J.; Lortholary, O.; Donnelly, P.J.; Schlamm, H.T.; et al. Early serum galactomannan trend as a predictor of outcome of invasive aspergillosis. J. Clin. Microbiol. 2012, 50, 2330–2336. [Google Scholar]
- Neofytos, D.; Railkar, R.; Mullane, K.M.; Fredricks, D.N.; Granwehr, B.; Marr, K.A.; Almyroudis, N.G.; Kontoyiannis, D.P.; Maertens, J.; Fox, R.; et al. Correlation between Circulating Fungal Biomarkers and Clinical Outcome in Invasive Aspergillosis. PLoS ONE 2015, 10, e0129022. [Google Scholar] [CrossRef]
- Vehreschild, J.J.; Heussel, C.P.; Groll, A.H.; Vehreschild, M.J.G.T.; Silling, G.; Würthwein, G.; Brecht, M.; Cornely, O.A. Serial assessment of pulmonary lesion volume by computed tomography allows survival prediction in invasive pulmonary aspergillosis. Eur. Radiol. 2017, 27, 3275–3282. [Google Scholar] [PubMed]
- Mercier, T.; Wera, J.; Chai, L.Y.A.; Lagrou, K.; Maertens, J. A Mortality Prediction Rule for Hematology Patients with Invasive Aspergillosis Based on Serum Galactomannan Kinetics. J. Clin. Med. 2020, 9, 610. [Google Scholar] [CrossRef] [Green Version]
- Maertens, J.A.; Raad, I.I.; Marr, K.A.; Patterson, T.F.; Kontoyiannis, D.P.; Cornely, O.A.; Bow, E.J.; Rahav, G.; Neofytos, D.; Aoun, M.; et al. Isavuconazole versus voriconazole for primary treatment of invasive mould disease caused by Aspergillus and other filamentous fungi (SECURE): A phase 3, randomised-controlled, non-inferiority trial. Lancet 2016, 387, 760–769. [Google Scholar]
- Herbrecht, R.; Denning, D.W.; Patterson, T.F.; Bennett, J.E.; Greene, R.E.; Oestmann, J.W.; Kern, W.V.; Marr, K.A.; Ribaud, P.; Lortholary, O.; et al. Invasive Fungal Infections Group of the European Organisation for Research and Treatment of Cancer and the Global Aspergillus Study Group. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N. Engl. J. Med. 2002, 347, 408–415. [Google Scholar] [CrossRef] [Green Version]
- Segal, B.H.; Herbrecht, R.; Stevens, D.A.; Ostrosky-Zeichner, L.; Sobel, J.; Viscoli, C.; Walsh, T.J.; Maertens, J.; Patterson, T.F.; Perfect, J.R.; et al. Defining responses to therapy and study outcomes in clinical trials of invasive fungal diseases: Mycoses Study Group and European Organization for Research and Treatment of Cancer consensus criteria. Clin. Infect. Dis. 2008, 47, 674–683. [Google Scholar] [CrossRef]
- Nouér, S.A.; Nucci, M.; Kumar, N.S.; Grazziutti, M.; Barlogie, B.; Anaissie, E. Earlier response assessment in invasive aspergillosis based on the kinetics of serum Aspergillus galactomannan: Proposal for a new definition. Clin. Infect. Dis. 2011, 53, 671–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delgado-Araneda, M.; Valenzuela, R.; de la Maza, V.; Rabello, M.; Álvarez, A.M.; Contardo, V.; Zubieta, M.; Gutierrez, V.; Claverie, X.; Torres, J.P.; et al. Usefulness of serum galactomannan in initiating and modifying antifungal therapy in children with cancer and persistent high-risk febrile neutropenia. Mycoses 2020, 63, 802–811. [Google Scholar] [PubMed]
- Han, S.B.; Kim, S.K.; Lee, J.W.; Yoon, J.-S.; Chung, N.-G.; Cho, B.; Jeong, D.C.; Kang, J.H.; Kim, H.-K.; Lee, D.-G.; et al. Serum galactomannan index for early prediction of mortality in immunocompromised children with invasive pulmonary aspergillosis. BMC Infect. Dis. 2015, 15, 271. [Google Scholar]
- Huurneman, L.J.; Neely, M.; Veringa, A.; Docobo Pérez, F.; Ramos-Martin, V.; Tissing, W.J.; Alffenaar, J.W.; Hope, W. Pharmacodynamics of Voriconazole in Children: Further Steps along the Path to True Individualized Therapy. Antimicrob. Agents Chemother. 2016, 60, 2336–2342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taghizadeh-Armaki, M.; Hedayati, M.T.; Moqarabzadeh, V.; Ansari, S.; Mahdavi Omran, S.; Zarrinfar, H.; Saber, S.; Verweij, P.E.; Denning, D.W.; Seyedmousavi, S. Effect of involved Aspergillus species on galactomannan in bronchoalveolar lavage of patients with invasive aspergillosis. J. Med. Microbiol. 2017, 66, 898–904. [Google Scholar]
- Thompson, G.R., 3rd; Boulware, D.R.; Bahr, N.C.; Clancy, C.J.; Harrison, T.S.; Kauffman, C.A.; Le, T.; Miceli, M.H.; Mylonakis, E.; Nguyen, M.H.; et al. Noninvasive Testing and Surrogate Markers in Invasive Fungal Diseases. Open Forum Infect. Dis. 2022, 9, 112. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tragiannidis, A.; Linke, C.; Correa-Martinez, C.L.; Herbrüggen, H.; Schaumburg, F.; Groll, A.H. Long-Term Kinetics of Serum Galactomannan during Treatment of Complicated Invasive Pulmonary Aspergillosis. J. Fungi 2023, 9, 157. https://doi.org/10.3390/jof9020157
Tragiannidis A, Linke C, Correa-Martinez CL, Herbrüggen H, Schaumburg F, Groll AH. Long-Term Kinetics of Serum Galactomannan during Treatment of Complicated Invasive Pulmonary Aspergillosis. Journal of Fungi. 2023; 9(2):157. https://doi.org/10.3390/jof9020157
Chicago/Turabian StyleTragiannidis, Athanasios, Christina Linke, Carlos L. Correa-Martinez, Heidrun Herbrüggen, Frieder Schaumburg, and Andreas H. Groll. 2023. "Long-Term Kinetics of Serum Galactomannan during Treatment of Complicated Invasive Pulmonary Aspergillosis" Journal of Fungi 9, no. 2: 157. https://doi.org/10.3390/jof9020157