
First Report of Neocucurbitaria unguis-hominis Keratitis
 ,
,  , and
, and 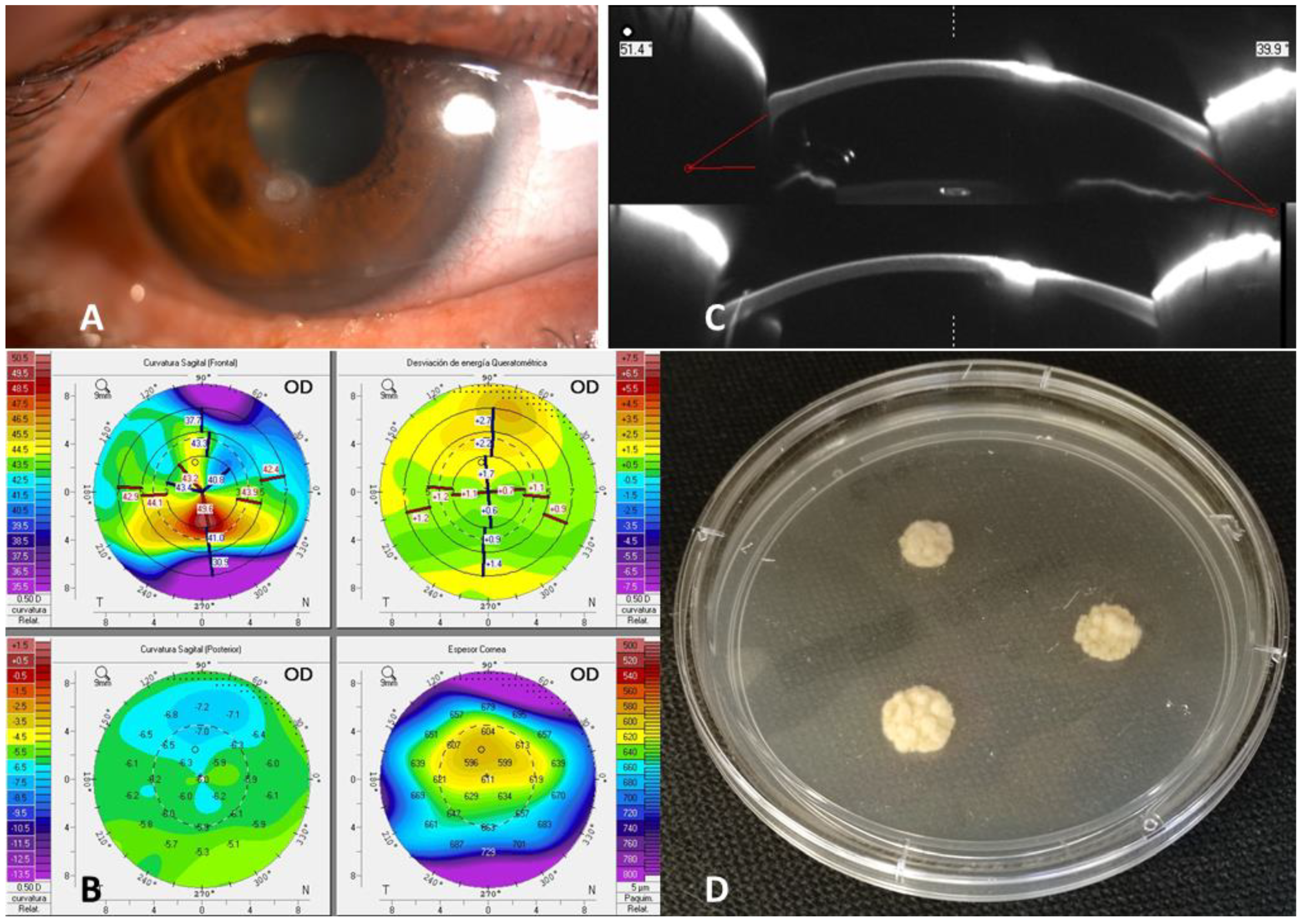{kind=link}
Abstract
:1. Introduction
2. Clinical Description
3. Clinical Course and Microbiological Studies
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sharma, N.; Bagga, B.; Singhal, D.; Nagpal, R.; Kate, A.; Saluja, G.; Maharana, P.K. Fungal keratitis: A review of clinical presentations, treatment strategies and outcomes. Ocul. Surf. 2021, 24, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Ahmadikia, K.; Gharehbolagh, S.A.; Fallah, B.; Eshkaleti, M.N.; Malekifar, P.; Rahsepar, S.; Getso, M.I.; Sharma, S.; Mahmoudi, S. Distribution, Prevalence, and Causative Agents of Fungal Keratitis: A Systematic Review and Meta-Analysis (1990 to 2020). Front. Cell. Infect. Microbiol. 2021, 11, 698780. [Google Scholar] [CrossRef] [PubMed]
- Verkley, G.J.; Gené, J.; Guarro, J.; Pérez-Santonja, J.J.; Rodríguez, A.E.; Colom, M.F.; Alio, J.L.; Ferrer, C. Pyrenochaeta keratinophila sp. nov., isolated from an ocular infection in Spain. Rev. Iberoam. Micol. 2010, 27, 22–24. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela-Lopez, N.; Sutton, D.A.; Cano-Lira, J.F.; Paredes, K.; Wiederhold, N.; Guarro, J.; Stchigel, A.M. Coelomycetous Fungi in the Clinical Setting: Morphological Convergence and Cryptic Diversity. J. Clin. Microbiol. 2017, 55, 552–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Hermoso, D.; Valenzuela-Lopez, N.; Rivero-Menendez, O.; Alastruey-Izquierdo, A.; Guarro, J.; Cano-Lira, J.F.; Stchigel, A.M. Diversity of coelomycetous fungi in human infections: A 10-y experience of two European reference centres. Fungal Biol. 2019, 123, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela-Lopez, N.; Cano-Lira, J.F.; Stchigel, A.M.; Guarro, J. DNA sequencing to clarify the taxonomical conundrum of the clinical coelomycetes. Mycoses 2018, 61, 708–717. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, C.; Peérez-Santonja, J.J.; Rodriíguez, A.E.; Colom, M.F.; Geneé, J.; Alio, J.L.; Verkley, G.J.M.; Guarro, J. New Pyrenochaeta Species Causing Keratitis. J. Clin. Microbiol. 2009, 47, 1596–1598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aoki, T.; Fukuoka, H.; Inatomi, T.; Horiuchi, N.; Kamei, K.; Sotozono, C. A Case of Black Fungal Keratitis Caused by Biatriospora mackinnonii. Cornea 2021, 40, 1344–1347. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela-Lopez, N.; Cano-Lira, J.F.; Stchigel, A.M.; Rivero-Menendez, O.; Alastruey-Izquierdo, A.; Guarro, J. Neocucurbitaria keratinophila: An emerging opportunistic fungus causing superficial mycosis in Spain. Med. Mycol. 2019, 57, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Guégan, S.; Garcia-Hermoso, D.; Sitbon, K.; Ahmed, S.; Moguelet, P.; Dromer, F.; Lortholary, O.; Ait-Ammar, N.; Dunand, J.; Levy, B.; et al. Ten-Year Experience of Cutaneous and/or Subcutaneous Infections Due to Coelomycetes in France. Open Forum Infect. Dis. 2016, 3, ofw106. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, A.; Meis, J.; Guarro, J.; de Hoog, G.; Kathuria, S.; Arendrup, M.; Arikan-Akdagli, S.; Akova, M.; Boekhout, T.; Caira, M.; et al. ESCMID and ECMM joint clinical guidelines for the diagnosis and management of systemic phaeohyphomycosis: Diseases caused by black fungi. Clin. Microbiol. Infect. 2014, 20 (Suppl. S3), 47–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donovan, C.; Arenas, E.; Ayyala, R.S.; Margo, C.E.; Espana, E.M. Fungal keratitis: Mechanisms of infection and management strategies. Surv. Ophthalmol. 2021, 67, 758–769. [Google Scholar] [CrossRef] [PubMed]
- Prajna, N.V.; Krishnan, T.; Rajaraman, R.; Patel, S.; Shah, R.; Srinivasan, M.; Das, M.; Ray, K.J.; Oldenburg, C.E.; McLeod, S.D.; et al. Predictors of Corneal Perforation or Need for Therapeutic Keratoplasty in Severe Fungal Keratitis: A Secondary Analysis of the Mycotic Ulcer Treatment Trial II. JAMA Ophthalmol. 2017, 135, 987–991. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sáenz-Madrazo, N.; Baeza, A.; Guinea, J.; Martín-Rabadán, P.; Ruiz-Velasco-Santacruz, A.; Urcelay, J.L. First Report of Neocucurbitaria unguis-hominis Keratitis. J. Fungi 2023, 9, 8. https://doi.org/10.3390/jof9010008
Sáenz-Madrazo N, Baeza A, Guinea J, Martín-Rabadán P, Ruiz-Velasco-Santacruz A, Urcelay JL. First Report of Neocucurbitaria unguis-hominis Keratitis. Journal of Fungi. 2023; 9(1):8. https://doi.org/10.3390/jof9010008
Chicago/Turabian StyleSáenz-Madrazo, Nerea, Azucena Baeza, Jesús Guinea, Pablo Martín-Rabadán, Alejandro Ruiz-Velasco-Santacruz, and José Luis Urcelay. 2023. "First Report of Neocucurbitaria unguis-hominis Keratitis" Journal of Fungi 9, no. 1: 8. https://doi.org/10.3390/jof9010008