
High Incidence of Candidemia in Critically Ill COVID-19 Patients Supported by Veno-Venous Extracorporeal Membrane Oxygenation: A Retrospective Study
 , , , , , , , , , , and
, , , , , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design of the Study, Population, Settings, Data Collection and Outcomes
2.2. Diagnosis of SARS-CoV-2 Infection
2.3. COVID-19 Treatments
2.4. Sample Collection and Microbiological Analysis
2.5. Clinical Definitions
2.6. Statistical Analysis
2.7. Ethics Committee Approval
3. Results
3.1. Characteristics of the Patients
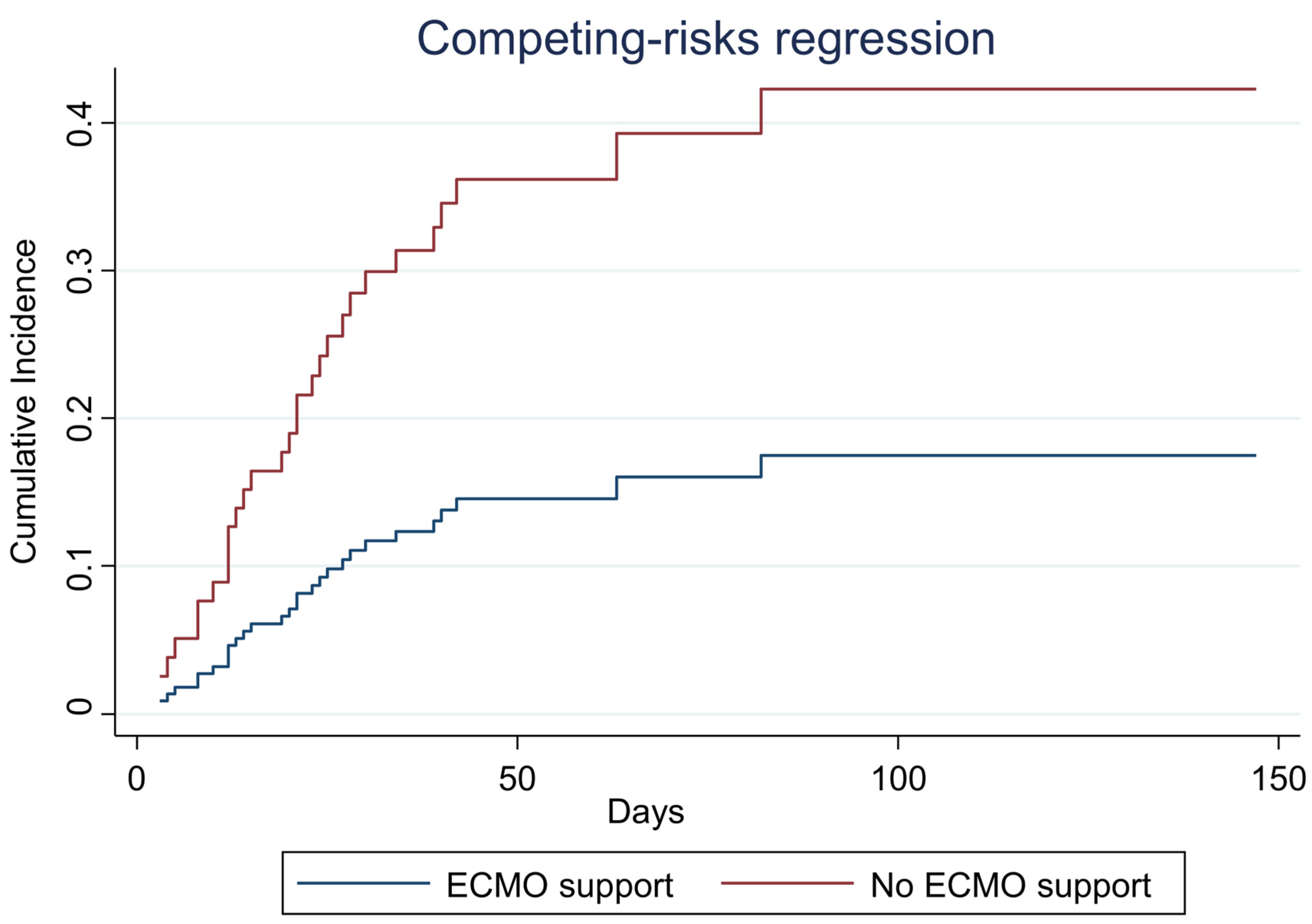
3.2. Impact of ECMO Support on Candidaemia
3.3. Stratified Analysis of Predictor for Candidaemia
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Brandi, N.; Ciccarese, F.; Balacchi, C.; Rimondi, M.R.; Modolon, C.; Sportoletti, C.; Capozzi, C.; Renzulli, M.; Paccapelo, A.; Castelli, A.; et al. Co-Infections and Superinfections in COVID-19 Critically Ill Patients Are Associated with CT Imaging Abnormalities and the Worst Outcomes. Diagnostics 2022, 12, 1617. [Google Scholar] [CrossRef] [PubMed]
- Baddley, J.W.; Thompson, G.R., III; Chen, S.C.A.; White, P.L.; Johnson, M.D.; Nguyen, M.H.; Schwartz, I.S.; Spec, A.; Ostrosky- Zeichner, L.; Jackson, B.R.; et al. Coronavirus Disease 2019–Associated Invasive Fungal Infection. Open Forum Infect. Dis. 2021, 8, ofab510. [Google Scholar] [CrossRef]
- Gangneux, J.P.; Dannaoui, E.; Fekkar, A.; Luyt, C.E.; Botterel, F.; De Prost, N.; Tadié, J.M.; Reizine, F.; Houzé, S.; Timsit, J.F.; et al. Fungal infections in mechanically ventilated patients with COVID-19 during the first wave: The French multicentre MYCOVID study. Lancet Respir. Med. 2022, 10, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Kayaaslan, B.; Eser, F.; Kaya Kalem, A.; Bilgic, Z.; Asilturk, D.; Hasanoglu, I.; Ayhan, M.; Tezer Tekce, Y.; Erdem, D.; Turan, S.; et al. Characteristics of candidemia in COVID-19 patients; increased incidence, earlier occurrence and higher mortality rates compared to non-COVID-19 patients. Mycoses 2021, 64, 1083–1091. [Google Scholar] [CrossRef] [PubMed]
- Kaur, H.; Shankarnarayana, S.A.; Hallur, V.; Muralidharan, J.; Biswal, M.; Ghosh, A.K.; Ray, P.; Chakrabarti, A.; Rudramurthy, S.M. Prolonged Outbreak of Candida krusei Candidemia in Paediatric Ward of Tertiary Care Hospital. Mycopathologia 2020, 185, 257–268. [Google Scholar] [CrossRef]
- Oliva, A.; Miele, M.C.; Di Timoteo, F.; De Angelis, M.; Mauro, V.; Aronica, R.; Al Ismail, D.; Ceccarelli, G.; Pinacchio, C.; d’Ettorre, G.; et al. Persistent Systemic Microbial Translocation and Intestinal Damage During Coronavirus Disease-19. Front. Immunol. 2021, 12, 708149. [Google Scholar] [CrossRef]
- Bastard, P.; Gervais, A.; Le Voyer, T.; Rosain, J.; Philippot, Q.; Manry, J.; Michailidis, E.; Hoffmann, H.H.; Eto, S.; Garcia-Prat, M.; et al. Autoantibodies neutralizing type I IFNs are present in ~4% of uninfected individuals over 70 years old and account for ~20% of COVID-19 deaths. Sci. Immunol. 2021, 6, eabl4340. [Google Scholar] [CrossRef]
- Aubron, C.; Cheng, A.C.; Pilcher, D.; Leong, T.; Magrin, G.; Cooper, D.J.; Scheinkestel, C.; Pellegrino, V. Infections acquired by adults who receive extracorporeal membrane oxygenation: Risk factors and outcome. Infect. Control Hosp. Epidemiol. 2013, 34, 24–30. [Google Scholar] [CrossRef] [Green Version]
- Poissy, J.; Damonti, L.; Bignon, A.; Khanna, N.; Von Kietzell, M.; Boggian, K.; Neofytos, D.; Vuotto, F.; Coiteux, V.; Artru, F.; et al. Risk factors for candidemia: A prospective matched case-control study. Crit. Care 2020, 24, 109. [Google Scholar] [CrossRef]
- Kett, D.H.; Azoulay, E.; Echeverria, P.M.; Vincent, J.L. Extended Prevalence of Infection in ICU Study (EPIC II) Group of Investigators. Candida bloodstream infections in intensive care units: Analysis of the extended prevalence of infection in intensive care unit study. Crit. Care Med. 2011, 39, 665–670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poth, J.M.; Schewe, J.C.; Putensen, C.; Ehrentraut, S.F. Impact of Invasive Fungal Diseases on Survival under Veno-Venous Extracorporeal Membrane Oxygenation for ARDS. J. Clin. Med. 2022, 11, 1940. [Google Scholar] [CrossRef]
- Monk, E.J.M.; Rautemaa-Richardson, R.; Felton, T.; Montalti, A.; Parkes, M.; Templeton, R.; Ashworth, A.; Garcia, M.; Barker, J.; Thomas, S. Incidence of candidaemia in prolonged venovenous extracorporeal membrane oxygenation. J. Hosp. Infect. 2022, 119, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Tonna, J.E.; Abrams, D.; Brodie, D.; Greenwood, J.C.; Mateo-Sidron, J.A.R.; Usman, A.; Fan, E. Management of Adult Patients Supported with Venovenous Extracorporeal Membrane Oxygenation (VV ECMO): Guideline from the Extracorporeal Life Support Organization (ELSO). ASAIO J. 2021, 67, 601–610. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Case Definition for Coronavirus Disease 2019 (COVID-19). 2020. Available online: https://www.ecdc.europa.eu/en/covid-19/surveillance/case-definition (accessed on 1 February 2021).
- World Health Organization. Clinical Management of COVID-19: Interim Guidance. World Health Organization. 2020. Available online: https://apps.who.int/iris/handle/10665/332196 (accessed on 27 May 2020).
- Mussini, C.; Falcone, M.; Nozza, S.; Sagnelli, C.; Parrella, R.; Meschiari, M.; Petrosillo, N.; Mastroianni, C.; Cascio, A.; Iaria, C.; et al. Italian Society of Infectious and Tropical Diseases. Therapeutic strategies for severe COVID-19: A position paper from the Italian Society of Infectious and Tropical Diseases (SIMIT). Clin. Microbiol. Infect. 2021, 27, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Eucast: EUCAST. Available online: https://www.eucast.org (accessed on 24 December 2022).
- Cornely, O.A.; Bassetti, M.; Calandra, T.; Garbino, J.; Kullberg, B.J.; Lortholary, O.; Meersseman, W.; Akova, M.; Arendrup, M.C.; Arikan-Akdagli, S. ESCMID guideline for the diagnosis and management of Candida diseases 2012: Non-neutropenic adult patients. Clin. Microbiol. Infect. 2012, 18 (Suppl. 7), 19–37. [Google Scholar] [CrossRef] [Green Version]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- ARDS Definition Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar]
- León, C.; Ruiz-Santana, S.; Saavedra, P.; Almirante, B.; Nolla-Salas, J.; Álvarez-Lerma, F.; Garnacho-Montero, J.; León, M.A.; EPCAN Study Group. A bedside scoring system (“Candida score”) for early antifungal treatment in nonneutropenic critically ill patients with Candida colonization. Crit. Care Med. 2006, 34, 730–737. [Google Scholar] [CrossRef]
- Vittinghoff, E.; Mc Culloch, C.E. Relaxing the rule of ten events per variable in logistic and Cox regression. Am. J. Epidemiol. 2007, 165, 710–718. [Google Scholar] [CrossRef] [Green Version]
- Mastrangelo, A.; Germinario, B.N.; Ferrante, M.; Frangi, C.; Li Voti, R.; Muccini, C.; Ripa, M. Candidemia in Coronavirus Disease 2019 (COVID-19) Patients: Incidence and Characteristics in a Prospective Cohort Compared With Historical Non-COVID-19 Controls. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 73, e2838–e2839. [Google Scholar] [CrossRef] [PubMed]
- Blaize, M.; Raoelina, A.; Kornblum, D.; Kamus, L.; Lampros, A.; Berger, M.; Demeret, S.; Constantin, J.M.; Monsel, A.; Mayaux, J.; et al. Occurrence of Candidemia in Patients with COVID-19 Admitted to Five ICUs in France. J. Fungi 2022, 8, 678. [Google Scholar] [CrossRef] [PubMed]
- Eggimann, P.; Que, Y.A.; Revelly, J.P.; Pagani, J.J. Preventing invasive Candida infections. where could we do better? J. Hosp. Infect. 2015, 89, 302–308. [Google Scholar] [CrossRef] [Green Version]
- Akhtar, N.; Khurshid Wani, A.; Kant Tripathi, S.; Prakash, A.; Amin-Ul Mannan, M. The role of SARS-CoV-2 immunosuppression and the therapy used to manage COVID-19 disease in the emergence of opportunistic fungal infections: A review. Curr. Res. Biotechnol. 2022, 4, 337–349. [Google Scholar] [CrossRef] [PubMed]
- Krause, R.; Schwab, E.; Bachhiesl, D.; Daxböck, F.; Wenisch, C.; Krejs, G.J.; Reisinger, E.C. Role of Candida in antibiotic-associated diarrhea. J. Infect. Dis. 2001, 184, 1065–1069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceccarelli, G.; Alessandri, F.; Oliva, A.; Borrazzo, C.; Dell’Isola, S.; Ialungo, A.M.; Rastrelli, E.; Pelli, M.; Raponi, G.; Turriziani, O.; et al. The role of teicoplanin in the treatment of SARS-CoV-2 infection: A retrospective study in critically ill COVID-19 patients (Tei-COVID study). J. Med. Virol. 2021, 93, 4319–4325. [Google Scholar] [CrossRef]
- Rocchi, G.; Giovanetti, M.; Benedetti, F.; Borsetti, A.; Ceccarelli, G.; Zella, D.; Altomare, A.; Ciccozzi, M.; Guarino, M.P.L. Gut Microbiota and COVID-19: Potential Implications for Disease Severity. Pathogens 2022, 11, 1050. [Google Scholar] [CrossRef]
- Yin, Y.S.; Minacapelli, C.D.; Parmar, V.; Catalano, C.C.; Bhurwal, A.; Gupta, K.; Rustgi, V.K.; Blaser, M.J. Alterations of the fecal microbiota in relation to acute COVID-19 infection and recovery. Mol. Biomed. 2022, 3, 36. [Google Scholar] [CrossRef]
- Lv, L.; Gu, S.; Jiang, H.; Yan, R.; Chen, Y.; Chen, Y.; Luo, R.; Huang, C.; Lu, H.; Zheng, B.; et al. Gut mycobiota alterations in patients with COVID-19 and H1N1 infections and their associations with clinical features. Commun. Biol. 2021, 4, 480. [Google Scholar] [CrossRef]
- Zuo, T.; Zhan, H.; Zhang, F.; Liu, Q.; Tso, E.Y.K.; Lui, G.C.Y.; Chen, N.; Li, A.; Lu, W.; Chan, F.K.L.; et al. Alterations in Fecal Fungal Microbiome of Patients With COVID-19 During Time of Hospitalization until Discharge. Gastroenterology 2020, 159, 1302–1310. [Google Scholar] [CrossRef]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. HLH Across Speciality Collaboration, UK. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef] [PubMed]
- Moser, D.; Biere, K.; Han, B.; Hoerl, M.; Schelling, G.; Choukér, A.; Woehrle, T. COVID-19 Impairs Immune Response to Candida albicans. Front. Immunol. 2021, 12, 640644. [Google Scholar] [CrossRef]
- Tóth, R.; Nosek, J.; Mora-Montes, H.M.; Gabaldon, T.; Bliss, J.M.; Nosanchuk, J.D.; Turner, S.A.; Butler, G.; Vágvölgyi, C.; Gácser, A. Candida parapsilosis: From Genes to the Bedside. Clin. Microbiol. Rev. 2019, 32, e00111-18. [Google Scholar] [CrossRef] [Green Version]
- Leroy, G.; Lambiotte, F.; Thévenin, D.; Lemaire, C.; Parmentier, E.; Devos, P.; Leroy, O. Evaluation of “Candida score” in critically ill patients: A prospective, multicenter, observational, cohort study. Ann. Intensive Care. 2011, 1, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seagle, E.E.; Jackson, B.R.; Lockhart, S.R.; Georgacopoulos, O.; Nunnally, N.S.; Roland, J.; Barter, D.M.; Johnston, H.L.; Czaja, C.A.; Kayalioglu, H.; et al. The Landscape of Candidemia During the Coronavirus Disease 2019 (COVID-19) Pandemic. Clin. Infect. Dis. 2022, 74, 802–811. [Google Scholar] [CrossRef] [PubMed]
- Dixit, D.; Jen, P.; Maxwell, T.D.; Smoke, S.; McCracken, J.A.; Cardinale-King, M.; Haribhakti, A.; Patel, P.; Cani, E.; Choi, S.C. Risk Factors and Clinical Outcomes of Candidemia Associated With Severe COVID-19. Crit. Care Explor. 2022, 4, e0762. [Google Scholar] [CrossRef]
- Biffi, S.; Di Bella, S.; Scaravilli, V.; Peri, A.M.; Grasselli, G.; Alagna, L.; Pesenti, A.; Gori, A. Infections during extracorporeal membrane oxygenation: Epidemiology, risk factors, pathogenesis and prevention. Int. J. Antimicrob. Agents 2017, 50, 9–16. [Google Scholar] [CrossRef]
- Kato, R.; Pinsky, M.R. Personalizing blood pressure management in septic shock. Ann. Intensive Care 2015, 5, 41. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| ECMO Support | |||
|---|---|---|---|
| Patients | Yes | No | p-Value |
| N | 45 | 93 | |
| Age, years | 51 (40–58) | 69 (60–76)) | <0.001 |
| Gender | |||
| Male | 34 (75.6) | 63 (67.7) | 0.35 |
| Female | 11 (24.4) | 30 (32.3) | |
| BMI | 29 (25–34) | 28 (26–31) | 0.17 |
| Pre-existing comorbidity | |||
| Chronic obstructive pulmonary disease | 3 (6.7) | 14 (15.1) | 0.16 |
| Diabetes | 8 (17.8) | 18 (19.4) | 0.82 |
| Renal Insufficiency | 0 (0) | 2 (2.2) | 0.32 |
| Hypertension | 13 (28.9) | 45 (48.4) | 0.03 |
| Cardiovascular Disease | 6 (13.3) | 15 (16.1) | 0.67 |
| Chronic liver failure | 4 (8.9) | 0 (0.0) | 0.004 |
| Ever Smoker | 3 (6.7) | 7 (7.5) | 0.86 |
| Ethnicity | 9 (20.0) | 8 (8.6) | 0.056 |
| SAPS II | 24 (24–27) | 34 (28–42) | <0.001 |
| Medical therapy | 45 (100) | 92 (98.9) | 0.49 |
| Antibiotic therapy | 45 (100) | 92 (98.9) | 0.49 |
| Tocilizumab | 5 (11.1) | 22 (23.7) | 0.082 |
| Antiviral Drugs | 23 (51.1) | 54 (58.1) | 0.44 |
| Parenteral nutrition | 22 (48.9) | 32 (34.4) | 0.1 |
| Inotropes | 3 (6.7) | 35 (37.6) | <0.001 |
| Vasopressor | 26 (57.8) | 80 (86.) | <0.001 |
| Prone Therapy | 17 (37.8) | 35 (37.6) | 0.99 |
| ICU Stay, days | 27 (17–38) | 18 (13–27) | <0.001 |
| Lung bacterial superinfection | 27 (60.0) | 52 (55.9) | 0.65 |
| Bacterial colonization | 31 (68.9) | 45 (48.4) | 0.023 |
| BSI | 24 (53.3) | 32 (34.4) | 0.034 |
| Non-candidaemic BSI | 19 (42.2) | 29 (31.2) | 0.2 |
| Candida score | 1 (1–3) | 1 (0–2) | 0.78 |
| Mortality rate | 37 (82.2) | 71 (76.3) | 0.43 |
| ECMO Support | |||
|---|---|---|---|
| Patients | Yes | No | p-Value |
| N | 45 | 93 | |
| Candidaemia | 16 (36.0) | 13 (14.0) | 0.004 |
| Candida species | |||
| albicans/tropicalis | 5 (31.3) | 4 (30.8) | 0.98 |
| Parapsilosis | 11 (68.8) | 9 (69.2) | |
| Candidaemia | ||
|---|---|---|
| aSHR (95% CI) | p-Value | |
| ECMO support | 3.91 (1.73–8.86) | 0.001 |
| Non-candidaemic BSI | 1.61 (0.65–4.01) | 0.308 |
| Tocilizumab therapy | 0.40 (0.12–1.40) | 0.153 |
| Inotropes Therapy | 0.97 (0.29–3.18) | 0.957 |
| Vasopressor Therapy | 0.15 (0.05–0.43) | <0.001 |
| Candida score | 3.04 (2.09–4.42) | <0.001 |
| Propensity score quantiles | 4.15 (1.78–9.64) | 0.001 |
| I quintile | Ref. | |
| II quintile | 1.96 (0.43–8.99) | 0.387 |
| III quintile | 0.68 (0.17–2.80) | 0.593 |
| IV quintile | 0.25 (0.06–1.09) | 0.064 |
| V quintile | 0.52 (0.11–2.44) | 0.408 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alessandri, F.; Ceccarelli, G.; Migliara, G.; Baccolini, V.; Russo, A.; Marzuillo, C.; Ceparano, M.; Giordano, G.; Tozzi, P.; Galardo, G.; et al. High Incidence of Candidemia in Critically Ill COVID-19 Patients Supported by Veno-Venous Extracorporeal Membrane Oxygenation: A Retrospective Study. J. Fungi 2023, 9, 119. https://doi.org/10.3390/jof9010119
Alessandri F, Ceccarelli G, Migliara G, Baccolini V, Russo A, Marzuillo C, Ceparano M, Giordano G, Tozzi P, Galardo G, et al. High Incidence of Candidemia in Critically Ill COVID-19 Patients Supported by Veno-Venous Extracorporeal Membrane Oxygenation: A Retrospective Study. Journal of Fungi. 2023; 9(1):119. https://doi.org/10.3390/jof9010119
Chicago/Turabian StyleAlessandri, Francesco, Giancarlo Ceccarelli, Giuseppe Migliara, Valentina Baccolini, Alessandro Russo, Carolina Marzuillo, Mariateresa Ceparano, Giovanni Giordano, Pierfrancesco Tozzi, Gioacchini Galardo, and et al. 2023. "High Incidence of Candidemia in Critically Ill COVID-19 Patients Supported by Veno-Venous Extracorporeal Membrane Oxygenation: A Retrospective Study" Journal of Fungi 9, no. 1: 119. https://doi.org/10.3390/jof9010119