
Epicardial Adipose Tissue in Patients with Coronary Artery Disease: A Meta-Analysis


Abstract
:1. Introduction
2. Methods
2.1. Literature Search and Selection
2.2. Data Extraction and Quality Assessment
2.3. Statistical Analysis
3. Results
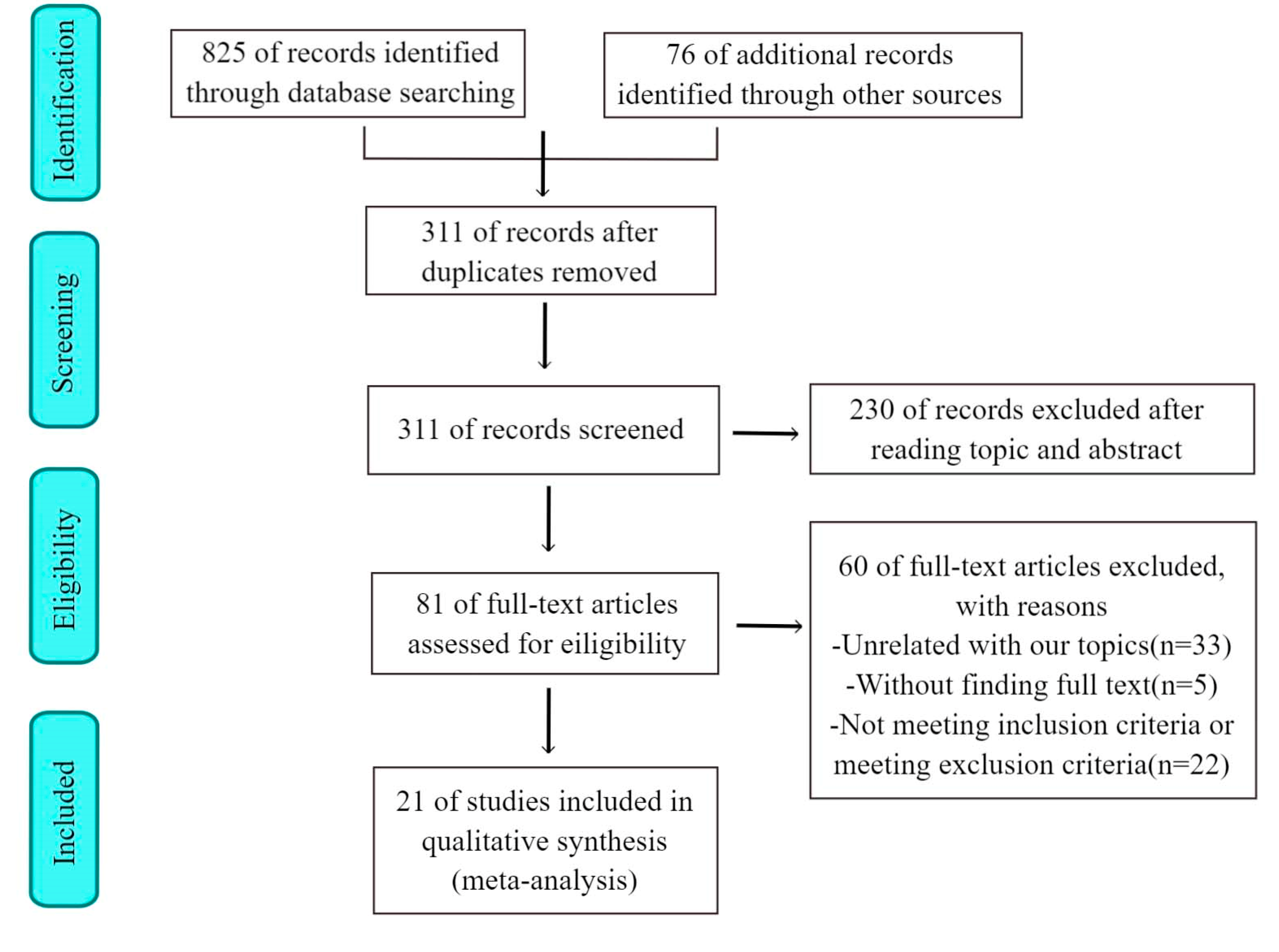
3.1. Study Selection and Quality Assessment
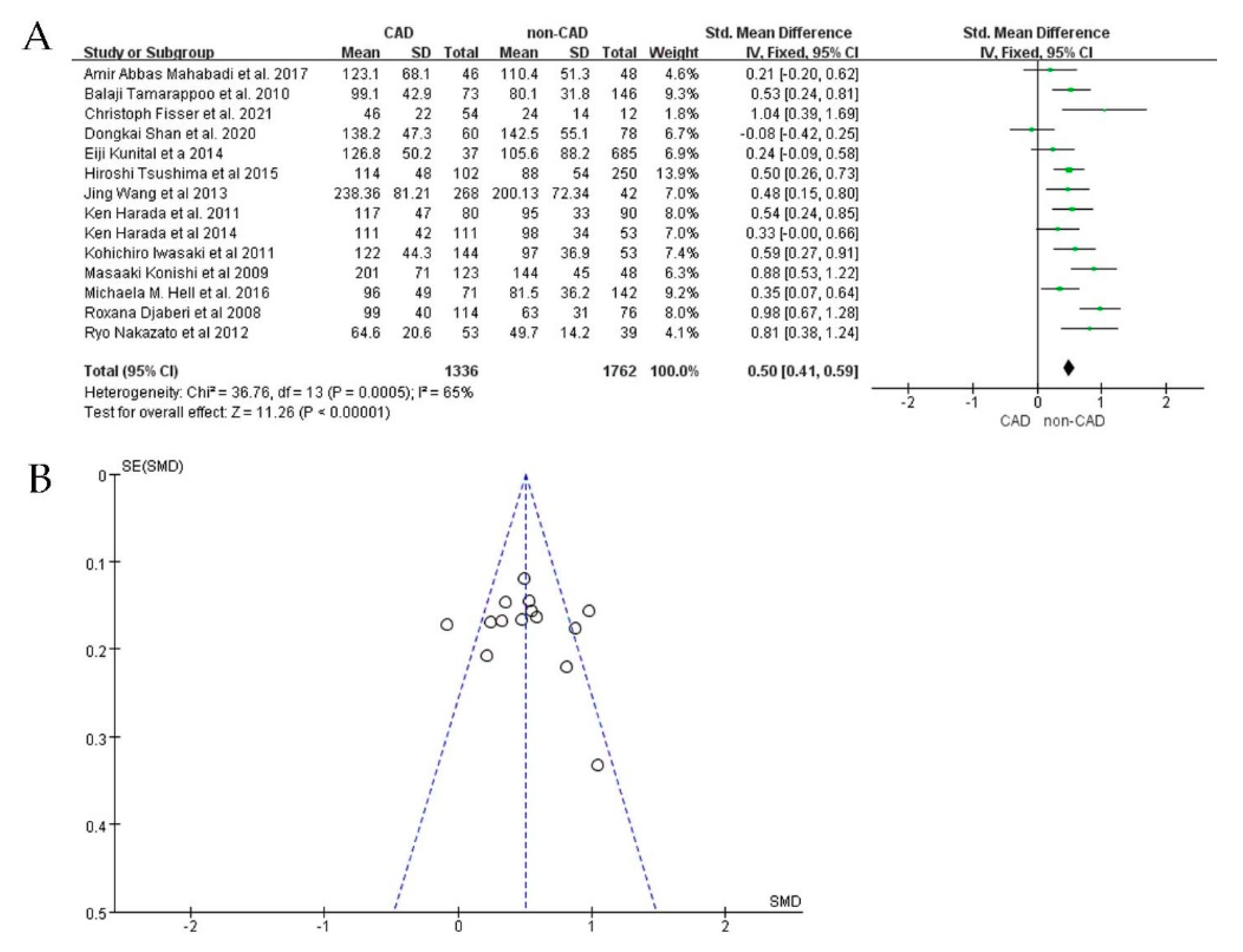
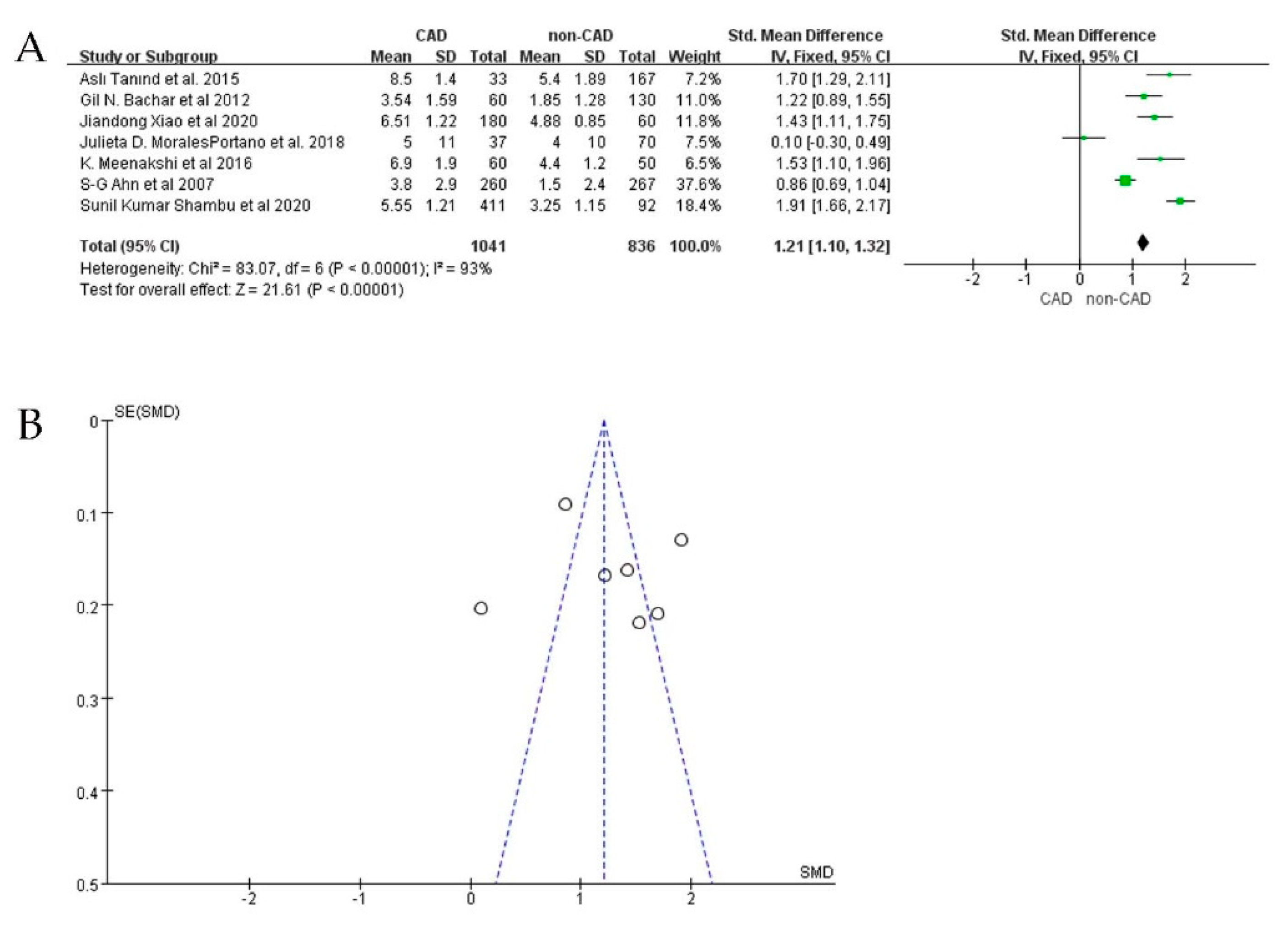
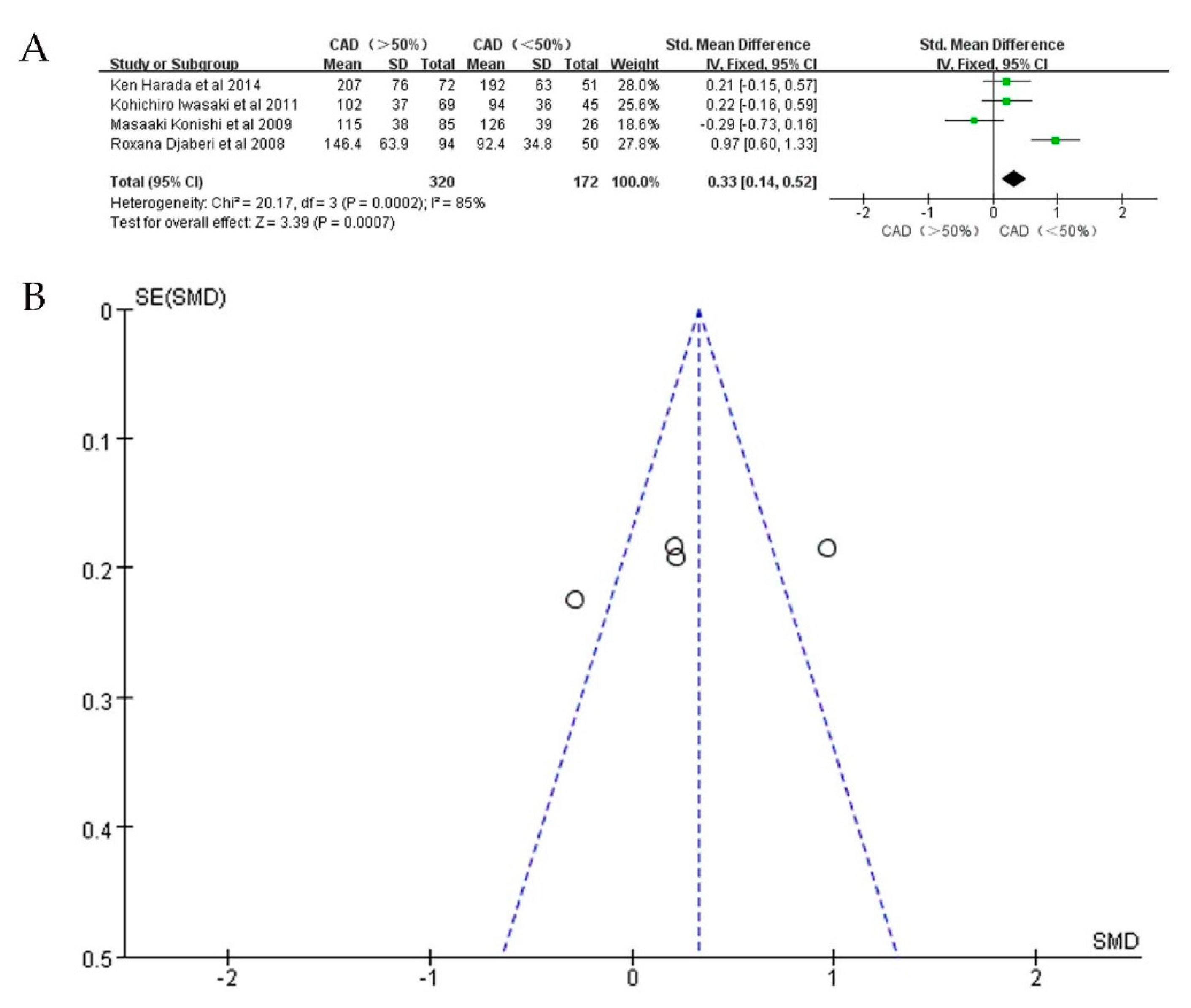
3.2. CAD Group versus Non-CAD Group
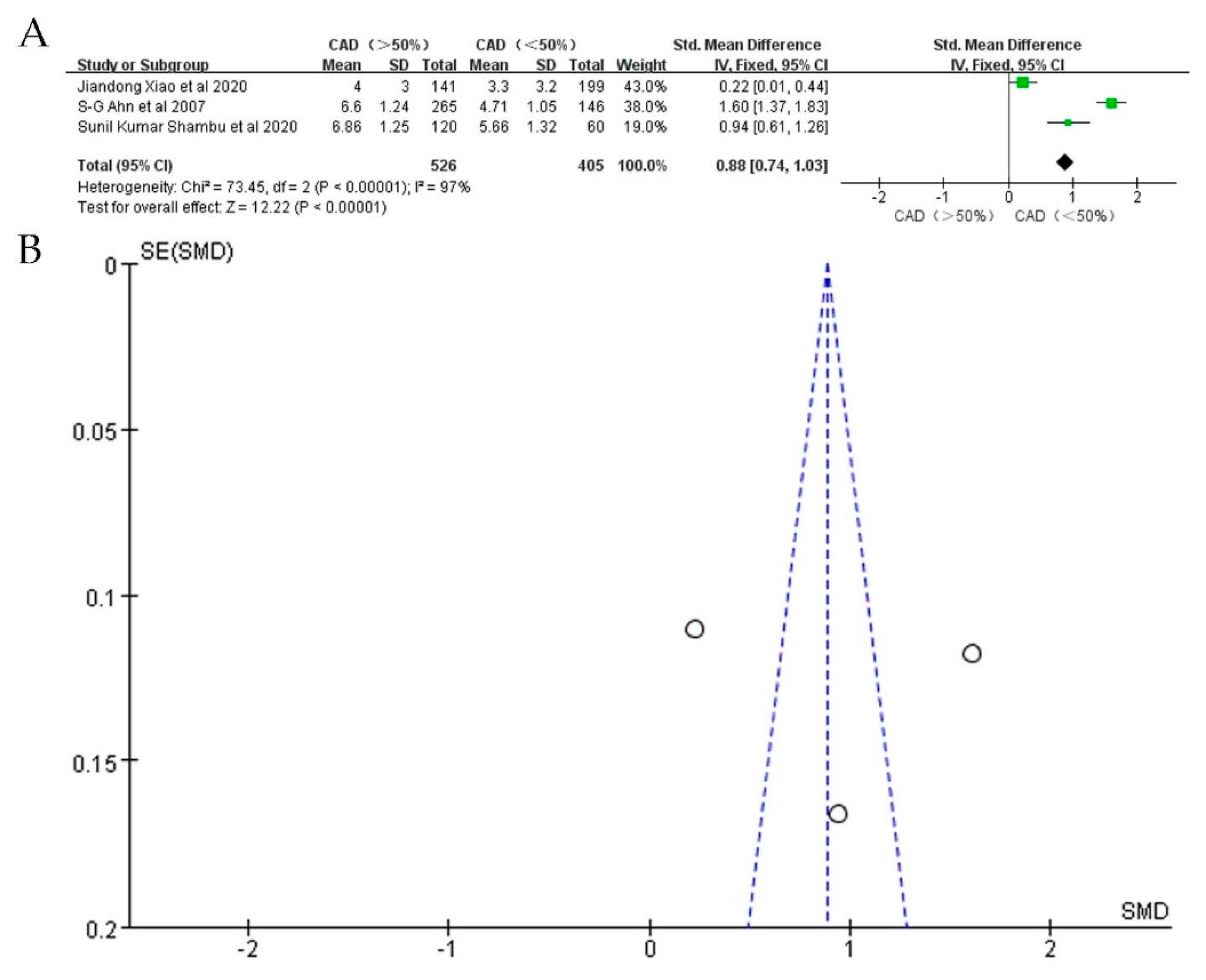
3.3. Subgroup Analysis
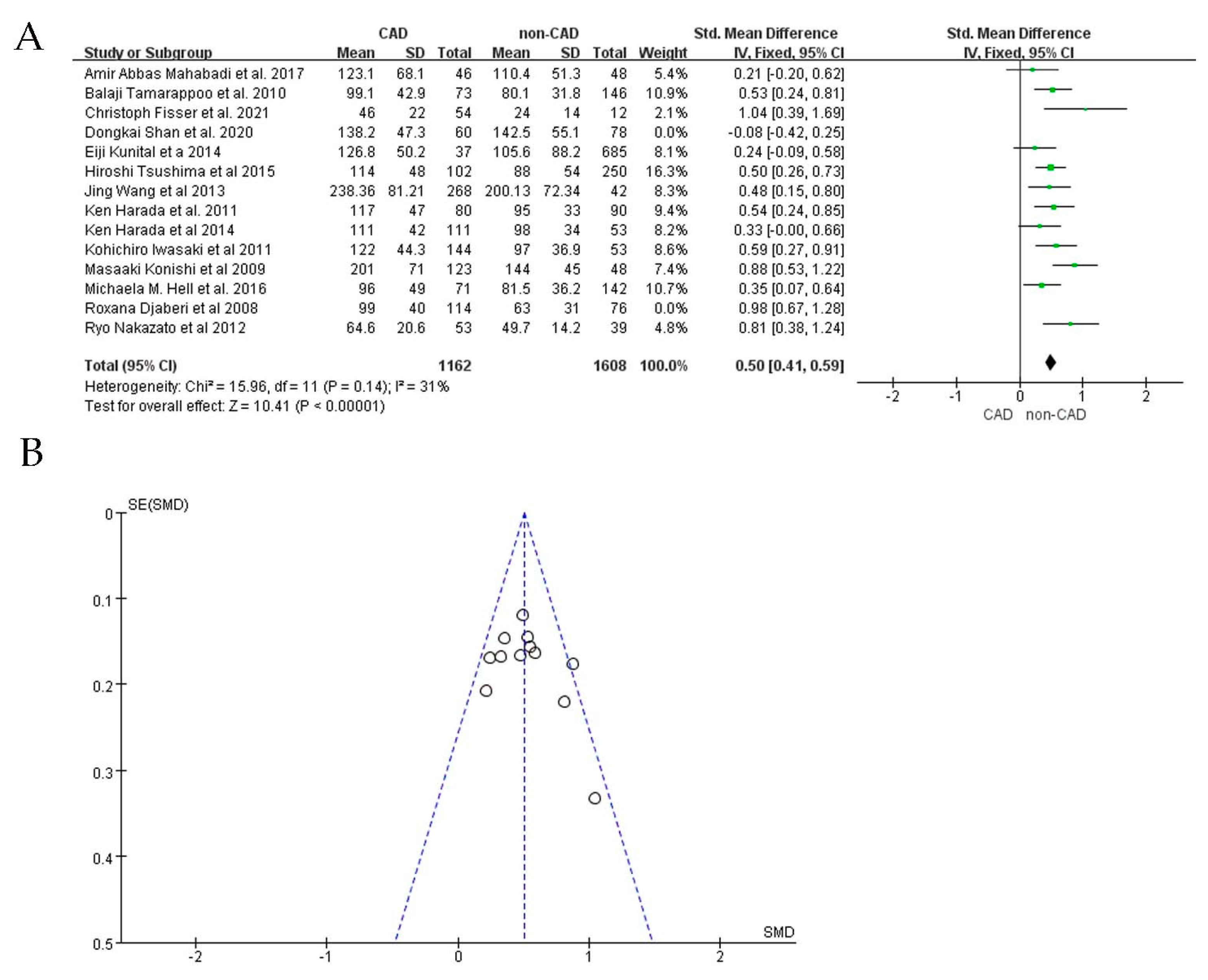
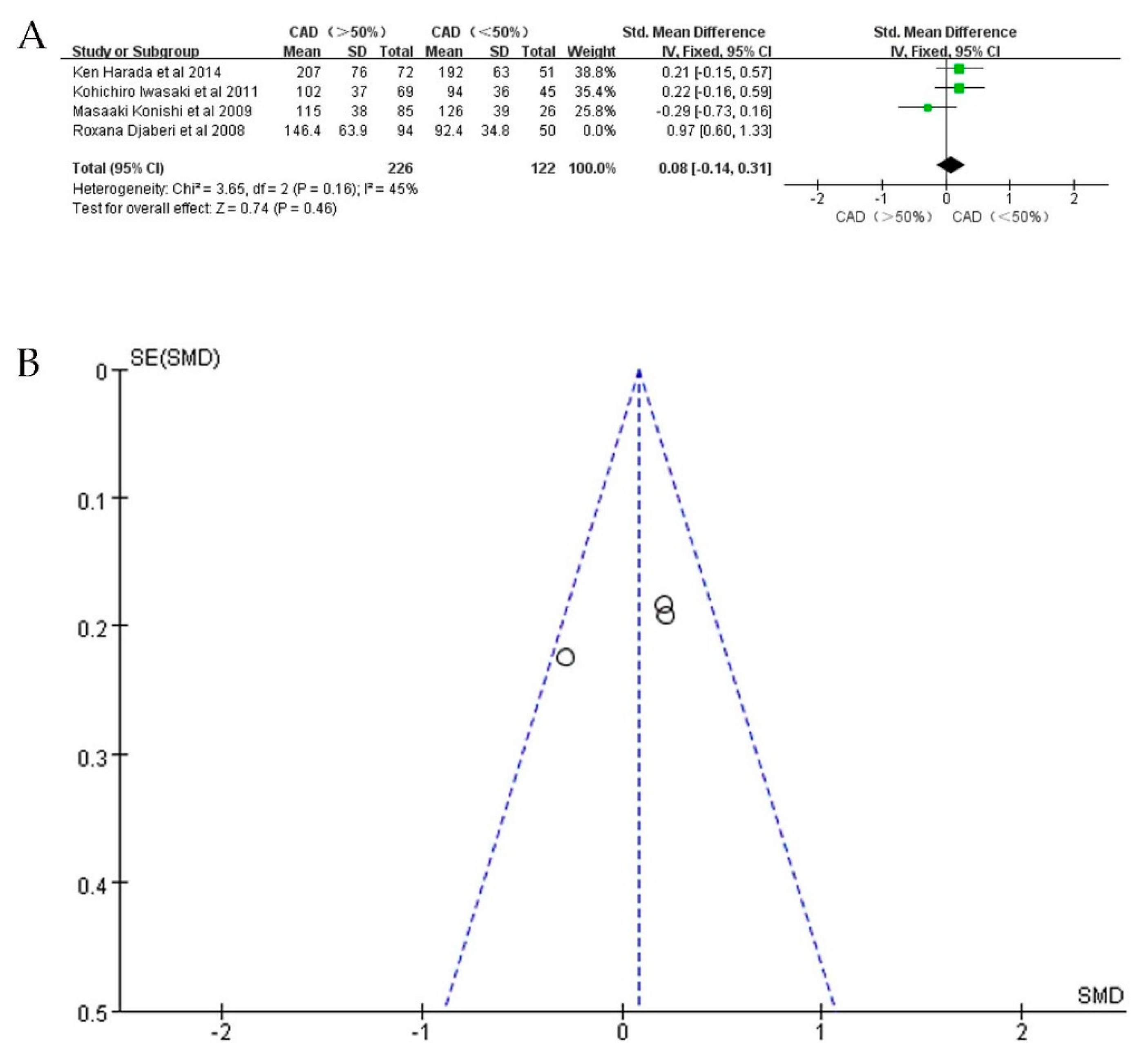
3.4. Publication Bias and Sensitivity Analysis
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khera, A.V.; Kathiresan, S. Genetics of Coronary Artery Disease: Discovery, Biology and Clinical Translation. Nat. Rev. Genet. 2017, 18, 331–344. [Google Scholar] [CrossRef] [PubMed]
- Malakar, A.K.; Choudhury, D.; Halder, B.; Paul, P.; Uddin, A.; Chakraborty, S. A Review on Coronary Artery Disease, Its Risk Factors, and Therapeutics. J. Cell. Physiol. 2019, 234, 16812–16823. [Google Scholar] [CrossRef] [PubMed]
- Fox, K.A.; Metra, M.; Morais, J.; Atar, D. The Myth of ‘Stable’ Coronary Artery Disease. Nat. Rev. Cardiol. 2020, 17, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Sakers, A.; de Siqueira, M.K.; Seale, P.; Villanueva, C.J. Adipose-Tissue Plasticity in Health and Disease. Cell 2022, 185, 419–446. [Google Scholar] [CrossRef]
- Harvey, I.; Boudreau, A.; Stephens, J.M. Adipose Tissue in Health and Disease. Open Biol. 2020, 10, 200291. [Google Scholar] [CrossRef]
- Yan, L.; Ding, S.; Chen, Y.; Xiang, M.; Xie, Y. Cardiac Adipose Tissue Contributes to Cardiac Repair: A Review. Stem Cell Rev. Rep. 2021, 17, 1137–1153. [Google Scholar]
- Gabriela, B.; Miksztowicz, V.; Morales, C.; Barchuk, M. Epicardial Adipose Tissue in Cardiovascular Disease. Adv. Exp. Med. Biol. 2019, 1127, 131–143. [Google Scholar]
- Monti, C.B.; Codari, M.; de Cecco, C.N.; Secchi, F.; Sardanelli, F.; Stillman, A.E. Novel Imaging Biomarkers: Epicardial Adipose Tissue Evaluation. Br. J. Radiol. 2020, 93, 20190770. [Google Scholar] [CrossRef]
- Vishal, V.; Blythe, H.; Wood, E.G.; Sandhar, B.; Sarker, S.-J.; Balmforth, D.; Ambekar, S.G.; Yap, J.; Edmondson, S.J.; di Salvo, C.; et al. Obesity and Diabetes Are Major Risk Factors for Epicardial Adipose Tissue Inflammation. JCI Insight 2021, 6, 16. [Google Scholar]
- McLaughlin, T.; Schnittger, I.; Nagy, A.; Zanley, E.; Xu, Y.; Song, Y.; Nieman, K.; Tremmel, J.A.; Dey, D.; Boyd, J.; et al. Relationship between Coronary Atheroma, Epicardial Adipose Tissue Inflammation, and Adipocyte Differentiation across the Human Myocardial Bridge. J. Am. Heart Assoc. 2021, 10, e021003. [Google Scholar] [CrossRef]
- Gruzdeva, O.V.; Dyleva, Y.A.; Belik, E.V.; Sinitsky, M.Y.; Stasev, A.N.; Kokov, A.N.; Brel, N.K.; Krivkina, E.O.; Bychkova, E.E.; Tarasov, R.S.; et al. Relationship between Epicardial and Coronary Adipose Tissue and the Expression of Adiponectin, Leptin, and Interleukin 6 in Patients with Coronary Artery Disease. J. Pers. Med. 2022, 12, 129. [Google Scholar] [CrossRef]
- Tanaka, K.; Fukuda, D.; Sata, M. Roles of Epicardial Adipose Tissue in the Pathogenesis of Coronary Atherosclerosis—An Update on Recent Findings. Circ. J. 2020, 85, 2–8. [Google Scholar] [CrossRef]
- Ayton, S.L.; Gulsin, G.S.; McCann, G.P.; Moss, A.J. Epicardial Adipose Tissue in Obesity-Related Cardiac Dysfunction. Heart 2022, 108, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Konwerski, M.; Gąsecka, A.; Opolski, G.; Grabowski, M.; Mazurek, T. Role of Epicardial Adipose Tissue in Cardiovascular Diseases: A Review. Biology 2022, 11, 355. [Google Scholar] [CrossRef] [PubMed]
- Yuvaraj, J.; Cheng, K.; Lin, A.; Psaltis, P.J.; Nicholls, S.J.; Wong, D.T.L. The Emerging Role of Ct-Based Imaging in Adipose Tissue and Coronary Inflammation. Cells 2021, 10, 1196. [Google Scholar] [CrossRef] [PubMed]
- Guglielmo, M.; Lin, A.; Dey, D.; Baggiano, A.; Fusini, L.; Muscogiuri, G.; Pontone, G. Epicardial Fat and Coronary Artery Disease: Role of Cardiac Imaging. Atherosclerosis 2021, 321, 30–38. [Google Scholar] [CrossRef]
- Bettencourt, N.; Toschke, A.M.; Leite, D.; Rocha, J.; Carvalho, M.; Sampaio, F.; Xará, S.; Leite-Moreira, A.; Nagel, E.; Gama, V. Epicardial Adipose Tissue Is an Independent Predictor of Coronary Atherosclerotic Burden. Int. J. Cardiol. 2012, 158, 26–32. [Google Scholar] [CrossRef]
- Ledda, R.E.; Milanese, G.; Sverzellati, N. Might Eat Composition Help to Predict Coronary Artery Disease Severity? Int. J. Cardiol. 2021, 327, 39. [Google Scholar] [CrossRef]
- Ansaldo, A.M.; Montecucco, F.; Sahebkar, A.; Dallegri, F.; Carbone, F. Epicardial Adipose Tissue and Cardiovascular Diseases. Int. J. Cardiol. 2019, 278, 254–260. [Google Scholar] [CrossRef]
- Madonna, R.; Massaro, M.; Scoditti, E.; Pescetelli, I.; de Caterina, R. The Epicardial Adipose Tissue and the Coronary Arteries: Dangerous Liaisons. Cardiovasc. Res. 2019, 115, 1013–1025. [Google Scholar] [CrossRef] [Green Version]
- Russo, R.; di Iorio, B.; di Lullo, L.; Russo, D. Epicardial Adipose Tissue: New Parameter for Cardiovascular Risk Assessment in High Risk Populations. J. Nephrol. 2018, 31, 847–853. [Google Scholar] [CrossRef] [PubMed]
- Yamada, H. Epicardial Adipose Tissue Volume Is Not a Simple Marker of Coronary Artery Disease. Int. J. Cardiol. 2021, 322, 45. [Google Scholar] [CrossRef] [PubMed]
- Karampetsou, N.; Alexopoulos, L.; Minia, A.; Pliaka, V.; Tsolakos, N.; Kontzoglou, K.; Perrea, D.N.; Patapis, P. Epicardial Adipose Tissue as an Independent Cardiometabolic Risk Factor for Coronary Artery Disease. Cureus 2022, 14, e25578. [Google Scholar] [CrossRef] [PubMed]
- Mancio, J.; Azevedo, D.; Saraiva, F.; Azevedo, A.I.; Pires-Morais, G.; Leite-Moreira, A.; Falcao-Pires, I.; Lunet, N.; Bettencourt, N. Epicardial Adipose Tissue Volume Assessed by Computed Tomography and Coronary Artery Disease: A Systematic Review and Meta-Analysis. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 490–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajsadeghi, F.; Nabavi, V.; Bhandari, A.; Choi, A.; Vincent, H.; Flores, F.; Budoff, M.; Ahmadi, N. Increased Epicardial Adipose Tissue Is Associated with Coronary Artery Disease and Major Adverse Cardiovascular Events. Atherosclerosis 2014, 237, 486–489. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The Prisma 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Tachibana, M.; Miyoshi, T.; Osawa, K.; Toh, N.; Oe, H.; Nakamura, K.; Naito, T.; Sato, S.; Kanazawa, S.; Ito, H. Measurement of Epicardial Fat Thickness by Transthoracic Echocardiography for Predicting High-Risk Coronary Artery Plaques. Heart Vessel. 2016, 31, 1758–1766. [Google Scholar] [CrossRef]
- Xiao, J.; Lu, Y.; Yang, X. Ultrasound Detection of Epicardial Adipose Tissue Combined with Ischemic Modified Albumin in the Diagnosis of Coronary Heart Disease. Heart Surg. Forum 2020, 23, E461–E464. [Google Scholar] [CrossRef]
- Jia, S.; Liu, Y.; Yuan, J. Evidence in Guidelines for Treatment of Coronary Artery Disease. Adv. Exp. Med. Biol. 2020, 1177, 37–73. [Google Scholar]
- Tran, T.; Small, G.; Cocker, M.; Yam, Y.; Chow, B.J.W. A Single Slice Measure of Epicardial Adipose Tissue Can Serve as an Indirect Measure of Total Epicardial Adipose Tissue Burden and Is Associated with Obstructive Coronary Artery Disease. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 423–430. [Google Scholar] [CrossRef] [Green Version]
- Morales-Portano, J.D.; Peraza-Zaldivar, J.Á.; Suárez-Cuenca, J.A.; Aceves-Millán, R.; Amezcua-Gómez, L.; Ixcamparij-Rosales, C.H.; Trujillo-Cortés, R.; Robledo-Nolasco, R.; Mondragón-Terán, P.; de Vaca, R.P.; et al. Echocardiographic Measurements of Epicardial Adipose Tissue and Comparative Ability to Predict Adverse Cardiovascular Outcomes in Patients with Coronary Artery Disease. Int. J. Cardiovasc. Imaging 2018, 34, 1429–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muthalaly, R.G.; Nerlekar, N.; Wong, D.T.L.; Cameron, J.D.; Seneviratne, S.K.; Ko, B.S. Epicardial Adipose Tissue and Myocardial Ischemia Assessed by Computed Tomography Perfusion Imaging and Invasive Fractional Flow Reserve. J. Cardiovasc. Comput. Tomogr. 2017, 11, 46–53. [Google Scholar] [CrossRef]
- Nabati, M.; Saffar, N.; Yazdani, J.; Parsaee, M.S. Relationship between Epicardial Fat Measured by Echocardiography and Coronary Atherosclerosis: A Single-Blind Historical Cohort Study. Echocardiography 2013, 30, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Shambu, S.K.; Desai, N.; Sundaresh, N.; Babu, M.S.; Madhu, B.; Gona, O.J. Study of Correlation between Epicardial Fat Thickness and Severity of Coronary Artery Disease. Indian Heart J. 2020, 72, 445–447. [Google Scholar] [CrossRef] [PubMed]
- Rajani, R.; Shmilovich, H.; Nakazato, R.; Nakanishi, R.; Otaki, Y.; Cheng, V.Y.; Hayes, S.W.; Thomson, L.E.J.; Friedman, J.D.; Slomka, P.J.; et al. Relationship of Epicardial Fat Volume to Coronary Plaque, Severe Coronary Stenosis, and High-Risk Coronary Plaque Features Assessed by Coronary Ct Angiography. J. Cardiovasc. Comput. Tomogr. 2013, 7, 125–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassan, M.; Said, K.; Rizk, H.; ElMogy, F.; Donya, M.; Houseni, M.; Yacoub, M. Segmental Peri-Coronary Epicardial Adipose Tissue Volume and Coronary Plaque Characteristics. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 1169–1177. [Google Scholar] [CrossRef] [Green Version]
- Hirata, Y.; Yamada, H.; Kusunose, K.; Iwase, T.; Nishio, S.; Hayashi, S.; Bando, M.; Amano, R.; Yamaguchi, K.; Soeki, T.; et al. Clinical Utility of Measuring Epicardial Adipose Tissue Thickness with Echocardiography Using a High-Frequency Linear Probe in Patients with Coronary Artery Disease. J. Am. Soc. Echocardiogr. 2015, 28, 10. [Google Scholar] [CrossRef]
- Chen, O.; Sharma, A.; Ahmad, I.; Bourji, N.; Nestoiter, K.; Hua, P.; Hua, B.; Ivanov, A.; Yossef, J.; Klem, I.; et al. Correlation between Pericardial, Mediastinal, and Intrathoracic Fat Volumes with the Presence and Severity of Coronary Artery Disease, Metabolic Syndrome, and Cardiac Risk Factors. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 37–46. [Google Scholar] [CrossRef] [Green Version]
- Cabrera-Rego, J.O. Echocardiographic Measurement of Epicardial Fat Thickness: In Search for a Consensus/Correlation of Echocardiographic Epicardial Fat Thickness with Severity of Coronary Artery Disease-an Observational Study. Anadolu Kardiyol. Derg. 2012, 12, 5. [Google Scholar]
- Okura, K.; Maeno, K.; Okura, S.; Takemori, H.; Toya, D.; Tanaka, N.; Miyayama, S. Pericardial Fat Volume Is an Independent Risk Factor for the Severity of Coronary Artery Disease in Patients with Preserved Ejection Fraction. J. Cardiol. 2015, 65, 37–41. [Google Scholar] [CrossRef] [Green Version]
- Sulava, E.F.; Johnson, J.C. Management of Coronary Artery Disease. Surg. Clin. North Am. 2022, 102, 449–464. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G.; Willens, H.J. Echocardiographic Epicardial Fat: A Review of Research and Clinical Applications. J. Am. Soc. Echocardiogr. 2009, 22, 12. [Google Scholar] [CrossRef] [PubMed]
- Rosito, G.A.; Massaro, J.M.; Hoffmann, U.; Ruberg, F.L.; Mahabadi, A.A.; Vasan, R.S.; O’Donnell, C.J.; Fox, C.S. Pericardial Fat, Visceral Abdominal Fat, Cardiovascular Disease Risk Factors, and Vascular Calcification in a Community-Based Sample: The Framingham Heart Study. Circulation 2008, 117, 605–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarin, S.; Wenger, C.; Marwaha, A.; Qureshi, A.; Go, B.D.M.; Woomert, C.A.; Clark, K.; Nassef, L.A.; Shirani, J. Clinical Significance of Epicardial Fat Measured Using Cardiac Multislice Computed Tomography. Am. J. Cardiol. 2008, 102, 767–771. [Google Scholar] [CrossRef] [PubMed]
- Tsushima, H.; Yamamoto, H.; Kitagawa, T.; Urabe, Y.; Tatsugami, F.; Awai, K.; Kihara, Y. Association of Epicardial and Abdominal Visceral Adipose Tissue with Coronary Atherosclerosis in Patients with a Coronary Artery Calcium Score of Zero. Circ. J. 2015, 79, 1084–1091. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Wang, L.; Peng, Y.; Zhang, L.; Jiang, S.; Gong, J. Association of Pericardial Adipose Tissue Volume with Presence and Severity of Coronary Atherosclerosis. Clin. Invest. Med. 2013, 36, E143–E150. [Google Scholar] [CrossRef] [Green Version]
- Konishi, M.; Sugiyama, S.; Sugamura, K.; Nozaki, T.; Ohba, K.; Matsubara, J.; Matsuzawa, Y.; Sumida, H.; Nagayoshi, Y.; Nakaura, T.; et al. Association of Pericardial Fat Accumulation Rather Than Abdominal Obesity with Coronary Atherosclerotic Plaque Formation in Patients with Suspected Coronary Artery Disease. Atherosclerosis 2010, 209, 573–578. [Google Scholar] [CrossRef]
- Djaberi, R.; Schuijf, J.D.; van Werkhoven, J.M.; Nucifora, G.; Jukema, J.W.; Bax, J.J. Relation of Epicardial Adipose Tissue to Coronary Atherosclerosis. Am. J. Cardiol. 2008, 102, 1602–1607. [Google Scholar] [CrossRef]
- Nakazato, R.; Dey, D.; Cheng, V.Y.; Gransar, H.; Slomka, P.J.; Hayes, S.W.; Thomson, L.E.J.; Friedman, J.D.; Min, J.K.; Berman, D.S. Epicardial Fat Volume and Concurrent Presence of Both Myocardial Ischemia and Obstructive Coronary Artery Disease. Atherosclerosis 2012, 221, 422–426. [Google Scholar] [CrossRef]
- Harada, K.; Amano, T.; Kataoka, T.; Takeshita, M.; Harada, K.; Kunimura, A.; Takayama, Y.; Shinoda, N.; Kato, B.; Uetani, T.; et al. Impact of Abdominal and Epicardial Fat on the Association between Plasma Adipocytokine Levels and Coronary Atherosclerosis in Non-Obese Patients. Atherosclerosis 2014, 237, 671–676. [Google Scholar] [CrossRef]
- Kunita, E.; Yamamoto, H.; Kitagawa, T.; Ohashi, N.; Oka, T.; Utsunomiya, H.; Urabe, Y.; Tsushima, H.; Awai, K.; Budoff, M.J.; et al. Prognostic Value of Coronary Artery Calcium and Epicardial Adipose Tissue Assessed by Non-Contrast Cardiac Computed Tomography. Atherosclerosis 2014, 233, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, K.; Matsumoto, T.; Aono, H.; Furukawa, H.; Samukawa, M. Relationship between Epicardial Fat Measured by 64-Multidetector Computed Tomography and Coronary Artery Disease. Clin. Cardiol. 2011, 34, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Bachar, G.N.; Dicker, D.; Kornowski, R.; Atar, E. Epicardial Adipose Tissue as a Predictor of Coronary Artery Disease in Asymptomatic Subjects. Am. J. Cardiol. 2012, 110, 534–538. [Google Scholar] [CrossRef]
- Meenakshi, K.; Rajendran, M.; Srikumar, S.; Chidambaram, S. Epicardial Fat Thickness: A Surrogate Marker of Coronary Artery Disease—Assessment by Echocardiography. Indian Heart J. 2016, 68, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Ahn, S.G.; Lim, H.S.; Joe, D.Y.; Kang, S.J.; Choi, B.J.; Choi, S.Y.; Yoon, M.H.; Hwang, G.S.; Tahk, S.J.; Shin, J.H. Relationship of Epicardial Adipose Tissue by Echocardiography to Coronary Artery Disease. Heart 2008, 94, e7. [Google Scholar] [CrossRef] [Green Version]
- Harada, K.; Amano, T.; Uetani, T.; Tokuda, Y.; Kitagawa, K.; Shimbo, Y.; Kunimura, A.; Kumagai, S.; Yoshida, T.; Kato, B.; et al. Cardiac 64-Multislice Computed Tomography Reveals Increased Epicardial Fat Volume in Patients with Acute Coronary Syndrome. Am. J. Cardiol. 2011, 108, 1119–1123. [Google Scholar] [CrossRef]
- Mahabadi, A.A.; Balcer, B.; Dykun, I.; Forsting, M.; Schlosser, T.; Heusch, G.; Rassaf, T. Cardiac Computed Tomography-Derived Epicardial Fat Volume and Attenuation Independently Distinguish Patients with and without Myocardial Infarction. PLoS ONE 2017, 12, e0183514. [Google Scholar] [CrossRef] [Green Version]
- Hell, M.M.; Ding, X.; Rubeaux, M.; Slomka, P.; Gransar, H.; Terzopoulos, D.; Hayes, S.; Marwan, M.; Achenbach, S.; Berman, D.S.; et al. Epicardial Adipose Tissue Volume but Not Density Is an Independent Predictor for Myocardial Ischemia. J. Cardiovasc. Comput. Tomogr. 2016, 10, 141–149. [Google Scholar] [CrossRef]
- Tamarappoo, B.; Dey, D.; Shmilovich, H.; Nakazato, R.; Gransar, H.; Cheng, V.Y.; Friedman, J.D.; Hayes, S.W.; Thomson, L.E.J.; Slomka, P.J.; et al. Increased Pericardial Fat Volume Measured from Noncontrast Ct Predicts Myocardial Ischemia by Spect. JACC Cardiovasc. Imaging 2010, 3, 1104–1112. [Google Scholar] [CrossRef] [Green Version]
- Fisser, C.; Colling, S.; Debl, K.; Hetzenecker, A.; Sterz, U.; Hamer, O.W.; Fellner, C.; Maier, L.S.; Buchner, S.; Arzt, M. The Impact of Epicardial Adipose Tissue in Patients with Acute Myocardial Infarction. Clin. Res. Cardiol. 2021, 110, 1637–1646. [Google Scholar] [CrossRef]
- Shan, D.; Wang, X.; Dou, G.; Zhang, W.; Jing, J.; He, B.; Li, Y.; Chen, Y.; Yang, J. Vascular-Specific Epicardial Adipose Tissue in Predicting Functional Myocardial Ischemia for Patients with Stable Chest Pain. J. Thromb. Thrombolysis 2021, 51, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Tanındı, A.; Kocaman, S.A.; Erkan, A.F.; Uğurlu, M.; Alhan, A.; Töre, H.F. Epicardial Adipose Tissue Thickness Is Associated with Myocardial Infarction and Impaired Coronary Perfusion. Anatol. J. Cardiol. 2015, 15, 224–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaborit, B.; Venteclef, N.; Ancel, P.; Pelloux, V.; Gariboldi, V.; Leprince, P.; Amour, J.; Hatem, S.N.; Jouve, E.; Dutour, A.; et al. Human Epicardial Adipose Tissue Has a Specific Transcriptomic Signature Depending on Its Anatomical Peri-Atrial, Peri-Ventricular, or Peri-Coronary Location. Cardiovasc. Res. 2015, 108, 62–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cherian, S.; Lopaschuk, G.D.; Carvalho, E. Cellular Cross-Talk between Epicardial Adipose Tissue and Myocardium in Relation to the Pathogenesis of Cardiovascular Disease. Am. J. Physiol. Endocrinol. Metab. 2012, 303, E937–E949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villasante Fricke, A.C.; Iacobellis, G. Epicardial Adipose Tissue: Clinical Biomarker of Cardio-Metabolic Risk. Int. J. Mol. Sci. 2019, 20, 5989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gormez, S.; Demirkan, A.; Atalar, F.; Caynak, B.; Erdim, R.; Sozer, V.; Gunay, D.; Akpinar, B.; Ozbek, U.; Buyukdevrim, A.S. Adipose Tissue Gene Expression of Adiponectin, Tumor Necrosis Factor-A and Leptin in Metabolic Syndrome Patients with Coronary Artery Disease. Intern. Med. 2011, 50, 805–810. [Google Scholar] [CrossRef] [Green Version]
- Eiras, S.; Teijeira-Fernández, E.; Shamagian, L.G.; Fernandez, A.L.; Vazquez-Boquete, A.; Gonzalez-Juanatey, J.R. Extension of Coronary Artery Disease Is Associated with Increased Il-6 and Decreased Adiponectin Gene Expression in Epicardial Adipose Tissue. Cytokine 2008, 43, 174–180. [Google Scholar] [CrossRef]
- Yañez-Rivera, T.G.; Baños-Gonzalez, M.A.; Ble-Castillo, J.L.; Torres-Hernandez, M.E.; Torres-Lopez, J.E.; Borrayo-Sanchez, G. Relationship between Epicardial Adipose Tissue, Coronary Artery Disease and Adiponectin in a Mexican Population. Cardiovasc. Ultrasound 2014, 12, 35. [Google Scholar] [CrossRef] [Green Version]
- Zhang, T.; Yang, P.; Li, T.; Gao, J.; Zhang, Y. Leptin Expression in Human Epicardial Adipose Tissue Is Associated with Local Coronary Atherosclerosis. Med. Sci. Monit. 2019, 25, 9913–9922. [Google Scholar] [CrossRef]
- Du, Y.; Ji, Q.; Cai, L.; Huang, F.; Lai, Y.; Liu, Y.; Yu, J.; Han, B.; Zhu, E.; Zhang, J.; et al. Association between Omentin-1 Expression in Human Epicardial Adipose Tissue and Coronary Atherosclerosis. Cardiovasc. Diabetol. 2016, 15, 90. [Google Scholar] [CrossRef] [Green Version]
- Gruzdeva, O.V.; Belik, E.V.; Dyleva, Y.A.; Borodkina, D.A.; Sinitsky, M.Y.; Naumov, D.Y.; Bychkova, E.E.; Fanaskova, E.V.; Palicheva, E.I.; Kuzmina, A.A.; et al. Expression of Adipocytokines in Heart Fat Depots Depending on the Degree of Coronary Artery Atherosclerosis in Patients with Coronary Artery Disease. PLoS ONE 2021, 16, e0248716. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G.; Bianco, A.C. Epicardial Adipose Tissue: Emerging Physiological, Pathophysiological and Clinical Features. Trends Endocrinol. Metab. TEM 2011, 22, 450–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ouwens, D.M.; Sell, H.; Greulich, S.; Eckel, J. The Role of Epicardial and Perivascular Adipose Tissue in the Pathophysiology of Cardiovascular Disease. J. Cell. Mol. Med. 2010, 14, 2223–2234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luna-Luna, M.; Medina-Urrutia, A.; Vargas-Alarcón, G.; Coss-Rovirosa, F.; Vargas-Barrón, J.; Pérez-Méndez, Ó. Adipose Tissue in Metabolic Syndrome: Onset and Progression of Atherosclerosis. Arch. Med. Res. 2015, 46, 392–407. [Google Scholar] [CrossRef]
- Packer, M. Epicardial Adipose Tissue May Mediate Deleterious Effects of Obesity and Inflammation on the Myocardium. J. Am. Coll. Cardiol. 2018, 71, 2360–2372. [Google Scholar] [CrossRef]
- Iwayama, T.; Nitobe, J.; Watanabe, T.; Ishino, M.; Tamura, H.; Nishiyama, S.; Takahashi, H.; Arimoto, T.; Shishido, T.; Miyashita, T.; et al. Role of Epicardial Adipose Tissue in Coronary Artery Disease in Non-Obese Patients. J. Cardiol. 2014, 63, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Lu, Y.; Wang, T.; Zhan, R.; Wang, X.; Ruan, X.; Qi, R.; Huang, S. Effects of Epicardial Adipose Tissue Volume and Density on Cardiac Structure and Function in Patients Free of Coronary Artery Disease. Jpn. J. Radiol. 2020, 38, 666–675. [Google Scholar] [CrossRef]
- Liu, Z.; Wang, S.; Wang, Y.; Zhou, N.; Shu, J.; Stamm, C.; Jiang, M.; Luo, F. Association of Epicardial Adipose Tissue Attenuation with Coronary Atherosclerosis in Patients with a High Risk of Coronary Artery Disease. Atherosclerosis 2019, 284, 230–236. [Google Scholar] [CrossRef]
- Petrini, M.; Alì, M.; Cannaò, P.M.; Zambelli, D.; Cozzi, A.; Codari, M.; Malavazos, A.E.; Secchi, F.; Sardanelli, F. Epicardial Adipose Tissue Volume in Patients with Coronary Artery Disease or Non-Ischaemic Dilated Cardiomyopathy: Evaluation with Cardiac Magnetic Resonance Imaging. Clin. Radiol. 2019, 74, e1–e81. [Google Scholar] [CrossRef]
- Mazurek, T.; Kobylecka, M.; Zielenkiewicz, M.; Kurek, A.; Kochman, J.; Filipiak, K.J.; Mazurek, K.; Huczek, Z.; Królicki, L.; Opolski, G. Pet/Ct Evaluation of F-Fdg Uptake in Pericoronary Adipose Tissue in Patients with Stable Coronary Artery Disease: Independent Predictor of Atherosclerotic Lesions’ Formation? J. Nucl. Cardiol. 2017, 24, 1075–1084. [Google Scholar] [CrossRef]
- Iacobellis, G.; Willens, H.J.; Barbaro, G.; Sharma, A.M. Threshold Values of High-Risk Echocardiographic Epicardial Fat Thickness. Obesity 2008, 16, 887–892. [Google Scholar] [CrossRef] [PubMed]
- Sade, L.E.; Eroglu, S.; Bozbaş, H.; Ozbiçer, S.; Hayran, M.; Haberal, A.; Müderrisoğlu, H. Relation between Epicardial Fat Thickness and Coronary Flow Reserve in Women with Chest Pain and Angiographically Normal Coronary Arteries. Atherosclerosis 2009, 204, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.-W.; Jeong, M.H.; Yun, K.H.; Oh, S.K.; Park, E.M.; Kim, Y.K.; Rhee, S.J.; Lee, E.M.; Lee, J.; Yoo, N.J.; et al. Echocardiographic Epicardial Fat Thickness and Coronary Artery Disease. Circ. J. 2007, 71, 536–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonini-Canterin, F.; Pellegrinet, M.; Marinigh, R.; Favretto, G. Role of Cardiovascular Ultrasound in the Evaluation of Obese Subjects. J. Cardiovasc. Echogr. 2014, 24, 67–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nerlekar, N.; Baey, Y.-W.; Brown, A.J.; Muthalaly, R.G.; Dey, D.; Tamarappoo, B.; Cameron, J.D.; Marwick, T.H.; Wong, D.T. Poor Correlation, Reproducibility, and Agreement between Volumetric Versus Linear Epicardial Adipose Tissue Measurement: A 3d Computed Tomography Versus 2d echocardiography comparison. JACC Cardiovasc. Imaging 2018, 11, 1035–1036. [Google Scholar] [CrossRef]
- Ridker, P.M.; Libby, P.; MacFadyen, J.G.; Thuren, T.; Ballantyne, C.; Fonseca, F.; Koenig, W.; Shimokawa, H.; Everett, B.M.; Glynn, R.J. Modulation of the Interleukin-6 Signalling Pathway and Incidence Rates of Atherosclerotic Events and All-Cause Mortality: Analyses from the Canakinumab Anti-Inflammatory Thrombosis Outcomes Study (Cantos). Eur. Heart J. 2018, 39, 3499–3507. [Google Scholar] [CrossRef] [Green Version]
- Parisi, V.; Petraglia, L.; Formisano, R.; Caruso, A.; Grimaldi, M.G.; Bruzzese, D.; Grieco, F.V.; Conte, M.; Paolillo, S.; Scatteia, A.; et al. Validation of the Echocardiographic Assessment of Epicardial Adipose Tissue Thickness at the Rindfleisch Fold for the Prediction of Coronary Artery Disease. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 99–105. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Country | Study Period | N | Male (%) | Age (yr) | Method | Expression | Study Type | Quality Score |
|---|---|---|---|---|---|---|---|---|---|---|
| Hiroshi Tsushima et al. [45] | 2015 | Japan | 01/2008–04/2013 | 352 | 57 | 61 ± 11 | CT | Volume | Retrospective | 6 |
| Jing Wang et al. [46] | 2013 | China | 12/2006–01/2010 | 310 | 68.4 | 62.69 ± 10.78 | CT | Volume | Retrospective | 6 |
| Masaaki Konishi et al. [47] | 2009 | Japan | 04/2006–12/2008 | 171 | 59 | 60 ± 11 | CT | Volume | Retrospective | 7 |
| Roxana Djaberi et al. [48] | 2008 | The Netherlands | NA | 190 | 55 | 56 ± 12 | CT | Volume | Retrospective | 7 |
| Ryo Nakazato et al. [49] | 2012 | USA | NA | 92 | 68.5 | 71 ± 11 | CT | Volume | Retrospective | 8 |
| Ken Harada et al. [50] | 2014 | Japan | 01/2008–02/2009 | 164 | 70 | 65 ± 10 | CT | Volume | Retrospective | 6 |
| Eiji Kunital et al. [51] | 2014 | Japan | 11/2004–09/2009 | 722 | 61 | 65.0 ± 10.9 | CT | Volume | Retrospective | 6 |
| Kohichiro Iwasaki et al. [52] | 2011 | Japan | 06/2008–05/2009 | 197 | 62.4 | 65.1 ± 9.9 | CT | Volume | Retrospective | 6 |
| Gil N. Bachar et al. [53] | 2012 | Israel | 11/2007–01/2009 | 190 | 85.3 | 56.48 ± 9.2 | CT | Thickness | Retrospective | 6 |
| K. Meenakshi et al. [54] | 2016 | India | NA | 110 | 63.6 | 52.6 ± 0.6 | Echo | Thickness | Retrospective | 6 |
| S-G Ahn et al. [55] | 2007 | Korea | NA | 527 | 50.7 | 58 ± 11 | Echo | Thickness | Prospective | 8 |
| Sunil Kumar Shambu et al. [34] | 2020 | India | 02/2017–01/2019 | 503 | 36.6 | 59.8 ± 12.3 | CT | Thickness | Retrospective | 6 |
| Jiandong Xiao et al. [28] | 2020 | China | 05/2017–12/2018 | 240 | 95.4 | 56.66 ± 8.33 | Echo | Thickness | Retrospective | 6 |
| Ken Harada et al. [56] | 2011 | Japan | 2009–2010 | 170 | 77 | 65 ± 12 | CT | Volume | Prospective | 6 |
| Amir Abbas Mahabadi et al. [57] | 2017 | Germany | 2010–2015 | 94 | 60.6 | 66.9 ± 14.7 | CT | Volume | Retrospective | 6 |
| Michaela M. Hell et al. [58] | 2016 | Germany | 2002–2008 | 213 | 90 | 60 ± 10 | CT | Volume | Prospective | 7 |
| Balaji Tamarappoo et al. [59] | 2010 | American | NA | 219 | 90.4 | 60.3 ± 10.4 | SPECT | Volume | Prospective | 7 |
| Christoph Fisser et al. [60] | 2021 | Germany | NA | 66 | 83.3 | 55 ± 10 | CT | Volume | Prospective | 6 |
| Dongkai Shan et al. [61] | 2020 | China | 2012–2016 | 138 | 66.7 | 61.7 ± 8.9 | CT | Volume | Retrospective | 8 |
| Julieta D. MoralesPorta et al. [31] | 2018 | Korea | 2013–2016 | 107 | 80.4 | 63.6 ± 9.67 | Echo | Thickness | Prospective | 8 |
| Aslı Tanınd et al. [62] | 2015 | Turkey | 2012–2012 | 200 | 80 | 63 ± 13 | Echo | Thickness | Prospective | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Q.; Chi, J.; Wang, C.; Yang, Y.; Tian, R.; Chen, X. Epicardial Adipose Tissue in Patients with Coronary Artery Disease: A Meta-Analysis. J. Cardiovasc. Dev. Dis. 2022, 9, 253. https://doi.org/10.3390/jcdd9080253
Wang Q, Chi J, Wang C, Yang Y, Tian R, Chen X. Epicardial Adipose Tissue in Patients with Coronary Artery Disease: A Meta-Analysis. Journal of Cardiovascular Development and Disease. 2022; 9(8):253. https://doi.org/10.3390/jcdd9080253
Chicago/Turabian StyleWang, Qingpeng, Jiangyang Chi, Chen Wang, Yun Yang, Rui Tian, and Xinzhong Chen. 2022. "Epicardial Adipose Tissue in Patients with Coronary Artery Disease: A Meta-Analysis" Journal of Cardiovascular Development and Disease 9, no. 8: 253. https://doi.org/10.3390/jcdd9080253