
Prognostic Value of High-Sensitivity C-Reactive Protein in In-Stent Restenosis: A Meta-Analysis of Clinical Trials


Abstract
:1. Introduction
2. Materials and Methods
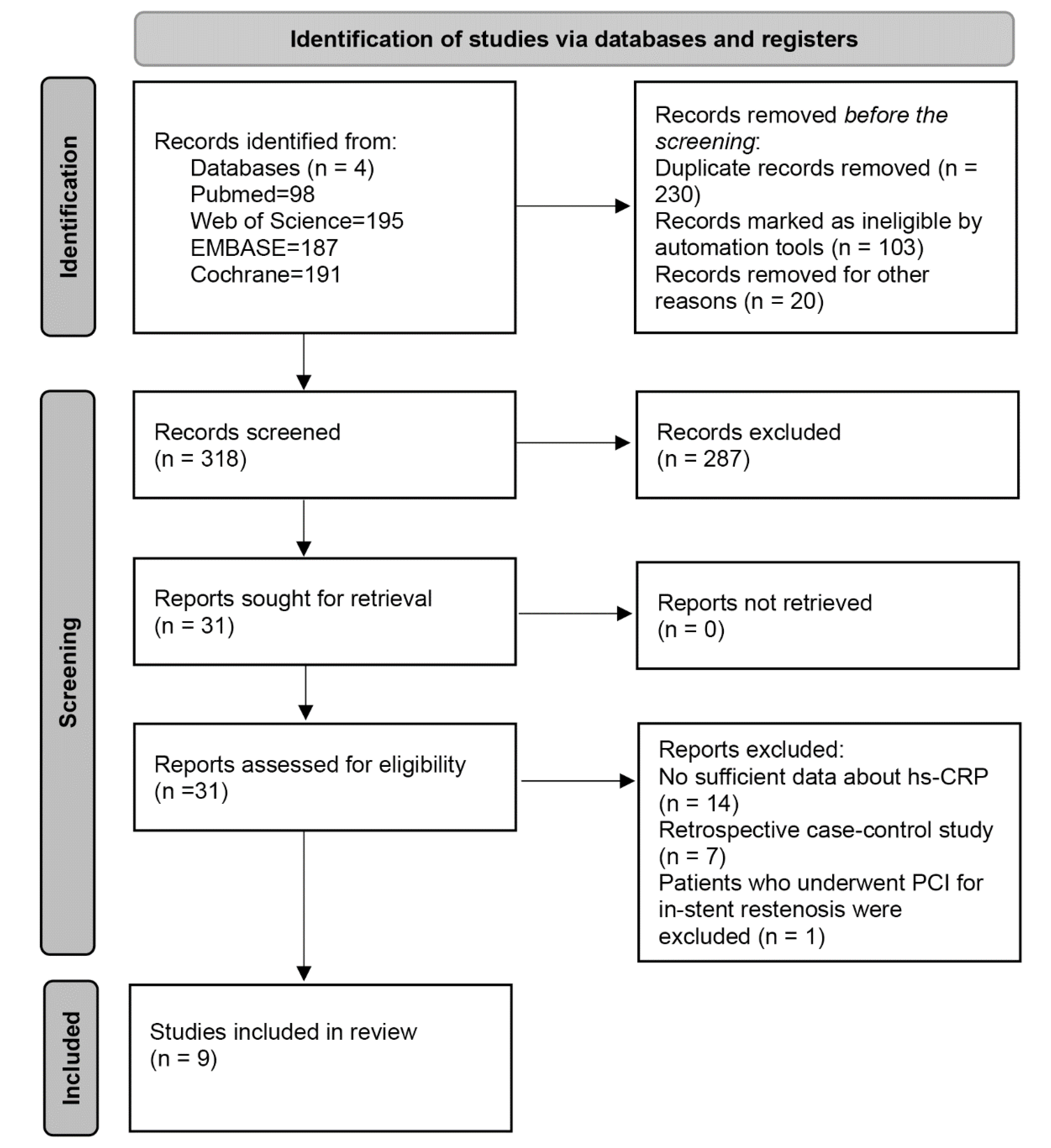
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Endpoint
2.4. Quality Assessment
2.5. Data Extraction
2.6. Statistical Analysis
3. Results
3.1. Search Results and Study Characteristics
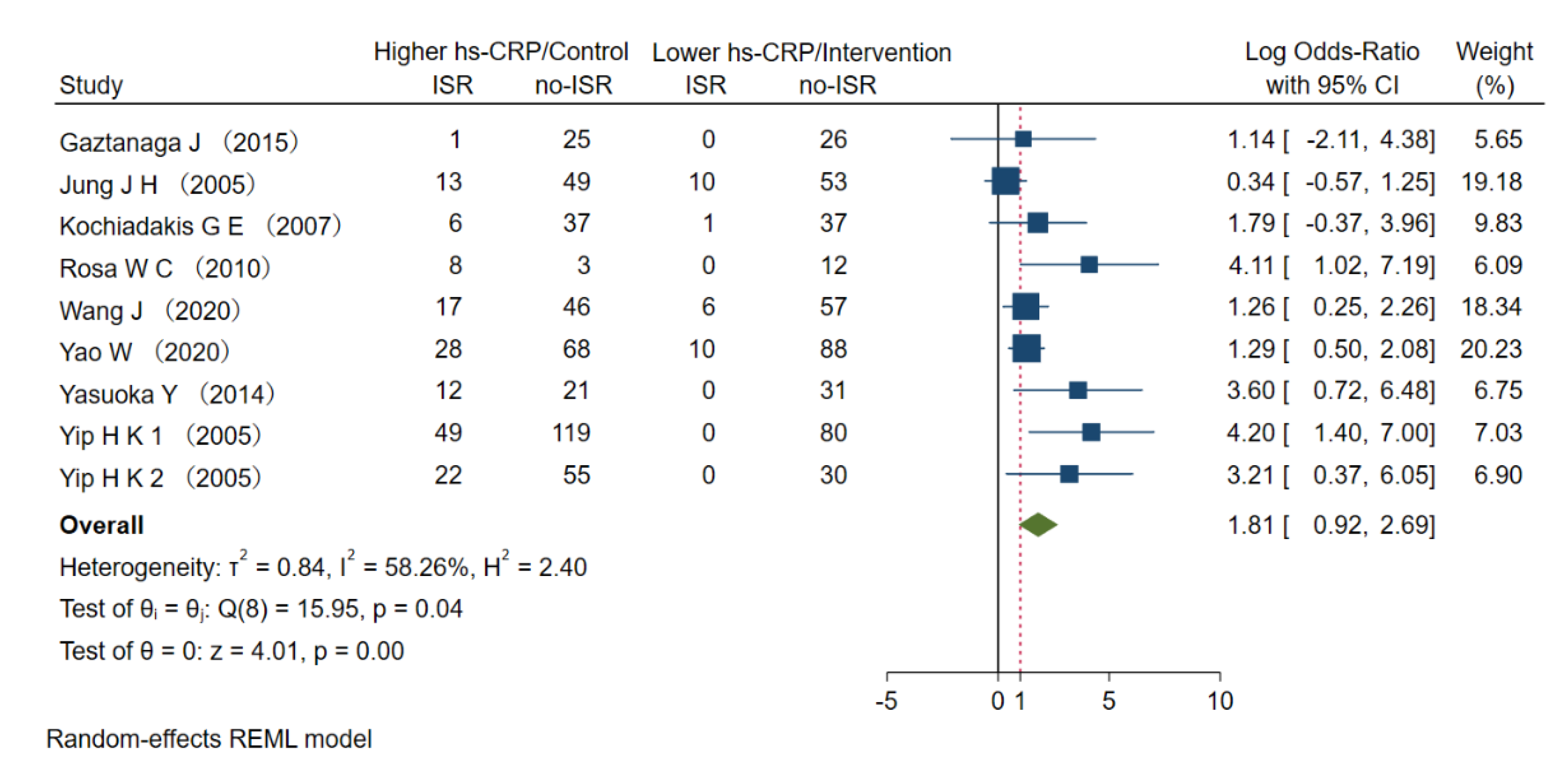
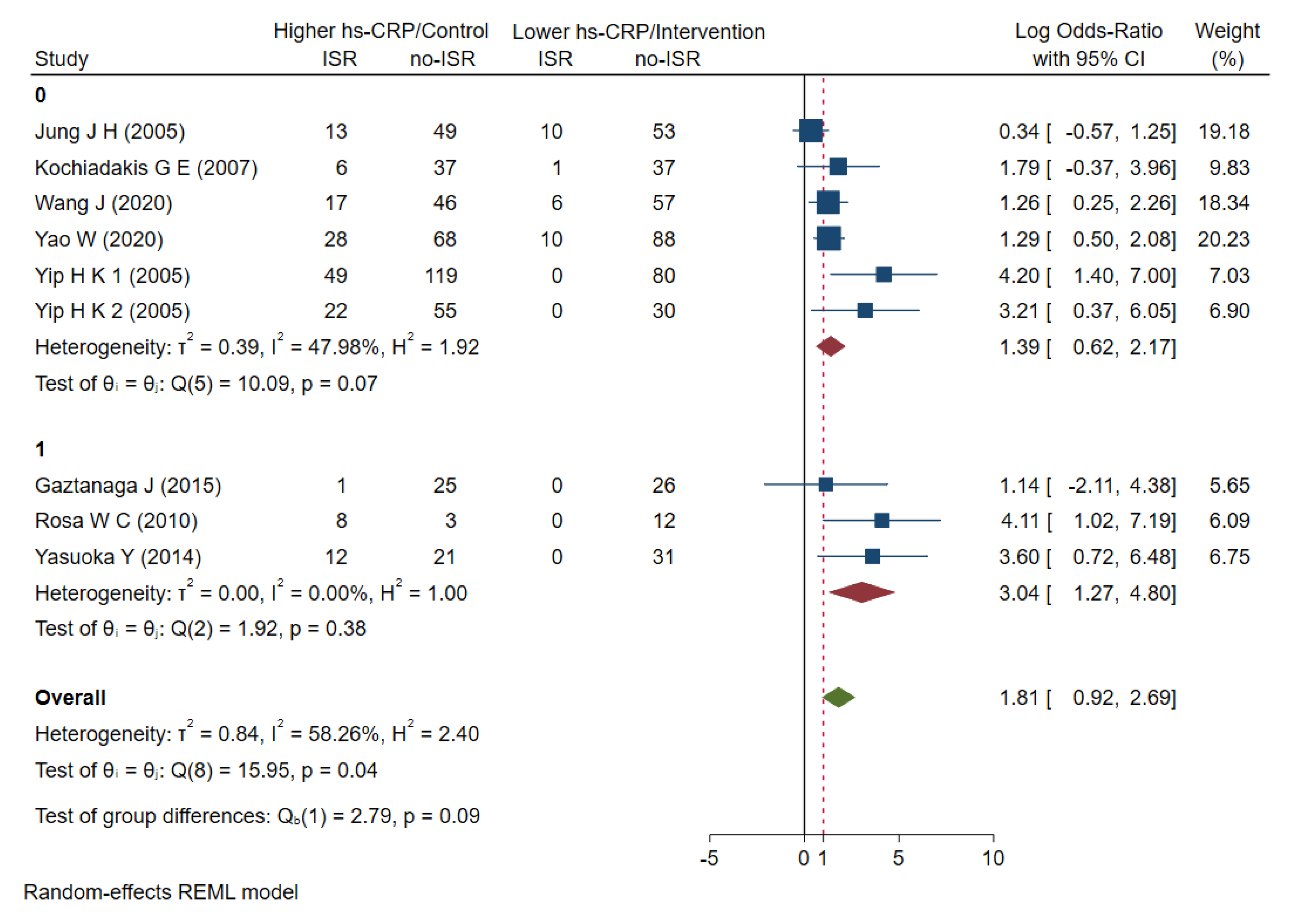
3.2. The Risk of Higher Hs-CRP to ISR
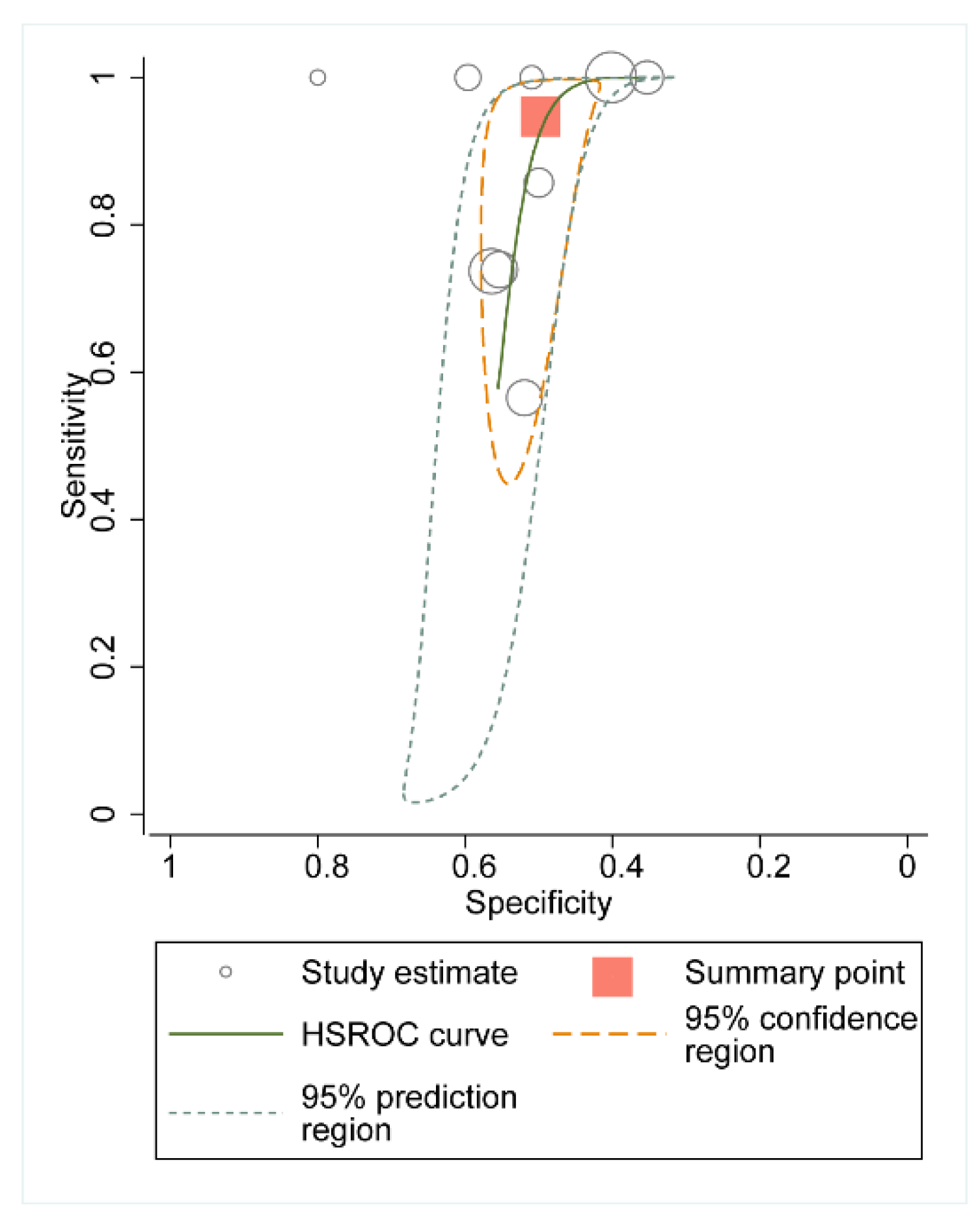
3.3. Summary Receiver Operating Characteristic Curve
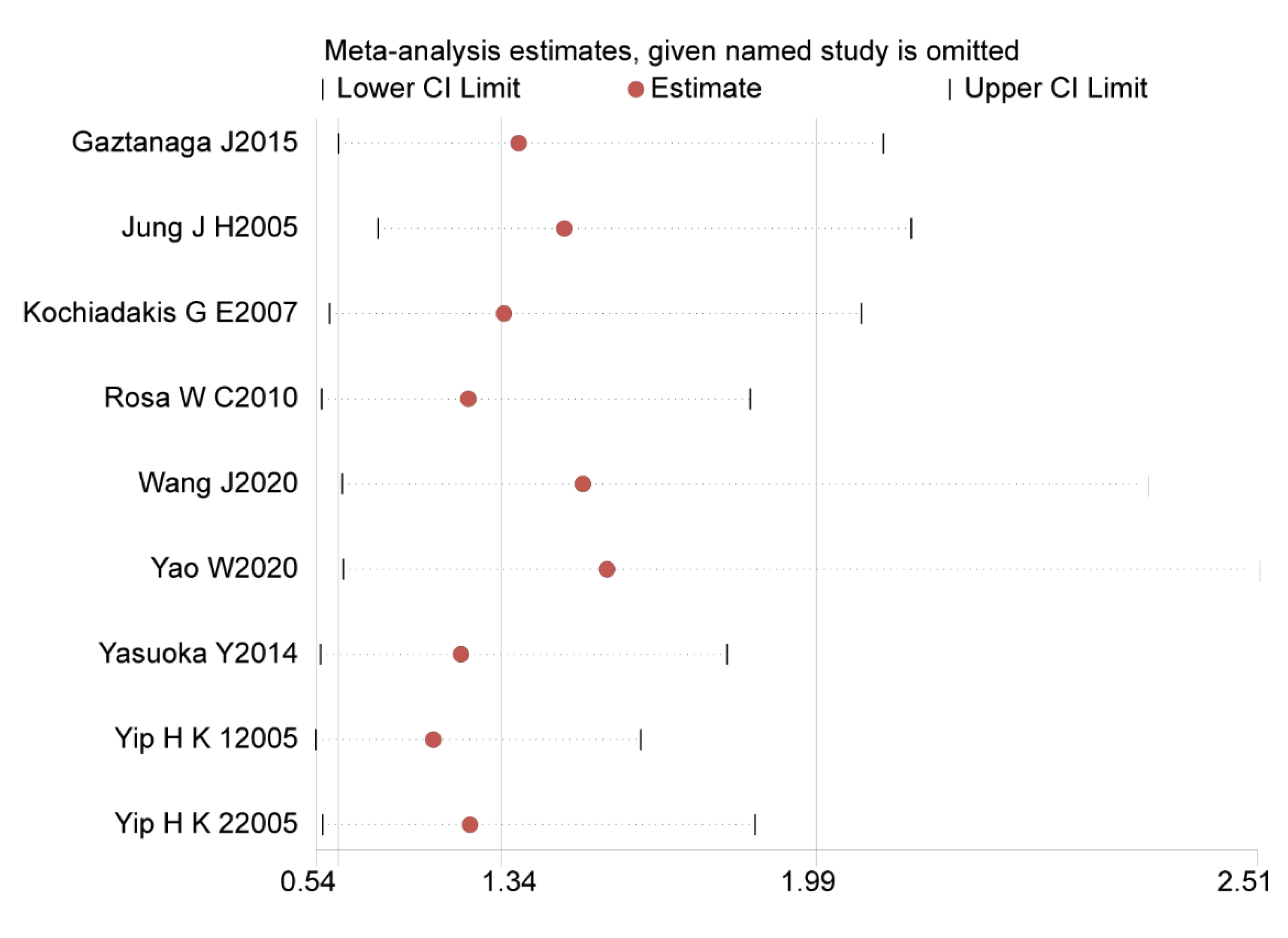
3.4. Sensitivity Analysis
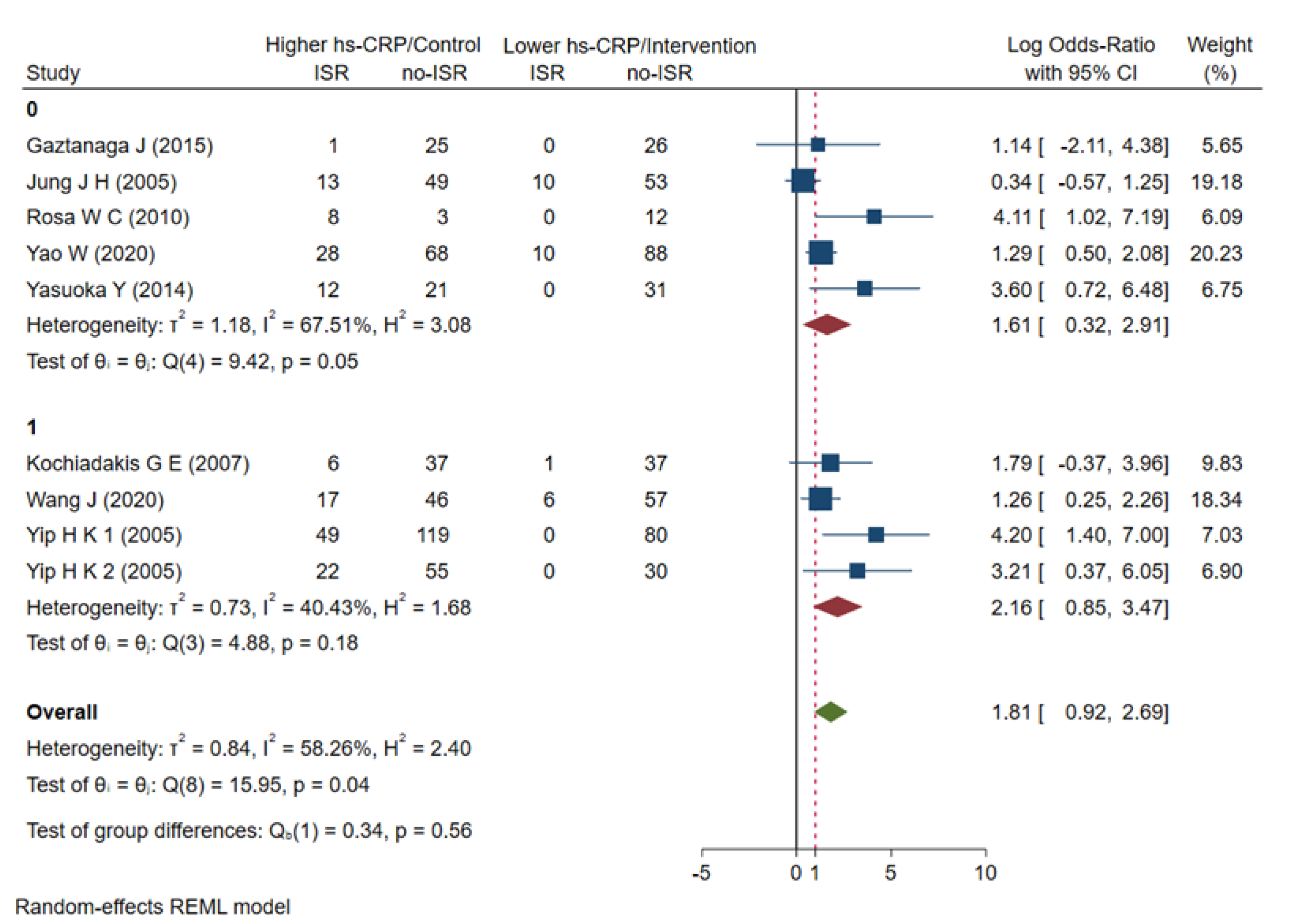
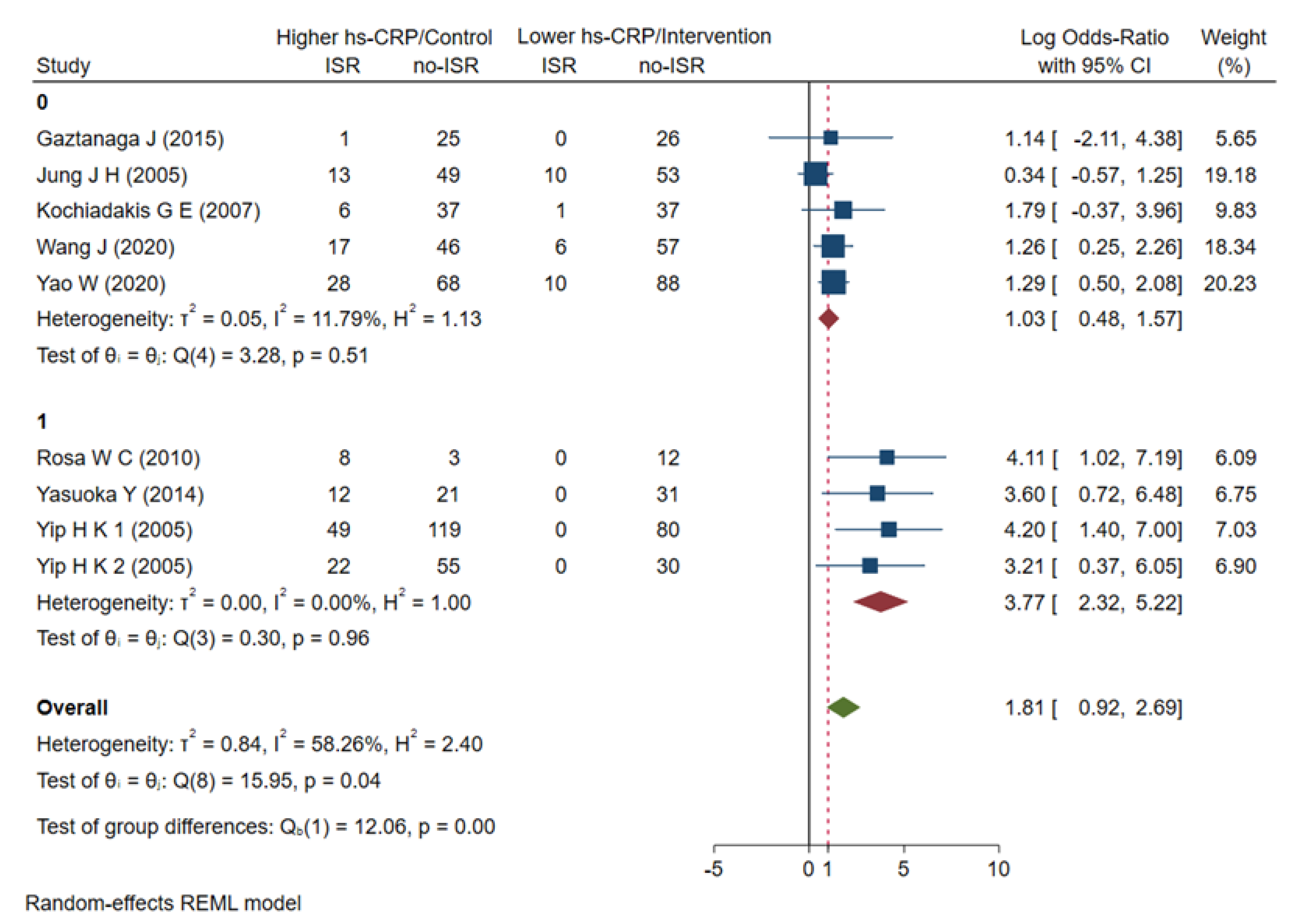
3.5. Subgroup Analyses
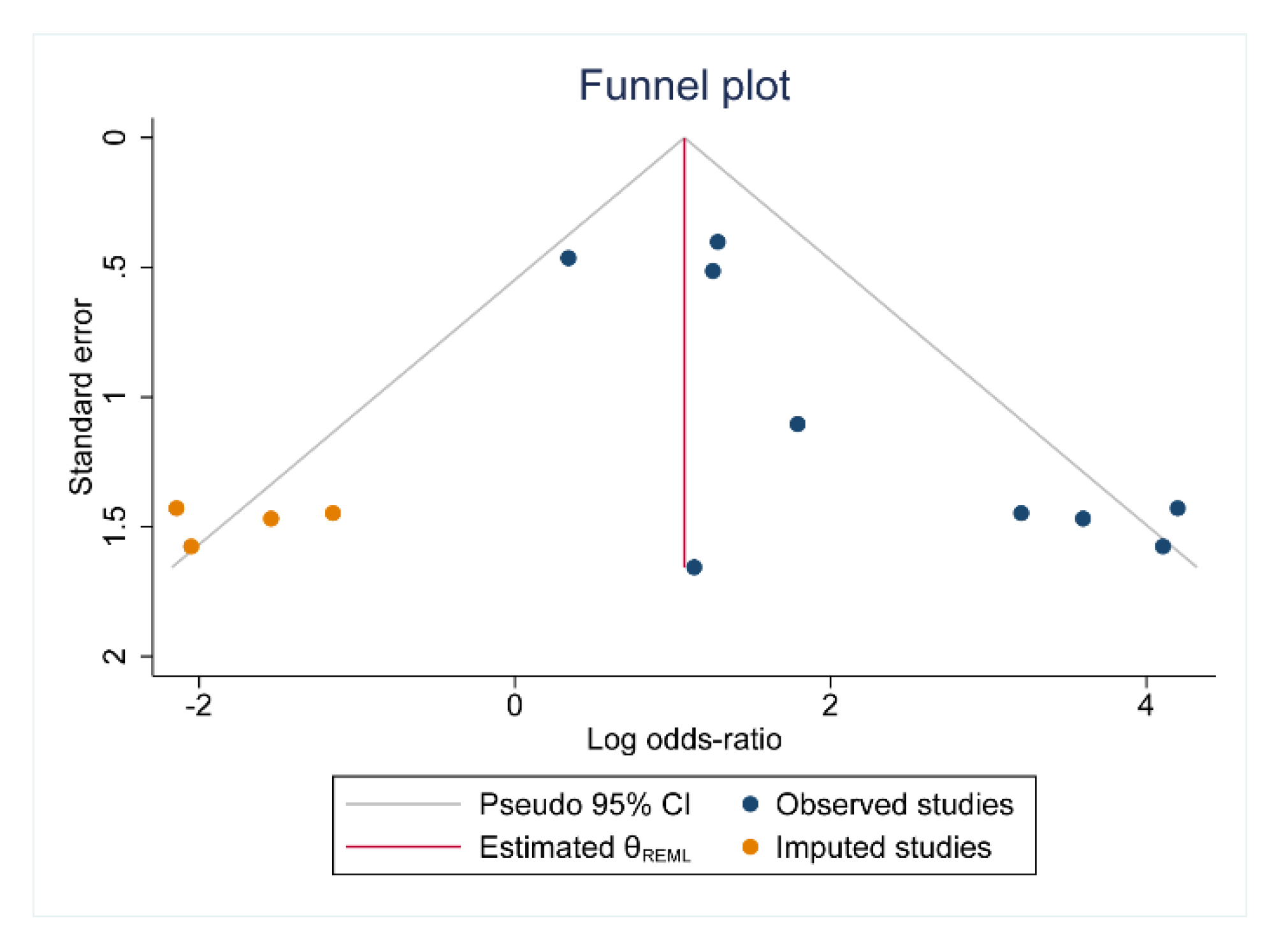
3.6. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yamamoto, K.; Matsumura-Nakano, Y.; Shiomi, H.; Natsuaki, M.; Morimoto, T.; Kadota, K.; Tada, T.; Takeji, Y.; Yoshikawa, Y.; Imada, K.; et al. Effect of Heart Failure on Long-Term Clinical Outcomes After Percutaneous Coronary Intervention Versus Coronary Artery Bypass Grafting in Patients With Severe Coronary Artery Disease. J. Am. Heart Assoc. 2021, 10, e021257. [Google Scholar] [PubMed]
- Wańha, W.; Bil, J.; Januszek, R.; Gilis-Malinowska, N.; Figatowski, T.; Milewski, M.; Pawlik, A.; Staszczak, B.; Wybraniec, M.; Tomasiewicz, B.; et al. Long-Term Outcomes Following Drug-Eluting Balloons Versus Thin-Strut Drug-Eluting Stents for Treatment of In-Stent Restenosis (DEB-Dragon-Registry). Circ. Cardiovasc. Interv. 2021, 14, e010868. [Google Scholar] [PubMed]
- Yabushita, H.; Kawamoto, H.; Fujino, Y.; Tahara, S.; Horikoshi, T.; Tada, M.; Amano, T.; Onishi, H.; Nakajima, A.; Warisawa, T.; et al. Clinical Outcomes of Drug-Eluting Balloon for In-Stent Restenosis Based on the Number of Metallic Layers. Circ. Cardiovasc. Interv. 2018, 11, e005935. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, D.; Dohi, T.; Ishihara, T.; Kikuchi, A.; Mori, N.; Yokoi, K.; Shiraki, T.; Mizote, I.; Mano, T.; Higuchi, Y.; et al. Predictors and outcomes of neoatherosclerosis in patients with in-stent restenosis. EuroIntervention 2021, 17, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Magalhaes, M.A.; Minha, S.; Chen, F.; Torguson, R.; Omar, A.F.; Loh, J.P.; Escarcega, R.O.; Lipinski, M.J.; Baker, N.C.; Kitabata, H.; et al. Clinical Presentation and Outcomes of Coronary In-Stent Restenosis Across 3-Stent Generations. Circ. Cardiovasc. Interv. 2014, 7, 768–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ullrich, H.; Olschewski, M.; Münzel, T.; Gori, T. Coronary In-Stent Restenosis: Predictors and Treatment. Dtsch. Arztebl. Int. 2021, 118, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Yi, M.; Tang, W.-H.; Xu, S.; Ke, X.; Liu, Q. Investigation Into the Risk Factors Related to In-stent Restenosis in Elderly Patients With Coronary Heart Disease and Type 2 Diabetes Within 2 Years After the First Drug-Eluting Stent Implantation. Front. Cardiovasc. Med. 2022, 9, 83730. [Google Scholar]
- Shlofmitz, E.; Iantorno, M.; Waksman, R. Restenosis of Drug-Eluting Stents: A New Classification System Based on Disease Mechanism to Guide Treatment and State-of-the-Art Review. Circ. Cardiovasc. Interv. 2019, 12, e007023. [Google Scholar]
- Zeng, M.; Yan, X.; Wu, W. Risk factors for revascularization and in-stent restenosis in patients with triple-vessel disease after second-generation drug-eluting stent implantation: A retrospective analysis. BMC Cardiovasc. Disord. 2021, 21, 446. [Google Scholar] [CrossRef]
- Wang, P.; Qiao, H.; Wang, R.; Hou, R.; Guo, J. The characteristics and risk factors of in-stent restenosis in patients with percutaneous coronary intervention: What can we do. BMC Cardiovasc. Disord. 2020, 20, 510. [Google Scholar] [CrossRef]
- Inamdar, V.; Zviman, M.; Bratinov, G.; Fitzpatrick, E.O.; Gardiner, K.; Alferiev, I.S.; Levy, R.J.; Stachelek, S.J.; Fishbein, I. Abstract P137: Hypercholesterolemia Aggravates In-stent Restenosis In Rabbits By Escalating Vascular Inflammation. Arterioscler. Thromb. Vasc. Biol. 2021, 41 (Suppl. S1), AP137. [Google Scholar] [CrossRef]
- Kelly, P.J.; Lemmens, R.; Tsivgoulis, G. Inflammation and Stroke Risk: A New Target for Prevention. Stroke 2021, 52, 2697–2706. [Google Scholar] [CrossRef]
- Castro, A.R.; Silva, S.O.; Soares, S.C. The Use of High Sensitivity C-Reactive Protein in Cardiovascular Disease Detection. J. Pharm. Pharm. Sci. 2018, 21, 496–503. [Google Scholar] [CrossRef] [Green Version]
- Gholoobi, A.; Askari, V.R.; Naghedinia, H.; Ahmadi, M.; Vakili, V.; Rahimi, V.B. Colchicine effectively attenuates inflammatory biomarker high-sensitivity C-reactive protein (hs-CRP) in patients with non-ST-segment elevation myocardial infarction: A randomised, double-blind, placebo-controlled clinical trial. Inflammopharmacology 2021, 29, 1379–1387. [Google Scholar] [CrossRef]
- Ribeiro, D.R.P.; Ramos, A.M.; Vieira, P.L.; Menti, E.; Bordin, O.L., Jr.; De Souza, P.A.L.; De Quadros, A.S.; Portal, V.L.; Bordin, O.L. High-sensitivity C-reactive protein as a predictor of cardiovascular events after ST-elevation myocardial infarction. Arq. Bras. Cardiol. 2014, 103, 69–75. [Google Scholar] [CrossRef]
- Hofer, F.; Perkmann, T.; Gager, G.; Winter, M.-P.; Niessner, A.; Hengstenberg, C.; Siller-Matula, J.M. Comparison of high-sensitivity C-reactive protein vs. C-reactive protein for diagnostic accuracy and prediction of mortality in patients with acute myocardial infarction. Ann. Clin. Biochem. 2021, 58, 342–349. [Google Scholar]
- Vodolazkaia, A.; Bossuyt, X.; Fassbender, A.; Kyama, C.M.; Meuleman, C.; Peeraer, K.; Tomassetti, C.; D’Hooghe, T.M. A high sensitivity assay is more accurate than a classical assay for the measurement of plasma CRP levels in endometriosis. Reprod. Biol. Endocrinol. 2011, 9, 113. [Google Scholar] [CrossRef] [Green Version]
- Bassuk, S.S.; Rifai, N.; Ridker, P.M. High-sensitivity C-reactive protein: Clinical importance. Curr. Probl. Cardiol. 2004, 29, 439–493. [Google Scholar]
- Zhu, X.; Chen, Y.; Xiang, L.; You, T.; Jiao, Y.; Xu, W.; Chen, J. The long-term prognostic significance of high-sensitive C-reactive protein to in-stent restenosis. Medicine 2018, 97, e10679. [Google Scholar] [CrossRef]
- Wang, M.; Zhang, W.; Zhang, L.; Wang, L.; Li, J.; Shu, C.; Li, X. Roles of MicroRNAs in Peripheral Artery In-Stent Restenosis after Endovascular Treatment. Biomed. Res. Int. 2021, 2021, 9935671. [Google Scholar] [CrossRef]
- Gaztanaga, J.; Farkouh, M.; Rudd, J.H.; Brotz, T.M.; Rosenbaum, D.; Mani, V.; Kerwin, T.C.; Taub, R.; Tardif, J.-C.; Tawakol, A.; et al. A phase 2 randomized, double-blind, placebo-controlled study of the effect of VIA-2291, a 5-lipoxygenase inhibitor, on vascular inflammation in patients after an acute coronary syndrome. Atherosclerosis 2015, 240, 53–60. [Google Scholar] [CrossRef]
- Rosa, W.C.; Campos, A.H.; Lima, V.C. Effect of oral sirolimus therapy on inflammatory biomarkers following coronary stenting. Braz. J. Med. Biol. Res. 2010, 43, 786–793. [Google Scholar] [CrossRef] [Green Version]
- Yao, W.; Wang, L.; Chen, Q.; Wang, F.; Feng, N. Effects of Valsartan on Restenosis in Patients with Arteriosclerosis Obliterans of the Lower Extremities Undergoing Interventional Therapy: A Prospective, Randomized, Single-Blind Trial. Med. Sci. Monit. 2020, 26, e919977. [Google Scholar] [CrossRef] [Green Version]
- Jung, J.H.; Min, P.K.; Kim, J.Y.; Park, S.; Choi, E.Y.; Ko, Y.G.; Choi, D.; Jang, Y.; Shim, W.H.; Cho, S.Y. Does a carbon ion-implanted surface reduce the restenosis rate of coronary stents? Cardiology 2005, 104, 72–75. [Google Scholar] [CrossRef] [PubMed]
- Kochiadakis, G.E.; Marketou, M.E.; Arfanakis, D.A.; Sfiridaki, K.; Skalidis, E.I.; Igoumenidis, N.E.; Hamilos, M.I.; Kolyvaki, S.; Chlouverakis, G.; Kantidaki, E.; et al. Reduced systemic inflammatory response to implantation of sirolimus-eluting stents in patients with stable coronary artery disease. Atherosclerosis 2007, 194, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zeng, Y.; Zhu, H. Rapamycin-eluting single and double stenting on serum markers in coronary bifurcation lesions. J. Coll. Physicians Surg. Pak. 2020, 30, 222–224. [Google Scholar] [CrossRef] [PubMed]
- Yasuoka, Y.; Kitatoube, A.; Kume, K.; Nakashima, T.; Kosugi, M.; Kohama, Y.; Araki, R.; Matsutera, R.; Noda, Y.; Hattori, S.; et al. Local release of inflammatory markers in coronary artery associated with the development of in-stent restenosis in patients with acute coronary syndrome. Exp. Clin. Cardiol. 2014, 20, 2549–2578. [Google Scholar]
- Yip, H.-K.; Wu, C.-J.; Yang, C.-H.; Chang, H.-W.; Fang, C.-Y.; Hung, W.-C. Serial Changes in Circulating Concentrations of Soluble CD40 Ligand and C-Reactive Protein in Patients With Unstable Angina Undergoing Coronary Stenting Role of Inflammatory Mediators in Predicting Late Restenosis. Circ. J. 2005, 69, 890–895. [Google Scholar] [CrossRef] [Green Version]
- Yip, H.-K.; Hung, W.-C.; Yang, C.-H.; Chen, Y.-H.; Cheng, C.-I.; Chen, S.-M.; Yeh, K.-H. Serum concentrations of high-sensitivity C-reactive protein predict progressively obstructive lesions rather than late restenosis in patients with unstable angina undergoing coronary artery stenting. Circ. J. 2005, 69, 1202–1207. [Google Scholar] [CrossRef] [Green Version]
- Demirtas, K. Inflammation and In-Stent Restenosis. Angiology 2018, 69, 89. [Google Scholar] [CrossRef] [Green Version]
- Akboga, M.K.; Yilmaz, S. Predictors of In-Stent Restenosis. Angiology 2019, 70, 279. [Google Scholar] [CrossRef]
- Zhang, W.; Speiser, J.L.; Ye, F.; Tsai, M.Y.; Cainzos-Achirica, M.; Nasir, K.; Herrington, D.M.; Shapiro, M.D. High-Sensitivity C-Reactive Protein Modifies the Cardiovascular Risk of Lipoprotein(a): Multi-Ethnic Study of Atherosclerosis. J. Am. Coll. Cardiol. 2021, 78, 1083–1094. [Google Scholar] [CrossRef]
- Ridker, P.M. From C-Reactive Protein to Interleukin-6 to Interleukin-1: Moving Upstream To Identify Novel Targets for Atheroprotection. Circ. Res. 2016, 118, 145–156. [Google Scholar] [CrossRef] [Green Version]
- Gaspardone, A.; Versaci, F. Coronary stenting and inflammation. Am. J. Cardiol. 2005, 96, 65l–701. [Google Scholar] [CrossRef]
- Kandelouei, T.; Abbasifard, M.; Imani, D.; Aslani, S.; Razi, B.; Fasihi, M.; Shafiekhani, S.; Mohammadi, K.; Jamialahmadi, T.; Reiner, Ž.; et al. Effect of Statins on Serum level of hs-CRP and CRP in Patients with Cardiovascular Diseases: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Mediat. Inflamm 2022, 2022, 8732360. [Google Scholar] [CrossRef]
- Prasad, K. Do statins have a role in reduction/prevention of post-PCI restenosis? Cardiovasc. Ther. 2013, 31, 12–26. [Google Scholar] [CrossRef]
- Herdeg, C.; Fitzke, M.; Oberhoff, M.; Baumbach, A.; Schroeder, S.; Karsch, K.R. Effects of atorvastatin on in-stent stenosis in normo- and hypercholesterolemic rabbits. Int. J. Cardiol. 2003, 91, 59–69. [Google Scholar] [CrossRef]
- Zago, A.C.; Matte, B.S.; Reginato, L.; Iturry-Yamamoto, G.; Krepsky, A.; Bergoli, L.C.; Balvedi, J.; Raudales, J.C.; Saadi, E.K.; Zago, A.J. First-in-man study of simvastatin-eluting stent in de novo coronary lesions: The SIMVASTENT study. Circ. J. 2012, 76, 1109–1114. [Google Scholar] [CrossRef] [Green Version]
- Li, J.-J.; Ren, Y.; Chen, K.-J.; Yeung, A.C.; Xu, B.; Ruan, X.-M.; Yang, Y.-J.; Chen, J.-L.; Gao, R.-L. Impact of C-reactive protein on in-stent restenosis: A meta-analysis. Tex. Heart Inst. J. 2010, 37, 49–57. [Google Scholar]
- Kocas, C.; Abaci, O.; Kocas, B.B.; Cetinkal, G.; Arslan, S.; Yildiz, A.; Ersanli, M. Impact of statin non-adherence on in-stent restenosis following bare-metal stent implantation. Int. J. Cardiol. 2016, 203, 529–531. [Google Scholar] [CrossRef]
- Tornyos, A.; Aradi, D.; Horváth, I.G.; Kónyi, A.; Magyari, B.; Pintér, T.; Vorobcsuk, A.; Tornyos, D.; Komócsi, A. Clinical outcomes in patients treated for coronary in-stent restenosis with drug-eluting balloons: Impact of high platelet reactivity. PLoS ONE 2017, 12, e0188493. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Country/Area | Design | Sample size | Age (Years) | Higher hs-CRP ISR/n | Higher hs-CRP non-ISR/n | Lower hs-CRP ISR/n | Lower hs-CRP non-ISR/n | Follow-Up (Months) | Comparision | Time for Test |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gaztanaga, J. [21] | 2015 | USA | RCT | 52 | 56.6 ± 9.67 | 1 | 25 | 0 | 26 | 6 | Higher hs-CRP vs. Lower hs-CRP 5-lipoxygenase inhibitor vs. placebo | 0 |
| Jung, J.H. [24] | 2005 | Korea | RCT | 125 | 59 ± 10.0 | 13 | 49 | 10 | 53 | 6 | Restenosis vs. non-restenosis Carbon-implanted surface stents vs. Control stents | 0/48 h/6 m |
| Kochiadakis, G.E. [25] | 2007 | Greece | RCT | 81 | 62 ± 11.0 | 6 | 37 | 1 | 37 | 1 | Higher hs-CRP vs. Lower hs-CRP Bare Metal Stents vs. Sirolimus-eluting Stents | 0/24 h/48 h/6 m |
| Rosa, W.C. [22] | 2010 | Brasil | RCT | 48 | 56.8 ± 13 | 8 | 3 | 0 | 12 | 2 | Restenosis vs. non-restenosis Oral sirolimus vs. Placebo | 0/24 h/7 d/49 d/2 m |
| Wang, J. [26] | 2020 | China | RCT | 126 | 66.93 ± 5.25 | 17 | 46 | 6 | 57 | 12 | Restenosis vs. non-restenosis Rapamycin-eluting double stenting vs. single stenting | 0/3 m |
| Yao, W. [23] | 2020 | China | RCT | 194 | 55.1 ± 8.3 | 28 | 68 | 10 | 88 | 6 | Restenosis vs. non-restenosis Valsartan vs. control | 0/6 m |
| Yasuoka, Y. [27] | 2014 | Japan | RCT | 68 | N/A | 12 | 21 | 0 | 31 | 6 | Restenosis vs. non-restenosis Bare Metal Stents vs. Control | 0/6 m |
| Yip, H.K. [28] | 2005 | China | Cohort | 248 | 61.3 ± 9.4 | 49 | 119 | 0 | 80 | 6 | Restenosis vs. non-restenosis Unstable angina vs. Risk control and Normal control | 0/21 d/3 m/6 m |
| Yip, H.K. [29] | 2005 | China | Cohort | 107 | 61.0 ± 10.3 | 22 | 55 | 0 | 30 | 7 | Restenosis vs. non-restenosis Unstable angina vs. Normal control | 0/21 d/3 m/7 m |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yi, M.; Wu, L.; Ke, X. Prognostic Value of High-Sensitivity C-Reactive Protein in In-Stent Restenosis: A Meta-Analysis of Clinical Trials. J. Cardiovasc. Dev. Dis. 2022, 9, 247. https://doi.org/10.3390/jcdd9080247
Yi M, Wu L, Ke X. Prognostic Value of High-Sensitivity C-Reactive Protein in In-Stent Restenosis: A Meta-Analysis of Clinical Trials. Journal of Cardiovascular Development and Disease. 2022; 9(8):247. https://doi.org/10.3390/jcdd9080247
Chicago/Turabian StyleYi, Ming, Lu Wu, and Xiao Ke. 2022. "Prognostic Value of High-Sensitivity C-Reactive Protein in In-Stent Restenosis: A Meta-Analysis of Clinical Trials" Journal of Cardiovascular Development and Disease 9, no. 8: 247. https://doi.org/10.3390/jcdd9080247