
A Cease in Shift Work Reverses Arterial Stiffness but Increases Weight and Glycosylated Hemoglobin A 5-Month Follow-Up in Industry

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schnall, P.L.; Dobson, M.; Landsbergis, P. Globalization, Work, and Cardiovascular Disease. Int. J. Health Serv. Plan. Adm. Eval. 2016, 46, 656–692. [Google Scholar] [CrossRef] [PubMed]
- Garde, A.H.; Hansen, J.; Kolstad, H.A.; Larsen, A.D.; Pedersen, J.; Petersen, J.D.; Hansen, M. Payroll data based description of working hours in the Danish regions. Chrono. Int. 2018, 35, 795–800. [Google Scholar] [CrossRef] [PubMed]
- Brum, M.C.B.; Filho, F.F.D.; Schnorr, C.C.; Bottega, G.B.; Rodrigues, T.C. Shift work and its association with metabolic disorders. Diabetol. Metab. Syndr. 2015, 7, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kecklund, G.; Axelsson, J. Health consequences of shift work and insufficient sleep. BMJ 2016, 355, i5210. [Google Scholar] [CrossRef] [PubMed]
- Torquati, L.; Mielke, G.; Brown, W.J.; Kolbe-Alexander, T. Shift work and the risk of cardiovascular disease. A systematic review and meta-analysis including dose–response relationship. Scand. J. Work. Environ. Health 2017, 44, 229–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skogstad, M.; Mamen, A.; Lunde, L.-K.; Ulvestad, B.; Matre, D.; Aass, H.C.D.; Øvstebø, R.; Nielsen, P.; Samuelsen, K.N.; Skare, Ø.; et al. Shift Work Including Night Work and Long Working Hours in Industrial Plants Increases the Risk of Atherosclerosis. Int. J. Environ. Res. Public Health 2019, 16, 521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lunde, L.-K.; Skare, Ø.; Mamen, A.; Sirnes, P.A.; Aass, H.C.D.; Øvstebø, R.; Goffeng, E.; Matre, D.; Nielsen, P.; Heglum, H.S.A.; et al. Cardiovascular Health Effects of Shift Work with Long Working Hours and Night Shifts: Study Protocol for a Three-Year Prospective Follow-Up Study on Industrial Workers. Int. J. Environ. Res. Public Health 2020, 17, 589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carney, C.E.; Buysse, D.J.; Ancoli-Israel, S.; Edinger, J.D.; Krystal, A.D.; Lichstein, K.L.; Morin, C.M. The Consensus Sleep Diary: Standardizing Prospective Sleep Self-Monitoring. Sleep 2012, 35, 287–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borazio, M.; Berlin, E.; Kucukyildiz, N.; Scholl, P.; van Laerhoven, K. Towards Benchmarked Sleep Detection with Wrist-Worn Sensing Units. In Proceedings of the 2014 IEEE International Conference on Healthcare Informatics, Verona, Italy, 15–17 September 2014. [Google Scholar]
- Katsifaraki, M.; Nilsen, K.B.; Christensen, J.O.; Wærsted, M.; Knardahl, S.; Bjorvatn, B.; Härmä, M.; Matre, D. Sleep duration mediates abdominal and lower-extremity pain after night work in nurses. Int. Arch. Occup. Environ. Health 2018, 92, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Pallesen, S.; Bjorvatn, B.; Nordhus, I.H.; Sivertsen, B.; Hjørnevik, M.; Morin, C.M. A new scale for measuring insomnia: The Bergen Insomnia Scale. Percept. Mot. Ski. 2008, 107, 691–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Kim, H.L.; Kim, S.H. Pulse Wave Velocity in Atherosclerosis. Front. Cardiovasc. Med. 2019, 6, 41. [Google Scholar] [CrossRef] [PubMed]
- Irwin, M.R.; Olmstead, R.; Carroll, J.E. Sleep Disturbance, Sleep Duration, and Inflammation: A Systematic Review and Meta-Analysis of Cohort Studies and Experimental Sleep Deprivation. Biol. Psychiatry 2016, 80, 40–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duprez, D.A.; Somasundaram, P.E.; Sigurdsson, G.; Hoke, L.; Florea, N.; Cohn, J.N. Relationship between C-reactive protein and arterial stiffness in an asymptomatic population. J. Hum. Hypertens. 2005, 19, 515–519. [Google Scholar] [CrossRef] [PubMed]
- James, S.M.; Honn, K.A.; Gaddameedhi, S.; Van Dongen, H.P. Shift Work: Disrupted Circadian Rhythms and Sleep-Implications for Health and Well-Being. Curr. Sleep Med. Rep. 2017, 3, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Proper, K.I.; van de Langenberg, D.; Rodenburg, W.; Vermeulen, R.C.; van der Beek, A.J.; van Steeg, H.; van Kerkhof, L.W. The Relationship Between Shift Work and Metabolic Risk Factors: A Systematic Review of Longitudinal Studies. Am. J. Prev. Med. 2016, 50, e147–e157. [Google Scholar] [CrossRef] [PubMed]
- Manson, J.E.; Nathan, D.M.; Krolewski, A.S.; Stampfer, M.J.; Willett, W.C.; Hennekens, C.H. A prospective study of exercise and incidence of diabetes among US male physicians. JAMA 1992, 268, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Martínez, A.; Ramírez-Vélez, R.; García-Alonso, Y.; Izquierdo, M.; García-Hermoso, A. Physical Activity, Sedentary Behavior, Sleep and Self-Regulation in Spanish Preschoolers during the COVID-19 Lockdown. Int. J. Environ. Res. Public Health 2021, 18, 693. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Shift Workers | |||||
|---|---|---|---|---|---|---|
| Number | Mean | Median | Min | Max | SD | |
| Age (years) | 41.3 | 40 | 24 | 64 | 12.3 | |
| Women | 1 | |||||
| Weight | 86.7 | 85.5 | 54 | 137 | 19.2 | |
| BMI (kg/m2) | 26.3 | 26.2 | 18.7 | 35.3 | 4.3 | |
| Pack-years | 6.0 | 1.12 | 0 | 37 | 9.8 | |
| Daily smokers | 5 | |||||
| Number of years as shift worker | 15.9 | 14.5 | 2 | 35 | 9.8 | |
| Physical activity (PA), high intensity (min/week) | 101 | 90 | 0 | 600 | 125 | |
| Variable | Pre-Shutdown | Post-Shut Down | Change (Post Minus Pre) during Five Months | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p-Value | p-Value † | Mean | SD | 95% CI | |
| CVD | |||||||||
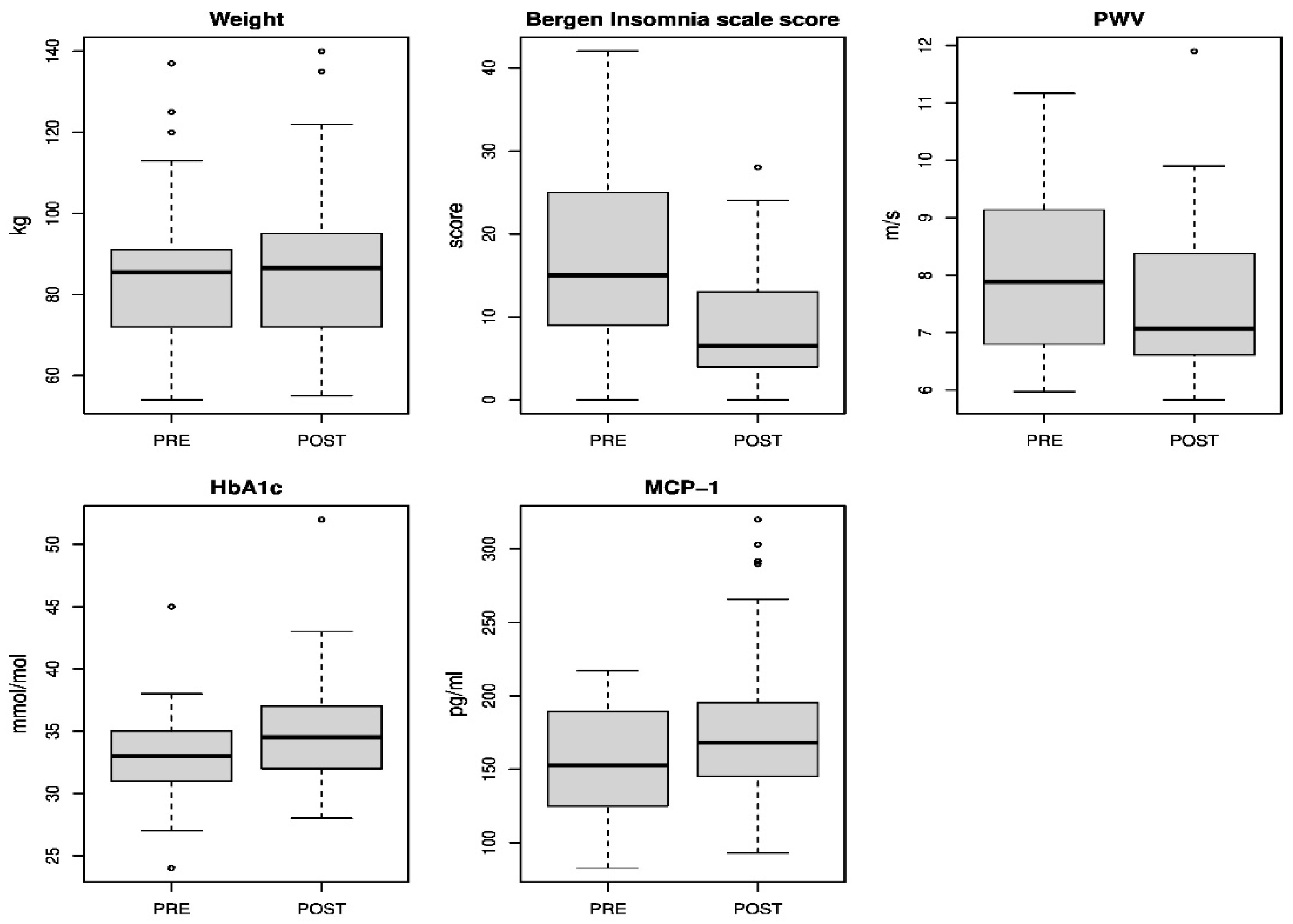
| Weight | 86.7 | 19.2 | 87.7 | 20.1 | 0.034 * | 1.0 | 2.5 | 0.085, 1.98 | |
| BMI | 26.3 | 4.3 | 26.6 | 4.5 | 0.03 * | 0.3 | 0.7 | 0.04, 0.79 | |
| PA, high intensity (min/week) | 100 | 125 | 85 | 116 | 0.55 | N.C. | −15.8 | 143 | −69.2, 37.6 |
| Systolic BP (mmHg) | 123.2 | 14.0 | 127.3 | 15.2 | 0.058 | 0.32 | 4.1 | 11.4 | −0.14, 8.35 |
| Diastolic BP (mmHg) | 81.4 | 10.0 | 83.5 | 8.9 | 0.11 | 0.38 | 2.1 | 6.8 | −0.46, 4.59 |
| Supine systolic BP (mmHg) | 125.5 | 12.1 | 126.2 | 13.1 | 0.74 | 0.94 | 0.7 | 12.0 | −3.76, 5.24 |
| Supine diastolic BP (mmHg) | 74.8 | 9.3 | 74.3 | 8.3 | 0.58 | 0.96 | −0.56 | 5.48 | −2.61, 1.49 |
| Systolic aorta pressure (mmHg) | 112.7 | 12.0 | 112.7 | 11.9 | 0.97 | 0.97 | 0.06 | 9.4 | −3.45, 3.57 |
| Diastolic aorta pressure (mmHg) | 75.3 | 9.6 | 75.2 | 8.4 | 0.94 | 0.97 | −0.09 | 6.0 | −2.32, 2.15 |
| Supine RHR (bpm) | 63.7 | 8.5 | 65.4 | 10.1 | 0.30 | 0.60 | 1.77 | 9.2 | −1.67, 5.21 |
| Augmentation pressure (mmHg) | 8.4 | 6.3 | 8.0 | 5.0 | 0.65 | 0.94 | −0.44 | 5.1 | −2.35, 1.48 |
| Pulse pressure (mmHg) | 37.2 | 6.5 | 37.5 | 7.4 | 0.79 | 0.97 | 0.34 | 7.1 | −2.29, 2.98 |
| Pulse-wave velocity (m/s) a | 8.1 | 1.5 | 7.6 | 1.5 | 0.005 | 0.03 * | −0.45 | 0.8 | −0.75, −0.15 |
| CRP (mg/L) | 2.6 | 2.9 | 1.8 | 2.2 | 0.09 | 0.38 | −0.72 | 2.2 | −1.55, 0.12 |
| Cholesterol (mmol/L) | 4.8 | 1.0 | 4.7 | 0.8 | 0.67 | 0.94 | −0.07 | 0.9 | −0.40, 0.25 |
| HDL (mmol/L) | 1.2 | 0.3 | 1.2 | 0.3 | 0.25 | 0.54 | −0.03 | 0.1 | −0.09, 0.23 |
| LDL (mmol/L) | 3.1 | 0.9 | 3.0 | 0.7 | 0.68 | 0.94 | −0.06 | 0.8 | −0.35, 0.23 |
| HbA1c (mmol/mol) | 32.9 | 4.2 | 34.8 | 4.9 | <0.001 | <0.001 ** | 1.93 | 1.7 | 1.29, 2.58 |
| MMP-9 (pg/mL) b | 64,233 | 34,834 | 73,592 | 37,216 | 0.12 | 0.38 | 9359 | 31,569 | −2649, 21,368 |
| P-selectin (pg/mL) b | 26,260 | 7716 | 26,359 | 6413 | 0.87 | 0.97 | 48.7 | 3110 | −1084, 1282 |
| TNF-α (pg/mL) b | 12.8 | 2.7 | 13.1 | 3.1 | 0.22 | 0.54 | 0.31 | 1.3 | −0.20, 0.82 |
| IL-1β (pg/mL) b | 19.1 | 4.1 | 19.2 | 4.0 | 0.95 | 0.97 | 0.03 | 2.4 | −0.87, 0.93 |
| IL-23 (pg/mL) b | 204 | 109 | 194 | 110 | 0.25 | 0.54 | −9.72 | 44.1 | −26.5, 7.0 |
| IL-6 (pg/mL) b | 5.6 | 1.5 | 5.5 | 1.4 | 0.64 | 0.94 | −0.08 | 0.9 | −0.43, 0.27 |
| MCP-1(pg/mL) b | 157 | 38.4 | 185 | 59.9 | 0.002 | 0.03 * | 27.3 | 44.1 | 10.5, 44.0 |
| Sleep | |||||||||
| Bergen Insomnia Scale Score, (0-42) | 16.5 | 10.3 | 8.9 | 6.8 | <0.001 ** | N.C. | −7.5 | 10.5 | −11.44, −3.63 |
| Subjective NA, n | 1.4 | 1.4 | 1.1 | 1.4 | 0.06 | −0.25 | −0.50, 0.01 | ||
| Objective NA, n | 11.3 | 4.8 | 11.1 | 4.8 | 0.81 | −0.15 | −1.36, 1.06 | ||
| Subjective WASO, min | 22.7 | 34.9 | 18.8 | 44.9 | 0.09 | −0.03 # | −0.06, 0.00 # | ||
| Objective WASO, min | 76.1 | 56.8 | 86.2 | 64.9 | 0.62 | 3.66 | −10.6, 17.9 | ||
| Subjective TST, h | 6.6 | 2.0 | 7.0 | 1.9 | 0.09 | 0.36 | −0.05, 0.78 | ||
| Objective TST, h | 5.4 | 1.7 | 5.4 | 1.6 | 0.78 | 0.06 | −0.36, 0.49 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skogstad, M.; Aass, H.C.D.; Lunde, L.-K.; Skare, Ø.; Sirnes, P.A.; Matre, D. A Cease in Shift Work Reverses Arterial Stiffness but Increases Weight and Glycosylated Hemoglobin A 5-Month Follow-Up in Industry. J. Cardiovasc. Dev. Dis. 2022, 9, 190. https://doi.org/10.3390/jcdd9060190
Skogstad M, Aass HCD, Lunde L-K, Skare Ø, Sirnes PA, Matre D. A Cease in Shift Work Reverses Arterial Stiffness but Increases Weight and Glycosylated Hemoglobin A 5-Month Follow-Up in Industry. Journal of Cardiovascular Development and Disease. 2022; 9(6):190. https://doi.org/10.3390/jcdd9060190
Chicago/Turabian StyleSkogstad, Marit, Hans Christian D. Aass, Lars-Kristian Lunde, Øivind Skare, Per Anton Sirnes, and Dagfinn Matre. 2022. "A Cease in Shift Work Reverses Arterial Stiffness but Increases Weight and Glycosylated Hemoglobin A 5-Month Follow-Up in Industry" Journal of Cardiovascular Development and Disease 9, no. 6: 190. https://doi.org/10.3390/jcdd9060190