
Effectiveness of the Combination of Enalapril and Nifedipine for the Treatment of Hypertension versus Empirical Treatment in Primary Care Patients

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Sample Size and Sampling Method
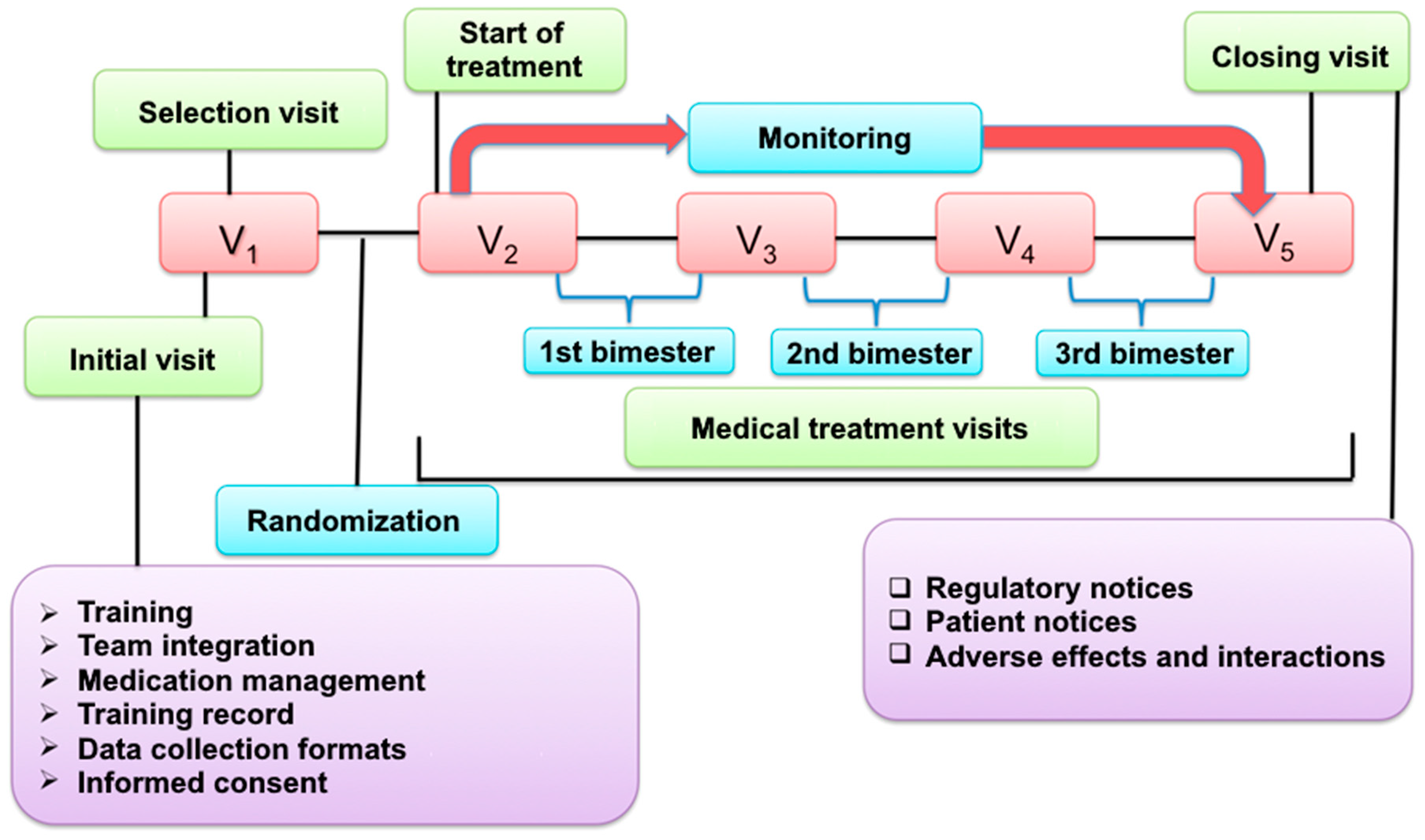
2.3. Study Protocol
2.3.1. Assessment of Blood Pressure, Vital Signs, Anthropometric Variables, and Biochemical Variables
2.3.2. Assessment of Therapeutic Adherence and Adverse Reactions
2.3.3. Study Variables
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
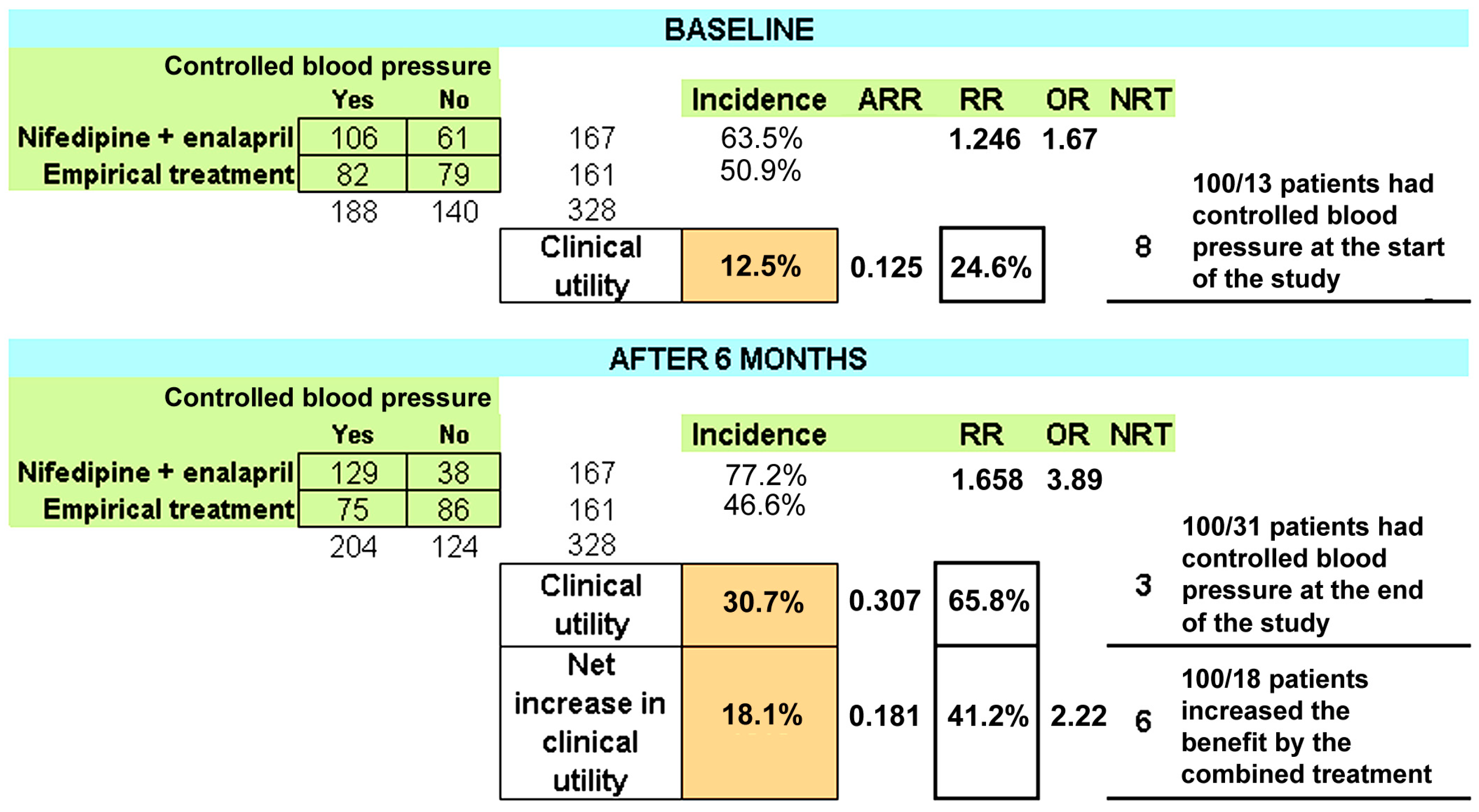
3.2. Outcome Variables and Treatment Efficacy
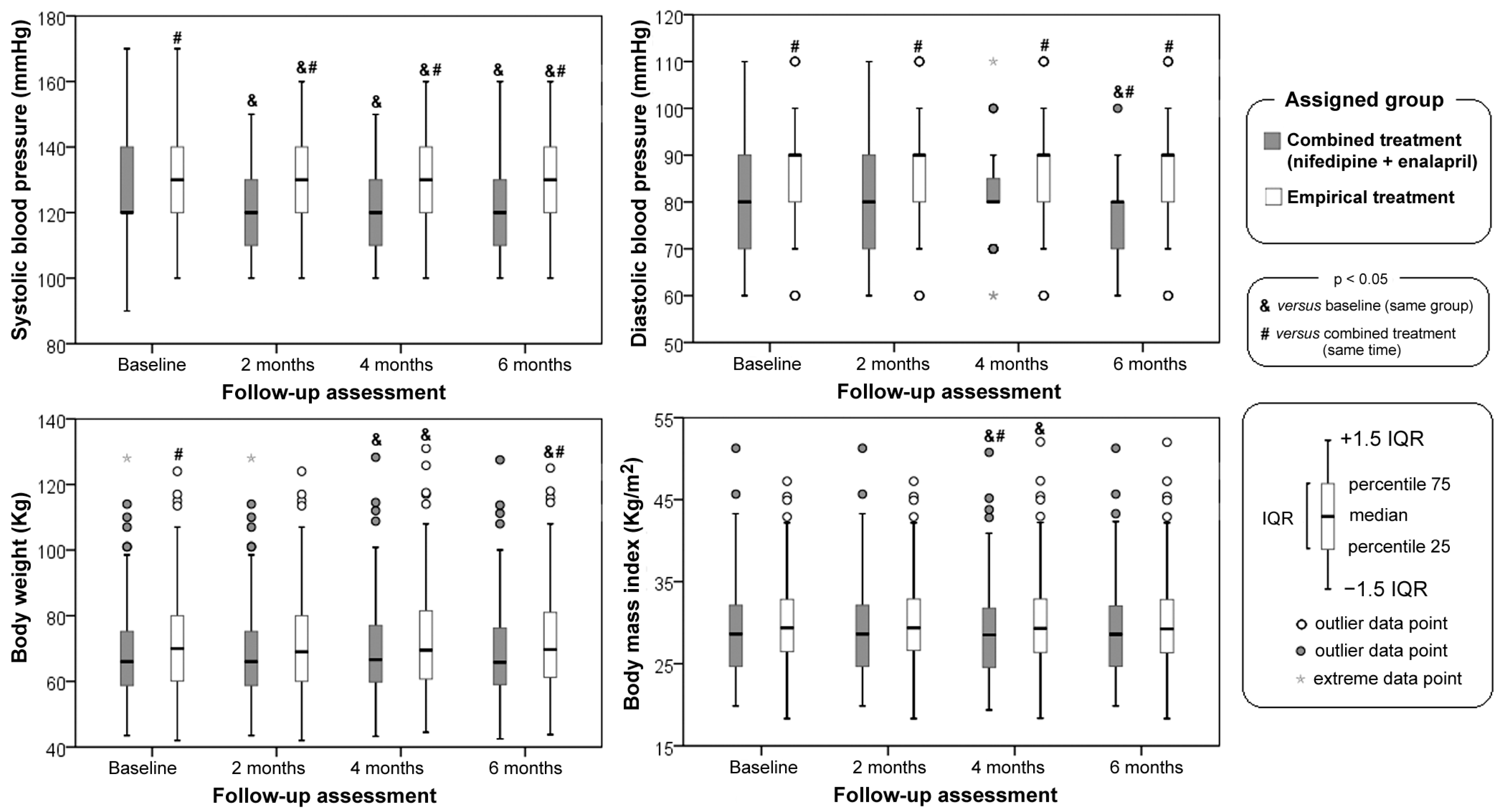
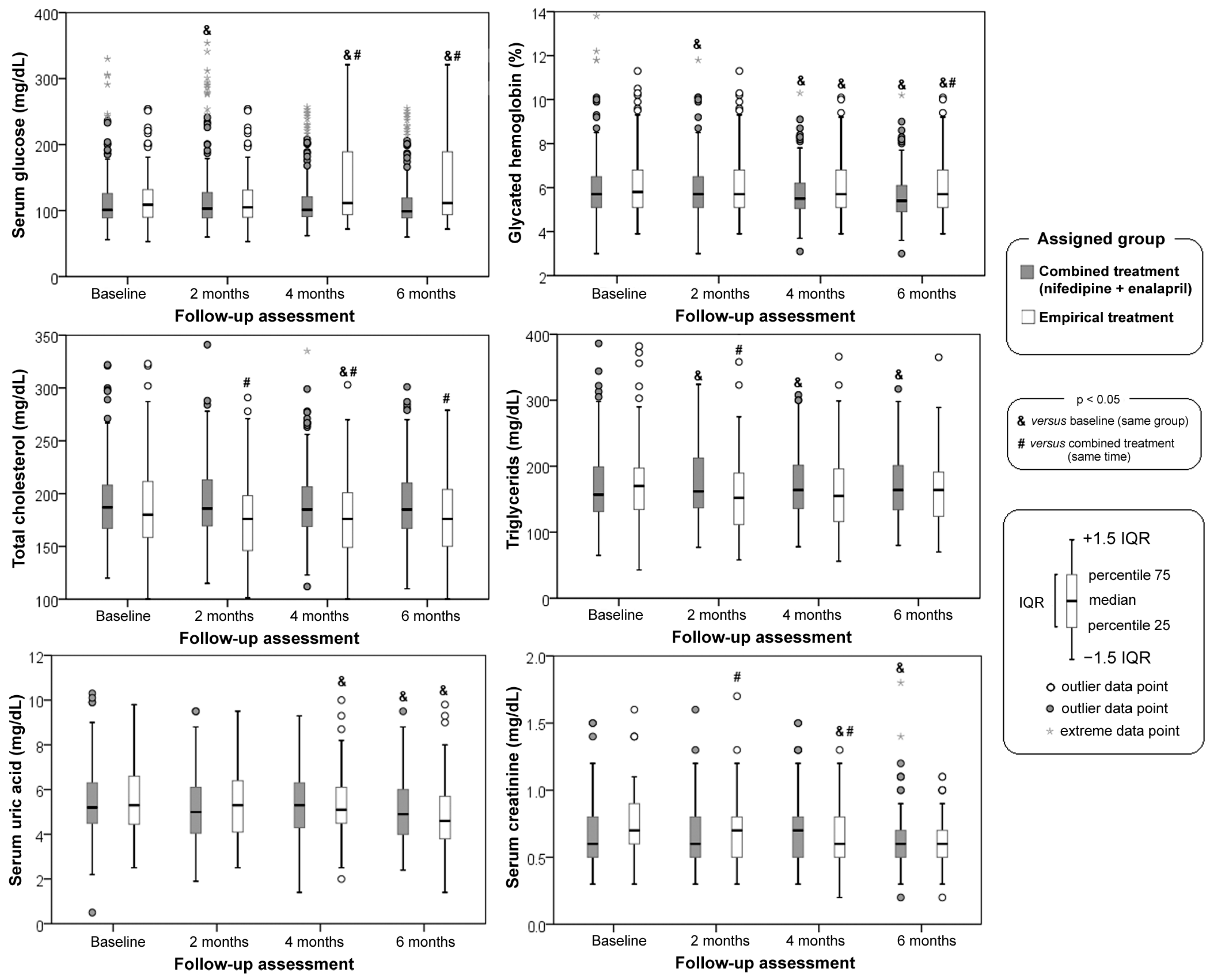
3.3. Anthropometric, Blood Pressure and Laboratory Variables Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Oparil, S.; Acelajado, M.C.; Bakris, G.L.; Berlowitz, D.R.; Cífková, R.; Dominiczak, A.F.; Grassi, G.; Jordan, J.; Poulter, N.R.; Rodgers, A.; et al. Hypertension. Nat. Rev. Dis. Prim. 2018, 4, 18014. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, M.G.; Frieden, T.R.; Campbell, N.R.C.; Matsushita, K.; Appel, L.J.; Lackland, D.T.; Zhang, X.H.; Muruganathan, A.; Whelton, P.K. Recommended treatment protocols to improve management of hypertension globally: A statement by Resolve to Save Lives and the World Hypertension League (WHL). J. Clin. Hypertens. 2018, 20, 829–836. [Google Scholar] [CrossRef]
- Ordunez, P.; Martinez, R.; Niebylski, M.L.; Campbell, N.R. Hypertension Prevention and Control in Latin America and the Caribbean. J. Clin. Hypertens. 2015, 17, 499–502. [Google Scholar] [CrossRef]
- Sica, D.A. Rationale for fixed-dose combinations in the treatment of hypertension: The cycle repeats. Drugs 2002, 62, 443–462. [Google Scholar] [CrossRef] [PubMed]
- Bress, A.P.; Greene, T.; Derington, C.G.; Shen, J.; Xu, Y.; Zhang, Y.; Ying, J.; Bellows, B.K.; Cushman, W.C.; Whelton, P.K.; et al. Patient Selection for Intensive Blood Pressure Management Based on Benefit and Adverse Events. J. Am. Coll. Cardiol. 2021, 77, 1977–1990. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Him-melfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. Authors/Task Force Members: 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J. Hypertens. 2018, 36, 1953–2041. [Google Scholar] [CrossRef]
- Task Force of the Latin American Society of Hypertension. Guidelines on the management of arterial hypertension and related comorbidities in Latin America. J. Hypertens. 2017, 35, 1529–1545. [Google Scholar] [CrossRef]
- de la Sierra, A. Mitigation of calcium channel blocker-related oedema in hypertension by antagonists of the renin-angiotensin system. J. Hum. Hypertens. 2009, 23, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Lam, S.K.; Owen, A. Incident diabetes in clinical trials of antihypertensive drugs. Lancet 2007, 369, 1513–1514. [Google Scholar] [CrossRef] [PubMed]
- Karlberg, B.E.; Andrup, M.; Odén, A. Efficacy and safety of a new long-acting drug combination, trandolapril/verapamil as compared to monotherapy in primary hyper-tension. Swedish TARKA trialists. Blood Press. 2000, 9, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Mancia, G.; Asmar, R.; Amodeo, C.; Mourad, J.J.; Taddei, S.; Gamba, M.A.; Chazova, I.E.; Puig, J.G. Comparison of single-pill strategies first line in hypertension: Perin-dopril/amlodipine versus valsartan/amlodipine. J. Hypertens. 2015, 33, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Lubianca, J.N.; Moreira, L.B.; Gus, M.; Fuchs, F.D. Stopping oral contraceptives: An effective blood pressure-lowering intervention in women with hypertension. J. Hum. Hypertens. 2005, 19, 451–455. [Google Scholar] [CrossRef]
- Val Jimenez, A.; Amoros Ballestero, G.; Martinez Visa, P.; Fernández Ferre, M.L.; León Sanroma, M. Estudio descriptivo del cumplimiento del tratamiento farmacológico antihipertensivo y validación del test de Morisky y Green [Descriptive study of patient compliance in pharmacologic antihypertensive treatment and validation of the Morisky and Green test]. Aten Primaria. 1992, 10, 767–770. [Google Scholar]
- Ruilope, L.M.; Nunes Filho, A.C.B.; Nadruz, W., Jr.; Rodríguez Rosales, F.F.; Verdejo-Paris, J. Obesity and hypertension in Latin America: Current perspectives. Hipertens. Riesgo Vasc. 2018, 3, 70–76. [Google Scholar] [CrossRef]
- Cohen, H.W.; Hailpern, S.M.; Fang, J.; Alderman, M.H. Sodium intake and mortality in the NHANES II follow-up study. Am. J. Med. 2006, 119, 275.e7–275.e14. [Google Scholar] [CrossRef]
- Intersalt Cooperative Research Group. Intersalt: An international study of electrolyte excretion and blood pressure. Results for 24 hour urinary sodium and potassium excretion. BMJ 1988, 297, 319–328. [Google Scholar] [CrossRef]
- Mancia, G.; Rea, F.; Corrao, G.; Grassi, G. Two-Drug Combinations as First-Step Antihypertensive Treatment. Circ. Res. 2019, 124, 1113–1123. [Google Scholar] [CrossRef] [PubMed]
- Julius, S.; Kjeldsen, S.E.; Weber, M.; Brunner, H.R.; Ekman, S.; Hansson, L.; Hua, T.; Laragh, J.; McInnes, G.T.; Mitchell, L.; et al. Outcomes in hypertensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: The VALUE randomised trial. Lancet 2004, 363, 2022–2031. [Google Scholar] [CrossRef]
- Liebson, P.R. ASCOT-Blood Pressure Trial (ASCOT-BPLA) and HOPE-TOO. Prev. Cardiol. 2006, 9, 60–63. [Google Scholar] [CrossRef] [PubMed]
- Adrogué, H.J.; Madias, N.E. Sodium and potassium in the pathogenesis of hypertension. N. Engl. J. Med. 2007, 356, 1966–1978. [Google Scholar] [CrossRef] [PubMed]
- Hyman, D.J.; Pavlik, V. Medication adherence and resistant hypertension. J. Hum. Hypertens. 2015, 29, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Kim, S.Y.; Choi, K.J.; Yoo, B.S.; Cha, D.H.; Jung, H.O.; Ryu, D.R.; Choi, J.H.; Lee, K.J.; Park, T.H.; et al. A Randomized, Multicenter, Double-blind, Placebo-controlled Study to Evaluate the Efficacy and the Tolerability of a Triple Combination of Amlodipine/Losartan/Rosuvastatin in Patients with Comorbid Essential Hypertension and Hyperlipidemia. Clin. Ther. 2017, 39, 2366–2379. [Google Scholar] [CrossRef]
- Rosas-Peralta, M.; Jiménez-Genchi, G.M. New Challenges for Hypertension Treatment. Arch. Med. Res. 2018, 49, 548–557. [Google Scholar] [CrossRef]
- Jarraya, F. Treatment of Hypertension: Which Goal for Which Patient? Adv. Exp. Med. Biol. 2017, 956, 117–127. [Google Scholar] [CrossRef]
- De Backer, T.; Van Nieuwenhuyse, B.; De Bacquer, D. Antihypertensive treatment in a general uncontrolled hypertensive population in Belgium and Luxembourg in primary care: Therapeutic inertia and treatment simplification. The SIMPLIFY study. PLoS ONE 2021, 16, e0248471. [Google Scholar] [CrossRef]
- Carey, R.M.; Muntner, P.; Bosworth, H.B.; Whelton, P.K. Prevention and Control of Hypertension: JACC Health Promotion Series. J. Am. Coll. Cardiol. 2018, 72, 1278–1293. [Google Scholar] [CrossRef]
- Choi, H.Y.; Oh, I.J.; Lee, J.A.; Lim, J.; Kim, Y.S.; Jeon, T.H.; Cheong, Y.S.; Kim, D.H.; Kim, M.C.; Lee, S.Y. Factors Affecting Adherence to Antihypertensive Medication. Korean J. Fam. Med. 2018, 39, 325–332. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 Practice Guidelines for the management of arterial hypertension of the European Society of Hypertension and the European Society of Cardiology: ESH/ESC Task Force for the Management of Arterial Hypertension. J. Hypertens. 2018, 36, 2284–2309. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Empirical Treatment (N = 161) | Combined Treatment (Enalapril + Nifedipine) (N = 167) | p Value |
|---|---|---|---|
| Age (years) | 61 (53–70) | 62 (55–71) | 0.501 |
| BMI (kg/m2) | 29.2 (26.3–32.8) | 28.6 (24.7–32.0) | 0.092 |
| Female sex | 120 (75%) | 123 (74%) | 0.855 |
| Overweight or obese | 139 (86%) | 122 (73%) | 0.003 |
| Diabetes mellitus | 91 (56%) | 94 (65%) | 0.966 |
| Dyslipidemia | 58 (36%) | 69 (41%) | 0.325 |
| Metabolic syndrome | 72 (45%) | 75 (45%) | 0.972 |
| Uncontrolled diabetes | 43 (47%) | 34 (36%) | 0.126 |
| Uncontrolled dyslipidemia | 58 (36%) | 69 (41%) | 0.325 |
| Uncontrolled metabolic syndrome | 74 (45%) | 75 (45%) | 0.972 |
| Variable | Empirical Treatment | Enalapril + Nifedipine | p Value |
|---|---|---|---|
| Acetylsalicylic acid | 19 (12%) | 16 (10%) | 0.515 |
| Metformin | 74 (45%) | 91 (54%) | 0.098 |
| Glibenclamide | 20 (12%) | 42 (25%) | 0.003 |
| Linagliptin | 1 (1%) | 1 (1%) | 0.742 |
| Acarbose | 3 (2%) | 3 (2%) | 0.640 |
| Fast insulin | 2 (1%) | 4 (2%) | 0.360 |
| Glargine insulin | 39 (24%) | 29 (17%) | 0.126 |
| NPH insulin | 1 (1%) | 2 (1%) | 0.514 |
| Captopril | 49 (30%) | 0 (0%) | <0.001 |
| Hydrochlorothiazide | 6 (4%) | 0 (0%) | 0.013 |
| Chlorthalidone | 4 (3%) | 0 (0%) | 0.057 |
| Metoprolol | 26 (16%) | 0 (0%) | <0.001 |
| Propranolol | 2 (1%) | 1 (1%) | 0.486 |
| Telmisartan | 12 (7%) | 0 (0%) | <0.001 |
| Losartan | 44 (27%) | 0 (0%) | <0.001 |
| Alopurinol | 0 (0%) | 2 (1%) | 0.258 |
| Pravastatin | 33 (21%) | 34 (20%) | 0.542 |
| Atorvastatin | 5 (3%) | 6 (4%) | 0.525 |
| Bezafibrate | 17 (11%) | 25 (15%) | 0.232 |
| Verapamil | 1 (1%) | 0 (0%) | 0.491 |
| Furosemide | 1 (1%) | 0 (0%) | 0.491 |
| Baseline | Empirical Treatment | Enalapril + Nifedipine | p Value |
| Controlled blood pressure | 0.022 | ||
| Yes | 82 (51%) | 106 (64%) | |
| No | 79 (49%) | 61 (36%) | |
| Treatment adherence | 0.038 | ||
| Yes | 103 (64%) | 88 (53%) | |
| No | 58 (36%) | 79 (74%) | |
| Adverse reactions | 0.298 | ||
| Yes | 3 (2%) | 1 (1%) | |
| No | 158 (98%) | 166 (99%) | |
| After 6 months of treatment | Empirical treatment | Enalapril + nifedipine | p value |
| Controlled blood pressure | <0.001 | ||
| Yes | 75 (47%) | 129 (77%) | |
| No | 86 (53%) | 38 (23%) | |
| Treatment adherence | <0.001 | ||
| Yes | 95 (59%) | 155 (93%) | |
| No | 66 (41%) | 12 (7%) | |
| Adverse reactions | 0.298 | ||
| Yes | 3 (2%) | 1 (1%) | |
| No | 158 (98%) | 166 (99%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Badillo-Alonso, H.; Martínez-Alanis, M.; Sánchez-Huesca, R.; Lerma, A.; Lerma, C. Effectiveness of the Combination of Enalapril and Nifedipine for the Treatment of Hypertension versus Empirical Treatment in Primary Care Patients. J. Cardiovasc. Dev. Dis. 2023, 10, 243. https://doi.org/10.3390/jcdd10060243
Badillo-Alonso H, Martínez-Alanis M, Sánchez-Huesca R, Lerma A, Lerma C. Effectiveness of the Combination of Enalapril and Nifedipine for the Treatment of Hypertension versus Empirical Treatment in Primary Care Patients. Journal of Cardiovascular Development and Disease. 2023; 10(6):243. https://doi.org/10.3390/jcdd10060243
Chicago/Turabian StyleBadillo-Alonso, Humberto, Marisol Martínez-Alanis, Ramiro Sánchez-Huesca, Abel Lerma, and Claudia Lerma. 2023. "Effectiveness of the Combination of Enalapril and Nifedipine for the Treatment of Hypertension versus Empirical Treatment in Primary Care Patients" Journal of Cardiovascular Development and Disease 10, no. 6: 243. https://doi.org/10.3390/jcdd10060243