
Platelet-to-Albumin Ratio: The Prognostic Utility in the Prediction of 2-Month Postoperative Heart Transplant Complications
 , , , ,
, , , ,
Abstract
:1. Introduction
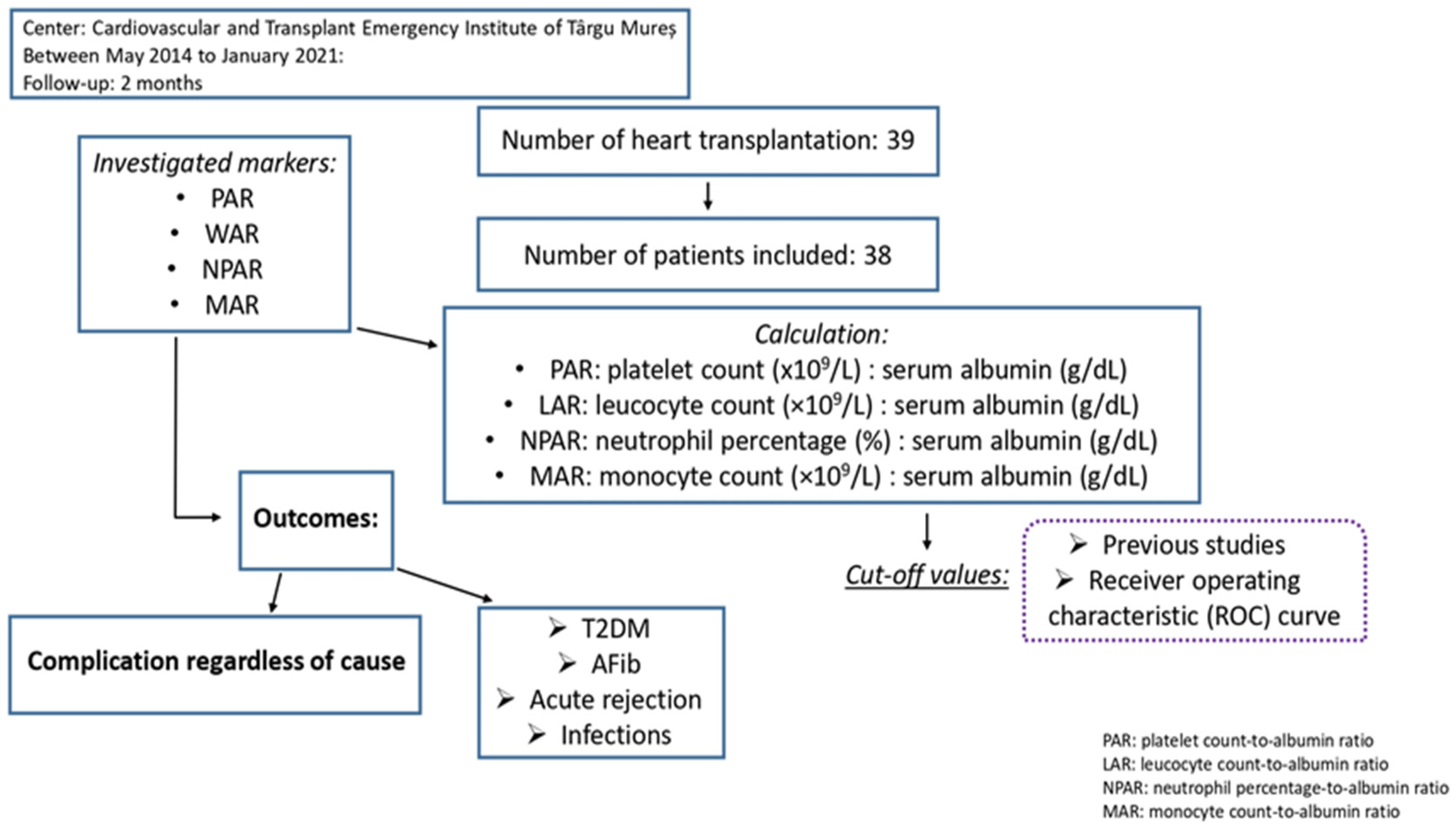
2. Materials and Methods
2.1. Study Design and Patients
2.2. Management and Follow-Up
2.3. Statistical Analysis
2.4. Previous Researches That Examined LAR, NPAR MAR, and PAR Prognostic Roles
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brink, J.G.; Hassoulas, J. The first human heart transplant and further advances in cardiac transplantation at Groote Schuur Hospital and the University of Cape Town—With reference to: The operation. A human cardiac transplant: An interim report of a successful operation performed at Groote Schuur Hospital, Cape Town. Cardiovasc. J. Afr. 2009, 20, 31–35. [Google Scholar] [PubMed]
- Alba, A.C.; Bain, E.; Ng, N.; Stein, M.; O’Brien, K.; Foroutan, F.; Ross, H. Complications after Heart Transplantation: Hope for the Best, but Prepare for the Worst. Int. J. Organ Transplant. Med. 2016, 2, 022. [Google Scholar] [CrossRef]
- Costanzo, M.R.; Dipchand, A.; Starling, R.; Anderson, A.; Chan, M.; Desai, S.; Fedson, S.; Fisher, P.; Gonzales-Stawinski, G.; Martinelli, L.; et al. The international society of heart and lung transplantation guidelines for the care of heart transplant recipients. J. Heart Lung Transplant. 2010, 29, 914–956. [Google Scholar] [CrossRef] [PubMed]
- Rauchhaus, M.; Doehner, W.; Francis, D.P.; Davos, C.; Kemp, M.; Liebenthal, C.; Niebauer, J.; Hooper, J.; Volk, H.D.; Coats, A.J.; et al. Plasma cytokine parameters and mortality in patients with chronic heart failure. Circulation 2000, 102, 3060–3067. [Google Scholar] [CrossRef] [PubMed]
- Shirazi, L.F.; Bissett, J.; Romeo, F.; Mehta, J.L. Role of Inflammation in Heart Failure. Curr. Atheroscler. Rep. 2017, 19, 27. [Google Scholar] [CrossRef] [PubMed]
- Schalk, B.W.; Visser, M.; Bremmer, M.A.; Penninx, B.W.; Bouter, L.M.; Deeg, D.J. Change of serum albumin and risk of cardiovascular disease and all-cause mortality: Longitudinal Aging Study Amsterdam. Am. J. Epidemiol. 2006, 164, 969–977. [Google Scholar] [CrossRef]
- Garcia-Martinez, R.; Caraceni, P.; Bernardi, M.; Gines, P.; Arroyo, V.; Jalan, R. Albumin: Pathophysiologic basis of its role in the treatment of cirrhosis and its complications. Hepatology 2013, 58, 1836–1846. [Google Scholar] [CrossRef]
- Kirsch, R.; Frith, L.; Black, E.; Hoffenberg, R. Regulation of albumin synthesis and catabolism by alteration of dietary protein. Nature 1968, 217, 578–579. [Google Scholar] [CrossRef]
- Don, B.R.; Kaysen, G. Serum albumin: Relationship to inflammation and nutrition. Semin. Dial. 2004, 17, 432–437. [Google Scholar] [CrossRef]
- Avram, C.; Mărușteri, M. Normality Assessment, Few Paradigms and Use Cases. Rev. Rom. Med. Lab. 2022, 30, 251–260. [Google Scholar] [CrossRef]
- Li, C.; Peng, W.; Zhang, X.Y.; Wen, T.F.; Chen, L.P. The preoperative platelet to albumin ratio predicts the prognosis of hepatocellular carcinoma patients without portal hypertension after liver resection. Medicine 2019, 98, e17920. [Google Scholar] [CrossRef]
- Tan, J.; Song, G.; Wang, S.; Dong, L.; Liu, X.; Jiang, Z.; Qin, A.; Tang, Y.; Qin, W. Platelet-to-Albumin Ratio: A Novel IgA Nephropathy Prognosis Predictor. Front. Immunol. 2022, 13, 842362. [Google Scholar] [CrossRef]
- Yang, Y.; Yuan, J.; Liu, L.; Qie, S.; Yang, L.; Yan, Z. Platelet-to-albumin ratio: A risk factor associated with technique failure and mortality in peritoneal dialysis patients. Ren. Fail. 2021, 43, 1359–1367. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Zheng, Q.; Yu, Y.; Zheng, H.; Wu, Y.; Wang, Z.; Liu, L.; Zhang, M.; Liu, T.; Li, H.; et al. Prognostic significance of platelet-to-albumin ratio in patients with esophageal squamous cell carcinoma receiving definitive radiotherapy. Sci. Rep. 2022, 12, 3535. [Google Scholar] [CrossRef]
- Lessomo, F.Y.N.; Fan, Q.; Wang, Z.Q.; Mukuka, C. The relationship between leukocyte to albumin ratio and atrial fibrillation severity. BMC Cardiovasc. Disord. 2023, 23, 67. [Google Scholar] [CrossRef] [PubMed]
- Ko, C.A.; Fang, K.H.; Tsai, M.S.; Lee, Y.C.; Lai, C.H.; Hsu, C.M.; Huang, E.I.; Chang, G.H.; Tsai, Y.T. Prognostic Value of Neutrophil Percentage-to-Albumin Ratio in Patients with Oral Cavity Cancer. Cancers 2022, 14, 4892. [Google Scholar] [CrossRef]
- Ferro, M.; Babă, D.F.; de Cobelli, O.; Musi, G.; Lucarelli, G.; Terracciano, D.; Porreca, A.; Busetto, G.M.; Del Giudice, F.; Soria, F.; et al. Neutrophil percentage-to-albumin ratio predicts mortality in bladder cancer patients treated with neoadjuvant chemotherapy followed by radical cystectomy. Future Sci. OA 2021, 7, FSO709. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Xue, Y.; Wang, J.; Xiang, H.; Ji, K.; Wang, J.; Lin, C. Association between neutrophil-to-albumin ratio and mortality in patients with cardiogenic shock: A retrospective cohort study. BMJ Open 2020, 10, e039860. [Google Scholar] [CrossRef]
- Yu, Y.; Liu, Y.; Ling, X.; Huang, R.; Wang, S.; Min, J.; Xiao, J.; Zhang, Y.; Wang, Z. The Neutrophil Percentage-to-Albumin Ratio as a New Predictor of All-Cause Mortality in Patients with Cardiogenic Shock. BioMed Res. Int. 2020, 2020, 7458451. [Google Scholar] [CrossRef]
- Zhang, Z.L.; Guo, Q.Q.; Tang, J.N.; Zhang, J.C.; Cheng, M.D.; Song, F.H.; Liu, Z.Y.; Wang, K.; Jiang, L.Z.; Fan, L.; et al. Monocyte-to-albumin ratio as a novel predictor of long-term adverse outcomes in patients after percutaneous coronary intervention. Biosci. Rep. 2021, 41, BSR20210154. [Google Scholar] [CrossRef]
- Arques, S. Human serum albumin in cardiovascular diseases. Eur. J. Intern. Med. 2018, 52, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.S.; Cheema, F.H.; Yang, J.; Kawano, Y.; Takayama, H.; Naka, Y.; Farr, M.; Lederer, D.J.; Baldwin, M.R.; Jin, Z.; et al. Preoperative serum albumin levels predict 1-year postoperative survival of patients undergoing heart transplantation. Circ. Heart Fail. 2013, 6, 785–791. [Google Scholar] [CrossRef]
- Castleberry, C.; White-Williams, C.; Naftel, D.; Tresler, M.A.; Pruitt, E.; Miyamoto, S.D.; Murphy, D.; Spicer, R.; Bannister, L.; Schowengerdt, K.; et al. Hypoalbuminemia and poor growth predict worse outcomes in pediatric heart transplant recipients. Pediatr. Transplant. 2014, 18, 280–287. [Google Scholar] [CrossRef]
- Srivastava, A.; Bodnar, J.; Osman, F.; Jorgenson, M.R.; Astor, B.C.; Mandelbrot, D.A.; Parajuli, S. Serum Albumin Level Before Kidney Transplant Predicts Post-transplant BK and Possibly Cytomegalovirus Infection. Kidney Int. Rep. 2020, 5, 2228–2237. [Google Scholar] [CrossRef] [PubMed]
- Hognestad, A.; Michelsen, A.; Brosstad, F.; Damås, J.K.; Holm, T.; Simonsen, S.; Kjekshus, J.K.; Aukrust, P.; Andreassen, A.K. Platelet activation in heart transplant recipients. Clin. Transplant. 2004, 18, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Gawaz, M. Role of platelets in coronary thrombosis and reperfusion of ischemic myocardium. Cardiovasc. Res. 2004, 61, 498–511. [Google Scholar] [CrossRef]
- Dhaliwal, A.; Thohan, V. Cardiac allograft vasculopathy: The Achilles’ heel of long-term survival after cardiac transplantation. Curr. Atheroscler. Rep. 2006, 8, 119–130. [Google Scholar] [CrossRef]
- He, Z.; Wang, H.; Wang, S.; Li, L. Predictive Value of Platelet-to-Albumin Ratio (PAR) for the Cardiac-Associated Acute Kidney Injury and Prognosis of Patients in the Intensive Care Unit. Int. J. Gen. Med. 2022, 15, 8315–8326. [Google Scholar] [CrossRef]
- Rosales, C. Neutrophil: A Cell with Many Roles in Inflammation or Several Cell Types? Front. Physiol. 2018, 9, 113. [Google Scholar] [CrossRef]
- Gaul, D.S.; Stein, S.; Matter, C.M. Neutrophils in cardiovascular disease. Eur. Heart J. 2017, 38, 1702–1704. [Google Scholar] [CrossRef]
- Kain, V.; Halade, G.V. Role of neutrophils in ischemic heart failure. Pharmacol. Ther. 2020, 205, 107424. [Google Scholar] [CrossRef]
- Kawasaki, M.; Meulendijks, E.R.; van den Berg, N.W.E.; Nariswari, F.A.; Neefs, J.; Wesselink, R.; Baalman, S.W.E.; Jongejan, A.; Schelfhorst, T.; Piersma, S.R.; et al. Neutrophil degranulation interconnects over-represented biological processes in atrial fibrillation. Sci. Rep. 2021, 11, 2972. [Google Scholar] [CrossRef] [PubMed]
- Cui, H.; Ding, X.; Li, W.; Chen, H.; Li, H. The neutrophil percentage to albumin ratio as a new predictor of in-hospital mortality in patients with ST-segment elevation myocardial infarction. Med. Sci. Monit. 2019, 25, 7845–7852. [Google Scholar] [CrossRef] [PubMed]
- Dai, K.; Li, Z.; Luo, Y.; Xiong, Q.; Xiong, Y.; Song, Z.; Xiong, W. Neutrophil percentage-to-albumin ratio and monocyte-to-lymphocyte ratio as predictors of free-wall rupture in patients with acute myocardial infarction. J. Clin. Lab. Anal. 2022, 36, e24136. [Google Scholar] [CrossRef] [PubMed]
- Sun, T.; Shen, H.; Guo, Q.; Yang, J.; Zhai, G.; Zhang, J.; Zhang, B.; Ding, Y.; Cai, C.; Zhou, Y. Association between Neutrophil Percentage-to-Albumin Ratio and All-Cause Mortality in Critically Ill Patients with Coronary Artery Disease. BioMed Res. Int. 2020, 2020, 8137576. [Google Scholar] [CrossRef]
- Chiu, S.; Bharat, A. Role of monocytes and macrophages in regulating immune response following lung transplantation. Curr. Opin. Organ Transplant. 2016, 21, 239–245. [Google Scholar] [CrossRef]
- Shi, C.; Pamer, E.G. Monocyte recruitment during infection and inflammation. Nat. Rev. Immunol. 2011, 11, 762–774. [Google Scholar] [CrossRef]
- Knoll, R.; Schultze, J.L.; Schulte-Schrepping, J. Monocytes and Macrophages in COVID-19. Front. Immunol. 2021, 12, 720109. [Google Scholar] [CrossRef]
- Devêvre, E.F.; Renovato-Martins, M.; Clément, K.; Sautès-Fridman, C.; Cremer, I.; Poitou, C. Profiling of the three circulating monocyte subpopulations in human obesity. J. Immunol. 2015, 194, 3917–3923. [Google Scholar] [CrossRef]
- Mossanen, J.C.; Jansen, T.U.; Pracht, J.; Liepelt, A.; Buendgens, L.; Stoppe, C.; Goetzenich, A.; Simon, T.P.; Autschbach, R.; Marx, G.; et al. Elevated circulating CD14++CD16+ intermediate monocytes are independently associated with extracardiac complications after cardiac surgery. Sci. Rep. 2020, 10, 947. [Google Scholar] [CrossRef]
- Talari, K.; Goyal, M. Retrospective studies—Utility and caveats. J. R. Coll. Physicians Edinb. 2020, 50, 398–402. [Google Scholar] [CrossRef] [PubMed]
- Bacușcă, A.E.; Burlacu, A.; Tinică, G.; Enache, M.; Ţărus, A.; Gavriluţă, C.; Brinza, C.; Hanganu, B.; Ioan, B.G. Organ Pro-curement, Donation, and Transplant Awareness in an Urban Eastern European Region: A General Population Survey. Ann. Transplant. 2022, 27, e938016. [Google Scholar] [CrossRef] [PubMed]
- Hackshaw, A. Small studies: Strengths and limitations. Eur. Respir. J. 2008, 32, 1141–1143. [Google Scholar] [CrossRef] [PubMed]
- Feng, D.; Cortese, G.; Baumgartner, R. A comparison of confidence/credible interval methods for the area under the ROC curve for continuous diagnostic tests with small sample size. Stat. Methods Med. Res. 2017, 26, 2603–2621. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Cut-off Value | Author | Year of Publication | Title |
|---|---|---|---|
| PAR > 48 | Li C, et al. [11] | 2019 | The preoperative platelet-to-albumin ratio predicts the prognosis of hepatocellular carcinoma patients without portal hypertension after liver resection |
| PAR > 60.8 | Tan J, et al. [12] | 2022 | Platelet-to-albumin ratio: a novel IgA nephropathy prognosis predictor |
| PAR > 62.7 | Yang Y, et al. [13] | 2021 | Platelet-to-albumin ratio: a risk factor associated with technique failure and mortality in peritoneal dialysis patients |
| PAR > 57 | Huang Z, et al. [14] | 2022 | Prognostic significance of platelet-to-albumin ratio in patients with esophageal squamous cell carcinoma receiving definitive radiotherapy |
| LAR > 2 | Lessomo FYN, et al. [15] | 2023 | The relationship between leukocyte-to-albumin ratio and atrial fibrillation severity |
| NPAR > 16.93 | Ko CA, et al. [16] | 2022 | Prognostic value of neutrophil percentage-to-albumin ratio in patients with oral cavity cancer |
| NPAR > 18 | Ferro M, et al. [17] | 2021 | Neutrophil percentage-to-albumin ratio predicts mortality in bladder cancer patients treated with neoadjuvant chemotherapy followed by radical cystectomy |
| NPAR > 23.54 | Peng Y, et al. [18] | 2020 | Association between neutrophil-to-albumin ratio and mortality in patients with cardiogenic shock: a retrospective cohort study |
| NPAR > 25.3 | Yu Y, et al. [19] | 2020 | The neutrophil percentage-to-albumin ratio as a new predictor of all-cause mortality in patients with cardiogenic shock |
| MAR > 0.14 | Zhang ZL, et al. [20] | 2021 | Monocyte-to-albumin ratio as a novel predictor of long-term adverse outcomes in patients after percutaneous coronary intervention |
| Total (n = 38) | Age < 40 yrs (n = 13) | Age ≥ 40 yrs (n = 25) | |
|---|---|---|---|
| BMI (kg/m2) | |||
| • Mean (SD) | 23.81 (5.18) | 21.01 (5.75) | 25.27 (4.29) |
| • Min | 13.20 | 13.20 | 15.20 |
| • Max | 33.90 | 30.40 | 33.90 |
| ABO blood type | |||
| • O | 13 (34.2%) | 4 (10.5%) | 9 (23.7%) |
| • A | 16 (42.1%) | 4 (10.5%) | 12 (31.6%) |
| • B | 4 (10.5%) | 1 (2.6%) | 3 (7.9%) |
| • AB | 5 (13.2%) | 4 (10.5%) | 1 (2.6%) |
| Diagnosis | |||
| • Non-ischemic (%) | 18 (47.4%) | 6 (15.8%) | 12 (31.6%) |
| • Ischemic (%) | 8 (21.1%) | 1 (2.6%) | 7 (18.4%) |
| • Congenital (%) | 6 (15.8%) | 3 (7.9%) | 3 (7.9%) |
| • Valvular (%) | 3 (7.9%) | 1 (2.6%) | 2 (5.3%) |
| • Hypertrophic (%) | 1 (2.6%) | 0 (0.0%) | 1 (2.6%) |
| • Restrictive (%) | 2 (5.3%) | 2 (5.3%) | 0 (0.0%) |
| Leucocyte count (×109/L) | |||
| • Mean (SD) | 9.00 (4.26) | 9.29 (5.06) | 8.85 (3.89) |
| • Min | 3.47 | 3.47 | 3.91 |
| • Max | 24.74 | 24.55 | 24.74 |
| Neutrophil count (×109/L) | |||
| • Mean (SD) | 6.51 (4.17) | 6.46 (5.10) | 6.54 (3.71) |
| • Min | 2.09 | 2.09 | 2.94 |
| • Max | 22.40 | 22.27 | 22.40 |
| Monocyte count (×109/L) | |||
| • Mean (SD) | 0.77 (0.34) | 0.95 (0.41) | 0.67 (0.25) |
| • Min | 0.17 | 0.41 | 0.17 |
| • Max | 1.89 | 1.89 | 1.19 |
| Platelet count (×109/L) | |||
| • Mean (SD) | 202.11 (62.61) | 201.69 (67.46) | 202.32 (61.38) |
| • Min | 82.00 | 93.00 | 82.00 |
| • Max | 327.00 | 327.00 | 327.00 |
| Albumin (g/dL) | |||
| • Mean (SD) | 4.08 (0.56) | 4.01 (0.37) | 4.12 (0.64) |
| • Min | 2.20 | 3.50 | 2.20 |
| • Max | 5.00 | 4.60 | 5.00 |
| Postoperative complications | |||
| • Any cause | 30 (78.9%) | 11 (28.9%) | 19 (50.0%) |
| • Type 2 DM | 8 (21.1%) | 2 (5.3%) | 6 (15.8%) |
| • Paroxysmal AFib | 6 (15.8%) | 1 (2.6%) | 5 (13.2%) |
| • Acute rejection | 7 (18.4%) | 1 (2.6%) | 6 (15.8%) |
| • Infections | 19 (50.0%) | 8 (21.1%) | 11 (28.9%) |
| Pre- | Post- | p-Values | |
|---|---|---|---|
| ALBUMIN | |||
| • Mean (SD) | 4.08 (0.56) | 3.34 (0.63) | |
| • Min | 2.20 | 1.70 | <0.0001 * |
| • Max | 5.00 | 4.80 | |
| PAR | |||
| • Mean (SD) | 50.48 (17.97) | 40.15 (14.91) | |
| • Min | 20.75 | 18.33 | 0.0010 * |
| • Max | 99.33 | 78.24 | |
| LAR | |||
| • Mean (SD) | 2.26 (1.15) | 4.92 (2.25) | |
| • Min | 0.85 | 0.76 | <0.0001 * |
| • Max | 7.01 | 10.98 | |
| NPAR | |||
| • Mean (SD) | 17.72 (4.19) | 27.19 (6.17) | |
| • Min | 8.73 | 10.91 | <0.0001 * |
| • Max | 27.88 | 48.35 | |
| MAR | |||
| • Mean (SD) | 0.20 (0.10) | 0.28 (0.19) | |
| • Min | 0.03 | 0.05 | 0.0465 ** |
| • Max | 0.54 | 0.96 |
| Complications OR/95% CI | Type 2 DM OR/95% CI | AFib OR/95% CI | Acute Rejection OR/95% CI | Infections OR/95% CI | |
|---|---|---|---|---|---|
| PAR > 48 | 6.40 0.50–80.86 | 0.68 0.11–4.07 | 2.07 0.24–17.50 | 0.31 0.03–2.47 | 3.49 0.57–21.24 |
| PAR > 57 | 1.42 0.09–21.44 | 0.88 0.11–6.75 | 0.91 0.11–7.44 | 0.16 0.01–1.86 | 5.23 0.74–36.98 |
| PAR > 60.8 | 1.75 0.12–25.75 | 0.42 0.03–4.47 | 0.51 0.04–5.87 | 0.32 0.02–3.64 | 2.75 0.38–19.94 |
| PAR > 62.7 | - * - | 0.40 0.03–4.35 | 0.58 0.04–7.25 | 0.35 0.03–4.18 | 2.64 0.36–19.30 |
| LAR > 0.2 | 0.74 0.09–5.55 | 1.42 0.23–8.67 | 4.25 0.42–42.21 | 0.80 0.12–5.23 | 2.06 0.36–11.63 |
| NPAR > 16.93 | 3.23 0.38–27.40 | 0.66 0.08–5.01 | 9.68 0.73–128.36 | 0.09 0.006–1.37 | 0.67 0.11–4.01 |
| NPAR > 18 | 0.94 0.11–7.79 | 0.18 0.01–2.37 | 3.70 0.47–29.00 | 0.27 0.02–3.20 | 1.10 0.17–7.02 |
| NPAR > 23.54 | 0.52 0.03–8.33 | 1.33 0.04–38.84 | 3.75 0.14–97.55 | - * - | * - |
| NPAR > 25.3 | 0.83 0.04–16.99 | * - | - * - | - * - | - * - |
| MAR > 0.14 | 0.43 0.05–3.74 | 7.63 0.45–127.48 | 0.23 0.02–2.61 | - * - | 9.68 1.01–91.95 p = 0.0480 |
| Cut-Off | AUC | 95% CI | p-Value | Sensitivity | Specificity | |
|---|---|---|---|---|---|---|
| PAR | >38.84 | 0.771 | 0.606–0.891 | 0.0039 | 83.3 | 75.0 |
| LAR | <3.17 | 0.600 | 0.429–0.755 | 0.4768 | 96.7 | 37.5 |
| NPAR | >15.35 | 0.538 | 0.369–0.700 | 0.7913 | 76.7 | 50.0 |
| MAR | >0.14 | 0.625 | 0.453–0.776 | 0.3341 | 73.3 | 62.5 |
| Cut-Off | AUC | 95%CI | p-Value | Sensitivity | Specificity | |
|---|---|---|---|---|---|---|
| PAR | >40.26 | 0.720 | 0.551–0.853 | 0.0123 | 89.5 | 57.9 |
| LAR | >1.83 | 0.518 | 0.350–0.683 | 0.8633 | 79.0 | 53.6 |
| NPAR | <20.18 | 0.548 | 0.379–0.710 | 0.6178 | 94.7 | 26.3 |
| MAR | >0.15 | 0.687 | 0.516–0.827 | 0.0429 | 84.2 | 57.9 |
| Complications | Infections | |||||
|---|---|---|---|---|---|---|
| R-Value | 95% CI | p-Value | R-Value | 95% CI | p-Value | |
| PAR | 0.38 | 0.07–0.62 | 0.0177 | 0.38 | 0.07–0.62 | 0.0181 |
| LAR | −0.14 | −0.44–0.18 | 0.3975 | 0.03 | −0.29–0.34 | 0.8525 |
| NPAR | 0.05 | −0.27–0.36 | 0.7521 | −0.08 | −0.39–0.24 | 0.6161 |
| MAR | 0.17 | −0.15–0.47 | 0.2881 | 0.32 | 0.005–0.58 | 0.0468 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baba, D.-F.; Suciu, H.; Huma, L.; Avram, C.; Danilesco, A.; Moldovan, D.A.; Opincar, A.S.; Sin, A.I. Platelet-to-Albumin Ratio: The Prognostic Utility in the Prediction of 2-Month Postoperative Heart Transplant Complications. J. Cardiovasc. Dev. Dis. 2023, 10, 241. https://doi.org/10.3390/jcdd10060241
Baba D-F, Suciu H, Huma L, Avram C, Danilesco A, Moldovan DA, Opincar AS, Sin AI. Platelet-to-Albumin Ratio: The Prognostic Utility in the Prediction of 2-Month Postoperative Heart Transplant Complications. Journal of Cardiovascular Development and Disease. 2023; 10(6):241. https://doi.org/10.3390/jcdd10060241
Chicago/Turabian StyleBaba, Dragos-Florin, Horatiu Suciu, Laurentiu Huma, Calin Avram, Alina Danilesco, Diana Andreea Moldovan, Andrei Stefan Opincar, and Anca Ileana Sin. 2023. "Platelet-to-Albumin Ratio: The Prognostic Utility in the Prediction of 2-Month Postoperative Heart Transplant Complications" Journal of Cardiovascular Development and Disease 10, no. 6: 241. https://doi.org/10.3390/jcdd10060241