
Left Ventricular Ejection Fraction Association with Acute Ischemic Stroke Outcomes in Patients Undergoing Thrombolysis
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
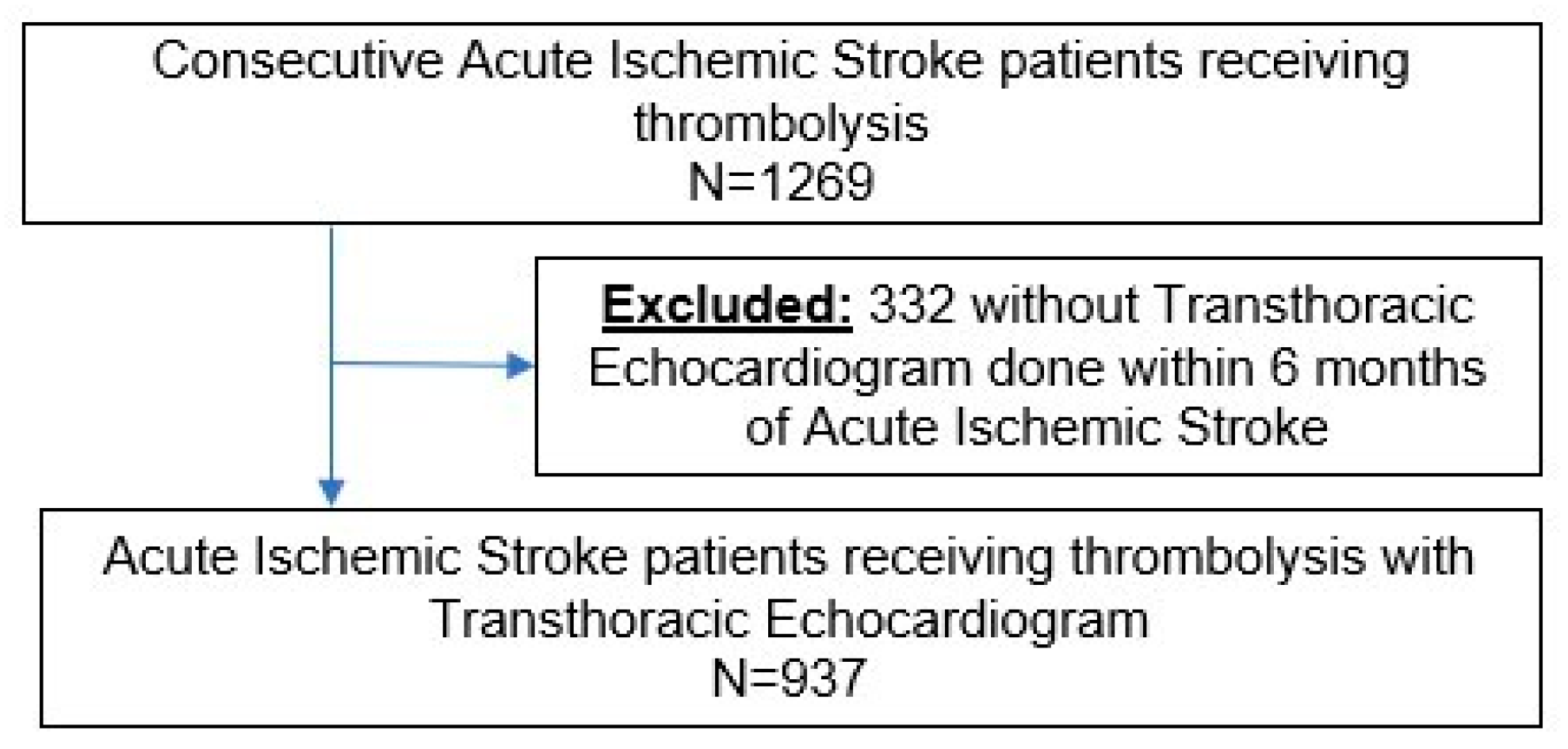
2.1. Study Design and Patient Demographics
2.2. Echocardiographic Data Acquisition and Analysis
2.3. Evaluation of Outcomes
2.4. Statistical Analysis
2.5. Ethics Approval
3. Results
3.1. Demographics
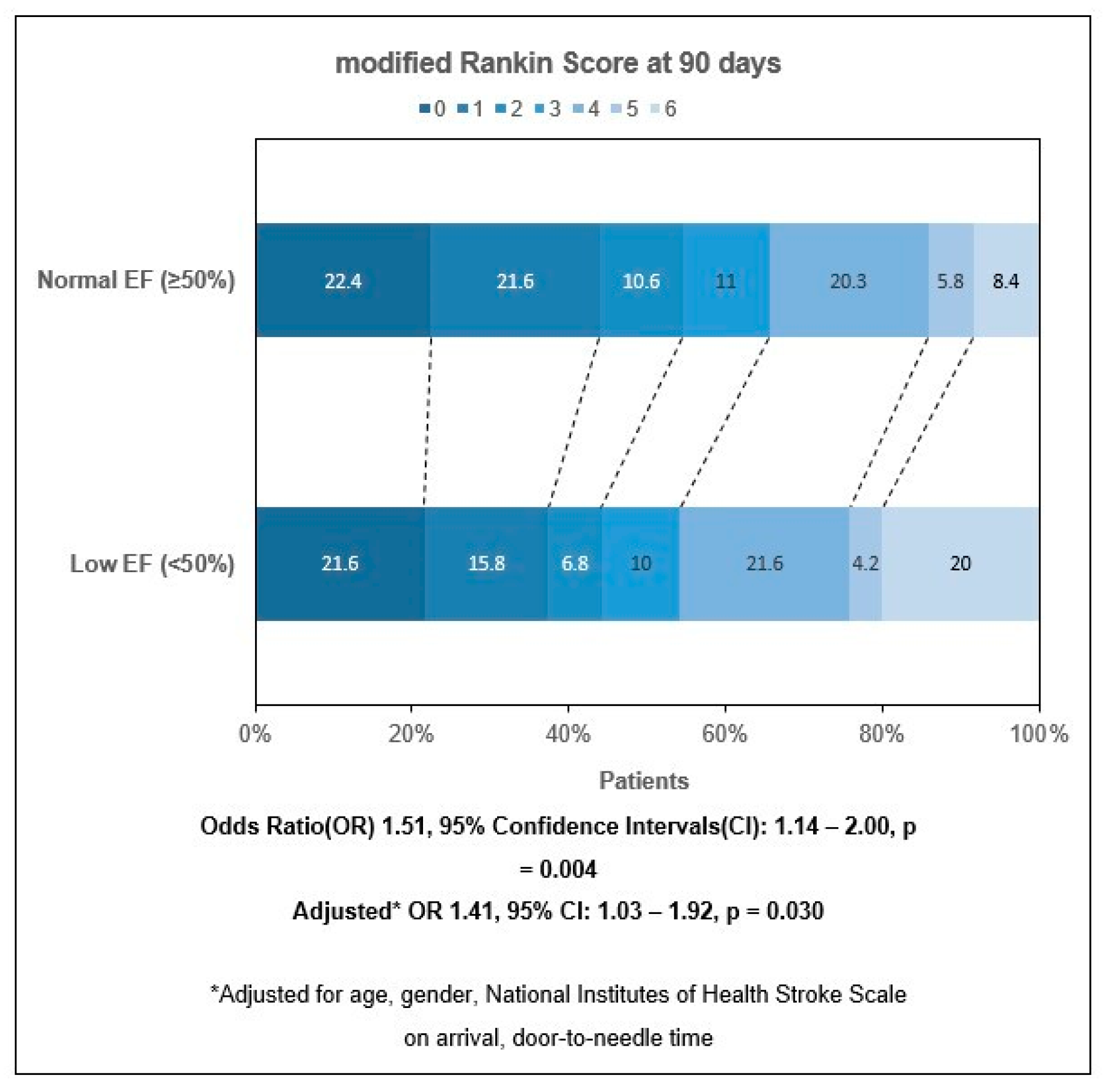
3.2. mRS Outcomes at 3 Months
3.3. Outcomes of All Cause Mortality, Subsequent HF Admission and Subsequent MI Event
4. Discussion
4.1. Moving Forward
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feigin, V.L.; Stark, B.A.; Johnson, C.O.; Roth, G.A.; Bisignano, C.; Abady, G.G.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V.; et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Lees, K.R.; Bluhmki, E.; von Kummer, R.; Brott, T.G.; Toni, D.; Grotta, J.C.; Albers, G.W.; Kaste, M.; Marler, J.R.; Hamilton, S.A.; et al. Time to treatment with intravenous alteplase and outcome in stroke: An updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet 2010, 375, 1695–1703. [Google Scholar] [CrossRef] [PubMed]
- Arboix, A. Cardiovascular risk factors for acute stroke: Risk profiles in the different subtypes of ischemic stroke. World J. Clin. Cases 2015, 3, 418–429. [Google Scholar] [CrossRef] [PubMed]
- Hays, A.G.; Sacco, R.L.; Rundek, T.; Sciacca, R.R.; Jin, Z.; Liu, R.; Homma, S.; Di Tullio, M.R. Left ventricular systolic dysfunction and the risk of ischemic stroke in a multiethnic population. Stroke 2006, 37, 1715–1719. [Google Scholar] [CrossRef]
- Loh, E.; Sutton, M.S.; Wun, C.C.; Rouleau, J.L.; Flaker, G.C.; Gottlieb, S.S.; Lamas, G.A.; Moyé, L.A.; Goldhaber, S.Z.; Pfeffer, M.A. Ventricular dysfunction and the risk of stroke after myocardial infarction. N. Engl. J. Med. 1997, 336, 251–257. [Google Scholar] [CrossRef]
- Cuadrado-Godia, E.; Ois, A.; Roquer, J. Heart failure in acute ischemic stroke. Curr. Cardiol. Rev. 2010, 6, 202–213. [Google Scholar] [CrossRef]
- Choi, B.R.; Kim, J.S.; Yang, Y.J.; Park, K.M.; Lee, C.W.; Kim, Y.H.; Hong, M.K.; Song, J.K.; Park, S.W.; Park, S.J.; et al. Factors associated with decreased cerebral blood flow in congestive heart failure secondary to idiopathic dilated cardiomyopathy. Am. J. Cardiol. 2006, 97, 1365–1369. [Google Scholar] [CrossRef]
- Georgiadis, D.; Sievert, M.; Cencetti, S.; Uhlmann, F.; Krivokuca, M.; Zierz, S.; Werdan, K. Cerebrovascular reactivity is impaired in patients with cardiac failure. Eur. Heart J. 2000, 21, 407–413. [Google Scholar] [CrossRef]
- Kim, J.H.; Shah, P.; Tantry, U.S.; Gurbel, P.A. Coagulation abnormalities in heart failure: Pathophysiology and therapeutic implications. Curr. Heart Fail. Rep. 2016, 13, 319–328. [Google Scholar] [CrossRef]
- Hopper, I.; Skiba, M.; Krum, H. Updated meta-analysis on antithrombotic therapy in patients with heart failure and sinus rhythm. Eur. J. Heart Fail. 2013, 15, 69–78. [Google Scholar] [CrossRef]
- Abdul-Rahim, A.H.; Fulton, R.L.; Frank, B.; McMurray, J.J.; Lees, K.R. Associations of chronic heart failure with outcome in acute ischaemic stroke patients who received systemic thrombolysis: Analysis from VISTA. Eur. J. Neurol. 2015, 22, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Ois, A.; Gomis, M.; Cuadrado-Godia, E.; Jiménez-Conde, J.; Rodríguez-Campello, A.; Bruguera, J.; Molina, L.; Comin, J.; Roquer, J. Heart failure in acute ischemic stroke. J. Neurol. 2008, 255, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Milionis, H.; Faouzi, M.; Cordier, M.; D’Ambrogio-Remillard, S.; Eskandari, A.; Michel, P. Characteristics and early and long-term outcome in patients with acute ischemic stroke and low ejection fraction. Int. J. Cardiol. 2013, 168, 1082–1087. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, V.; Baldasseroni, S.; Nencini, P.; Pracucci, G.; Arba, F.; Piccardi, B.; Marella, G.A.; Di Bari, M.; Gensini, G.F.; Marchionni, N.; et al. The coexistence of heart failure predicts short term mortality, but not disability, in patients with acute ischemic stroke treated with thrombolysis: The Florence area Registry. Eur. J. Intern. Med. 2012, 23, 552–557. [Google Scholar] [CrossRef]
- Kim, W.J.; Nah, H.W.; Kim, D.H.; Cha, J.K. Association between Left Ventricular Dysfunction and Functional Outcomes at Three Months in Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2016, 25, 2247–2252. [Google Scholar] [CrossRef]
- Tan, B.Y.Q.; Leow, A.S.; Lee, T.H.; Gontu, V.K.; Andersson, T.; Holmin, S.; Wong, H.F.; Lin, C.M.; Cheng, C.K.; Sia, C.H.; et al. Left ventricular systolic dysfunction is associated with poor functional outcomes after endovascular thrombectomy. J. Neurointerv. Surg. 2021, 13, 515–518. [Google Scholar] [CrossRef]
- Lyden, P.; Raman, R.; Liu, L.; Emr, M.; Warren, M.; Marler, J. National Institutes of Health Stroke Scale certification is reliable across multiple venues. Stroke 2009, 40, 2507–2511. [Google Scholar] [CrossRef]
- Rankin, J. Cerebral vascular accidents in patients over the age of 60: II. Prognosis. Scott. Med. J. 1957, 2, 200–215. [Google Scholar] [CrossRef]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef]
- Zaidat, O.O.; Lazzaro, M.A.; Liebeskind, D.S.; Janjua, N.; Wechsler, L.; Nogueira, R.G.; Edgell, R.C.; Kalia, J.S.; Badruddin, A.; English, J.; et al. Revascularization grading in endovascular acute ischemic stroke therapy. Neurology 2012, 79, S110–S116. [Google Scholar] [CrossRef]
- Ministry of Health, Singapore. Available online: https://www.moh.gov.sg/hpp/doctors/guidelines/GuidelineDetails/clinical-practice-guidelines-medical (accessed on 28 April 2023).
- Ministry of Health, Singapore. Available online: https://www.moh.gov.sg/hpp/doctors/guidelines/GuidelineDetails/cpgmed_hypertension (accessed on 28 April 2023).
- Ministry of Health, Singapore. Available online: https://www.moh.gov.sg/hpp/doctors/guidelines/GuidelineDetails/cpgmed_diabetes_mellitus (accessed on 28 April 2023).
- Ministry of Health, Singapore. Available online: https://www.moh.gov.sg/hpp/doctors/guidelines/GuidelineDetails/cpgmed_lipids (accessed on 28 April 2023).
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 16, 233–271. [Google Scholar]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, e263–e421. [Google Scholar] [CrossRef] [PubMed]
- Kosaraju, A.; Goyal, A.; Grigorova, Y.; Makaryus, A.N. Left Ventricular Ejection Fraction; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Banks, J.L.; Marotta, C.A. Outcomes validity and reliability of the modified Rankin scale: Implications for stroke clinical trials: A literature review and synthesis. Stroke 2007, 38, 1091–1096. [Google Scholar] [CrossRef] [PubMed]
- Berge, E.; Whiteley, W.; Audebert, H.; De Marchis, G.M.; Fonseca, A.C.; Padiglioni, C.; de la Ossa, N.P.; Strbian, D.; Tsivgoulis, G.; Turc, G. European Stroke Organisation (ESO) guidelines on intravenous thrombolysis for acute ischaemic stroke. Eur. Stroke J. 2021, 6, I–lxii. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.P., Jr.; Brott, T.G.; Furlan, A.J.; Gomez, C.R.; Grotta, J.; Helgason, C.M.; Kwiatkowski, T.; Lyden, P.D.; Marler, J.R.; Torner, J.; et al. Guidelines for thrombolytic therapy for acute stroke: A supplement to the guidelines for the management of patients with acute ischemic stroke. A statement for healthcare professionals from a Special Writing Group of the Stroke Council, American Heart Association. Circulation 1996, 94, 1167–1174. [Google Scholar]
- Wechsler, L.R. Intravenous thrombolytic therapy for acute ischemic stroke. N. Engl. J. Med. 2011, 364, 2138–2146. [Google Scholar] [CrossRef]
- Wardlaw, J.M.; Murray, V.; Berge, E.; del Zoppo, G.J. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst. Rev. 2014, 2014, Cd000213. [Google Scholar] [CrossRef]
- Nagakane, Y.; Christensen, S.; Brekenfeld, C.; Ma, H.; Churilov, L.; Parsons, M.W.; Levi, C.R.; Butcher, K.S.; Peeters, A.; Barber, P.A.; et al. EPITHET: Positive Result After Reanalysis Using Baseline Diffusion-Weighted Imaging/Perfusion-Weighted Imaging Co-Registration. Stroke 2011, 42, 59–64. [Google Scholar] [CrossRef]
- Hacke, W.; Kaste, M.; Bluhmki, E.; Brozman, M.; Dávalos, A.; Guidetti, D.; Larrue, V.; Lees, K.R.; Medeghri, Z.; Machnig, T.; et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N. Engl. J. Med. 2008, 359, 1317–1329. [Google Scholar] [CrossRef]
- The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue Plasminogen Activator for Acute Ischemic Stroke. N. Engl. J. Med. 1995, 333, 1581–1588. [Google Scholar] [CrossRef]
- Albers, G.W.; Clark, W.M.; Madden, K.P.; Hamilton, S.A. ATLANTIS trial: Results for patients treated within 3 hours of stroke onset. Alteplase Thrombolysis for Acute Noninterventional Therapy in Ischemic Stroke. Stroke 2002, 33, 493–495. [Google Scholar] [CrossRef]
- Li, Y.; Fitzgibbons, T.P.; McManus, D.D.; Goddeau, R.P., Jr.; Silver, B.; Henninger, N. Left Ventricular Ejection Fraction and Clinically Defined Heart Failure to Predict 90-Day Functional Outcome After Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2019, 28, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Siedler, G.; Sommer, K.; Macha, K.; Marsch, A.; Breuer, L.; Stoll, S.; Engelhorn, T.; Dörfler, A.; Arnold, M.; Schwab, S.; et al. Heart Failure in Ischemic Stroke: Relevance for Acute Care and Outcome. Stroke 2019, 50, 3051–3056. [Google Scholar] [CrossRef] [PubMed]
- Rojek, A.; Gąsecki, D.; Fijałkowski, M.; Kowalczyk, K.; Kwarciany, M.; Wolf, J.; Nyka, W.; Boutouyrie, P.; Laurent, S.; Narkiewicz, K.; et al. Left ventricular ejection fraction and aortic stiffness are independent predictors of neurological outcome in acute ischemic stroke. J. Hypertens. 2016, 34, 2441–2448. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.O.; Kilbreath, S.L.; Davis, G.M.; Zeman, B.; Raymond, J. Cardiorespiratory fitness and walking ability in subacute stroke patients. Arch. Phys. Med. Rehabil. 2003, 84, 1780–1785. [Google Scholar] [CrossRef] [PubMed]
- Prosser, J.; MacGregor, L.; Lees, K.R.; Diener, H.C.; Hacke, W.; Davis, S. Predictors of early cardiac morbidity and mortality after ischemic stroke. Stroke 2007, 38, 2295–2302. [Google Scholar] [CrossRef] [PubMed]
- Wrigley, P.; Khoury, J.; Eckerle, B.; Alwell, K.; Moomaw, C.J.; Woo, D.; Flaherty, M.L.; De Los Rios la Rosa, F.; Mackey, J.; Adeoye, O.; et al. Prevalence of Positive Troponin and Echocardiogram Findings and Association with Mortality in Acute Ischemic Stroke. Stroke 2017, 48, 1226–1232. [Google Scholar] [CrossRef]
- Scheitz, J.F.; Nolte, C.H.; Doehner, W.; Hachinski, V.; Endres, M. Stroke-heart syndrome: Clinical presentation and underlying mechanisms. Lancet Neurol. 2018, 17, 1109–1120. [Google Scholar] [CrossRef]
- Choi, J.Y.; Cha, J.; Jung, J.M.; Seo, W.K.; Oh, K.; Cho, K.H.; Yu, S. Left ventricular wall motion abnormalities are associated with stroke recurrence. Neurology 2017, 88, 586–594. [Google Scholar] [CrossRef]
- Wang, M.; Peng, Y. Advances in brain-heart syndrome: Attention to cardiac complications after ischemic stroke. Front. Mol. Neurosci. 2022, 15, 1053478. [Google Scholar] [CrossRef]
- Chen, Z.; Venkat, P.; Seyfried, D.; Chopp, M.; Yan, T.; Chen, J. Brain-Heart Interaction: Cardiac Complications After Stroke. Circ. Res. 2017, 121, 451–468. [Google Scholar] [CrossRef] [PubMed]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar] [PubMed]
- Jung, J.M.; Kim, Y.H.; Yu, S.O.K.; Kim, C.K.; Song, T.J.; Kim, Y.J.; Kim, B.J.; Heo, S.H.; Park, K.Y.; Kim, J.M. Long-Term Outcomes of Real-World Korean Patients with Atrial-Fibrillation-Related Stroke and Severely Decreased Ejection Fraction. J. Clin. Neurol. 2019, 15, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Yaghi, S.; Moon, Y.P.; Mora-McLaughlin, C.; Willey, J.Z.; Cheung, K.; Di Tullio, M.R.; Homma, S.; Kamel, H.; Sacco, R.L.; Elkind, M.S. Left atrial enlargement and stroke recurrence: The Northern Manhattan Stroke Study. Stroke 2015, 46, 1488–1493. [Google Scholar] [CrossRef] [PubMed]
- Kaarisalo, M.M.; Immonen-Räihä, P.; Marttila, R.J.; Salomaa, V.; Kaarsalo, E.; Salmi, K.; Sarti, C.; Sivenius, J.; Torppa, J.; Tuomilehto, J. Atrial fibrillation and stroke. Mortality and causes of death after the first acute ischemic stroke. Stroke 1997, 28, 311–315. [Google Scholar] [CrossRef]
- Marini, C.; De Santis, F.; Sacco, S.; Russo, T.; Olivieri, L.; Totaro, R.; Carolei, A. Contribution of atrial fibrillation to incidence and outcome of ischemic stroke: Results from a population-based study. Stroke 2005, 36, 1115–1119. [Google Scholar] [CrossRef]
- Lau, L.H.; Lew, J.; Borschmann, K.; Thijs, V.; Ekinci, E.I. Prevalence of diabetes and its effects on stroke outcomes: A meta-analysis and literature review. J. Diabetes Investig. 2019, 10, 780–792. [Google Scholar] [CrossRef]
- Gofir, A.; Mulyono, B.; Sutarni, S. Hyperglycemia as a prognosis predictor of length of stay and functional outcomes in patients with acute ischemic stroke. Int. J. Neurosci. 2017, 127, 923–929. [Google Scholar] [CrossRef]
- Tokgoz, S.; Kayrak, M.; Akpinar, Z.; Seyithanoğlu, A.; Güney, F.; Yürüten, B. Neutrophil lymphocyte ratio as a predictor of stroke. J. Stroke Cerebrovasc. Dis. 2013, 22, 1169–1174. [Google Scholar] [CrossRef]
- Thanvi, B.; Treadwell, S.; Robinson, T. Early neurological deterioration in acute ischaemic stroke: Predictors, mechanisms and management. Postgrad. Med. J. 2008, 84, 412–417. [Google Scholar] [CrossRef]
- Kenchaiah, S.; Pfeffer, M.A. Cardiac remodeling in systemic hypertension. Med. Clin. N. Am. 2004, 88, 115–130. [Google Scholar] [CrossRef] [PubMed]
- Oh, G.C.; Cho, H.J. Blood pressure and heart failure. Clin. Hypertens 2020, 26, 1. [Google Scholar] [CrossRef] [PubMed]
- Szapáry, L.; Tornyos, D.; Kupó, P.; Lukács, R.; El Alaoui El Abdallaoui, O.; Komócsi, A. Combination of antiplatelet and anticoagulant therapy, component network meta-analysis of randomized controlled trials. Front. Cardiovasc. Med. 2022, 9, 1036609. [Google Scholar] [CrossRef] [PubMed]
- Bálint, A.; Tornyos, D.; El Alaoui El Abdallaoui, O.; Kupó, P.; Komócsi, A. Network Meta-Analysis of Ticagrelor for Stroke Prevention in Patients at High Risk for Cardiovascular or Cerebrovascular Events. Stroke 2021, 52, 2809–2816. [Google Scholar] [CrossRef] [PubMed]
- Elnour, A.A.; Komócsi, A.; Kupó, P.; El Khidir, I.Y.; Zachariah, S.; Sam, K.G.; Asim, S.; Sadeq, A. The Role of Direct Oral Anticoagulant in Patients with Acute Coronary Syndrome on Single or Dual Antiplatelet Regime: Review of Opportunities and Challenges. Curr. Rev. Clin. Exp. Pharmacol. 2021, 16, 52–63. [Google Scholar] [CrossRef]
- Tornyos, D.; Komócsi, A.; Bálint, A.; Kupó, P.; El Abdallaoui, O.E.A.; Szapáry, L.; Szapáry, L.B. Antithrombotic therapy for secondary prevention in patients with stroke or transient ischemic attack: A multiple treatment network meta-analysis of randomized controlled trials. PLoS ONE 2022, 17, e0273103. [Google Scholar] [CrossRef]
- Barnes, G.D. Combining antiplatelet and anticoagulant therapy in cardiovascular disease. Hematol. Am. Soc. Hematol. Educ. Program 2020, 2020, 642–648. [Google Scholar] [CrossRef]
- Kumbhani, D.J.; Cannon, C.P.; Beavers, C.J.; Bhatt, D.L.; Cuker, A.; Gluckman, T.J.; Marine, J.E.; Mehran, R.; Messe, S.R.; Patel, N.S.; et al. 2020 ACC Expert Consensus Decision Pathway for Anticoagulant and Antiplatelet Therapy in Patients with Atrial Fibrillation or Venous Thromboembolism Undergoing Percutaneous Coronary Intervention or With Atherosclerotic Cardiovascular Disease. J. Am. Coll. Cardiol. 2021, 77, 629–658. [Google Scholar] [CrossRef]
- Homma, S.; Thompson, J.L.P.; Pullicino, P.M.; Levin, B.; Freudenberger, R.S.; Teerlink, J.R.; Ammon, S.E.; Graham, S.; Sacco, R.L.; Mann, D.L.; et al. Warfarin and Aspirin in Patients with Heart Failure and Sinus Rhythm. N. Engl. J. Med. 2012, 366, 1859–1869. [Google Scholar] [CrossRef]
- Schäfer, A.; Flierl, U.; Bauersachs, J. Anticoagulants for stroke prevention in heart failure with reduced ejection fraction. Clin. Res. Cardiol. 2022, 111, 1–13. [Google Scholar] [CrossRef]
- Zannad, F.; Anker, S.D.; Byra, W.M.; Cleland, J.G.F.; Fu, M.; Gheorghiade, M.; Lam, C.S.P.; Mehra, M.R.; Neaton, J.D.; Nessel, C.C.; et al. Rivaroxaban in Patients with Heart Failure, Sinus Rhythm, and Coronary Disease. N. Engl. J. Med. 2018, 379, 1332–1342. [Google Scholar] [CrossRef] [PubMed]
- Soman, P.; Lahiri, A.; Mieres, J.H.; Calnon, D.A.; Wolinsky, D.; Beller, G.A.; Sias, T.; Burnham, K.; Conway, L.; McCullough, P.A.; et al. Etiology and pathophysiology of new-onset heart failure: Evaluation by myocardial perfusion imaging. J. Nucl. Cardiol. 2009, 16, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Yatteau, R.F.; Peter, R.H.; Behar, V.S.; Bartel, A.G.; Rosati, R.A.; Kong, Y. Ischemic cardiomyopathy: The myopathy of coronary artery disease. Natural history and results of medical versus surgical treatment. Am. J. Cardiol. 1974, 34, 520–525. [Google Scholar] [CrossRef] [PubMed]
- Scheitz, J.F.; Sposato, L.A.; Schulz-Menger, J.; Nolte, C.H.; Backs, J.; Endres, M. Stroke-Heart Syndrome: Recent Advances and Challenges. J. Am. Heart Assoc. 2022, 11, e026528. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [PubMed]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2018, 49, e46–e110. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | LVSD (n = 190) | Normal LVEF (n = 747) | p-Value |
|---|---|---|---|
| Baseline characteristics | |||
| Age (years), mean (SD) | 65.4 (13.8) | 65.2 (13.5) | 0.877 |
| Female, % (n) | 30.1 (56) | 40.4 (296) | 0.010 |
| Ethnicity, % (n) | 0.002 | ||
| Chinese | 56.3 (94) | 69.5 (459) | 0.001 |
| Malay | 30.5 (51) | 18.9 (125) | 0.001 |
| Indian | 9.0 (15) | 5.9 (39) | 0.151 |
| Others | 4.2 (7) | 5.6 (37) | 0.467 |
| Comorbidities | |||
| Hypertension, % (n) | 76.3 (145) | 77.1 (576) | 0.817 |
| Dyslipidemia, % (n) | 62.1 (118) | 49.9 (373) | 0.003 |
| Diabetes Mellitus, % (n) | 52.6 (100) | 37.5 (280) | <0.001 |
| Atrial Fibrillation, % (n) | 36.3 (69) | 28.4 (212) | 0.033 |
| Ischemic Heart Disease, % (n) | 68.4 (130) | 19.4 (145) | <0.001 |
| Heart Failure, % (n) | 78.9 (150) | 6.2 (46) | <0.001 |
| Previous Percutaneous Coronary Intervention, % (n) | 18.4 (35) | 5.6 (42) | <0.001 |
| Previous Coronary Artery Bypass Graft, % (n) | 11.1 (21) | 2.8 (21) | <0.001 |
| National Institutes of Health Stroke Scale on arrival, median (IQR) | 18.0 (11.0–22.0) | 15.0 (8.0–21.0) | 0.003 |
| Variables | LVSD (n = 190) | Normal LVEF (n = 747) | p-Value |
|---|---|---|---|
| Investigation findings | |||
| Left Ventricular Ejection Fraction (%), mean (SD) | 33.5 (9.84) | 63.0 (5.02) | <0.001 |
| Site of occlusion | 0.179 | ||
| M1—Middle Cerebral Artery, % (n) | 34.2 (65) | 29.2 (218) | 0.178 |
| M2—Middle Cerebral Artery, % (n) | 2.6 (5) | 1.1 (8) | 0.154 |
| Terminal Internal Carotid Artery, % (n) | 14.2 (27) | 11.8 (88) | 0.362 |
| No Large Vessel Occlusion, % (n) | 13.7 (26) | 27.7 (207) | <0.001 |
| Basilar Artery, % (n) | 6.3 (12) | 7.5 (56) | 0.575 |
| Tandem, % (n) | 7.9 (15) | 8.4 (63) | 0.810 |
| TOAST Classification | <0.001 | ||
| 1 | 17.4 (33) | 23.2 (173) | |
| 2 | 42.6 (81) | 31.7 (237) | |
| 3 | 3.2 (6) | 9.1 (68) | |
| 4 | 0 (0) | 1.9 (14) | |
| 5 | 18.4 (35) | 12.2 (91) | |
| Procedure | |||
| Time from stroke onset to needle (min), mean (SD) | 157.3 (57.8) | 165.0 (62.4) | 0.133 |
| Time from door to needle (min), mean (SD) | 82.7 (41.3) | 81.9 (50.5) | 0.856 |
| Recanalization of vascular occlusion, % (n) | 0.006 | ||
| Complete recanalization, % (n) | 20.5 (39) | 21.2 (158) | |
| Partial recanalization, % (n) | 7.4 (14) | 6.3 (47) | |
| No recanalization, % (n) | 18.4 (35) | 13.1 (98) | |
| No occlusion, % (n) | 13.7 (26) | 25.6 (191) | |
| Variables | LVSD (n = 190) | Normal LVEF (n = 747) | p-Value |
|---|---|---|---|
| Outcomes | |||
| Modified Rankin Scale (mRS) at 3 months, % (n) | <0.001 | ||
| 0 | 21.6 (41) | 22.4 (167) | 0.818 |
| 1 | 15.8 (30) | 21.6 (161) | 0.078 |
| 2 | 6.8 (13) | 10.6 (79) | 0.123 |
| 3 | 10.0 (19) | 11.0 (82) | 0.698 |
| 4 | 21.6 (41) | 20.3 (152) | 0.708 |
| 5 | 4.2 (8) | 5.8 (43) | 0.402 |
| 6 | 20.0 (38) | 8.4 (63) | <0.001 |
| Functional independence at 3 months (mRS 0–2), % (n) | 45.3 (86) | 55.0 (411) | 0.016 |
| All-cause mortality, % (n) | 58.9 (112) | 29.6 (221) | <0.001 |
| Subsequent heart failure admission, % (n) | 28.4 (54) | 6.6 (49) | <0.001 |
| Subsequent myocardial infarction, % (n) | 16.3 (31) | 6.2 (4.6) | <0.001 |
| Recurrent stroke/transient ischemic attack, % (n) | 15.3 (29) | 17.0 (127) | 0.566 |
| Symptomatic intracerebral hemorrhage, % (n) | 5.3 (10) | 3.1 (23) | 0.145 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Covariates | Hazards Ratio (95% CI) | p Value | Adjusted Hazards Ratio (95% CI) | p Value |
| Left Ventricular Systolic Dysfunction | 0.399 [0.318, 0.501] | <0.001 | 3.38 [1.74, 6.54] | <0.001 |
| Age | 1.04 [1.03, 1.05] | <0.001 | 1.07 [1.04, 1.09] | <0.001 |
| Female Sex | 1.01 [0.809, 1.26] | 0.921 | ||
| Race | ||||
| Chinese (REF) | 0.441 | |||
| Malay | 1.29 [0.989, 1.69] | 0.061 | 1.25 [0.676, 2.30] | 0.479 |
| Indian | 0.952 [0.587, 1.54] | 0.841 | 1.90 [0.719, 5.00] | 0.196 |
| Other | 0.434 [0.204, 0.922] | 0.030 | 0.615 [0.159, 2.38] | 0.481 |
| Hypertension | 1.26 [0.963, 1.64] | 0.093 | ||
| Dyslipidemia | 1.29 [1.04, 1.61] | 0.022 | 0.914 [0.545, 1.53] | 0.733 |
| Diabetes Mellitus | 1.72 [1.38, 213] | <0.001 | 1.84 [1.10, 3.07] | 0.020 |
| Atrial Fibrillation | 1.39 [1.11, 1.74] | 0.004 | 0.327 [0.115, 0.930] | 0.036 |
| Ischemic Heart Disease | 2.04 [1.64, 2.54] | <0.001 | 1.63 [0.895, 2.96] | 0.111 |
| National Institutes of Health Stroke Scale on arrival | 1.06 [1.04, 1.07] | <0.001 | 1.03 [0.991, 1.07] | 0.129 |
| TOAST Classification | ||||
| 1 (REF) | 0.001 | 0.054 | ||
| 2 | 1.57 [1.10, 2.26] | 0.014 | 1.83 [0.627, 5.33] | 0.269 |
| 3 | 0.704 [0.391, 1.27] | 0.242 | 0.814 [0.288, 2.30] | 0.699 |
| 4 | 0.761 [0.230, 2.51] | 0.653 | 0.978 [0.082, 11.7] | 0.986 |
| 5 | 0.703 [0.432, 1.14] | 0.156 | 0.351 [0.151, 0.817] | 0.015 |
| Recanalization | ||||
| No occlusion (REF) | 0.002 | 0.389 | ||
| Complete recanalization | 2.02 [1.33, 3.07] | 0.001 | 1.33 [0.598, 2.94] | 0.482 |
| Partial recanalization | 1.37 [0.732, 2.55] | 0.327 | 0.931 [0.327, 2.65] | 0.893 |
| No recanalization | 2.13 [1.34, 3.38] | 0.001 | 1.84 [0.764, 4.41] | 0.175 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Covariates | Hazards Ratio (95% CI) | p Value | Adjusted Hazards Ratio (95% CI) | p Value |
| Left Ventricular Systolic Dysfunction | 6.75 [4.57, 9.95] | <0.002 | 4.23 [2.17, 8.26] | <0.001 |
| Age | 1.03 [1.01, 1.04] | 0.001 | 1.02 [0.995, 1.04] | 0.008 |
| Female Sex | 0.895 [0.598, 1.34] | 0.590 | ||
| Race | ||||
| Chinese (REF) | 0.752 | |||
| Malay | 1.24 [0.763, 2.03] | 0.382 | ||
| Indian | 1.31 [0.627, 2.75] | 0.472 | ||
| Other | 1.25 [0.540, 2.89] | 0.607 | ||
| Hypertension | 1.05 [0.665, 1.64] | 0.848 | ||
| Dyslipidemia | 1.85 [1.23, 2.79] | 0.003 | 1.50 [0.833, 2.72] | 0.175 |
| Diabetes Mellitus | 2.14 [1.45, 3.16] | <0.001 | 0.966 [0.538, 1.73] | 0.907 |
| Atrial Fibrillation | 1.94 [1.31, 2.86] | 0.001 | 1.54 [0.835, 2.83] | 0.168 |
| Ischemic Heart Disease | 3.21 [2.18, 4.72] | <0.001 | 1.09 [0.566, 2.10] | 0.797 |
| National Institutes of Health Stroke Scale on arrival | 0.992 [0.965, 1.02] | 0.552 | ||
| TOAST Classification | ||||
| 1 (REF) | 0.329 | |||
| 2 | 1.61 [0.925, 2.81] | 0.092 | ||
| 3 | 0.821 [0.316, 2.13] | 0.684 | ||
| 4 | 0.715 [0.089, 5.76] | 0.753 | ||
| 5 | 1.26 [0.618, 2.56] | 0.528 | ||
| Recanalization | ||||
| No occlusion (REF) | 0.032 | 0.071 | ||
| Complete recanalization | 2.35 [1.24, 4.44] | 0.009 | 1.81 [0.904, 3.63] | 0.094 |
| Partial recanalization | 1.12 [0.394, 3.20] | 0.830 | 0.727 [0.235, 2.25] | 0.581 |
| No recanalization | 1.13 [0.509, 2.52] | 0.760 | 0.775 [0.330, 1.83] | 0.560 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Covariates | Hazards Ratio (95% CI) | p Value | Adjusted Hazards Ratio (95% CI) | p Value |
| Left Ventricular Systolic Dysfunction | 3.56 [2.24, 5.66] | <0.001 | 2.49 [1.44, 4.32] | 0.001 |
| Age | 1.02 [1.00, 1.04] | 0.034 | 1.01 [0.994, 1.03] | 0.187 |
| Female Sex | 1.08 [0.677, 1.73] | 0.742 | ||
| Race | ||||
| Chinese (REF) | 0.799 | |||
| Malay | 1.15 [0.639, 2.07] | 0.642 | ||
| Indian | 0.963 [0.345, 2.69] | 0.943 | ||
| Other | 0.548 [0.133, 2.26] | 0.406 | ||
| Hypertension | 1.27 [0.721, 2.24] | 0.405 | ||
| Dyslipidemia | 2.29 [1.39, 3.76] | 0.001 | 1.41 [0.819, 2.44] | 0.214 |
| Diabetes Mellitus | 3.18 [1.98, 5.11] | <0.001 | 2.53 [1.53, 4.19] | <0.001 |
| Atrial Fibrillation | 1.86 [1.18, 2.95] | 0.008 | 1.55 [0.960, 2.51] | 0.076 |
| Ischemic Heart Disease | 2.61 [1.66, 4.11] | <0.001 | 1.35 [0.786, 2.31] | 0.278 |
| National Institutes of Health Stroke Scale on arrival | 1.00 [0.969, 1.03] | 0.995 | ||
| TOAST Classification | ||||
| 1 (REF) | 0.510 | |||
| 2 | 1.48 [0.653, 2.13] | 0.586 | ||
| 3 | 0.562 [0.185, 1.71] | 0.311 | ||
| 4 | 0.00 [0.00, 0.00] | 0.999 | ||
| 5 | 0.667 [0.283, 1.57] | 0.355 | ||
| Recanalization | ||||
| No occlusion (REF) | 0.895 | |||
| Complete recanalization | 0.754 [0.370, 1.54] | 0.436 | ||
| Partial recanalization | 0.879 [0.316, 2.45] | 0.806 | ||
| No recanalization | 0.888 [0.411, 1.92] | 0.763 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chee, R.C.H.; Lin, N.H.; Ho, J.S.Y.; Leow, A.S.T.; Li, T.Y.W.; Lee, E.C.Y.; Chan, M.Y.; Kong, W.K.F.; Yeo, T.-C.; Chai, P.; et al. Left Ventricular Ejection Fraction Association with Acute Ischemic Stroke Outcomes in Patients Undergoing Thrombolysis. J. Cardiovasc. Dev. Dis. 2023, 10, 231. https://doi.org/10.3390/jcdd10060231
Chee RCH, Lin NH, Ho JSY, Leow AST, Li TYW, Lee ECY, Chan MY, Kong WKF, Yeo T-C, Chai P, et al. Left Ventricular Ejection Fraction Association with Acute Ischemic Stroke Outcomes in Patients Undergoing Thrombolysis. Journal of Cardiovascular Development and Disease. 2023; 10(6):231. https://doi.org/10.3390/jcdd10060231
Chicago/Turabian StyleChee, Ryan C. H., Norman H. Lin, Jamie S. Y. Ho, Aloysius S. T. Leow, Tony Y. W. Li, Edward C. Y. Lee, Mark Y. Chan, William K. F. Kong, Tiong-Cheng Yeo, Ping Chai, and et al. 2023. "Left Ventricular Ejection Fraction Association with Acute Ischemic Stroke Outcomes in Patients Undergoing Thrombolysis" Journal of Cardiovascular Development and Disease 10, no. 6: 231. https://doi.org/10.3390/jcdd10060231