
Practical Guide to Interpreting Cardiac Magnetic Resonance in Patients with Cardiac Masses
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Epidemiology
3. Clinical Presentation
4. Localization
5. Clinical Pills
6. Diagnostic Imaging
7. Cardiac Magnetic Resonance
7.1. Bright Blood Imaging
7.1.1. Balanced-Steady-State Free Precession (B-SSFP) Slices of Thorax in Axial, Coronal, and Sagittal Planes
- Early localization of the mass and subsequent sequences may be targeted on it
- Panoramic view of the anatomical structures of the thorax
7.1.2. Cine Sequences
- Two-chamber (2CH SSFP): along a plane passing between the center of the mitral-tricuspid annulus and the apex of the left and right ventricles, depending on the location of the tumor.
- Four-chamber (4CH SSFP): along an image plane passing through the center of the left ventricular cavity and the right ventricular costophrenic angle
- Three-chamber (3CH SSFP): along a plane passing between the aortic and mitral annulus and the apex of the left ventricle
- Short-axis (SAX SSFP) acquisitions are acquired along an image plane perpendicular to the interventricular septum, passing through both ventricles and sometimes the atria.
- To evaluate motion and myocardial contraction
- To assess border, size, and location
- Very useful for stable anatomical relationships of the mass with myocardium (intramyocardial or pedunculated) and with adjacent structures
- To evaluate mobile masses, such as atrial myxomas or papillary valve fibroelastoma
- To reveal pericardial effusion
- Cardiac valve function and visualization of stenotic or regurgitant flow jets
7.2. Black Blood Imaging
7.2.1. T2-Weighted Triple-Inversion Recovery Images
- Short tau inversion recovery (STIR) [40]: STIR is a robust method of fat suppression. Inversion recovery (IR) is the most used method of magnetization preparation. IR depends on the fact that different tissues have different T1 characteristics. If the time between inversion and imaging (TI) is chosen carefully, the signal from a given tissue can be eliminated. STIR relies on the short T1 of fat compared with other tissues. Therefore, the fat magnetization will pass through the null point of an IR sequence before the tissue of interest. If imaging is carried out at the null point of fat, the signal from the fat will be suppressed.
- Spectral inversion recovery (SPIR): spectral-selective pulses rely on the fact that water and fat precess at slightly different frequencies (approximately 220 Hz difference at 1.5T). Therefore, a special RF pulse that only excites fat can be utilized. In SPIR, a spectrally selective 180° pulse is used to invert only the fat magnetization. The water magnetization is unchanged by the spectrally selective 180° pulse. The fat magnetization is then allowed to recover, and a TI that coincides with the null point of fat is chosen. Unlike STIR, at the onset of imaging, all the water magnetization is in the longitudinal axis, and therefore, there is no loss in SNR.
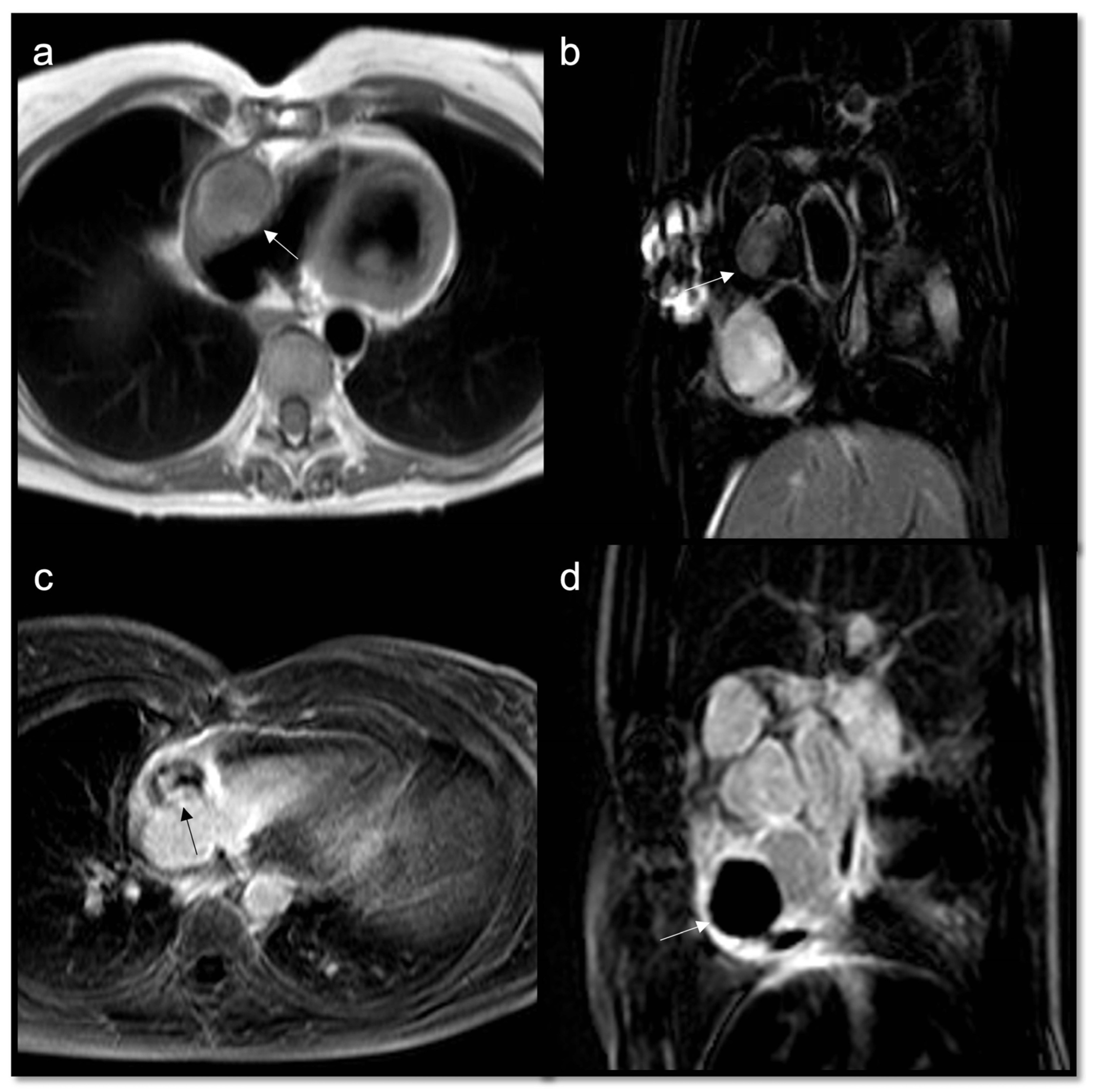
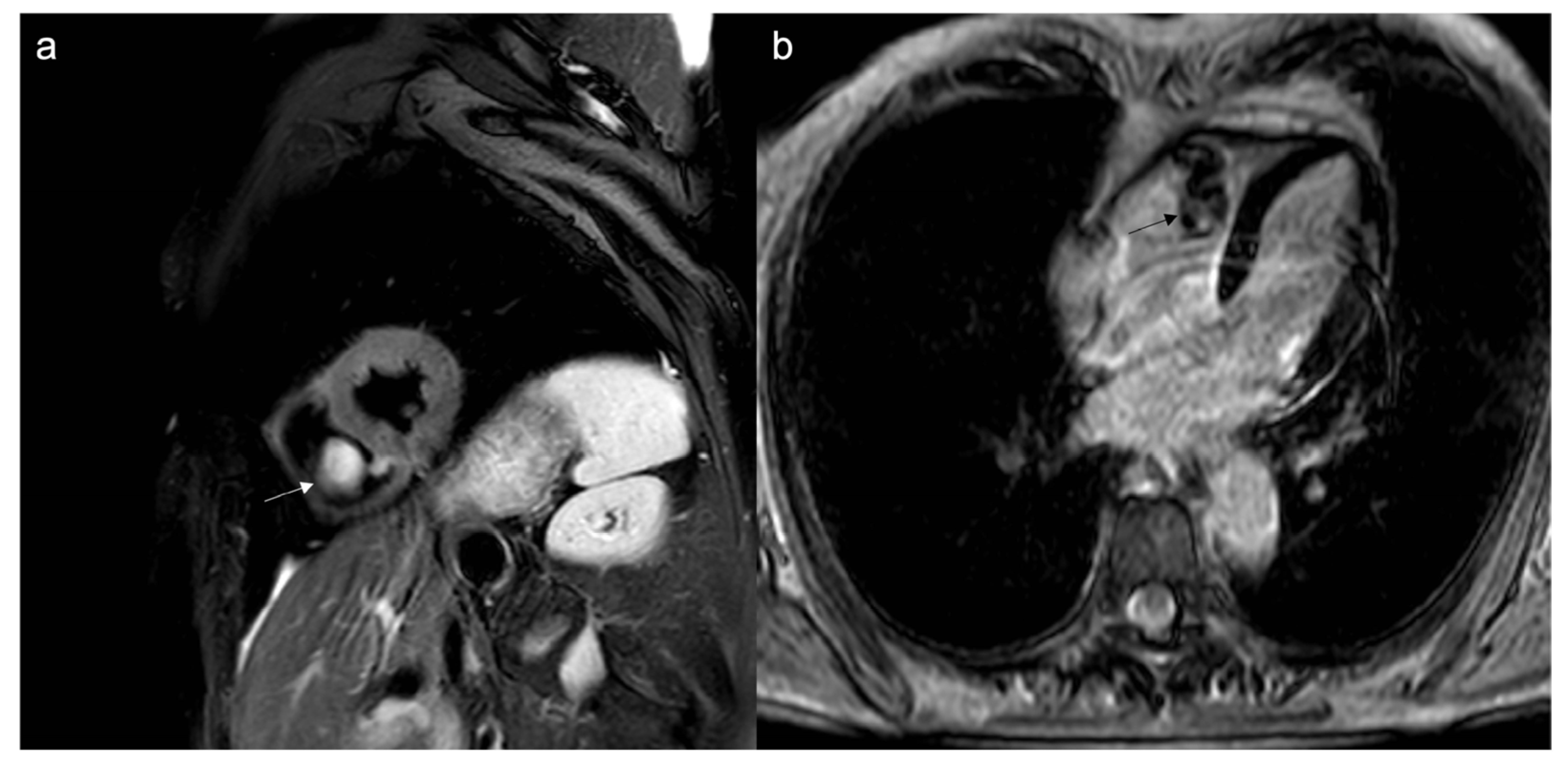
- High signal: fluid, myxomatous components
- Low signal: calcific components
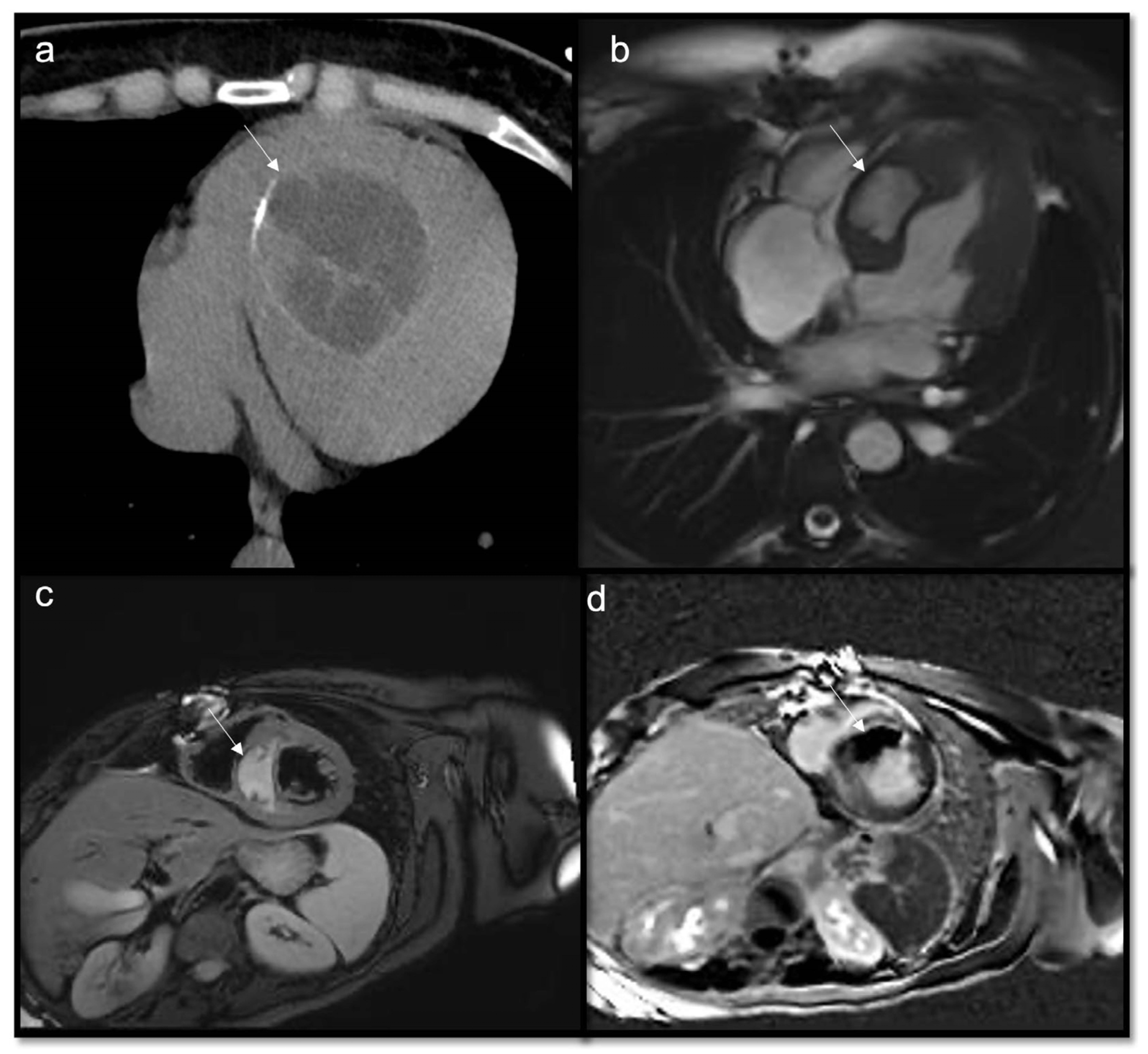
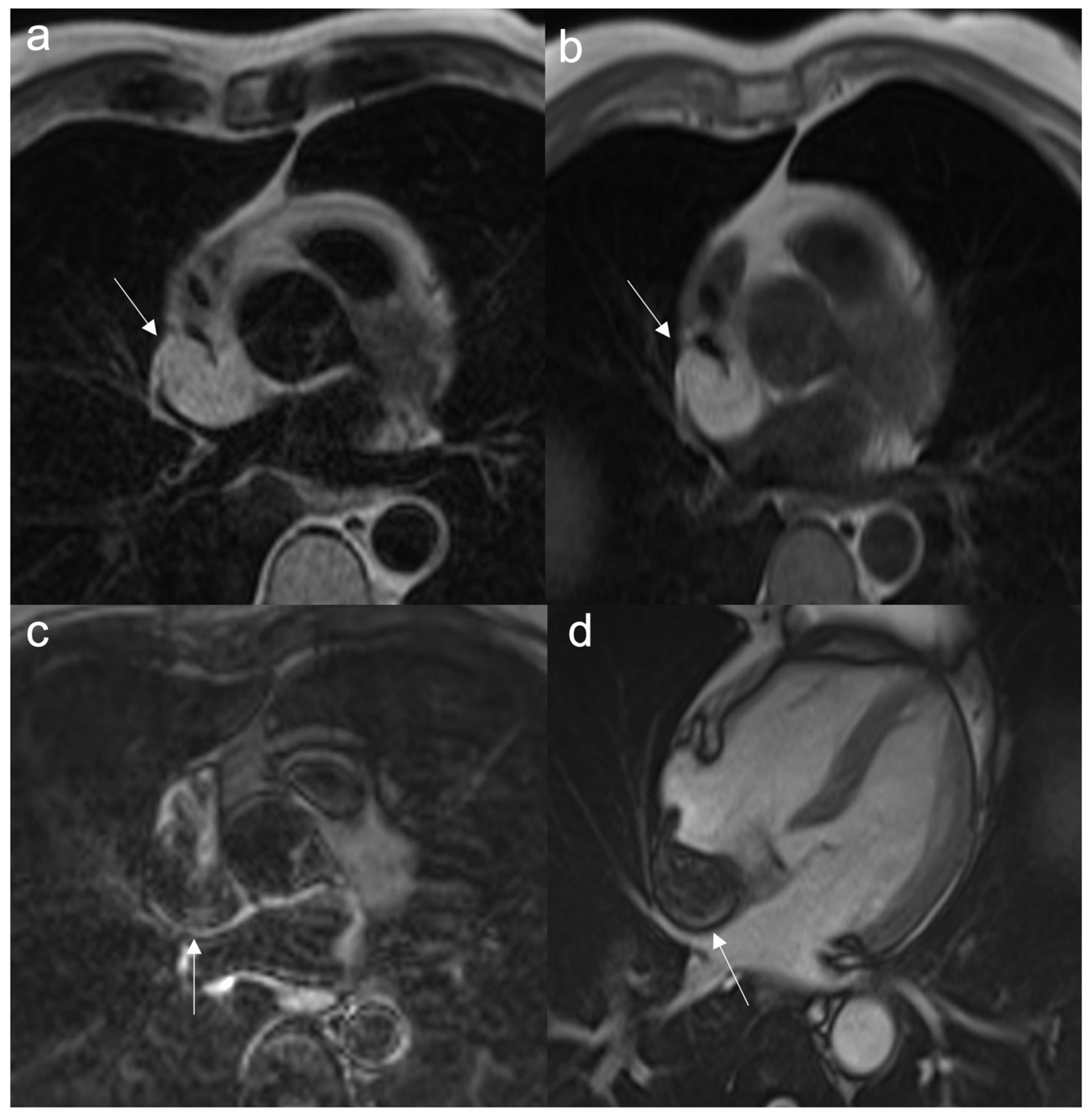
- To recognize fluid content such as a pericardial cyst or myocardial cyst (Figure 3)
- To assess for edema or necrosis in the mass.
7.2.2. T1-Weighted Double-Inversion Recovery Images
- To achieve a better anatomic definition than T2w ones
- High signal: lipid content, melanin, blood catabolites (methemoglobin)
- Low signal: indicates fibrosis
7.2.3. First-Pass Perfusion Sequences
- Assessment of vascularity
- Malignant masses often show heterogeneous enhancement; typically, angiosarcoma shows early avid enhancement as it is richly vascularized.
- Trombi due to their avascular nature appear non-enhanced.
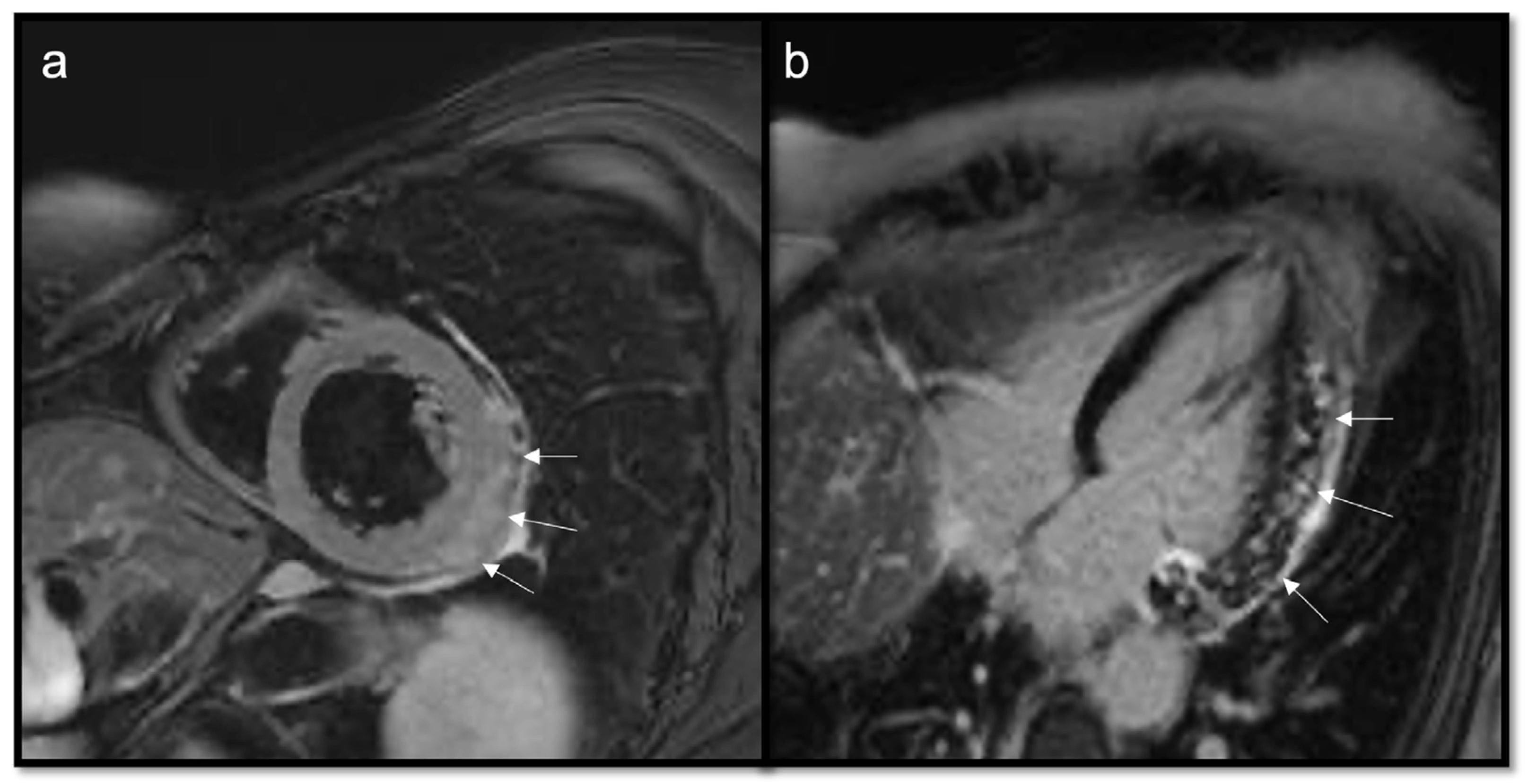
7.2.4. Early Gadolinium Enhancement (EGE)
- Organized thrombi may show peripheral enhancement on LGE images, owing to their fibrous content.
- T1w and T2w signal characteristics vary depending on the age of a thrombus. Thrombi generally showed T1 values similar to those of the normal myocardium, with a significant difference between recent (shorter T1) and old (longer T1) thrombi. The T2 relaxation times of thrombi were consistently longer than myocardial T2, regardless of their age [46]. Most of the literature reviews classify thrombi according to their age as acute, subacute, or chronic. Theoretically, at the very acute phase of their formation, thrombi are usually T1- and T2-hyperintense (short T1 and long T2) because hemoglobin is still oxygenated. In a subacute thrombus, hemoglobin is metabolized into methemoglobin. The paramagnetic effect of methemoglobin (shortening of the relaxation times) is responsible for a high T1 signal (shortening of T1). The T2 signal is generally increased (longer T2) because of water content due to red cell lysis. After a longer period, the thrombus is depleted of water, and cell debris containing methemoglobin is replaced by fibrous tissue, responsible for a decrease of signal on T1-weighted images (longer T1) and a decrease of signal on T2-weighted images (shortening of T2) [47,48].
7.2.5. Late Gadolinium Enhancement (LGE)
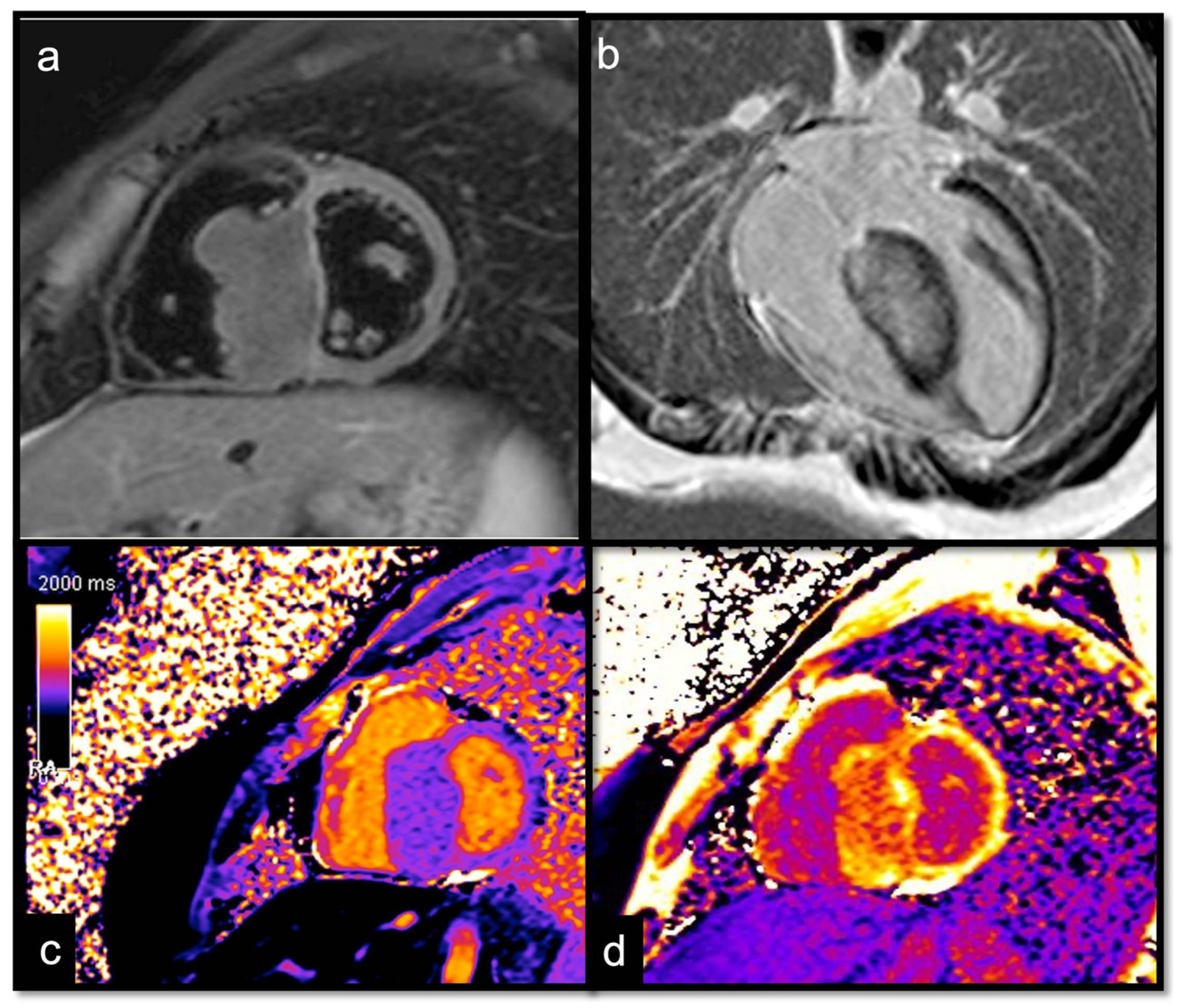
7.2.6. T1 and T2 Mapping
- Using inversion preparation
- Modified look-locker imaging (MOLLI) is the most widely used T1 measurement sequence. In 5 (3), MOLLI measurements are obtained at different TIs over 5 + 3 = 8 heartbeats with a 3-beat recovery period in between, while in the post-contrast sequences, a 4 (3) 3 scheme is used due to shortener T1 times.
- Shortened MOLLI (SHMOLLI) is used for patients who cannot hold their breaths for more than 20 s; shortened MOLLI (shMOLLI) using a 5–1–1 scheme is available.
- Using saturation preparation
- Saturation-recovery single-shot acquisition (SASHA) recovery methods use 90° instead of 180° pulses, which have the advantage of removing magnetization memory from prior cycles and allowing a direct estimate of THE true T1 to be made. Disadvantages include lower SNR and more artifacts [55].
- Using a combination of inversion and saturation
- Saturation-pulse prepared heart-rate independent inversion-recovery (SAPPHIRE) uses a hybrid of saturation and inversion pulses to improve the precision of the saturation-recovery approach while maintaining accuracy.
- T2 turbo spin multi-echo (T2-TSE)
- T2 prepared steady-state free precession (T2p-SSFP)
- T2 gradient spin-echo mapping sequences (T2-GraSE) [57]
- Short T1/short T2 (as compared with the myocardium) for calcifications
- Short T1/long T2 for melanoma or lipomas and lipomatosis [64]
- Long T1/long T2 for most tumors, whether benign or malignant, with different degrees in particular for the T1 (close to the myocardium for rhabdomyoma, long or very long for myxomas [65] and fibroelastomas)
- T1 mapping allows for highlighting the difference between recent (<1 week) and old thrombi (>1 month), as recent thrombi have a significantly shorter T1.
7.2.7. Extracellular Volume
7.2.8. Phase Contrast (PhC) Sequences
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Basso, C.; Rizzo, S.; Valente, M.; Thiene, G. Cardiac Masses and Tumours. Heart 2016, 102, 1230–1245. [Google Scholar] [CrossRef] [PubMed]
- Tyebally, S.; Chen, D.; Bhattacharyya, S.; Mughrabi, A.; Hussain, Z.; Manisty, C.; Westwood, M.; Ghosh, A.K.; Guha, A. Cardiac Tumors: JACC CardioOncology State-of-the-Art Review. JACC CardioOncol. 2020, 2, 293–311. [Google Scholar] [CrossRef] [PubMed]
- Hoey, E.; Ganeshan, A.; Nader, K.; Randhawa, K.; Watkin, R. Cardiac Neoplasms and Pseudotumors: Imaging Findings on Multidetector CT Angiography. Diagn. Interv. Radiol. 2012, 18, 67–77. [Google Scholar] [CrossRef]
- Poterucha, T.J.; Kochav, J.; O’Connor, D.S.; Rosner, G.F. Cardiac Tumors: Clinical Presentation, Diagnosis, and Management. Curr. Treat. Options Oncol. 2019, 20, 66. [Google Scholar] [CrossRef]
- Lau, C.; Leonard, J.R.; Schwann, A.N.; Soletti, G.; Abouarab, A.A.; Munjal, M.; Gaudino, M.; Girardi, L.N. A 20-Year Experience with Resection of Primary Cardiac Tumors and Metastatic Tumors of the Heart. Ann. Thorac. Surg. 2019, 107, 1126–1131. [Google Scholar] [CrossRef]
- Aldea, G.S.; Verrier, E.D. Cardiac Tumors. Oper. Card. Surg. Fifth Ed. 2004, 2011, 525–531. [Google Scholar] [CrossRef]
- Lanzoni, L.; Bonapace, S.; Dugo, C.; Chiampan, A.; Anselmi, A.; Ghiselli, L.; Molon, G. Cardiac Masses and Contrast Echocardiography. Eur. Heart J. Cardiovasc. Imaging 2022, 23 (Suppl. S1), jeab289.296. [Google Scholar] [CrossRef]
- Kassop, D.; Donovan, M.S.; Cheezum, M.K.; Nguyen, B.T.; Gambill, N.B.; Blankstein, R.; Villines, T.C. Cardiac Masses on Cardiac CT: A Review. Curr. Cardiovasc. Imaging Rep. 2014, 7, 9281. [Google Scholar] [CrossRef]
- Gatti, M.; D’Angelo, T.; Muscogiuri, G.; Dell’aversana, S.; Andreis, A.; Carisio, A.; Darvizeh, F.; Tore, D.; Pontone, G.; Faletti, R. Cardiovascular Magnetic Resonance of Cardiac Tumors and Masses. World J. Cardiol. 2021, 13, 628–649. [Google Scholar] [CrossRef]
- Yin, H.; Mao, W.; Tan, H.; Zhu, N.; Wan, Q.; Shi, J.; Qiu, L.; Xiu, Y.; Luo, R.; Yu, H.; et al. Role of 18F-FDG PET/CT Imaging in Cardiac and Pericardial Masses. J. Nucl. Cardiol. 2022, 29, 1293–1303. [Google Scholar] [CrossRef]
- Rahouma, M.; Arisha, M.J.; Elmously, A.; El-Sayed Ahmed, M.M.; Spadaccio, C.; Mehta, K.; Baudo, M.; Kamel, M.; Mansor, E.; Ruan, Y.; et al. Cardiac Tumors Prevalence and Mortality: A Systematic Review and Meta-Analysis. Int. J. Surg. 2020, 76, 178–189. [Google Scholar] [CrossRef] [PubMed]
- Becker, A.E. Primary Heart Tumors in the Pediatric Age Group: A Review of Salient Pathologic Features Relevant for Clinicians. Pediatr. Cardiol. 2000, 21, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, N.; Cheezum, M.K.; Aghayev, A.; Padera, R.; Vita, T.; Steigner, M.; Hulten, E.; Bittencourt, M.S.; Dorbala, S.; di Carli, M.F.; et al. Assessment of Cardiac Masses by Cardiac Magnetic Resonance Imaging: Histological Correlation and Clinical Outcomes. J. Am. Heart Assoc. 2019, 8, e007829. [Google Scholar] [CrossRef] [PubMed]
- Aggeli, C.; Dimitroglou, Y.; Raftopoulos, L.; Sarri, G.; Mavrogeni, S.; Wong, J.; Tsiamis, E.; Tsioufis, C. Cardiac Masses: The Role of Cardiovascular Imaging in the Differential Diagnosis. Diagnostics 2020, 10, 1088. [Google Scholar] [CrossRef] [PubMed]
- Zitzelsberger, T.; Eigentler, T.K.; Krumm, P.; Nikolaou, K.; Garbe, C.; Gawaz, M.; Klumpp, B. Imaging Characteristics of Cardiac Metastases in Patients with Malignant Melanoma. Cancer Imaging 2017, 17, 19. [Google Scholar] [CrossRef] [PubMed]
- Burazor, I.; Aviel-Ronen, S.; Imazio, M.; Goitein, O.; Perelman, M.; Shelestovich, N.; Radovanovic, N.; Kanjuh, V.; Barshack, I.; Adler, Y. Metastatic Cardiac Tumors: From Clinical Presentation through Diagnosis to Treatment. BMC Cancer 2018, 18, 202. [Google Scholar] [CrossRef]
- Malik, S.B.; Kwan, D.; Shah, A.B.; Hsu, J.Y. The Right Atrium: Gateway to the Heart—Anatomic and Pathologic Imaging Findings. Radiographics 2015, 35, 14–31. [Google Scholar] [CrossRef]
- Penha, J.G.; Zorzanelli, L.; Barbosa-Lopes, A.A.; Aiello, V.D.; Carvalho, V.O.; Caneo, L.F.; Riso, A.d.A.; Tanamati, C.; Atik, E.; Jatene, M.B. Heart Neoplasms in Children: Retrospective Analysis. Arq. Bras. Cardiol. 2013, 100, 120–126. [Google Scholar] [CrossRef]
- Grebenc, M.L.; Rosado-De-Christenson, M.L.; Green, C.E.; Burke, A.P.; Galvin, J.R. From the Archives of the AFIP: Cardiac Myxoma: Imaging Features in 83 Patients. Radiographics 2002, 22, 673–689. [Google Scholar] [CrossRef]
- Pradella, S.; Grazzini, G.; Letteriello, M.; De Amicis, C.; Grassi, R.; Maggialetti, N.; Carbone, M.; Palumbo, P.; Carotti, M.; Di Cesare, E.; et al. Masses in Right Side of the Heart: Spectrum of Imaging Findings. Acta Biomed. 2020, 91, 60–79. [Google Scholar] [CrossRef]
- Buckley, O.; Madan, R.; Kwong, R.; Rybicki, F.J.; Hunsaker, A. Cardiac Masses, Part 1: Imaging Strategies and Technical Considerations. AJR Am. J. Roentgenol. 2011, 197, 837–841. [Google Scholar] [CrossRef] [PubMed]
- Mankad, R.; Herrmann, J. Cardiac Tumors: Echo Assessment. Echo Res. Pract. 2016, 3, R65–R77. [Google Scholar] [CrossRef] [PubMed]
- Nomoto, N.; Tani, T.; Konda, T.; Kim, K.; Kitai, T.; Ota, M.; Kaji, S.; Imai, Y.; Okada, Y.; Furukawa, Y. Primary and Metastatic Cardiac Tumors: Echocardiographic Diagnosis, Treatment and Prognosis in a 15-Years Single Center Study. J. Cardiothorac. Surg. 2017, 12, 103. [Google Scholar] [CrossRef] [PubMed]
- Obeid, A.I.; Al Mudamgha, A.; Smulyan, H. Diagnosis of Right Atrial Mass Lesions by Transesophageal and Transthoracic Echocardiography. Chest 1993, 103, 1447–1451. [Google Scholar] [CrossRef]
- Murugan, M.; Gulati, G. MR and CT Imaging Spectrum of Right-Sided Cardiac Masses: A Pictorial Essay. Nepal. J. Radiol. 2013, 2, 96–110. [Google Scholar] [CrossRef]
- Esposito, A.; De Cobelli, F.; Ironi, G.; Marra, P.; Canu, T.; Mellone, R.; Del Maschio, A. CMR in the Assessment of Cardiac Masses: Primary Malignant Tumors. JACC Cardiovasc. Imaging 2014, 7, 1057–1061. [Google Scholar] [CrossRef]
- Secinaro, A.; Ait-Ali, L.; Curione, D.; Clemente, A.; Gaeta, A.; Giovagnoni, A.; Alaimo, A.; Esposito, A.; Tchana, B.; Sandrini, C.; et al. Recommendations for Cardiovascular Magnetic Resonance and Computed Tomography in Congenital Heart Disease: A Consensus Paper from the CMR/CCT Working Group of the Italian Society of Pediatric Cardiology (SICP) and the Italian College of Cardiac Radiology Endorsed by the Italian Society of Medical and Interventional Radiology (SIRM) Part I. Radiol. Med. 2022, 127, 788–802. [Google Scholar] [CrossRef]
- Palumbo, P.; Cannizzaro, E.; Palumbo, M.M.; Di Cesare, A.; Bruno, F.; Acanfora, C.; Arceri, A.; Evangelista, L.; Arrigoni, F.; Grassi, F.; et al. Heart Failure and Cardiomyopathies: CT and MR from Basics to Advanced Imaging. Diagnostics 2022, 12, 2298. [Google Scholar] [CrossRef]
- Arnold, J.R.; McCann, G.P. Cardiovascular Magnetic Resonance: Applications and Practical Considerations for the General Cardiologist. Heart 2019, 106, 174–181. [Google Scholar] [CrossRef]
- Lichtenberger, J.P.; Dulberger, A.R.; Gonzales, P.E.; Bueno, J.; Carter, B.W. MR Imaging of Cardiac Masses. Top. Magn. Reson. Imaging 2018, 27, 103–111. [Google Scholar] [CrossRef]
- Grebenc, M.L.; Rosado De Christenson, M.L.; Burke, A.P.; Green, C.E.; Galvin, J.R. Primary Cardiac and Pericardial Neoplasms: Radiologic-Pathologic Correlation. Radiographics 2000, 20, 1073–1103. [Google Scholar] [CrossRef] [PubMed]
- Pontone, G.; Di Cesare, E.; Castelletti, S.; De Cobelli, F.; De Lazzari, M.; Esposito, A.; Focardi, M.; Di Renzi, P.; Indolfi, C.; Lanzillo, C.; et al. Appropriate Use Criteria for Cardiovascular Magnetic Resonance Imaging (CMR): SIC—SIRM Position Paper Part 1 (Ischemic and Congenital Heart Diseases, Cardio-Oncology, Cardiac Masses and Heart Transplant). Radiol. Med. 2021, 126, 365–379. [Google Scholar] [CrossRef] [PubMed]
- Esposito, A.; Francone, M.; Andreini, D.; Buffa, V.; Cademartiri, F.; Carbone, I.; Clemente, A.; Guaricci, A.I.; Guglielmo, M.; Indolfi, C.; et al. SIRM-SIC appropriateness criteria for the use of Cardiac Computed Tomography. Part 1: Congenital heart diseases, primary prevention, risk assessment before surgery, suspected CAD in symptomatic patients, plaque and epicardial adipose tissue characterization, and functional assessment of stenosis. Radiol. Med. 2021, 126, 1236–1248. [Google Scholar] [CrossRef] [PubMed]
- Krumm, P.; Mangold, S.; Gatidis, S.; Nikolaou, K.; Nensa, F.; Bamberg, F.; la Fougère, C. Clinical Use of Cardiac PET/MRI: Current State-of-the-Art and Potential Future Applications. Jpn. J. Radiol. 2018, 36, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.T.; Fox, J.; Perez Johnston, R.; Kim, J.; Brouwer, L.R.; Grizzard, J.; Kim, R.J.; Matasar, M.; Shia, J.; Moskowitz, C.S.; et al. Late Gadolinium Enhancement Cardiac Magnetic Resonance Tissue Characterization for Cancer-Associated Cardiac Masses: Metabolic and Prognostic Manifestations in Relation to Whole-Body Positron Emission Tomography. J. Am. Heart Assoc. 2019, 8, e011709. [Google Scholar] [CrossRef] [PubMed]
- Martineau, P.; Dilsizian, V.; Pelletier-Galarneau, M. Incremental Value of FDG-PET in the Evaluation of Cardiac Masses. Curr. Cardiol. Rep. 2021, 23, 78. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Singh, A.; Deshmukh, A.; Kumar, S. Cardiac MRI for the evaluation of cardiac neoplasms. Clin. Radiol. 2020, 75, 241–253. [Google Scholar] [CrossRef]
- Liddy, S.; McQuade, C.; Walsh, K.P.; Loo, B.; Buckley, O. The Assessment of Cardiac Masses by Cardiac CT and CMR Including Pre-op 3D Reconstruction and Planning. Curr. Cardiol. Rep. 2019, 21, 103. [Google Scholar] [CrossRef]
- Li, X.; Chen, Y.; Liu, J.; Xu, L.; Li, Y.; Liu, D.; Sun, Z.; Wen, Z. Cardiac magnetic resonance imaging of primary cardiac tumors. Quant. Imaging Med. Surg. 2020, 10, 294–313. [Google Scholar] [CrossRef]
- Araoz, P.A.; Mulvagh, S.L.; Tazelaar, H.D.; Julsrud, P.R.; Breen, J.F. CT and MR Imaging of Benign Primary Cardiac Neoplasms with Echocardiographic Correlation. Radiographics 2000, 20, 1303–1319. [Google Scholar] [CrossRef]
- Araoz, P.A.; Eklund, H.E.; Welch, T.J.; Breen, J.F. CT and MR Imaging of Primary Cardiac Malignancies. Radiographics 1999, 19, 1421–1434. [Google Scholar] [CrossRef]
- Siripornpitak, S.; Higgins, C.B. MRI of Primary Malignant Cardiovascular Tumors. J. Comput. Assist. Tomogr. 1997, 21, 462–466. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, U.; Globits, S.; Schima, W.; Loewe, C.; Puig, S.; Oberhuber, G.; Frank, H. Usefulness of Magnetic Resonance Imaging of Cardiac and Paracardiac Masses. Am. J. Cardiol. 2003, 92, 890–895. [Google Scholar] [CrossRef] [PubMed]
- Simonetti, O.P.; Finn, J.P.; White, R.D.; Laub, G.; Henry, D.A. “Black Blood” T2-Weighted Inversion-Recovery MR Imaging of the Heart. Radiology 1996, 199, 49–57. [Google Scholar] [CrossRef]
- Grazzini, G.; Pradella, S.; Miele, V. Incidental Identification of Right Atrial Mass. Heart 2020, 106, 1502–1534. [Google Scholar] [CrossRef]
- Caspar, T.; el Ghannudi, S.; Ohana, M.; Labani, A.; Lawson, A.; Ohlmann, P.; Morel, O.; de Mathelin, M.; Roy, C.; Gangi, A.; et al. Magnetic Resonance Evaluation of Cardiac Thrombi and Masses by T1 and T2 Mapping: An Observational Study. Int. J. Cardiovasc. Imaging 2017, 33, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Corti, R.; Osende, J.I.; Fayad, Z.A.; Fallon, J.T.; Fuster, V.; Mizsei, G.; Dickstein, E.; Drayer, B.; Badimon, J.J. In Vivo Noninvasive Detection and Age Definition of Arterial Thrombus by MRI. J. Am. Coll. Cardiol. 2002, 39, 1366–1373. [Google Scholar] [CrossRef] [PubMed]
- Craig Blackmore, C.; Francis, C.W.; Bryant, R.G.; Brenner, B.; Marder, V.J. Magnetic Resonance Imaging of Blood and Clots in Vitro. Investig. Radiol. 1990, 25, 1316–1324. [Google Scholar] [CrossRef]
- Craft, J.; Li, Y.; Bhatti, S.; Cao, J.J. How to Do Left Atrial Late Gadolinium Enhancement: A Review. Radiol. Med. 2021, 126, 1159–1169. [Google Scholar] [CrossRef]
- Broadbent, D.; Kidambi, A.; Biglands, J.; Herzog, B.A.; Greenwood, J.P.; Plein, S. Cardiovascular Magnetic Resonance Physics for Clinicians Pocket Guide Series Editors. Available online: https://www.escardio.org/static-file/Escardio/Subspecialty/EACVI/CMR%20Physics%20Pocket%20Guide%20iBook%20v1.0.pdf (accessed on 15 March 2023).
- Palumbo, P.; Masedu, F.; De Cataldo, C.; Cannizzaro, E.; Bruno, F.; Pradella, S.; Arrigoni, F.; Valenti, M.; Splendiani, A.; Barile, A.; et al. Real-World Clinical Validity of Cardiac Magnetic Resonance Tissue Tracking in Primitive Hypertrophic Cardiomyopathy. Radiol. Med. 2021, 126, 1532–1543. [Google Scholar] [CrossRef]
- Pradella, S.; Mazzoni, L.N.; Letteriello, M.; Tortoli, P.; Bettarini, S.; De Amicis, C.; Grazzini, G.; Busoni, S.; Palumbo, P.; Belli, G.; et al. FLORA Software: Semi-Automatic LGE-CMR Analysis Tool for Cardiac Lesions Identification and Characterization. Radiol. Med. 2022, 127, 589–601. [Google Scholar] [CrossRef] [PubMed]
- Russo, V.; Lovato, L.; Ligabue, G. Cardiac MRI: Technical Basis. Radiol. Med. 2020, 125, 1040–1055. [Google Scholar] [CrossRef] [PubMed]
- Pradella, S.; Grazzini, G.; Miele, V. Mitral Valve Prolapse Imaging: The Role of Tissue Characterization. Quant. Imaging Med. Surg. 2020, 10, 2396–2400. [Google Scholar] [CrossRef] [PubMed]
- Roujol, S.; Weingärtner, S.; Foppa, M.; Chow, K.; Kawaji, K.; Ngo, L.H.; Kellman, P.; Manning, W.J.; Thompson, R.B.; Nezafat, R. Accuracy, Precision, and Reproducibility of Four T1 Mapping Sequences: A Head-to-Head Comparison of MOLLI, ShMOLLI, SASHA, and SAPPHIRE. Radiology 2014, 272, 683–689. [Google Scholar] [CrossRef]
- Zhao, L.; Li, S.; Ma, X.; Greiser, A.; Zhang, T.; An, J.; Bai, R.; Dong, J.; Fan, Z. Systolic MOLLI T1 Mapping with Heart-Rate-Dependent Pulse Sequence Sampling Scheme Is Feasible in Patients with Atrial Fibrillation. J. Cardiovasc. Magn. Reason. 2016, 18, 13. [Google Scholar] [CrossRef]
- Sprinkart, A.M.; Luetkens, J.A.; Träber, F.; Doerner, J.; Gieseke, J.; Schnackenburg, B.; Schmitz, G.; Thomas, D.; Homsi, R.; Block, W.; et al. Gradient Spin Echo (GraSE) Imaging for Fast Myocardial T2 Mapping. J. Cardiovasc. Magn. Reson. 2015, 17, 12. [Google Scholar] [CrossRef]
- Messroghli, D.R.; Moon, J.C.; Ferreira, V.M.; Grosse-Wortmann, L.; He, T.; Kellman, P.; Mascherbauer, J.; Nezafat, R.; Salerno, M.; Schelbert, E.B.; et al. Clinical Recommendations for Cardiovascular Magnetic Resonance Mapping of T1, T2, T2* and Extracellular Volume: A Consensus Statement by the Society for Cardiovascular Magnetic Resonance (SCMR) Endorsed by the European Association for Cardiovascular Imaging (EACVI). J. Cardiovasc. Magn. Reason. 2017, 19, 75. [Google Scholar] [CrossRef]
- Baeßler, B.; Schaarschmidt, F.; Stehning, C.; Schnackenburg, B.; Maintz, D.; Bunck, A.C. A Systematic Evaluation of Three Different Cardiac T2-Mapping Sequences at 1.5 and 3T in Healthy Volunteers. Eur. J. Radiol. 2015, 84, 2161–2170. [Google Scholar] [CrossRef]
- Ferreira, V.M.; Piechnik, S.K.; Robson, M.D.; Neubauer, S.; Karamitsos, T.D. Myocardial Tissue Characterization by Magnetic Resonance Imaging: Novel Applications of T1 and T2 Mapping. J. Thorac. Imaging 2014, 29, 147–154. [Google Scholar] [CrossRef]
- Reiter, U.; Reiter, C.; Kräuter, C.; Fuchsjäger, M.; Reiter, G. Cardiac Magnetic Resonance T1 Mapping. Part 2: Diagnostic Potential and Applications. Eur. J. Radiol. 2018, 109, 235–247. [Google Scholar] [CrossRef]
- Reiter, G.; Reiter, C.; Kräuter, C.; Fuchsjäger, M.; Reiter, U. Cardiac Magnetic Resonance T1 Mapping. Part 1: Aspects of Acquisition and Evaluation. Eur. J. Radiol. 2018, 109, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Pradella, S.; Grazzini, G.; Brandani, M.; Calistri, L.; Nardi, C.; Mori, F.; Miele, V.; Colagrande, S. Cardiac Magnetic Resonance in Patients with Mitral Valve Prolapse: Focus on Late Gadolinium Enhancement and T1 Mapping. Eur. Radiol. 2019, 29, 1546–1554. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, V.M.; Holloway, C.J.; Piechnik, S.K.; Karamitsos, T.D.; Neubauer, S. Is It Really Fat? Ask a T1-Map. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 1060. [Google Scholar] [CrossRef] [PubMed]
- Kübler, D.; Gräfe, M.; Schnackenburg, B.; Knosalla, C.; Wassilew, K.; Hassel, J.H.; Ivanitzkaja, E.; Messroghli, D.; Fleck, E.; Kelle, S. T1 and T2 Mapping for Tissue Characterization of Cardiac Myxoma. Int. J. Cardiol. 2013, 169, e17–e20. [Google Scholar] [CrossRef]
- Treibel, T.A.; Fontana, M.; Maestrini, V.; Castelletti, S.; Rosmini, S.; Simpson, J.; Nasis, A.; Bhuva, A.N.; Bulluck, H.; Abdel-Gadir, A.; et al. Automatic Measurement of the Myocardial Interstitium: Synthetic Extracellular Volume Quantification Without Hematocrit Sampling. JACC Cardiovasc. Imaging 2016, 9, 54–63. [Google Scholar] [CrossRef]
- Haaf, P.; Garg, P.; Messroghli, D.R.; Broadbent, D.A.; Greenwood, J.P.; Plein, S. Cardiac T1 Mapping and Extracellular Volume (ECV) in Clinical Practice: A Comprehensive Review. J. Cardiovasc. Magn. Reason. 2016, 18, 89. [Google Scholar] [CrossRef]
- Moon, J.C.; Messroghli, D.R.; Kellman, P.; Piechnik, S.K.; Robson, M.D.; Ugander, M.; Gatehouse, P.D.; Arai, A.E.; Friedrich, M.G.; Neubauer, S.; et al. Myocardial T1 Mapping and Extracellular Volume Quantification: A Society for Cardiovascular Magnetic Resonance (SCMR) and CMR Working Group of the European Society of Cardiology Consensus Statement. J. Cardiovasc. Magn. Reason. 2013, 15, 92. [Google Scholar] [CrossRef]
- Palmisano, A.; Darvizeh, F.; Cundari, G.; Rovere, G.; Ferrandino, G.; Nicoletti, V.; Cilia, F.; De Vizio, S.; Palumbo, R.; Esposito, A.; et al. Advanced cardiac imaging in athlete’s heart: Unravelling the grey zone between physiologic adaptation and pathology. Radiol. Med. 2021, 126, 1518–1531. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tumor in Order of Frequency | Steady-State Free Precession | T2W | Fat Sat | T1W | First-Pass | LGE |
|---|---|---|---|---|---|---|
| Benign | ||||||
| Mixoma | mobile, pedunculated | hyper | - | iso | + | + heterogeneous |
| Fibroma | ipo | - | iso | - | + homogeneous | |
| Lipoma | chemical shift dark rim | hyper | signal loss | hyper | - | none |
| Hemangioma | hyper | hyper | - | iso | + | + homogeneous |
| Malign | ||||||
| Metastases | heterogeneous | iso-hyper | - | iso, ipo, or hyper (melanin, blood) | + | + |
| Angiosarcoma | heterogeneous iso | heterogeneous hyper | - | heterogeneous hyper | ++ avid “sunray” aspect | ++ heterogeneous |
| Lymphoma | heterogeneous iso | slightly hyper | - | iso | + | + heterogeneous |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grazzini, G.; Pradella, S.; Rossi, A.; Basile, R.P.; Ruggieri, M.; Galli, D.; Palmisano, A.; Palumbo, P.; Esposito, A.; Miele, V. Practical Guide to Interpreting Cardiac Magnetic Resonance in Patients with Cardiac Masses. J. Cardiovasc. Dev. Dis. 2023, 10, 229. https://doi.org/10.3390/jcdd10060229
Grazzini G, Pradella S, Rossi A, Basile RP, Ruggieri M, Galli D, Palmisano A, Palumbo P, Esposito A, Miele V. Practical Guide to Interpreting Cardiac Magnetic Resonance in Patients with Cardiac Masses. Journal of Cardiovascular Development and Disease. 2023; 10(6):229. https://doi.org/10.3390/jcdd10060229
Chicago/Turabian StyleGrazzini, Giulia, Silvia Pradella, Alice Rossi, Rocco Pio Basile, Matteo Ruggieri, Daniele Galli, Anna Palmisano, Pierpaolo Palumbo, Antonio Esposito, and Vittorio Miele. 2023. "Practical Guide to Interpreting Cardiac Magnetic Resonance in Patients with Cardiac Masses" Journal of Cardiovascular Development and Disease 10, no. 6: 229. https://doi.org/10.3390/jcdd10060229