
Moderator Band and Ventricular Tachycardia: Structural or Functional Substrate?

 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Anatomy of the Moderator Band
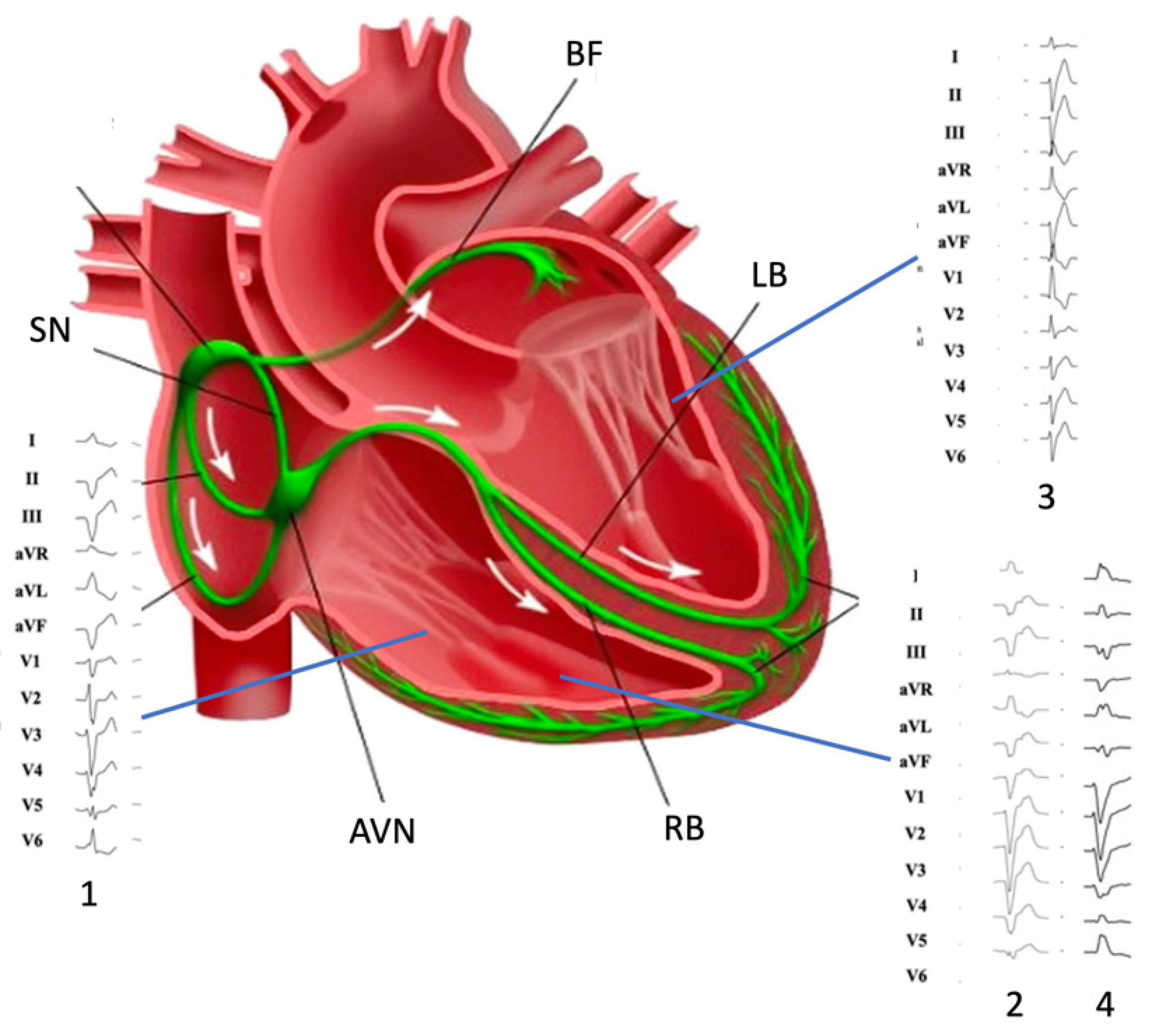
3. Electrical Properties of the Moderator Band
4. Moderator Band-Related Arrhythmias
4.1. Arrhythmogenic Mechanisms
4.2. Right Purkinje Network Arrhythmias: In Addition to the Moderator Band
5. Diagnostic of Moderator Band Related Tachycardia
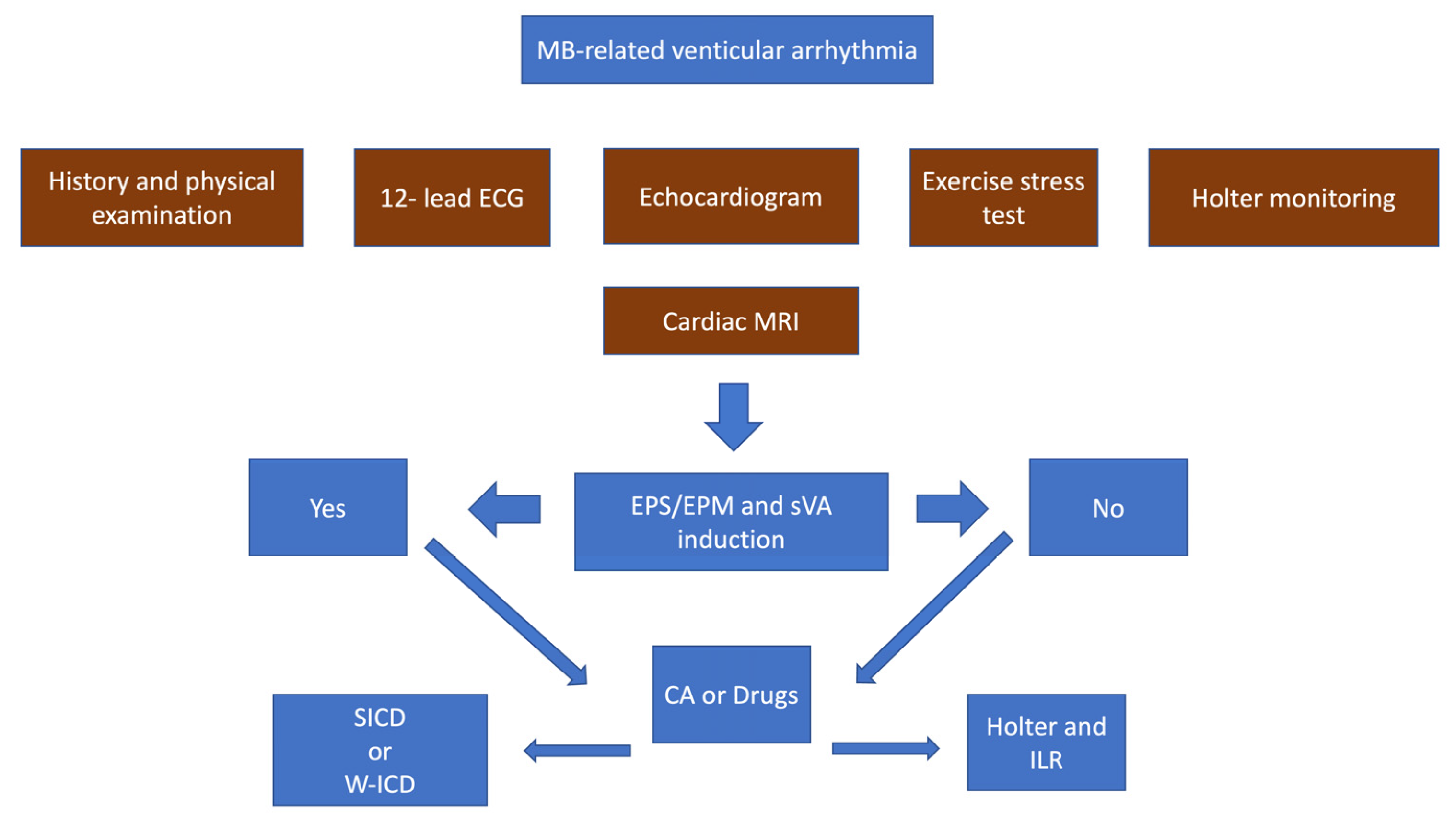
5.1. Initial Evaluation
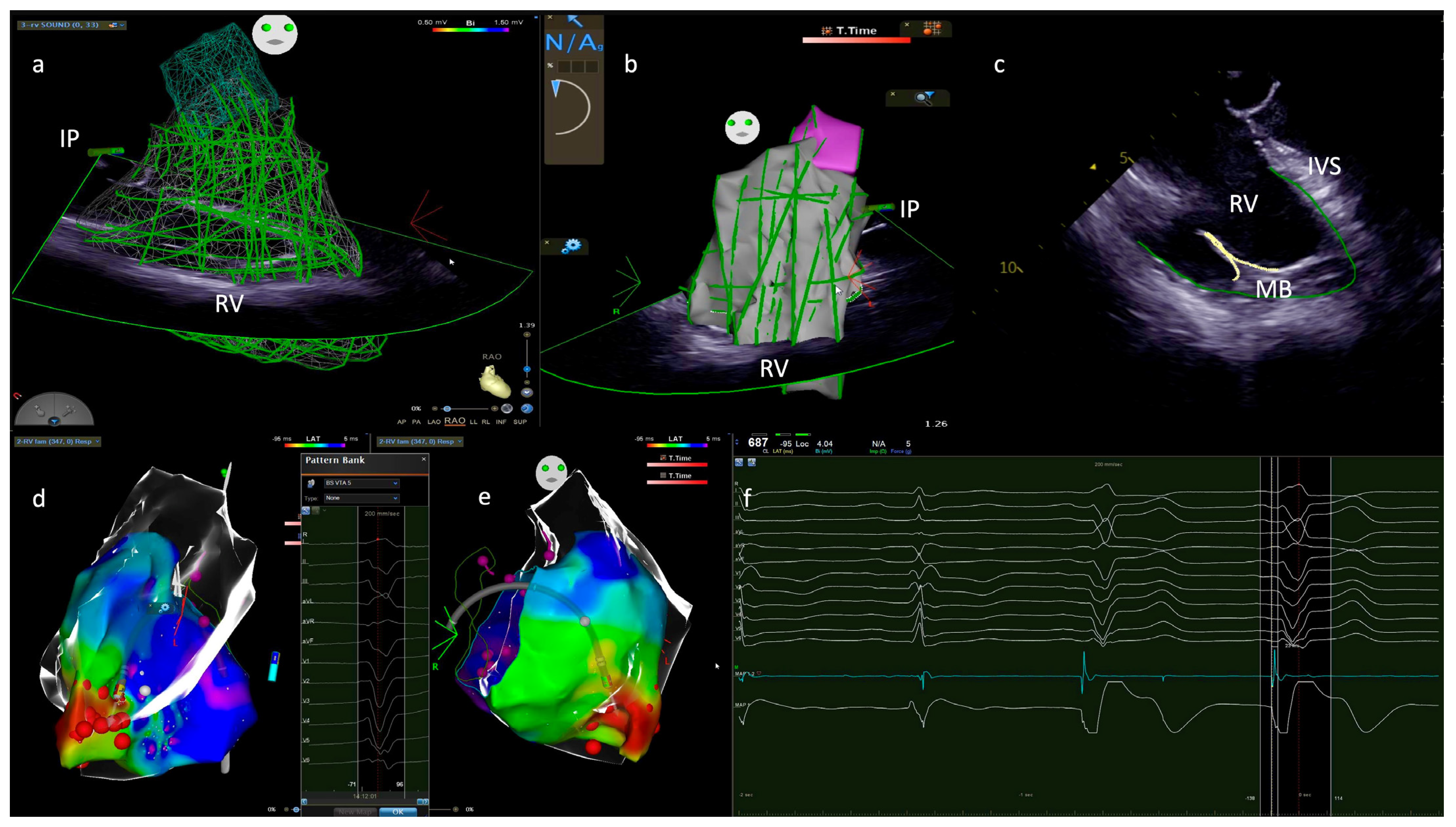
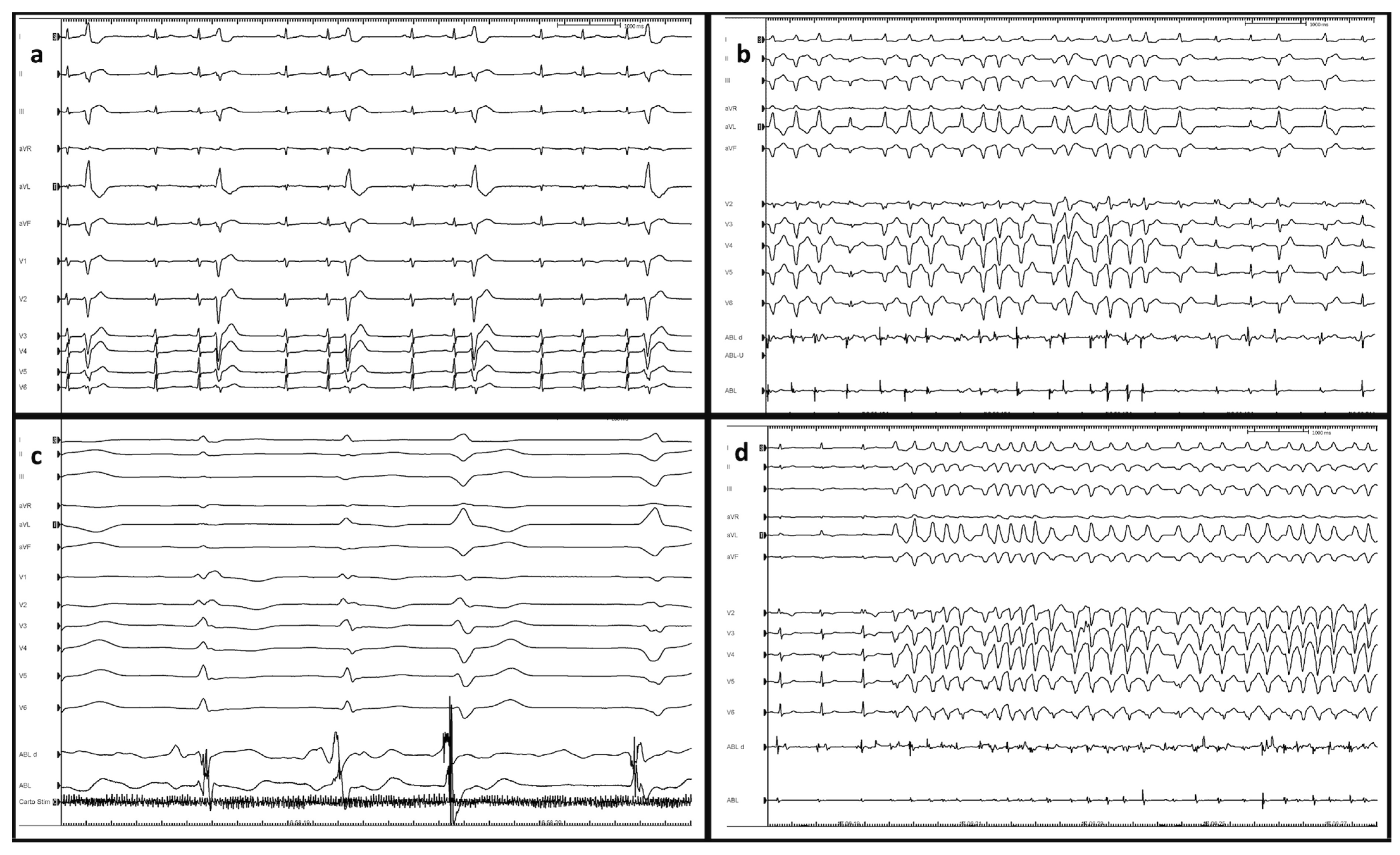
5.2. Diagnostic Tests
6. Management of Moderator-Band Ventricular Tachycardias
6.1. Ablation Targets
6.2. Pharmacological Therapy
6.3. Device Therapy
6.4. Sports Eligibility and Risk Stratification
6.5. Follow-Up
7. Conclusions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Loukas, M.; Klaassen, Z.; Tubbs, R.S.; Derderian, T.; Paling, D.; Chow, D.; Patel, S.; Anderson, R.H. Anatomical observations of the moderator band. Clin. Anat. 2010, 23, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Bojsen-Moller, F.; Tranum-Jensen, J. On nerves and nerve endings in the conducting sysetm of the moderator band (septomarginal trabecula). J. Anat. 1971, 108, 387–395. [Google Scholar] [PubMed]
- Belhassen, B.; Viskin, S. Idiopathic Ventricular Tachycardia and Fibrillation. J. Cardiovasc. Electrophysiol. 1993, 4, 356–368. [Google Scholar] [CrossRef]
- Viskin, S.; Rosso, R.; Rogowski, O.; Belhassen, B. The “Short-Coupled” Variant of Right Ventricular Outflow Ventricular Tachycardia: A Not-So-Benign Form of Benign Ventricular Tachycardia? J. Cardiovasc. Electrophysiol. 2005, 16, 912–916. [Google Scholar] [CrossRef] [PubMed]
- Boyden, P.A.; Dun, W.; Robinson, R.B. Cardiac Purkinje fibers and arrhythmias; The GK Moe Award Lecture 2015. Heart Rhythm. 2016, 13, 1172–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haïssaguerre, M.; Shoda, M.; Jaïs, P.; Nogami, A.; Shah, D.C.; Kautzner, J.; Arentz, T.; Kalushe, D.; Lamaison, D.; Griffith, M.; et al. Mapping and Ablation of Idiopathic Ventricular Fibrillation. Circulation 2002, 106, 962–967. [Google Scholar] [CrossRef]
- Haïssaguerre, M.; Shah, D.C.; Jaïs, P.; Shoda, M.; Kautzner, J.; Arentz, T.; Kalushe, D.; Kadish, A.; Griffith, M.; Gaita, F.; et al. Role of Purkinje conducting system in triggering of idiopathic ventricular fibrillation. Lancet 2002, 359, 677–678. [Google Scholar] [CrossRef]
- Sadek, M.M.; Benhayon, D.; Sureddi, R.; Chik, W.; Santangeli, P.; Supple, G.E.; Hutchinson, M.D.; Bala, R.; Carballeira, L.; Zado, E.S.; et al. Idiopathic ventricular arrhythmias originating from the moderator band: Electrocardiographic characteristics and treatment by catheter ablation. Heart Rhythm. 2015, 12, 67–75. [Google Scholar] [CrossRef]
- Anter, E.; Buxton, A.E.; Silverstein, J.R.; Josephson, M.E. Idiopathic Ventricular Fibrillation Originating from the Moderator Band. J. Cardiovasc. Electrophysiol. 2012, 24, 97–100. [Google Scholar] [CrossRef]
- Nogami, A.; Sugiyasu, A.; Kubota, S.; Kato, K. Mapping and ablation of idiopathic ventricular fibrillation from the Purkinje system. Heart Rhythm. 2005, 2, 646–649. [Google Scholar] [CrossRef]
- Walton, R.D.; Pashaei, A.; Martinez, M.E.; Constantin, M.; Duchateau, J.; Bear, L.; Cros, C.; Pascarel-Auclerc, C.; Guo, Y.; Benoist, D.; et al. Compartmentalized Structure of the Moderator Band Provides a Unique Substrate for Macroreentrant Ventricular Tachycardia. Circ. Arrhythmia Electrophysiol. 2018, 11, e005913. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, A.; Inada, S.; Li, J.; Tellez, J.O.; Yanni, J.; Sleiman, R.; Allah, E.A.; Anderson, R.H.; Zhang, H.; Boyett, M.R.; et al. Anatomical and molecular mapping of the left and right ventricular His–Purkinje conduction networks. J. Mol. Cell. Cardiol. 2011, 51, 689–701. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Hur, M.S. Morphological classification of the moderator band and its relationship with the anterior papillary muscle. Anat. Cell Biol. 2019, 52, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Dobrzynski, H.; Anderson, R.H.; Atkinson, A.; Borbas, Z.; D’Souza, A.; Fraser, J.F.; Inada, S.; Logantha, S.J.; Monfredi, O.; Morris, G.M.; et al. Structure, function and clinical relevance of the cardiac conduction system, including the atrioventricular ring and outflow tract tissues. Pharmacol. Ther. 2013, 139, 260–288. [Google Scholar] [CrossRef]
- Sommer, J.R.; Johnson, E.A. Cardiac muscle: A comparative study of Purkinje fibers and ventricular fibers. J. Cell Biol. 1968, 36, 497–526. [Google Scholar] [CrossRef]
- Schmid, P.G.; Greif, B.J.; Lund, D.D.; Roskoski, R., Jr. Regional choline acetyltransferase activity in the guinea pig heart. Circ. Res. 1978, 42, 657–660. [Google Scholar] [CrossRef] [Green Version]
- Xiao, L.; Koopmann, T.T.; Ördög, B.; Postema, P.G.; Verkerk, A.O.; Iyer, V.; Sampson, K.J.; Boink, G.J.; Mamarbachi, M.A.; Varro, A.; et al. Unique cardiac Purkinje fiber transient outward current β-subunit composition: A potential molecular link to idiopathic ventricular fibrillation. Circ. Res. 2013, 112, 1310–1322. [Google Scholar] [CrossRef]
- Myerburg, R.J.; Stewart, J.W.; Hoffman, B.F. Electrophysiological Properties of the Canine Peripheral A-V Conducting System. Circ. Res. 1970, 26, 361–378. [Google Scholar] [CrossRef] [Green Version]
- He, B.; Lu, Z.; He, W.; Huang, B.; Yu, L.; Wu, L.; Cui, B.; Hu, X.; Jiang, H. The effects of atrial ganglionated plexi stimulation on ventricular electro-physiology in a normal canine heart. J. Interv. Card. Electrophysiol. 2013, 37, 1–8. [Google Scholar] [CrossRef]
- Antzelevitch, C.; Sicouri, S. Clinical relevance of cardiac arrhythmias generated by afterdepolarizations: Role of M cells in the generation of U waves, triggered activity and torsade de pointes. J. Am. Coll. Cardiol. 1994, 23, 259–277. [Google Scholar] [CrossRef] [Green Version]
- Li, P.; Rudy, Y. A model of canine purkinje cell electrophysiology and Ca(2+) cycling: Rate dependence, triggered activity, and comparison to ventricular myocytes. Circ. Res. 2011, 109, 71–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quinn, T.A.; Jin, H.; Lee, P.; Kohl, P. Mechanically Induced Ectopy via Stretch-Activated Cation-Nonselective Channels Is Caused by Local Tissue Deformation and Results in Ventricular Fibrillation if Triggered on the Repolarization Wave Edge (Commotio Cordis). Circ. Arrhythmia Electrophysiol. 2017, 10, e004777. [Google Scholar] [CrossRef] [PubMed]
- Zeppenfeld, K.; Tfelt-Hansen, J.; de Riva, M.; Winkel, B.G.; Behr, E.R.; Blom, N.A.; Charron, P.; Corrado, D.; Dagres, N.; de Chillou, C.; et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur. Heart J. 2022, 43, 3997–4126. [Google Scholar]
- Steinfurt, J.; Nazer, B.; Aguilar, M.; Moss, J.; Higuchi, S.; Zarse, M.; Trolese, L.; Gressler, A.; Faber, T.S.; Odening, K.E.; et al. Catheter ablation of short-coupled variant of torsade de pointes. Clin. Res. Cardiol. 2021, 111, 502–510. [Google Scholar] [CrossRef] [PubMed]
- Crawford, T.; Mueller, G.; Good, E.; Jongnarangsin, K.; Chugh, A.; Pelosi, F.; Ebinger, M.; Oral, H.; Morady, F.; Bogun, F. Ventricular arrhythmias originating from papillary muscles in the right ventricle. Heart Rhythm. 2010, 7, 725–730. [Google Scholar] [CrossRef]
- Enriquez, A.; Baranchuk, A.; Briceno, D.; Saenz, L.; Garcia, F. How to use the 12-lead ECG to predict the site of origin of idiopathic ventricular arrhythmias. Heart Rhythm. 2019, 16, 1538–1544. [Google Scholar] [CrossRef]
- Efremidis, M.; Vlachos, K.; Kyriakopoulou, M.; Mililis, P.; Martin, C.A.; Bazoukis, G.; Dragasis, S.; Megarisiotou, A.; Unger, P.; Frontera, A.; et al. The RV1-V3 transition ratio: A novel electrocardiographic criterion for the differentiation of right versus left outflow tract premature ventricular complexes. Heart Rhythm. O2 2021, 2, 521–528. [Google Scholar] [CrossRef]
- Fries, B.; Johnson, V.; Rutsatz, W.; Schmitt, J.; Bogossian, H. Lokalisation ventrikulärer Extrasystolen im 12-Kanal-EKG [Localization of ventricular premature contractions by 12-lead ECG]. Herzschrittmachertherapie Elektrophysiologie 2021, 32, 21–26. [Google Scholar] [CrossRef]
- Santoro, F.; Di Biase, L.; Hranitzky, P.; Sanchez, J.E.; Santangeli, P.; Perini, A.P.; Burkhardt, J.D.; Natale, A. Ventricular Tachycardia Originating from the Septal Papillary Muscle of the Right Ventricle: Electrocardiographic and Electrophysiological Characteristics. J. Cardiovasc. Electrophysiol. 2014, 26, 145–150. [Google Scholar] [CrossRef]
- Chen, H.; Shi, L.; Yang, B.; Ju, W.; Zhang, F.; Yang, G.; Gu, K.; Li, M.; Cao, K.; Ouyang, F.; et al. Electrophysiological Characteristics of Bundle Branch Reentry Ventricular Tachycardia in Patients Without Structural Heart Disease. Circ. Arrhythmia Electrophysiol. 2018, 11, e006049. [Google Scholar] [CrossRef]
- Chinitz, J.S.; Sedaghat, D.; Harding, M.; Darge, A.; Epstein, L.M.; John, R. Adjuvant use of a cryoballoon to facilitate ablation of premature ventricular contraction–triggered ventricular fibrillation originating from the moderator band. Heart Case Rep. 2019, 5, 578–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.-Q.; Wang, Y.-X.; Que, D.-D.; Shao, J.; Song, X.-D.; Yang, P.-Z. Successful Ablation of Moderator Band-Originated Ventricular Tachycardia at Its Ventricle Insertion Sites. Chin. Med. J. 2018, 131, 1371–1372. [Google Scholar] [CrossRef] [PubMed]
- Li, J.-Y.; Jiang, J.-B.; He, Y.; Luo, J.-C.; Zhong, G.-Q. Ventricular Tachycardia Originating from Moderator Band: New Perspective on Catheter Ablation. Case Rep. Cardiol. 2017, 2017, 3414360. [Google Scholar] [CrossRef]
- Serdoz, L.V.; Rittger, H.; Furlanello, F.; Bastian, D. Quinidine—A legacy within the modern era of antiarrhythmic therapy. Pharmacol. Res. 2019, 144, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Fumagalli, S.; Pieragnoli, P.; Haugaa, K.H.; Potpara, T.S.; Rasero, L.; Ramacciati, N.; Ricciardi, G.; Solimene, F.; Mascia, G.; Mascioli, G.; et al. The influence of age on the psychological profile of patients with cardiac implantable electronic devices: Results from the Italian population in a multicenter study conducted by the European Heart Rhythm Association. Aging Clin. Exp. Res. 2018, 31, 1219–1226. [Google Scholar] [CrossRef]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Collet, J.-P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur. Heart J. 2021, 42, 17–96, Erratum in Eur. Heart J. 2021, 42, 548–549. [Google Scholar] [CrossRef]
- Porcedda, G.; Brambilla, A.; Favilli, S.; Spaziani, G.; Mascia, G.; Giaccardi, M. Frequent Ventricular Premature Beats in Children and Adolescents: Natural History and Relationship with Sport Activity in a Long-Term Follow-Up. Pediatr. Cardiol. 2019, 41, 123–128. [Google Scholar] [CrossRef]
- Russo, A.D.; Compagnucci, P.; Casella, M.; Gasperetti, A.; Riva, S.; Dessanai, M.A.; Pizzamiglio, F.; Catto, V.; Guerra, F.; Stronati, G.; et al. Ventricular arrhythmias in athletes: Role of a comprehensive diagnostic workup. Heart Rhythm. 2021, 19, 90–99. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Landra, F.; Marallo, C.; Santoro, A.; Taddeucci, S.; Tavera, M.C.; Baiocchi, C.; Palazzuoli, A. Moderator Band and Ventricular Tachycardia: Structural or Functional Substrate? J. Cardiovasc. Dev. Dis. 2023, 10, 159. https://doi.org/10.3390/jcdd10040159
Landra F, Marallo C, Santoro A, Taddeucci S, Tavera MC, Baiocchi C, Palazzuoli A. Moderator Band and Ventricular Tachycardia: Structural or Functional Substrate? Journal of Cardiovascular Development and Disease. 2023; 10(4):159. https://doi.org/10.3390/jcdd10040159
Chicago/Turabian StyleLandra, Federico, Carmine Marallo, Amato Santoro, Simone Taddeucci, Maria Cristina Tavera, Claudia Baiocchi, and Alberto Palazzuoli. 2023. "Moderator Band and Ventricular Tachycardia: Structural or Functional Substrate?" Journal of Cardiovascular Development and Disease 10, no. 4: 159. https://doi.org/10.3390/jcdd10040159