
Electro-Mechanical Alterations in Atrial Fibrillation: Structural, Electrical, and Functional Correlates

Abstract
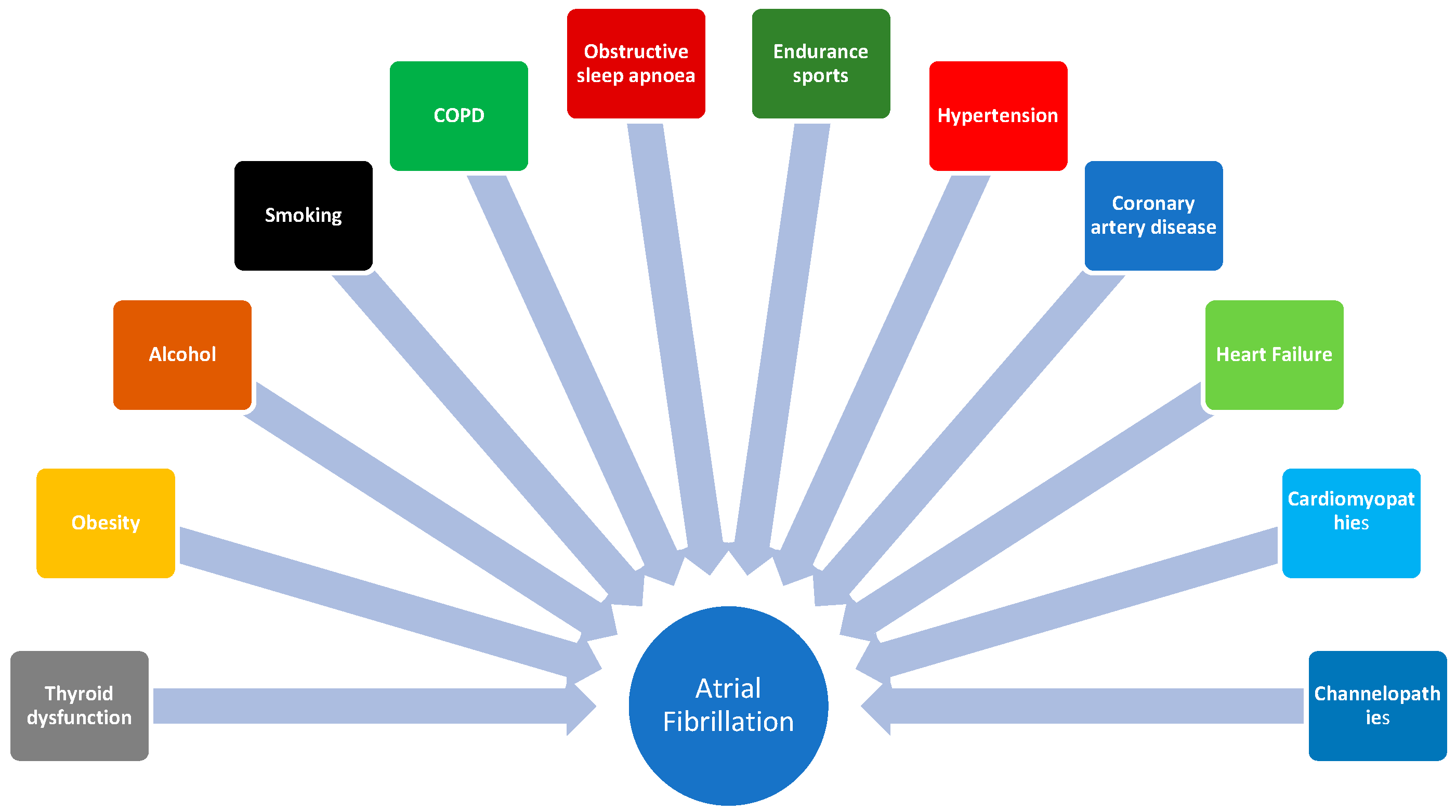
:1. Introduction
2. Structural Correlates of Conduction Disturbances
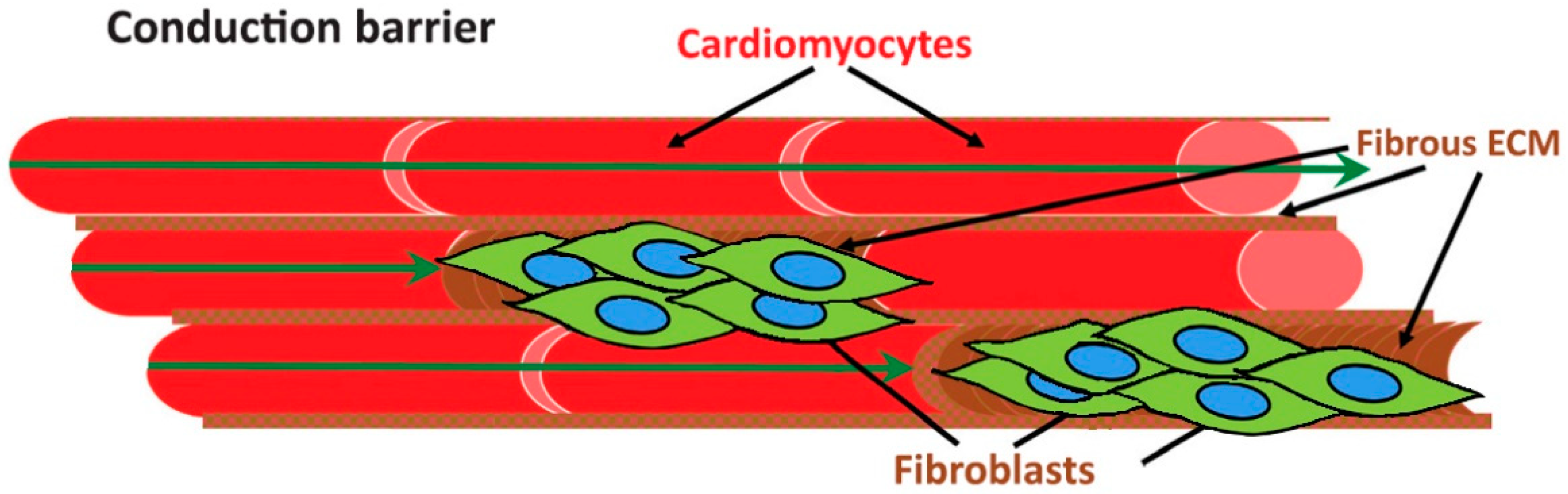
2.1. Atrial Fibrosis as a Hallmark Alteration in AF
2.2. Altered Connexin Expression
2.3. The Role of Interatrial Conduction
2.4. The Effect of Stretch on Atrial Conduction
3. Electrical Correlates of Conduction Disturbances
3.1. Alterations in P Wave Parameters
3.1.1. P Wave Duration
3.1.2. P Wave Axis
3.1.3. P Wave Voltage
3.1.4. P Wave Area
3.1.5. P Wave Terminal Force in Lead V1
3.1.6. P Wave Dispersion
3.2. Abnormal Electrophysiological Characteristics
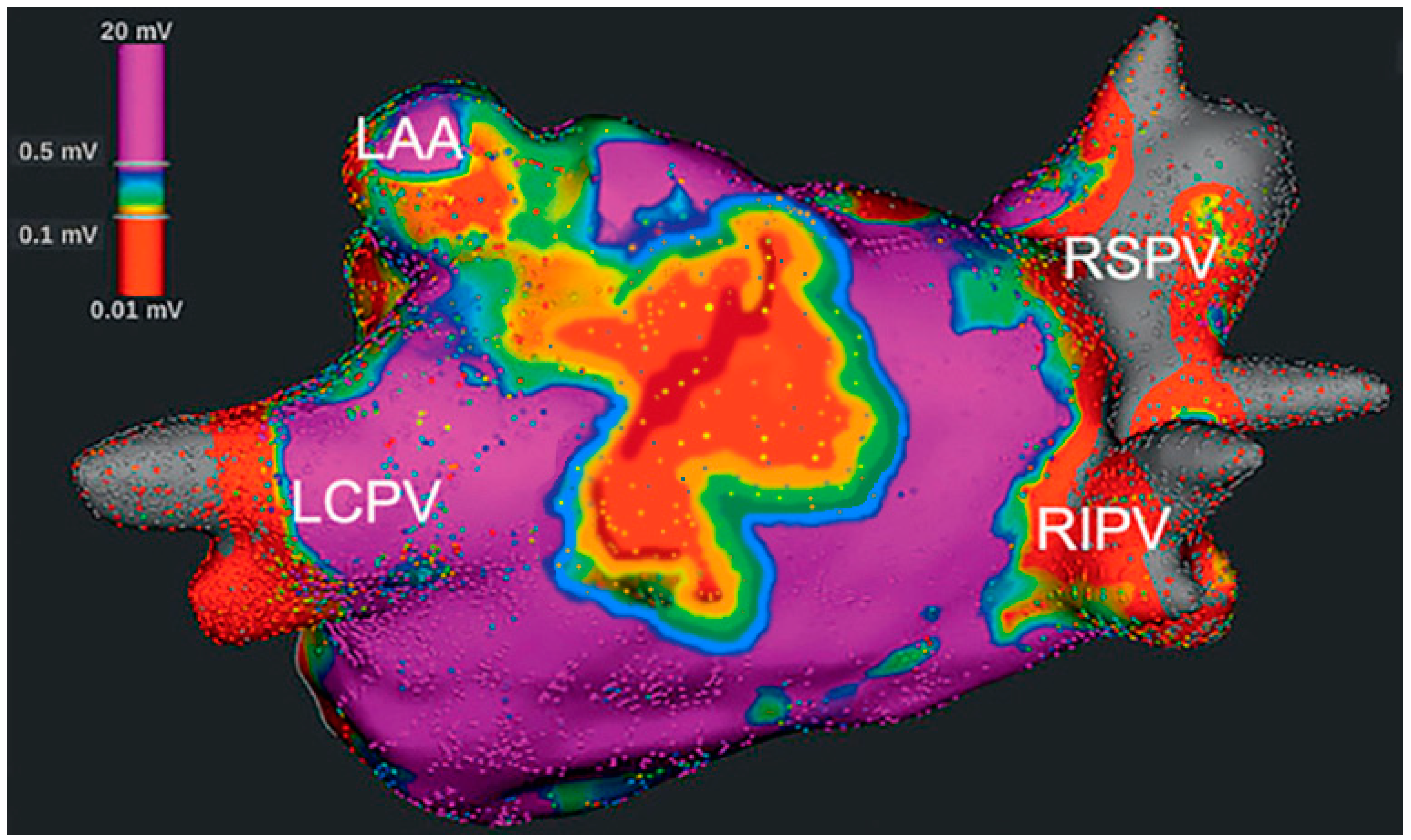
3.2.1. Bipolar Voltage Mapping
3.2.2. Unipolar Voltage Mapping
3.2.3. Electrogram Fractionation
3.2.4. Endo-Epicardial Asynchrony of the Atrial Wall
3.2.5. Cardiac Conduction Velocity
4. Functional Correlates of Conduction Disturbances
4.1. Left Atrial Size and Strain
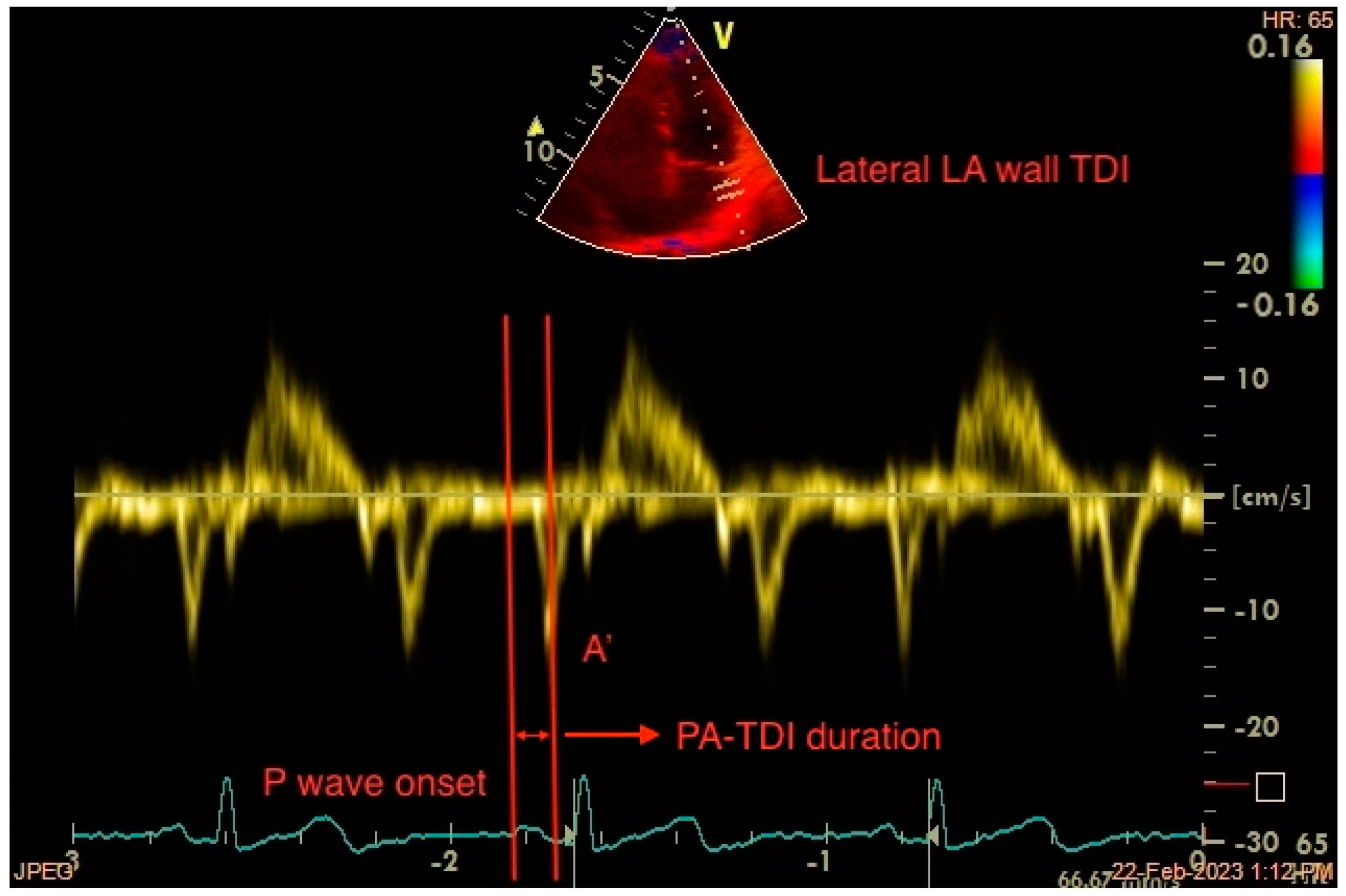
4.2. Total Atrial Conduction Time (PA-TDI Duration)
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [PubMed]
- Andrade, J.; Khairy, P.; Dobrev, D.; Nattel, S. The clinical profile and pathophysiology of atrial fibrillation: Relationships among clinical features, epidemiology, and mechanisms. Circ. Res. 2014, 114, 1453–1468. [Google Scholar] [CrossRef] [PubMed]
- Dilaveris, P.; Antoniou, C.K.; Manolakou, P.; Tsiamis, E.; Gatzoulis, K.; Tousoulis, D. Biomarkers Associated with Atrial Fibrosis and Remodeling. Curr. Med. Chem. 2019, 26, 780–802. [Google Scholar] [CrossRef]
- Sutanto, H. Individual Contributions of Cardiac Ion Channels on Atrial Repolarization and Reentrant Waves: A Multiscale In-Silico Study. J. Cardiovasc. Dev. Dis. 2022, 9, 28. [Google Scholar] [CrossRef] [PubMed]
- Wakili, R.; Voigt, N.; Kääb, S.; Dobrev, D.; Nattel, S. Recent advances in the molecular pathophysiology of atrial fibrillation. J. Clin. Investig. 2011, 12, 2955–2968. [Google Scholar] [CrossRef] [Green Version]
- Nattel, S.; Harada, M. Atrial remodeling and atrial fibrillation: Recent advances and translational perspectives. J. Am. Coll. Cardiol. 2014, 63, 2335–2345. [Google Scholar] [CrossRef] [Green Version]
- Graziano, F.; Juhasz, V.; Brunetti, G.; Cipriani, A.; Szabo, L.; Merkely, B.; Corrado, D.; D’Ascenzi, F.; Vago, H.; Zorzi, A. May Strenuous Endurance Sports Activity Damage the Cardiovascular System of Healthy Athletes? A Narrative Review. J. Cardiovasc. Dev. Dis. 2022, 9, 347. [Google Scholar] [CrossRef]
- Frost, L.; Vestergaard, P.; Mosekilde, L. Hyperthyroidism and risk of atrial fibrillation or flutter: A population-based study. Arch. Intern. Med. 2004, 164, 1675–1678. [Google Scholar] [CrossRef] [Green Version]
- Mont, L.; Elosua, R.; Brugada, J. Endurance sport practice as a risk factor for atrial fibrillation and atrial flutter. Europace 2009, 11, 11–17. [Google Scholar] [CrossRef]
- Mascia, G.; Arbelo, E.; Porto, I.; Brugada, R.; Brugada, J. The arrhythmogenic right ventricular cardiomyopathy in comparison to the athletic heart. J. Cardiovasc. Electrophysiol. 2020, 31, 1836–1843. [Google Scholar] [CrossRef]
- Chamberlain, A.M.; Agarwal, S.K.; Folsom, A.R.; Duval, S.; Soliman, E.Z.; Ambrose, M.; Eberly, L.E.; Alonso, A. Smoking and incidence of atrial fibrillation: Results from the Atherosclerosis Risk in Communities (ARIC) study. Heart Rhythm 2011, 8, 1160–1166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mascia, G.; Crotti, L.; Groppelli, A.; Canepa, M.; Merlo, A.C.; Benenati, S.; Di Donna, P.; Della Bona, R.; Soranna, D.; Zambon, A.; et al. Syncope in hypertrophic cardiomyopathy (part I): An updated systematic review and meta-analysis. Int. J. Cardiol. 2022, 357, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Vlachos, K.; Mascia, G.; Martin, C.A.; Bazoukis, G.; Frontera, A.; Cheniti, G.; Letsas, K.P.; Efremidis, M.; Georgopoulos, S.; Gkalapis, C.; et al. Atrial fibrillation in Brugada syndrome: Current perspectives. J. Cardiovasc. Electrophysiol. 2020, 31, 975–984. [Google Scholar] [CrossRef]
- Platonov, P.G.; McNitt, S.; Polonsky, B.; Rosero, S.Z.; Zareba, W. Atrial Fibrillation in Long QT Syndrome by Genotype. Circ. Arrhythmia Electrophysiol. 2019, 12, e007213. [Google Scholar] [CrossRef]
- Schotten, U.; Verheule, S.; Kirchhof, P.; Goette, A. Pathophysiological mechanisms of atrial fibrillation: A translational appraisal. Physiol. Rev. 2011, 91, 265–325. [Google Scholar] [CrossRef]
- Maesen, B.; Verheule, S.; Zeemering, S.; La Meir, M.; Nijs, J.; Lumeij, S.; Lau, D.H.; Granier, M.; Crijns, H.J.; Maessen, J.G.; et al. Endomysial fibrosis, rather than overall connective tissue content, is the main determinant of conduction disturbances in human atrial fibrillation. Europace 2022, 24, 1015–1024. [Google Scholar] [CrossRef]
- Yue, L.; Xie, J.; Nattel, S. Molecular determinants of cardiac fibroblast electrical function and therapeutic implications for atrial fibrillation. Cardiovasc. Res. 2011, 89, 744–753. [Google Scholar] [CrossRef] [Green Version]
- Han, F.T.; Akoum, N.; Marrouche, N. Value of magnetic resonance imaging in guiding atrial fibrillation management. Can. J. Cardiol. 2013, 29, 1194–1202. [Google Scholar] [CrossRef]
- McDowell, K.S.; Vadakkumpadan, F.; Blake, R.; Blauer, J.; Plank, G.; Macleod, R.S.; Trayanova, N.A. Mechanistic inquiry into the role of tissue remodeling in fibrotic lesions in human atrial fibrillation. Biophys. J. 2013, 104, 2764–2773. [Google Scholar] [CrossRef] [Green Version]
- Goette, A.; Kalman, J.M.; Aguinaga, L.; Akar, J.; Cabrera, J.A.; Chen, S.A.; Chugh, S.S.; Corradi, D.; D’Avila, A.; Dobrev, D.; et al. Document Reviewers: EHRA/HRS/APHRS/SOLAECE expert consensus on atrial cardiomyopathies: Definition, characterization, and clinical implication. Europace 2016, 18, 1455–1490. [Google Scholar] [CrossRef]
- Burstein, B.; Comtois, P.; Michael, G.; Nishida, K.; Villeneuve, L.; Yeh, Y.H.; Nattel, S. Changes in connexin expression and the atrial fibrillation substrate in congestive heart failure. Circ. Res. 2009, 105, 1213–1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polontchouk, L.; Haefliger, J.A.; Ebelt, B.; Schaefer, T.; Stuhlmann, D.; Mehlhorn, U.; Kuhn-Regnier, F.; De Vivie, E.R.; Dhein, S. Effects of chronic atrial fibrillation on gap junction distribution in human and rat atria. J. Am. Coll. Cardiol. 2001, 38, 883–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bikou, O.; Thomas, D.; Trappe, K.; Lugenbiel, P.; Kelemen, K.; Koch, M.; Soucek, R.; Voss, F.; Becker, R.; Katus, H.A.; et al. Connexin 43 gene therapy prevents persistent atrial fibrillation in a porcine model. Cardiovasc. Res. 2011, 92, 218–225. [Google Scholar] [CrossRef] [PubMed]
- Cosio, F.G.; Palacios, J.; Vidal, J.M.; Cocina, E.G.; Gómez-Sánchez, M.A.; Tamargo, L. Electrophysiologic studies in atrial fibrillation. Slow conduction of premature impulses: A possible manifestation of the background for reentry. Am. J. Cardiol. 1983, 51, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Kumagai, K.; Khrestian, C.; Waldo, A.L. Simultaneous multisite mapping studies during induced atrial fibrillation in the sterile pericarditis model. Insights into the mechanism of its maintenance. Circulation 1997, 95, 511–521. [Google Scholar] [CrossRef]
- Platonov, P.G.; Mitrofanova, L.B.; Chireikin, L.V.; Olsson, S.B. Morphology of inter- atrial conduction routes in patients with atrial fibrillation. Europace 2002, 4, 183–192. [Google Scholar] [CrossRef] [Green Version]
- Bachmann, G. The inter-auricular time interval. Am. J. Physiol. 1916, 41, 309–320. [Google Scholar] [CrossRef]
- Chauvin, M.; Shah, D.C.; Haïssaguerre, M.; Marcellin, L.; Brechenmacher, C. The anatomic basis of connections between the coronary sinus musculature and the left atrium in humans. Circulation 2000, 101, 647–652. [Google Scholar] [CrossRef] [Green Version]
- Johner, N.; Namdar, M.; Shah, D.C. Intra- and interatrial conduction abnormalities: Hemodynamic and arrhythmic significance. J. Interv. Card. Electrophysiol. 2018, 52, 293–302. [Google Scholar] [CrossRef]
- Benito, E.M.; De Luna, A.B.; Baranchuk, A.; Mont, L. Extensive atrial fibrosis assessed by late gadolinium enhancement cardiovascular magnetic resonance associated with advanced interatrial block electrocardiogram pattern. Europace 2017, 19, 377. [Google Scholar] [CrossRef]
- The, A.W.; Kistler, P.M.; Lee, G.; Medi, C.; Heck, P.M.; Spence, S.J.; Sparks, P.B.; Morton, J.B.; Kalman, J.M. Electroanatomic remodeling of the left atrium in paroxysmal and persistent atrial fibrillation patients without structural heart disease. J. Cardiovasc. Electrophysiol. 2012, 23, 232–238. [Google Scholar]
- Lin, Y.; Yang, B.; Garcia, F.C.; Ju, W.; Zhang, F.; Chen, H.; Yu, J.; Li, M.; Gu, K.; Cao, K.; et al. Comparison of left atrial electrophysiologic abnormalities during sinus rhythm in patients with different type of atrial fibrillation. J. Interv. Card. Electrophysiol. 2014, 39, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Mouws, E.M.J.P.; van der Does, L.J.M.E.; Kik, C.; Lanters, E.A.H.; Teuwen, C.P.; Knops, P.; Bogers, A.J.J.C.; de Groot, N.M.S. Impact of the arrhythmogenic potential of long lines of conduction slowing at the pulmonary vein area. Heart Rhythm 2019, 16, 511–519. [Google Scholar] [CrossRef] [Green Version]
- van der Does, W.F.B.; Heida, A.; van der Does, L.J.M.E.; Bogers, A.J.J.C.; de Groot, N.M.S. Conduction Disorders during Sinus Rhythm in Relation to Atrial Fibrillation Persistence. J. Clin. Med. 2021, 10, 2846. [Google Scholar] [CrossRef]
- Kojodjojo, P.; Kanagaratnam, P.; Markides, V.; Davies, D.W.; Peters, N. Age-related changes in human left and right atrial conduction. J. Cardiovasc. Electrophysiol. 2006, 17, 120–127. [Google Scholar] [CrossRef]
- Kistler, P.M.; Sanders, P.; Fynn, S.P.; Stevenson, I.H.; Spence, S.J.; Vohra, J.K.; Sparks, P.B.; Kalman, J.M. Electrophysiologic and electroanatomic changes in the human atrium associated with age. J. Am. Coll. Cardiol. 2004, 44, 109–116. [Google Scholar] [CrossRef]
- Roberts-Thomson, K.C.; Kistler, P.M.; Sanders, P.; Morton, J.B.; Haqqani, H.M.; Stevenson, I.; Vohra, J.K.; Sparks, P.B.; Kalman, J.M. Fractionated atrial electrograms during sinus rhythm: Relationship to age, voltage, and conduction velocity. Heart Rhythm 2009, 6, 587–591. [Google Scholar] [CrossRef]
- Spach, M.S.; Dolber, P.C.; Heidlage, J.F. Influence of the passive anisotropic properties on directional differences in propagation following modification of the sodium conductance in human atrial muscle. A model of reentry based on anisotropic discontinuous propagation. Circ. Res. 1988, 62, 811–832. [Google Scholar] [CrossRef] [Green Version]
- Koura, T.; Hara, M.; Takeuchi, S.; Ota, K.; Okada, Y.; Miyoshi, S.; Watanabe, A.; Shiraiwa, K.; Mitamura, H.; Kodama, I.; et al. Anisotropic conduction properties in canine atria analyzed by high-resolution optical mapping: Preferential direction of conduction block changes from longitudinal to transverse with increasing age. Circulation 2002, 105, 2092–2098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravelli, F.; Masè, M.; del Greco, M.; Marini, M.; Disertori, M. Acute atrial dilatation slows conduction and increases AF vulnerability in the human atrium. J. Cardiovasc. Electrophysiol. 2011, 22, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Kuijpers, N.H.; ten Eikelder, H.M.; Bovendeerd, P.H.; Verheule, S.; Arts, T.; Hilbers, P.A. Mechanoelectric feedback leads to conduction slowing and block in acutely dilated atria: A modeling study of cardiac electromechanics. Am. J. Physiol. Heart Circ. Physiol. 2007, 292, H2832–H2853. [Google Scholar] [CrossRef]
- Kamkin, A.; Kiseleva, I.; Wagner, K.D.; Bohm, J.; Theres, H.; Günther, J.; Scholz, H. Characterization of stretch-activated ion currents in isolated atrial myocytes from human hearts. Pflügers Arch. 2003, 446, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Mills, R.W.; Narayan, S.M.; McCulloch, A.D. Mechanisms of conduction slowing during myocardial stretch by ventricular volume loading in the rabbit. Am. J. Physiol. Heart Circ. Physiol. 2008, 295, H1270–H1278. [Google Scholar] [CrossRef] [PubMed]
- Kalifa, J.; Jalife, J.; Zaitsev, A.V.; Bagwe, S.; Warren, M.; Moreno, J.; Berenfeld, O.; Nattel, S. Intra-atrial pressure increases rate and organization of waves emanating from the superior pulmonary veins during atrial fibrillation. Circulation 2003, 108, 668–671. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.L.; Chen, Y.C.; Chen, Y.J.; Wangcharoen, W.; Lee, S.H.; Lin, C.I.; Chen, S.A. Mechanoelectrical feedback regulates the arrhythmogenic activity of pulmonary veins. Heart 2007, 93, 82–88. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.Y.; Ribeiro, A.L.P.; Platonov, P.G.; Cygankiewicz, I.; Soliman, E.Z.; Gorenek, B.; Ikeda, T.; Vassilikos, V.P.; Steinberg, J.S.; Varma, N.; et al. P Wave Parameters and Indices: A Critical Appraisal of Clinical Utility, Challenges, and Future Research-A Consensus Document Endorsed by the International Society of Electrocardiology and the International Society for Holter and Noninvasive Electrocardiology. Circ. Arrhythmia Electrophysiol. 2022, 15, e010435. [Google Scholar]
- Intzes, S.; Zagoridis, K.; Symeonidou, M.; Spanoudakis, E.; Arya, A.; Dinov, B.; Dagres, N.; Hindricks, G.; Bollmann, A.; Kanoupakis, E.; et al. P-wave duration and atrial fibrillation recurrence after catheter ablation: A systematic review and meta-analysis. Europace 2022, 25, euac210. [Google Scholar] [CrossRef]
- Rangel, M.O.; O’Neal, W.T.; Soliman, E.Z. Usefulness of the Electrocardiographic P-Wave Axis as a Predictor of Atrial Fibrillation. Am. J. Cardiol. 2016, 117, 100–104. [Google Scholar] [CrossRef]
- Park, J.K.; Park, J.; Uhm, J.S.; Joung, B.; Lee, M.H.; Pak, H.N. Low P-wave amplitude (<0.1 mV) in lead I is associated with displaced inter-atrial conduction and clinical recurrence of paroxysmal atrial fibrillation after radiofrequency catheter ablation. Europace 2016, 18, 384–391. [Google Scholar]
- Zeng, C.; Wei, T.; Zhao, R.; Wang, C.; Chen, L.; Wang, L. Electrocardiographic diagnosis of left atrial enlargement in patients with mitral stenosis: The value of the P-wave area. Acta Cardiol. 2003, 58, 139–141. [Google Scholar] [CrossRef]
- Dilaveris, P.E.; Gialafos, E.J.; Andrikopoulos, G.K.; Richter, D.J.; Papanikolaou, V.; Poralis, K.; Gialafos, J.E. Clinical and electrocardiographic predictors of recurrent atrial fibrillation. Pacing Clin. Electrophysiol. 2000, 23, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Yamada, T.; Murakami, Y.; Okada, T.; Okamoto, M.; Shimizu, T.; Toyama, J.; Yoshida, Y.; Tsuboi, N.; Ito, T.; Muto, M.; et al. Incidence, location, and cause of recovery of electrical connections between the pulmonary veins and the left atrium after pulmonary vein isolation. Europace 2006, 8, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Rolf, S.; Kircher, S.; Arya, A.; Eitel, C.; Sommer, P.; Richter, S.; Gaspar, T.; Bollmann, A.; Altmann, D.; Piedra, C.; et al. Tailored atrial substrate modification based on low-voltage areas in catheter ablation of atrial fibrillation. Circ. Arrhythmia Electrophysiol. 2014, 7, 825–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yagishita, A.; Gimbel, J.R.; DE Oliveira, S.; Manyam, H.; Sparano, D.; Cakulev, I.; Mackall, J.; Arruda, M. Long-term outcome of left atrial voltage-guided substrate ablation during atrial fibrillation: A novel adjunctive ablation strategy. J. Cardiovasc. Electrophysiol. 2017, 28, 147–155. [Google Scholar] [CrossRef]
- Prabhu, S.; Voskoboinik, A.; McLellan, A.J.A.; Peck, K.Y.; Pathik, B.; Nalliah, C.J.; Wong, G.R.; Azzopardi, S.M.; Lee, G.; Mariani, J.; et al. A comparison of the electrophysiologic and electroanatomic characteristics between the right and left atrium in persistent atrial fibrillation: Is the right atrium a window into the left? J. Cardiovasc. Electrophysiol. 2017, 28, 1109–1116. [Google Scholar] [CrossRef]
- van Schie, M.S.; Starreveld, R.; Bogers, A.J.J.C.; de Groot, N.M.S. Sinus rhythm voltage fingerprinting in patients with mitral valve disease using a high-density epicardial mapping approach. Europace 2021, 23, 469–478. [Google Scholar] [CrossRef]
- Viles-Gonzalez, J.F.; Gomes, J.A.; Miller, M.A.; Dukkipati, S.R.; Koruth, J.S.; Eggert, C.; Coffey, J.; Reddy, V.Y.; d’Avila, A. Areas with complex fractionated atrial electrograms recorded after pulmonary vein isolation represent normal voltage and conduction velocity in sinus rhythm. Europace 2013, 15, 339–346. [Google Scholar] [CrossRef]
- de Groot, N.; van der Does, L.; Yaksh, A.; Lanters, E.; Teuwen, C.; Knops, P.; van de Woestijne, P.; Bekkers, J.; Kik, C.; Bogers, A.; et al. Direct Proof of Endo-Epicardial Asynchrony of the Atrial Wall During Atrial Fibrillation in Humans. Circ. Arrhythmia Electrophysiol. 2016, 9, e003648. [Google Scholar] [CrossRef]
- van der Does, L.J.M.E.; Starreveld, R.; Kharbanda, R.K.; Knops, P.; Kik, C.; Bogers, A.J.J.C.; de Groot, N.M.S. Detection of Endo-epicardial Asynchrony in the Atrial Wall Using One-Sided Unipolar and Bipolar Electrograms. J. Cardiovasc. Transl. Res. 2021, 14, 902–911. [Google Scholar] [CrossRef]
- Stiles, M.K.; John, B.; Wong, C.X.; Kuklik, P.; Brooks, A.G.; Lau, D.H.; Dimitri, H.; Roberts-Thomson, K.C.; Wilson, L.; De Sciscio, P.; et al. Paroxysmal lone atrial fibrillation is associated with an abnormal atrial substrate: Characterizing the ‘second factor’. J. Am. Coll. Cardiol. 2009, 53, 1182–1191. [Google Scholar] [CrossRef]
- Zheng, Y.; Xia, Y.; Carlson, J.; Kongstad, O.; Yuan, S. Atrial average conduction velocity in patients with and without paroxysmal atrial fibrillation. Clin. Physiol. Funct. Imaging 2017, 37, 596–601. [Google Scholar] [CrossRef] [PubMed]
- Rossi, P.; Cauti, F.M.; Limite, L.R.; Iaia, L.; Allegretti, G.; Di Renzi, P.; Longa, G.D.; Quaglione, R.; Piccirillo, G.; Bianchi, S. Interatrial conduction times in paroxysmal atrial fibrillation patients with normal atrial volume and their correlation with areas of local prolonged bipolar electrograms. J. Electrocardiol. 2020, 58, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Fraser, H.R.L.; Turner, R.W.D. Auricular Fibrillation. BMJ 1955, 2, 1414–1418. [Google Scholar] [CrossRef] [PubMed]
- Henry, W.L.; Morganroth, J.; Pearlman, A.S.; Clark, C.E.; Redwood, D.R.; Itscoitz, S.B.; Epstein, S.E. Relation between Echocardiographically Determined Left Atrial Size and Atrial Fibrillation. Circulation 1976, 53, 273–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasan, R.S.; Larson, M.G.; Levy, D.; Evans, J.C.; Benjamin, E.J. Distribution and Categorization of Echocardiographic Measurements in Relation to Reference Limits: The Framingham Heart Study: Formulation of a Height- and Sex-Specific Classification and Its Prospective Validation. Circulation 1997, 96, 1863–1873. [Google Scholar] [CrossRef] [PubMed]
- Vaziri, S.M.; Larson, M.G.; Benjamin, E.J.; Levy, D. Echocardiographic Predictors of Nonrheumatic Atrial Fibrillation. The Framingham Heart Study. Circulation 1994, 89, 724–730. [Google Scholar] [CrossRef] [Green Version]
- Ravelli, F.; Allessie, M. Effects of Atrial Dilatation on Refractory Period and Vulnerability to Atrial Fibrillation in the Isolated Langendorff-Perfused Rabbit Heart. Circulation 1997, 96, 1686–1695. [Google Scholar] [CrossRef] [PubMed]
- Solti, F.; Vecsey, T.; Kekesi, V.; Juhasz-Nagy, A. The Effect of Atrial Dilatation on the Genesis of Atrial Arrhythmias. Cardiovasc. Res. 1989, 23, 882–886. [Google Scholar] [CrossRef]
- Wijffels, M.C.E.F.; Kirchhof, C.J.H.J.; Dorland, R.; Power, J.; Allessie, M.A. Electrical Remodeling Due to Atrial Fibrillation in Chronically Instrumented Conscious Goats: Roles of Neurohumoral Changes, Ischemia, Atrial Stretch, and High Rate of Electrical Activation. Circulation 1997, 96, 3710–3720. [Google Scholar] [CrossRef]
- Sideris, D.A.; Toumanidis, S.T.; Thodorakis, M.; Kostopoulos, K.; Tselepatiotis, E.; Langoura, C.; Stringli, T.; Moulopoulos, S.D. Some Observations on the Mechanism of Pressure Related Atrial Fibrillation. Eur. Heart J. 1994, 15, 1585–1589. [Google Scholar] [CrossRef]
- Satoh, T.; Zipes, D.P. Unequal Atrial Stretch in Dogs Increases Dispersion of Refractoriness Conducive to Developing Atrial Fibrillation. J. Cardiovasc. Electrophysiol. 1996, 7, 833–842. [Google Scholar] [CrossRef] [PubMed]
- Nattel, S.; Burstein, B.; Dobrev, D. Atrial Remodeling and Atrial Fibrillation: Mechanisms and Implications. Circ. Arrhythmia Electrophysiol. 2008, 1, 62–73. [Google Scholar] [CrossRef] [Green Version]
- Casaclang-Verzosa, G.; Gersh, B.J.; Tsang, T.S.M. Structural and Functional Remodeling of the Left Atrium. J. Am. Coll. Cardiol. 2008, 51, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Allessie, M.A. Atrial Electrophysiologic Remodeling: Another Vicious Circle? J. Cardiovasc. Electrophysiol. 1998, 9, 1378–1393. [Google Scholar] [CrossRef]
- Wijffels, M.C.E.F.; Kirchhof, C.J.H.J.; Dorland, R.; Allessie, M.A. Atrial Fibrillation Begets Atrial Fibrillation: A Study in Awake Chronically Instrumented Goats. Circulation 1995, 92, 1954–1968. [Google Scholar] [CrossRef] [PubMed]
- Berruezo, A.; Tamborero, D.; Mont, L.; Benito, B.; Tolosana, J.M.; Sitges, M.; Vidal, B.; Arriagada, G.; Mendez, F.; Matiello, M.; et al. Pre-Procedural Predictors of Atrial Fibrillation Recurrence after Circumferential Pulmonary Vein Ablation. Eur. Heart J. 2007, 28, 836–841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hof, I.; Arbab-Zadeh, A.; Scherr, D.; Chilukuri, K.; Dalal, D.; Abraham, T.; Lima, J.; Calkins, H. Correlation of Left Atrial Diameter by Echocardiography and Left Atrial Volume by Computed Tomography. J. Cardiovasc. Electrophysiol. 2009, 20, 159–163. [Google Scholar] [CrossRef]
- den Uijl, D.W.; Bax, J.J. Left Atrial Size as a Predictor of Successful Radiofrequency Catheter Ablation for Atrial Fibrillation. Europace 2009, 11, 1255–1256. [Google Scholar] [CrossRef]
- Abecasis, J.; Dourado, R.; Ferreira, A.; Saraiva, C.; Cavaco, D.; Santos, K.R.; Morgado, F.B.; Adragao, P.; Silva, A. Left Atrial Volume Calculated by Multi-Detector Computed Tomography May Predict Successful Pulmonary Vein Isolation in Catheter Ablation of Atrial Fibrillation. Europace 2009, 11, 1289–1294. [Google Scholar] [CrossRef]
- Beinart, R.; Nazarian, S. Role of Magnetic Resonance Imaging in Atrial Fibrillation Ablation. Curr. Treat. Options Cardiovasc. Med. 2014, 16, 316. [Google Scholar] [CrossRef] [Green Version]
- Nori, D.; Raff, G.; Gupta, V.; Gentry, R.; Boura, J.; Haines, D.E. Cardiac Magnetic Resonance Imaging Assessment of Regional and Global Left Atrial Function before and after Catheter Ablation for Atrial Fibrillation. J. Interv. Card. Electrophysiol. 2009, 26, 109–117. [Google Scholar] [CrossRef]
- Kato, R.; Lickfett, L.; Meininger, G.; Dickfeld, T.; Wu, R.; Juang, G.; Angkeow, P.; LaCorte, J.; Bluemke, D.; Berger, R.; et al. Pulmonary Vein Anatomy in Patients Undergoing Catheter Ablation of Atrial Fibrillation: Lessons Learned by Use of Magnetic Resonance Imaging. Circulation 2003, 107, 2004–2010. [Google Scholar] [CrossRef] [PubMed]
- Ishimoto, N.; Ito, M.; Kinoshita, M. Signal-Averaged P-Wave Abnormalities and Atrial Size in Patients with and without Idiopathic Paroxysmal Atrial Fibrillation. Am. Heart J. 2000, 139, 684–689. [Google Scholar] [CrossRef] [PubMed]
- Anselmino, M.; Blandino, A.; Beninati, S.; Rovera, C.; Boffano, C.; Belletti, M.; Caponi, D.; Scaglione, M.; Cesarani, F.; Gaita, F. Morphologic Analysis of Left Atrial Anatomy by Magnetic Resonance Angiography in Patients with Atrial Fibrillation: A Large Single Center Experience. J. Cardiovasc. Electrophysiol. 2011, 22, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Manning, W.J.; Silverman, D.I.; Katz, S.E.; Riley, M.F.; Come, P.C.; Doherty, R.M.; Munson, J.T.; Douglas, P.S. Impaired Left Atrial Mechanical Function after Cardioversion: Relation to the Duration of Atrial Fibrillation. J. Am. Coll. Cardiol. 1994, 23, 1535–1540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manning, W.J.; Silverman, D.I.; Katz, S.E.; Riley, M.F.; Doherty, R.M.; Munson, J.T.; Douglas, P.S. Temporal Dependence of the Return of Atrial Mechanical Function on the Mode of Cardioversion of Atrial Fibrillation to Sinus Rhythm. Am. J. Cardiol. 1995, 75, 624–626. [Google Scholar] [CrossRef]
- Fatkin, D.; Kuchar, D.L.; Thorburn, C.W.; Feneley, M.P. Transesophageal Echocardiography before and during Direct Current Cardioversion of Atrial Fibrillation: Evidence for “Atrial Stunning” as a Mechanism of Thromboembolic Complications. J. Am. Coll. Cardiol. 1994, 23, 307–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, I.W.; Fatkin, D.; Sagar, K.B.; Khandheria, B.K.; Leung, D.Y.; Galloway, J.M.; Feneley, M.P.; Walsh, W.F.; Grimm, R.A.; Stollberger, C. Exclusion of Atrial Thrombus by Transesophageal Echocardiography Does Not Preclude Embolism after Cardioversion of Atrial Fibrillation. A Multicenter Study. Circulation 1994, 89, 2509–2513. [Google Scholar] [CrossRef] [Green Version]
- Grimm, R.A.; Leung, D.Y.; Black, I.W.; Stewart, W.J.; Thomas, J.D.; Klein, A.L. Left Atrial Appendage “Stunning” after Spontaneous Conversion of Atrial Fibrillation Demonstrated by Transesophageal Doppler Echocardiography. Am. Heart J. 1995, 130, 174–176. [Google Scholar] [CrossRef]
- Allessie, M. Electrical, Contractile and Structural Remodeling during Atrial Fibrillation. Cardiovasc. Res. 2002, 54, 230–246. [Google Scholar] [CrossRef]
- Schotten, U.; Allessie, M.A. Electrical and Mechanical Remodeling of the Atria: What Are the Underlying Mechanisms, the Time Course and the Clinical Relevance? In Cardiac Arrhythmias 2001, Proceedings of the 7th International Workshop on Cardiac Arrhythmias, Venice, Italy, 7–10 October 2001; Springer: Milan, Italy, 2002. [Google Scholar]
- Yue, L.; Feng, J.; Gaspo, R.; Li, G.-R.; Wang, Z.; Nattel, S. Ionic Remodeling Underlying Action Potential Changes in a Canine Model of Atrial Fibrillation. Circ. Res. 1997, 81, 512–525. [Google Scholar] [CrossRef] [PubMed]
- Schotten, U.; Neuberger, H.-R.; Allessie, M.A. The Role of Atrial Dilatation in the Domestication of Atrial Fibrillation. Prog. Biophys. Mol. Biol. 2003, 82, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Koca, H.; Demirtas, A.O.; Kaypaklı, O.; Icen, Y.K.; Sahin, D.Y.; Koca, F.; Koseoglu, Z.; Baykan, A.O.; Guler, E.C.; Demirtas, D.; et al. Decreased Left Atrial Global Longitudinal Strain Predicts the Risk of Atrial Fibrillation Recurrence after Cryoablation in Paroxysmal Atrial Fibrillation. J. Interv. Card. Electrophysiol. 2020, 58, 51–59. [Google Scholar] [CrossRef]
- Müller, P.; Weijs, B.; Bemelmans, N.M.A.A.; Mügge, A.; Eckardt, L.; Crijns, H.J.G.M.; Bax, J.J.; Linz, D.; den Uijl, D.W. Echocardiography-Derived Total Atrial Conduction Time (PA-TDI Duration): Risk Stratification and Guidance in Atrial Fibrillation Management. Clin. Res. Cardiol. 2021, 110, 1734–1742. [Google Scholar] [CrossRef] [PubMed]
- Leung, M.; van Rosendael, P.J.; Abou, R.; Ajmone Marsan, N.; Leung, D.Y.; Delgado, V.; Bax, J.J. Left Atrial Function to Identify Patients with Atrial Fibrillation at High Risk of Stroke: New Insights from a Large Registry. Eur. Heart J. 2018, 39, 1416–1425. [Google Scholar] [CrossRef] [Green Version]
- Osranek, M.; Bursi, F.; Bailey, K.R.; Grossardt, B.R.; Brown, R.D.; Kopecky, S.L.; Tsang, T.S.; Seward, J.B. Left Atrial Volume Predicts Cardiovascular Events in Patients Originally Diagnosed with Lone Atrial Fibrillation: Three-Decade Follow-Up. Eur. Heart J. 2005, 26, 2556–2561. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.K.; Anderson, P.L.; Caracciolo, G.; Kiotsekoglou, A.; Wilansky, S.; Govind, S.; Mori, N.; Sengupta, P.P. Global Left Atrial Strain Correlates with CHADS2 Risk Score in Patients with Atrial Fibrillation. J. Am. Soc. Echocardiogr. 2011, 24, 506–512. [Google Scholar] [CrossRef]
- Miyoshi, H.; Mizuguchi, Y.; Oishi, Y.; Iuchi, A.; Nagase, N.; Ara, N.; Oki, T. Early Detection of Abnormal Left Atrial-Left Ventricular-Arterial Coupling in Preclinical Patients with Cardiovascular Risk Factors: Evaluation by Two-Dimensional Speckle-Tracking Echocardiography. Eur. J. Echocardiogr. 2011, 12, 431–439. [Google Scholar] [CrossRef] [Green Version]
- Cameli, M.; Lisi, M.; Focardi, M.; Reccia, R.; Natali, B.M.; Sparla, S.; Mondillo, S. Left Atrial Deformation Analysis by Speckle Tracking Echocardiography for Prediction of Cardiovascular Outcomes. Am. J. Cardiol. 2012, 110, 264–269. [Google Scholar] [CrossRef]
- Lacalzada-Almeida, J.; Izquierdo-Gómez, M.M.; Belleyo-Belkasem, C.; Barrio-Martínez, P.; García-Niebla, J.; Elosua, R.; Jiménez-Sosa, A.; Escobar-Robledo, L.A.; Bayés de Luna, A. Interatrial Block and Atrial Remodeling Assessed Using Speckle Tracking Echocardiography. BMC Cardiovasc. Disord. 2018, 18, 38. [Google Scholar] [CrossRef]
- Müller, P.; Hars, C.; Schiedat, F.; Bösche, L.I.; Gotzmann, M.; Strauch, J.; Dietrich, J.W.; Vogt, M.; Tannapfel, A.; Deneke, T.; et al. Correlation Between Total Atrial Conduction Time Estimated via Tissue Doppler Imaging (PA-TDI Interval), Structural Atrial Remodeling and New-Onset of Atrial Fibrillation After Cardiac Surgery: The Role of Total Atrial Conduction Time in Patients Undergoing Cardiac Surgery. J. Cardiovasc. Electrophysiol. 2013, 24, 626–631. [Google Scholar]
- Abou, R.; Leung, M.; Tonsbeek, A.M.; Podlesnikar, T.; Maan, A.C.; Schalij, M.J.; Ajmone Marsan, N.; Delgado, V.; Bax, J.J. Effect of Aging on Left Atrial Compliance and Electromechanical Properties in Subjects without Structural Heart Disease. Am. J. Cardiol. 2017, 120, 140–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, M.; Abou, R.; van Rosendael, P.J.; van der Bijl, P.; van Wijngaarden, S.E.; Regeer, M.V.; Podlesnikar, T.; Ajmone Marsan, N.; Leung, D.Y.; Delgado, V.; et al. Relation of Echocardiographic Markers of Left Atrial Fibrosis to Atrial Fibrillation Burden. Am. J. Cardiol. 2018, 122, 584–591. [Google Scholar] [CrossRef] [PubMed]
- De Vos, C.B.; Weijs, B.; Crijns, H.J.G.M.; Cheriex, E.C.; Palmans, A.; Habets, J.; Prins, M.H.; Pisters, R.; Nieuwlaat, R.; Tieleman, R.G. Atrial Tissue Doppler Imaging for Prediction of New-Onset Atrial Fibrillation. Heart 2009, 95, 835–840. [Google Scholar] [CrossRef]
- Özlü, M.F.; Erdem, K.; Kırış, G.; Parlar, A.İ.; Demirhan, A.; Ayhan, S.S.; Erdem, A.; Öztürk, S.; Tekelioğlu, Ü.Y.; Yazıcı, M. Predictive Value of Total Atrial Conduction Time Measured with Tissue Doppler Imaging for Postoperative Atrial Fibrillation after Coronary Artery Bypass Surgery. J. Interv. Card. Electrophysiol. 2013, 37, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Müller, P.; Schiedat, F.; Dietrich, J.-W.; Shin, D.-I.; Kara, K.; Mügge, A.; Deneke, T. Reverse Atrial Remodeling in Patients Who Maintain Sinus Rhythm after Electrical Cardioversion: Evidence Derived from the Measurement of Total Atrial Conduction Time Assessed by PA-TDI Interval. J. Echocardiogr. 2014, 12, 142–150. [Google Scholar] [CrossRef] [PubMed]
- den Uijl, D.W.; Delgado, V.; Bertini, M.; Tops, L.F.; Trines, S.A.; van de Veire, N.R.; Zeppenfeld, K.; Schalij, M.J.; Bax, J.J. Impact of Left Atrial Fibrosis and Left Atrial Size on the Outcome of Catheter Ablation for Atrial Fibrillation. Heart 2011, 97, 1847–1851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chao, T.-F.; Lin, Y.-J.; Tsao, H.-M.; Chang, S.-L.; Lo, L.-W.; Hu, Y.-F.; Tuan, T.-C.; Li, C.-H.; Chang, H.-Y.; Wu, T.-J.; et al. Prolonged Atrium Electromechanical Interval Is Associated with Stroke in Patients with Atrial Fibrillation After Catheter Ablation. J. Cardiovasc. Electrophysiol. 2013, 24, 375–380. [Google Scholar] [CrossRef]
- Tjahjadi, C.; Hiemstra, Y.L.; van der Bijl, P.; Pio, S.M.; Bootsma, M.; Ajmone Marsan, N.; Delgado, V.; Bax, J.J. Assessment of Left Atrial Electro-Mechanical Delay to Predict Atrial Fibrillation in Hypertrophic Cardiomyopathy. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 589–596. [Google Scholar] [CrossRef]
- Erdem, F.H.; Erdem, A.; Özlü, F.; Ozturk, S.; Ayhan, S.S.; Çağlar, S.O.; Yazici, M. Electrophysiological Validation of Total Atrial Conduction Time Measurement by Tissue Doppler Echocardiography According to Age and Sex in Healthy Adults. J. Arrhythmia 2016, 32, 127–132. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| P Wave Parameters | Normal Values | Values Related to AF |
|---|---|---|
| P wave duration | <120 ms | ≥120 ms |
| P wave axis | Between 0° and +75° | <0° or >+75° |
| P wave voltage | <2.5 mV in limb leads | ≤0.1 mV in lead I |
| P wave area | <4 ms×mV | ≥4 ms×mV |
| P wave terminal force in lead V1 | ≤0.04 mm×s | >0.04 mm×s |
| P wave dispersion | ≤40 ms | >40 ms |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pozios, I.; Vouliotis, A.I.; Dilaveris, P.; Tsioufis, C. Electro-Mechanical Alterations in Atrial Fibrillation: Structural, Electrical, and Functional Correlates. J. Cardiovasc. Dev. Dis. 2023, 10, 149. https://doi.org/10.3390/jcdd10040149
Pozios I, Vouliotis AI, Dilaveris P, Tsioufis C. Electro-Mechanical Alterations in Atrial Fibrillation: Structural, Electrical, and Functional Correlates. Journal of Cardiovascular Development and Disease. 2023; 10(4):149. https://doi.org/10.3390/jcdd10040149
Chicago/Turabian StylePozios, Iraklis, Apostolos Ilias Vouliotis, Polychronis Dilaveris, and Constantinos Tsioufis. 2023. "Electro-Mechanical Alterations in Atrial Fibrillation: Structural, Electrical, and Functional Correlates" Journal of Cardiovascular Development and Disease 10, no. 4: 149. https://doi.org/10.3390/jcdd10040149