
Deep Learning-Based Automated Quantification of Coronary Artery Calcification for Contrast-Enhanced Coronary Computed Tomographic Angiography

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. CT Image Acquisition
2.3. Reference Calcium Scores
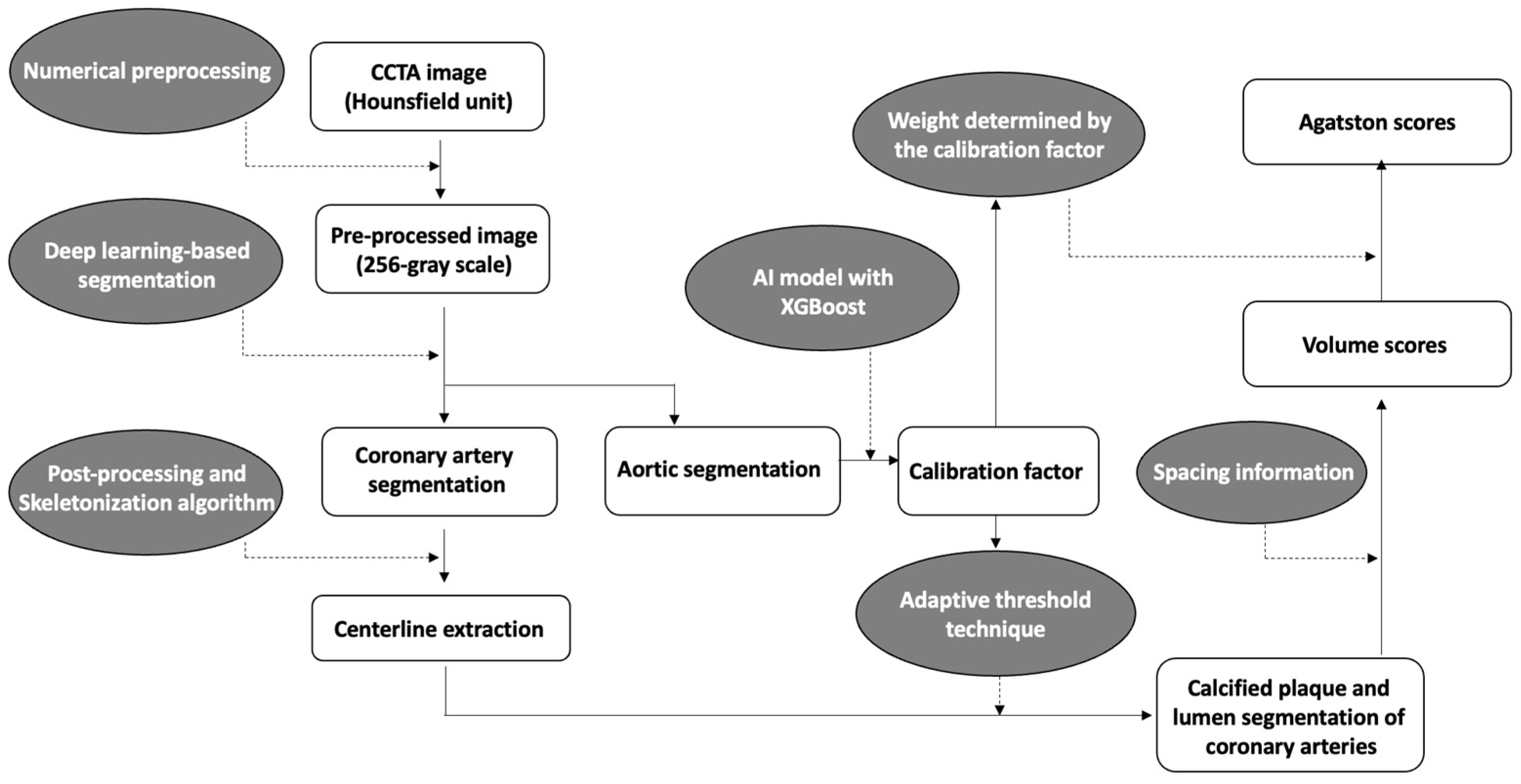
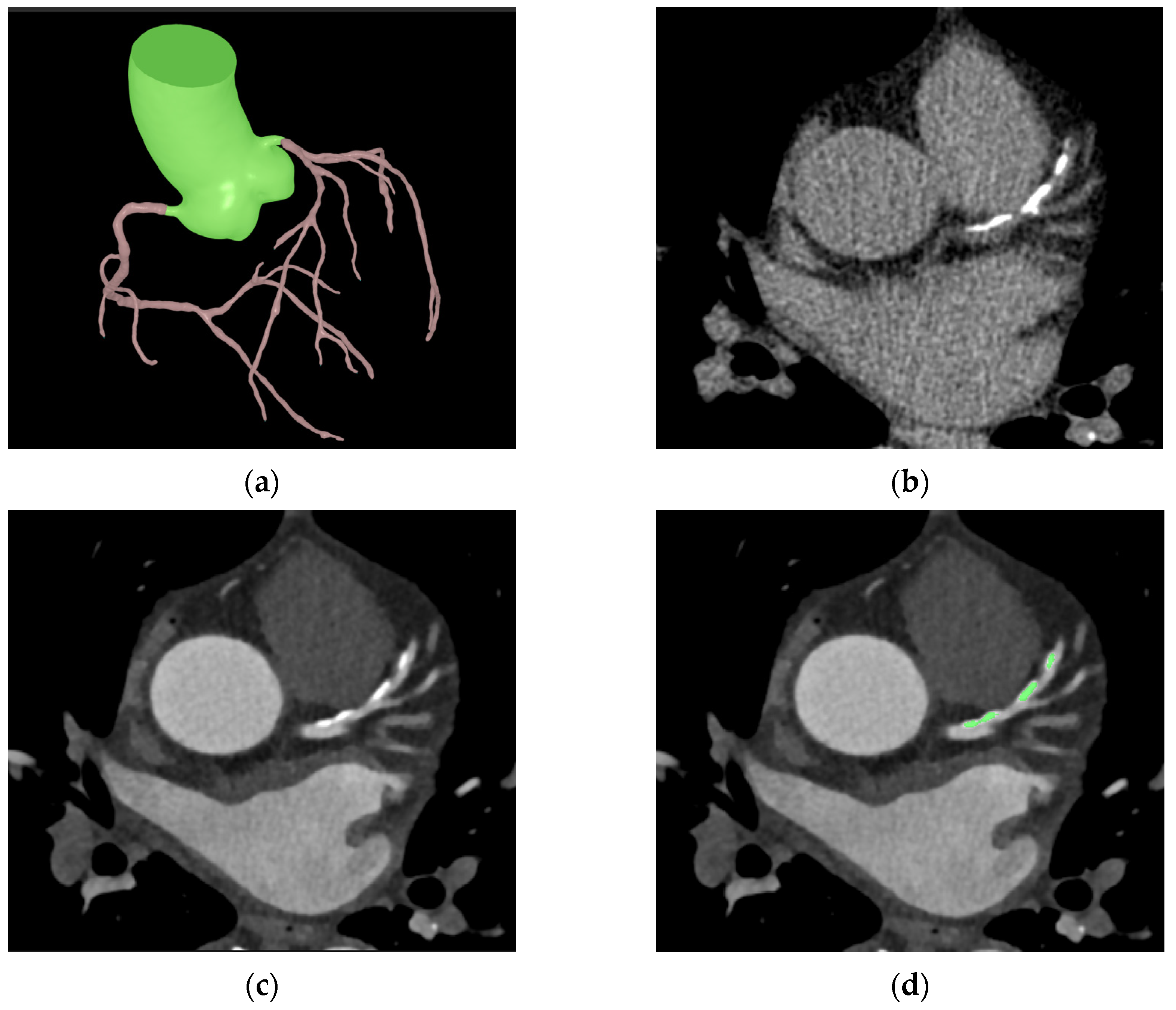
2.4. Automated Extraction and Quantification of Coronary Calcium on Contrast-Enhanced CCTA
2.5. Statistical Analysis
3. Results
3.1. Dataset Characteristics
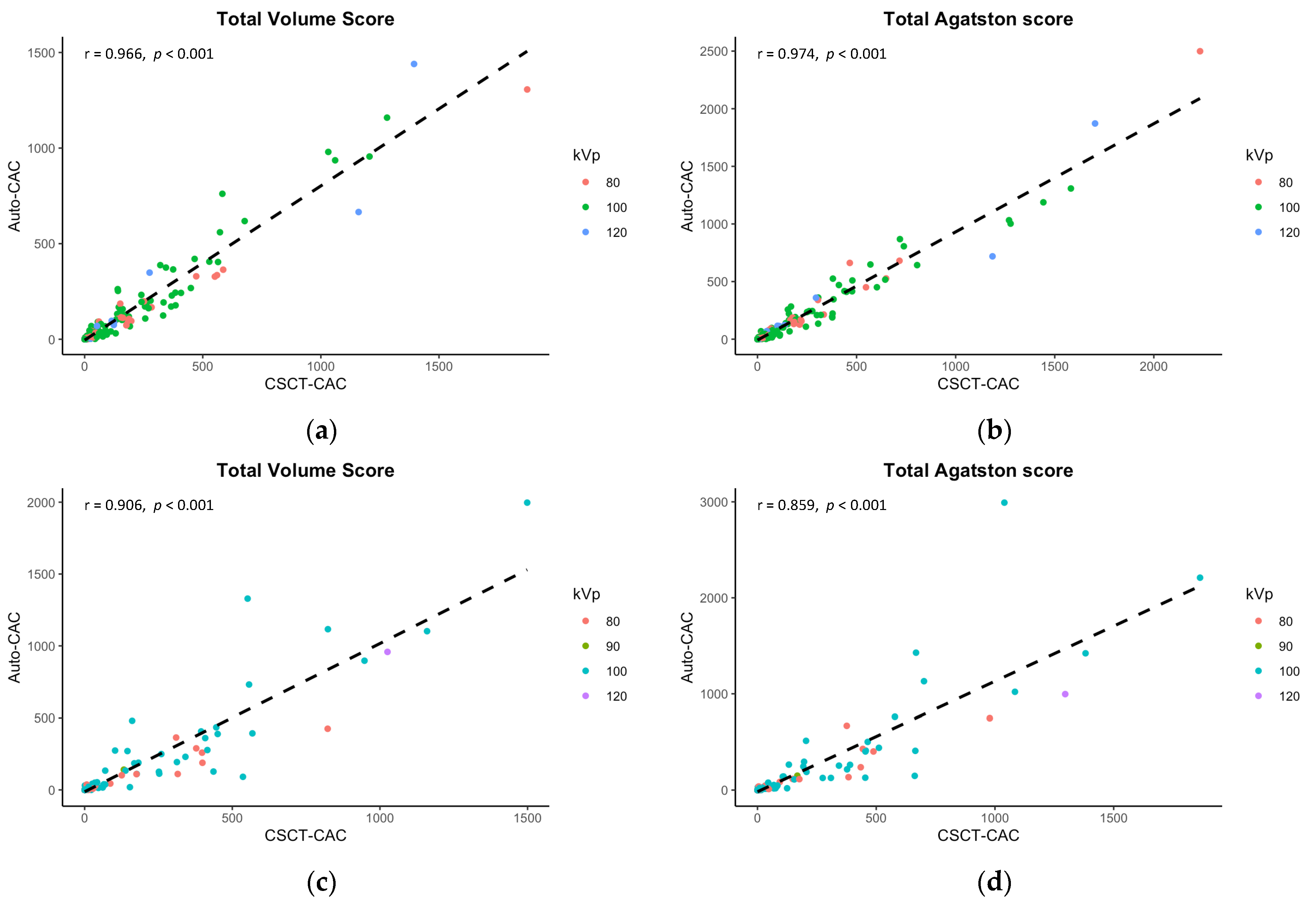
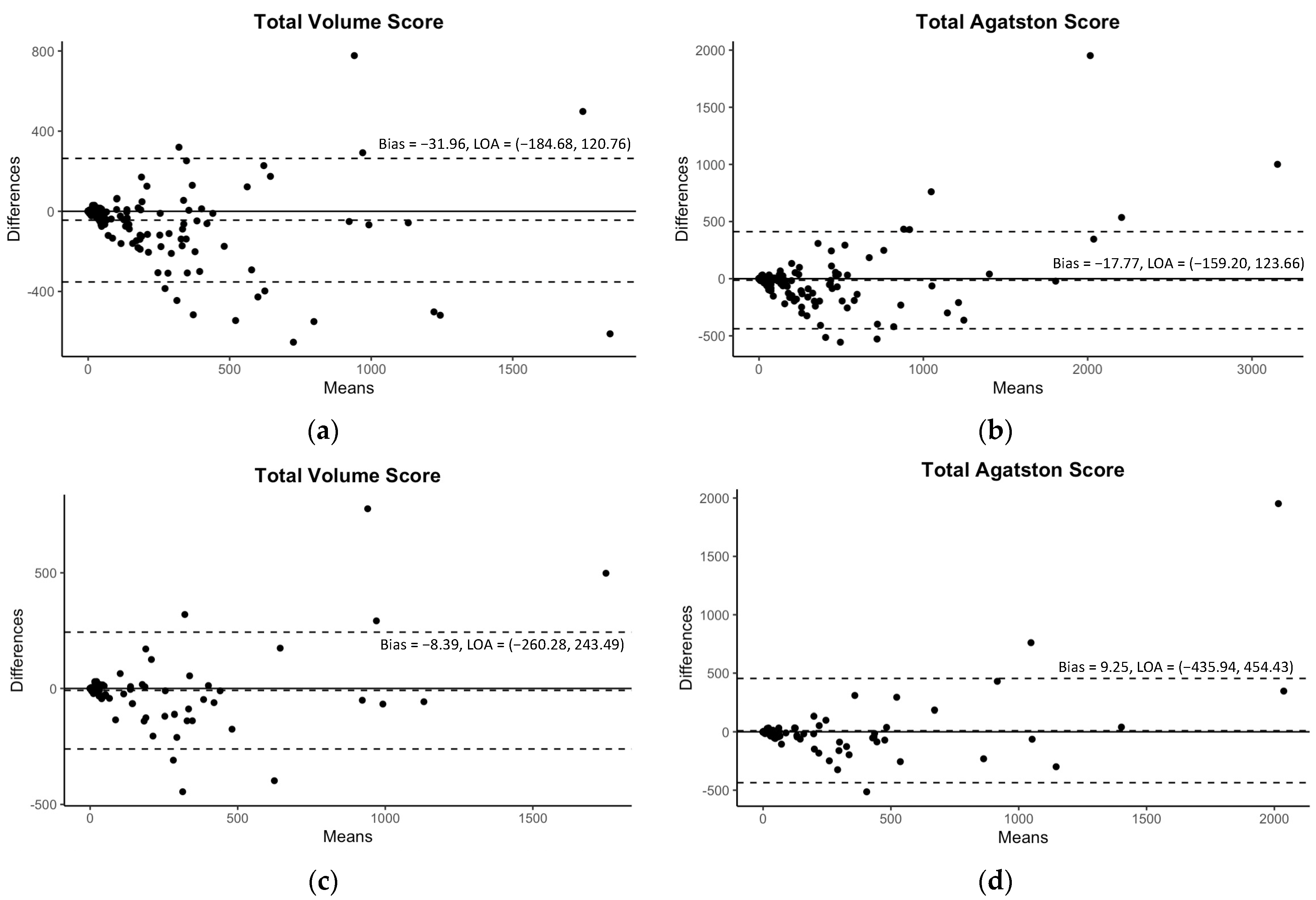
3.2. Performance of Automated Quantification of Coronary Calcium on Contrast-Enhanced CCTA
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Polonsky, T.S. Coronary Artery Calcium Score and Risk Classification for Coronary Heart Disease Prediction. JAMA 2010, 303, 1610. [Google Scholar] [CrossRef] [PubMed]
- Bild, D.E.; Bluemke, D.A.; Burke, G.L.; Detrano, R.; Diez Roux, A.V.; Folsom, A.R.; Greenland, P.; Jacob, D.R., Jr.; Kronmal, R.; Liu, K.; et al. Multi-Ethnic Study of Atherosclerosis: Objectives and Design. Am. J. Epidemiol. 2002, 156, 871–881. [Google Scholar] [CrossRef] [Green Version]
- Schmermund, A.; Möhlenkamp, S.; Stang, A.; Grönemeyer, D.; Seibel, R.; Hirche, H.; Mann, K.; Siffert, W.; Lauterbach, K.; Siegrist, J.; et al. Assessment of clinically silent atherosclerotic disease and established and novel risk factors for predicting myocardial infarction and cardiac death in healthy middle-aged subjects: Rationale and design of the Heinz Nixdorf RECALL Study. Am. Heart. J. 2002, 144, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Shaw, L.J.; Min, J.K.; Nasir, K.; Xie, J.X.; Berman, D.S.; Miedema, M.D.; Whelton, S.P.; Dardari, Z.A.; Rozanski, A.; Rumberger, J.; et al. Sex differences in calcified plaque and long-term cardiovascular mortality: Observations from the CAC Consortium. Eur. Heart J. 2018, 39, 3727–3735. [Google Scholar] [CrossRef] [Green Version]
- Miedema, M.D.; Dardari, Z.A.; Nasir, K.; Blankstein, R.; Knickelbine, T.; Oberembt, S.; Shaw, L.; Rumberger, J.; Michos, E.D.; Rozanski, A.; et al. Association of Coronary Artery Calcium With Long-term, Cause-Specific Mortality Among Young Adults. JAMA Netw. Open 2019, 2, e197440. [Google Scholar] [CrossRef] [PubMed]
- Uddin, S.M.I.; Mirbolouk, M.; Kianoush, S.; Orimoloye, O.A.; Dardari, Z.; Whelton, S.P.; Miedema, M.D.; Nasir, K.; Rumberger, J.A.; Shaw, L.J.; et al. Role of Coronary Artery Calcium for Stratifying Cardiovascular Risk in Adults With Hypertension: The Coronary Artery Calcium Consortium. Hypertension 2019, 73, 983–989. [Google Scholar] [CrossRef] [Green Version]
- Agatston, A.S.; Janowitz, W.R.; Hildner, F.J.; Zusmer, N.R.; Viamonte, M., Jr.; Detrano, R. Quantification of coronary artery calcium using ultrafast computed tomography. J. Am. Coll. Cardiol. 1990, 15, 827–832. [Google Scholar] [CrossRef] [Green Version]
- Newton, T.D.; Mehrez, H.; Wong, K.; Menezes, R.; Wintersperger, B.J.; Crean, A.; Nguyen, E.; Paul, N. Radiation dose threshold for coronary artery calcium score with MDCT: How low can you go? Eur. Radiol. 2011, 21, 2121–2129. [Google Scholar] [CrossRef]
- Baron, K.B.; Choi, A.D.; Chen, M.Y. Low Radiation Dose Calcium Scoring: Evidence and Techniques. Curr. Cardiovasc. Imaging Rep. 2016, 9, 12. [Google Scholar] [CrossRef] [Green Version]
- Marwan, M.; Mettin, C.; Pflederer, T.; Seltmann, M.; Schuhbäck, A.; Muschiol, G.; Ropers, D.; Daniel, W.G.; Achenbach, S. Very low-dose coronary artery calcium scanning with high-pitch spiral acquisition mode: Comparison between 120-kV and 100-kV tube voltage protocols. J. Cardiovasc. Comput. Tomogr. 2013, 7, 32–38. [Google Scholar] [CrossRef]
- Hecht, H.S.; Cronin, P.; Blaha, M.J.; Budoff, M.J.; Kazerooni, E.A.; Narula, J.; Yankelevitz, D.; Abbara, S. 2016 SCCT/STR guidelines for coronary artery calcium scoring of noncontrast noncardiac chest CT scans: A report of the Society of Cardiovascular Computed Tomography and Society of Thoracic Radiology. J. Cardiovasc. Comput. Tomogr. 2017, 11, 74–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, X.; Zhao, Y.; de Bock, G.H.; de Jong, P.A.; Mali, W.P.; Oudkerk, M.; Vliegenthart, R. Validation and Prognosis of Coronary Artery Calcium Scoring in Nontriggered Thoracic Computed Tomography: Systematic Review and Meta-analysis. Circ. Cardiovasc. Imaging 2013, 6, 514–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takx, R.A.; de Jong, P.A.; Leiner, T.; Oudkerk, M.; de Koning, H.J.; Mol, C.P.; Viergever, M.A.; Išgum, I. Automated Coronary Artery Calcification Scoring in Non-Gated Chest CT: Agreement and Reliability. PLoS ONE 2014, 9, e91239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nadjiri, J.; Kaissis, G.; Meurer, F.; Weis, F.; Laugwitz, K.L.; Straeter, A.S.; Muenzel, D.; Noël, P.B.; Rummeny, E.J.; Rasper, M. Accuracy of Calcium Scoring calculated from contrast-enhanced Coronary Computed Tomography Angiography using a dual-layer spectral CT: A comparison of Calcium Scoring from real and virtual non-contrast data. PLoS ONE 2018, 13, e0208588. [Google Scholar] [CrossRef] [PubMed]
- Otton, J.M.; Lønborg, J.T.; Boshell, D.; Feneley, M.; Hayen, A.; Sammel, N.; Sesel, K.; Bester, L.; McCrohon, J. A method for coronary artery calcium scoring using contrast-enhanced computed tomography. J. Cardiovasc. Comput. Tomogr. 2012, 6, 37–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubinshtein, R.; Halon, D.A.; Gaspar, T.; Lewis, B.S.; Peled, N. Automatic Assessment of Coronary Artery Calcium Score from Contrast-Enhanced 256-Row Coronary Computed Tomography Angiography. Am. J. Cardiol. 2014, 113, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Ebersberger, U.; Eilot, D.; Goldenberg, R.; Lev, A.; Spears, J.R.; Rowe, G.W.; Gallagher, N.Y.; Halligan, W.T.; Blanke, P.; Makowski, M.R.; et al. Fully automated derivation of coronary artery calcium scores and cardiovascular risk assessment from contrast medium-enhanced coronary CT angiography studies. Eur. Radiol. 2013, 23, 650–657. [Google Scholar] [CrossRef]
- Mylonas, I.; Alam, M.; Amily, N.; Small, G.; Chen, L.; Yam, Y.; Hibbert, B.; Chow, B.J. Quantifying coronary artery calcification from a contrast-enhanced cardiac computed tomography angiography study. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 210–215. [Google Scholar] [CrossRef] [Green Version]
- Wolterink, J.M.; Leiner, T.; de Vos, B.D.; van Hamersvelt, R.W.; Viergever, M.A.; Išgum, I. Automatic coronary artery calcium scoring in cardiac CT angiography using paired convolutional neural networks. Med. Image Anal. 2016, 34, 123–136. [Google Scholar] [CrossRef]
- Ahmed, W.; de Graaf, M.A.; Broersen, A.; Kitslaar, P.H.; Oost, E.; Dijkstra, J.; Bax, J.J.; Reiber, J.H.; Scholte, A.J. Automatic detection and quantification of the Agatston coronary artery calcium score on contrast computed tomography angiography. Int. J. Cardiovasc. Imaging 2015, 31, 151–161. [Google Scholar] [CrossRef]
- Schuhbaeck, A.; Otaki, Y.; Achenbach, S.; Schneider, C.; Slomka, P.; Berman, D.S.; Dey, D. Coronary calcium scoring from contrast coronary CT angiography using a semiautomated standardized method. J. Cardiovasc. Comput. Tomogr. 2015, 9, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Eilot, D.; Goldenberg, R. Fully automatic model-based calcium segmentation and scoring in coronary CT angiography. Int. J. Comput. Assist. Radiol. Surg. 2014, 9, 595–608. [Google Scholar] [CrossRef]
- Bischoff, B.; Kantert, C.; Meyer, T.; Hadamitzky, M.; Martinoff, S.; Schömig, A.; Hausleiter, J. Cardiovascular risk assessment based on the quantification of coronary calcium in contrast-enhanced coronary computed tomography angiography. Eur. Heart J. Cardiovasc. Imaging 2012, 13, 468–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Bijl, N.; Joemai, R.M.; Geleijns, J.; Bax, J.J.; Schuijf, J.D.; de Roos, A.; Kroft, L.J. Assessment of Agatston Coronary Artery Calcium Score Using Contrast-Enhanced CT Coronary Angiography. Am. J. Roentgenol. 2010, 195, 1299–1305. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Kitslaar, P.; Frenay, M.; Broersen, A.; Boogers, M.J.; Bax, J.J.; Reiber, J.H.; Dijkstra, J. Automatic centerline extraction of coronary arteries in coronary computed tomographic angiography. Int. J. Cardiovasc. Imaging 2012, 28, 921–933. [Google Scholar] [CrossRef] [Green Version]
- Callister, T.Q.; Cooil, B.; Raya, S.P.; Lippolis, N.J.; Russo, D.J.; Raggi, P. Coronary artery disease: Improved reproducibility of calcium scoring with an electron-beam CT volumetric method. Radiology 1998, 208, 807–814. [Google Scholar] [CrossRef]
- Reynolds, D. Gaussian Mixture Models. In Encyclopedia of Biometrics; Li, S.Z., Jain, A., Eds.; Springer: Boston, MA, USA, 2009; pp. 659–663. [Google Scholar]
- Moon, T.K. The expectation-maximization algorithm. IEEE Signal. Process. Mag. 1996, 13, 47–60. [Google Scholar] [CrossRef]
- Lefkimmiatis, S.; Bourquard, A. Unser M Hessian-Based Norm Regularization for Image Restoration With Biomedical Applications. IEEE Trans. Image Process. 2012, 21, 983–995. [Google Scholar] [CrossRef] [Green Version]
- Milletari, F.; Navab, N.; Ahmadi, S.-A. V-Net: Fully Convolutional Neural Networks for Volumetric Medical Image Segmentation. In Proceedings of the 2016 Fourth International Conference on 3D Vision (3DV), Stanford, CA, USA, 25–28 October 2016; IEEE: Stanford, CA, USA, 2016; pp. 565–571. [Google Scholar]
- Chen, L.-C.; Zhu, Y.; Papandreou, G.; Schroff, F.; Adam, H. Encoder-Decoder with Atrous Separable Convolution for Semantic Image Segmentation. In Computer Vision–ECCV 2018; Ferrari, V., Hebert, M., Sminchisescu, C., Weiss, Y., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 833–851. [Google Scholar]
- Chen, T.; Guestrin, C. XGBoost: A Scalable Tree Boosting System. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; ACM: San Francisco, CA, USA, 2016; pp. 785–794. [Google Scholar]
- Pudney, C. Distance-Ordered Homotopic Thinning: A Skeletonization Algorithm for 3D Digital Images. Comput. Vis. Image Underst. 1998, 72, 404–413. [Google Scholar] [CrossRef]
- Lin, L.I.-K. A Concordance Correlation Coefficient to Evaluate Reproducibility. Biometrics 1989, 45, 255. [Google Scholar] [CrossRef]
- Cohen, J.A. Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villines, T.C.; Hulten, E.A.; Shaw, L.J.; Goyal, M.; Dunning, A.; Achenbach, S.; Al-Mallah, M.; Berman, D.S.; Budoff, M.J.; Cademartiri, F.; et al. Prevalence and Severity of Coronary Artery Disease and Adverse Events Among Symptomatic Patients With Coronary Artery Calcification Scores of Zero Undergoing Coronary Computed Tomography Angiography. J. Am. Coll. Cardiol. 2011, 58, 2533–2540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolk, M.J.; Bailey, S.R.; Doherty, J.U.; Douglas, P.S.; Hendel, R.C.; Kramer, C.M.; Min, J.K.; Patel, M.R.; Rosenbaum, L.; Shaw, L.J.; et al. ACCF/AHA/ASE/ASNC/HFSA/HRS/SCAI/SCCT/SCMR/STS 2013 Multimodality Appropriate Use Criteria for the Detection and Risk Assessment of Stable Ischemic Heart Disease. J. Am. Coll. Cardiol. 2014, 63, 380–406. [Google Scholar] [CrossRef] [Green Version]
- Tay, S.Y.; Chang, P.Y.; Lao, W.T.; Lin, Y.C.; Chung, Y.H.; Chan, W.P. The proper use of coronary calcium score and coronary computed tomography angiography for screening asymptomatic patients with cardiovascular risk factors. Sci. Rep. 2017, 7, 17653. [Google Scholar] [CrossRef] [Green Version]
- Hou, Z.; Lu, B.; Gao, Y.; Jiang, S.; Wang, Y.; Li, W.; Budoff, M.J. Prognostic Value of Coronary CT Angiography and Calcium Score for Major Adverse Cardiac Events in Outpatients. JACC Cardiovasc. Imaging 2012, 5, 990–999. [Google Scholar] [CrossRef] [Green Version]
- Mühlenbruch, G.; Wildberger, J.E.; Koos, R.; Das, M.; Flohr, T.G.; Niethammer, M.; Weiss, C.; Günther, R.W.; Mahnken, A.H. Coronary Calcium Scoring Using 16-Row Multislice Computed Tomography: Nonenhanced Versus Contrast-Enhanced Studies In Vitro and In Vivo. Investg. Radiol. 2005, 40, 148–154. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Internal Validation Set (n = 200) | External Validation Set (n = 115) |
|---|---|---|
| Sex | ||
| Women, n (%) | 66 (33) | 45 (39.1) |
| Men, n (%) | 134 (67) | 70 (60.9) |
| Age (years), mean ± SD | 62.5 ± 8.57 | 62.4 ± 8.77 |
| Body mass index (kg/m2), mean ± SD | 24.5 ± 3.28 | 24.7 ± 3.06 |
| Hypertension, n (%) | 101 (50.5) | 57 (49.6) |
| Diabetes, n (%) | 64 (32) | 28 (24.3) |
| Hyperlipidemia, n (%) | 136 (68) | 56 (48.7) |
| Family history of MI, n (%) | 16 (8) | 4 (3.5) |
| Smoking history | ||
| Smokers, n (%) | 32 (16) | 17 (14.8) |
| Ex-smokers, > 1 month, n (%) | 64 (32) | 32 (27.8) |
| Non-smokers, n (%) | 104 (52) | 66 (57.4) |
| Heart rate (beat/min), mean ± SD | 62.3 ± 9.37 | 65.2 ± 11.24 |
| Internal Validation | |||||||
| Comparison | Correlation | Agreement | |||||
| Parameters | CSCT * | Auto-CAC * | p value | r † | p value | CCC | 95% CI |
| Overall | |||||||
| Volume score | 142.12 ± 267.4 | 110.16 ± 224.2 | <0.001 | 0.966 | <0.001 | 0.942 | 0.928, 0.954 |
| Agatston score | 159.83 ± 316.8 | 142.06 ± 306.6 | <0.001 | 0.974 | <0.001 | 0.972 | 0.963, 0.978 |
| LCA | |||||||
| Volume score | 102.22 ± 191.9 | 82.78 ± 176.6 | <0.001 | 0.956 | <0.001 | 0.947 | 0.931, 0.959 |
| Agatston score | 117.15 ± 230.4 | 105.40 ± 226.6 | 0.007 | 0.965 | <0.001 | 0.963 | 0.952, 0.972 |
| RCA | |||||||
| Volume score | 39.43 ± 112.8 | 27.38 ± 84.0 | <0.001 | 0.952 | <0.001 | 0.904 | 0.884, 0.921 |
| Agatston score | 43.14 ± 132.9 | 36.66 ± 137.6 | 0.007 | 0.970 | <0.001 | 0.968 | 0.958, 0.976 |
| External validation | |||||||
| Comparison | Correlation | Agreement | |||||
| Parameters | CSCT * | Auto-CAC * | p value | r † | p value | CCC | 95% CI |
| Overall | |||||||
| Volume score | 150.63 ± 267.5 | 142.24 ± 303.7 | 0.48 | 0.906 | <0.001 | 0.898 | 0.859, 0.928 |
| Agatston score | 178.22 ± 324.7 | 187.46 ± 433.9 | 0.66 | 0.859 | <0.001 | 0.824 | 0.765, 0.869 |
| LCA | |||||||
| Volume score | 98.76 ± 182.9 | 94.35 ± 196.6 | 0.46 | 0.947 | <0.001 | 0.944 | 0.921, 0.961 |
| Agatston score | 119.6 ± 227.3 | 129.4 ± 342.7 | 0.60 | 0.826 | <0.001 | 0.761 | 0.691, 0.817 |
| RCA | |||||||
| Volume score | 51.87 ± 126.9 | 47.89 ± 156.7 | 0.62 | 0.835 | <0.001 | 0.817 | 0.750, 0.867 |
| Agatston score | 58.62 ± 151.5 | 58.02 ± 185.6 | 0.94 | 0.896 | <0.001 | 0.877 | 0.832, 0.911 |
| Internal Validation | |||||||
| Comparison | Correlation | Agreement | |||||
| Parameters | CSCT * | Auto-CAC * | p value | r † | p value | CCC | 95% CI |
| 80 kVp (n = 48) | |||||||
| Volume score | 141.80 ± 297.6 | 93.69 ± 203.7 | 0.001 | 0.993 | <0.001 | 0.910 | 0.883, 0.930 |
| Agatston score | 161.50 ± 350.8 | 151.59 ± 383.7 | 0.27 | 0.990 | <0.001 | 0.985 | 0.976, 0.991 |
| 100 kVp (n = 137) | |||||||
| Volume score | 131.78 ± 231.3 | 106.05 ± 205.2 | <0.001 | 0.969 | <0.001 | 0.956 | 0.941, 0.967 |
| Agatston score | 148.13 ± 277.8 | 127.56 ± 243.6 | <0.001 | 0.977 | <0.001 | 0.965 | 0.954, 0.974 |
| 120 kVp (n = 13) | |||||||
| Volume score | 252.25 ± 464.1 | 214.32 ± 415.1 | 0.35 | 0.955 | <0.001 | 0.945 | 0.842, 0.981 |
| Agatston score | 276.99 ± 535.5 | 259.74 ± 526.0 | 0.67 | 0.964 | <0.001 | 0.963 | 0.884, 0.988 |
| External validation | |||||||
| Comparison | Correlation | Agreement | |||||
| Parameters | CSCT * | Auto-CAC * | p value | r † | p value | CCC | 95% CI |
| 80 kVp (n = 23) | |||||||
| Volume score | 135.29 ± 209.8 | 85.77 ± 129.7 | 0.009 | 0.929 | <0.001 | 0.798 | 0.673, 0.878 |
| Agatston score | 157.77 ± 248.8 | 131.85 ± 219.9 | 0.05 | 0.908 | <0.001 | 0.896 | 0.778, 0.952 |
| 100 kVp (n = 85) | |||||||
| Volume score | 149.73 ± 272.0 | 152.66 ± 330.3 | 0.08 | 0.915 | <0.001 | 0.898 | 0.853, 0.929 |
| Agatston score | 176.84 ± 329.2 | 199.75 ± 478.0 | 0.17 | 0.866 | <0.001 | 0.808 | 0.740, 0.860 |
| Internal validation | ||||||
| No. of patients in each risk classification by CAC Score from CSCT | ||||||
| 0 | 1–10 | 11–100 | 101–400 | >400 | ||
| No. of patients by auto-CAC | 0 | 46 | 5 | 0 | 0 | 0 |
| 1–10 | 0 | 15 | 6 | 0 | 0 | |
| 11–100 | 0 | 1 | 60 | 3 | 0 | |
| 101–400 | 0 | 0 | 0 | 39 | 0 | |
| >400 | 0 | 0 | 0 | 1 | 22 | |
| External validation | ||||||
| No. of patients in each risk classification by CAC score from CSCT | ||||||
| 0 | 1–10 | 11–100 | 101–400 | >400 | ||
| No. of patients by auto-CAC | 0 | 27 | 4 | 1 | 0 | 0 |
| 1–10 | 0 | 17 | 0 | 0 | 0 | |
| 11–100 | 0 | 5 | 21 | 1 | 0 | |
| 101–400 | 0 | 0 | 0 | 16 | 3 | |
| >400 | 0 | 0 | 0 | 2 | 16 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.O.; Park, E.-A.; Park, D.; Lee, W. Deep Learning-Based Automated Quantification of Coronary Artery Calcification for Contrast-Enhanced Coronary Computed Tomographic Angiography. J. Cardiovasc. Dev. Dis. 2023, 10, 143. https://doi.org/10.3390/jcdd10040143
Lee JO, Park E-A, Park D, Lee W. Deep Learning-Based Automated Quantification of Coronary Artery Calcification for Contrast-Enhanced Coronary Computed Tomographic Angiography. Journal of Cardiovascular Development and Disease. 2023; 10(4):143. https://doi.org/10.3390/jcdd10040143
Chicago/Turabian StyleLee, Jung Oh, Eun-Ah Park, Daebeom Park, and Whal Lee. 2023. "Deep Learning-Based Automated Quantification of Coronary Artery Calcification for Contrast-Enhanced Coronary Computed Tomographic Angiography" Journal of Cardiovascular Development and Disease 10, no. 4: 143. https://doi.org/10.3390/jcdd10040143