

IABP versus Impella Support in Cardiogenic Shock: “In Silico” Study
 , , and
, , and
Abstract
:1. Introduction
- ✓
- Intra-aortic balloon pump (IABP), consisting of a balloon positioned in the descending thoracic aorta that inflates (diastole) and deflates (systole) leading to an increase in coronary perfusion and a reduction in afterload;
- ✓
- Impella 2.5 [3], a coaxial pump that is retrogradely advanced in the aortic transvalvular position and works by aspirating blood from the left ventricle to expel it directly into the ascending aorta. This pump can deliver a flow of up to 2.5 L per minute;
- ✓
- Extracorporeal membrane oxygenation (ECMO), which can simultaneously provide mechanical support for the heart and oxygenation of the lungs.
2. Materials and Methods
2.1. The Cardiovascular and Heart Numerical Models
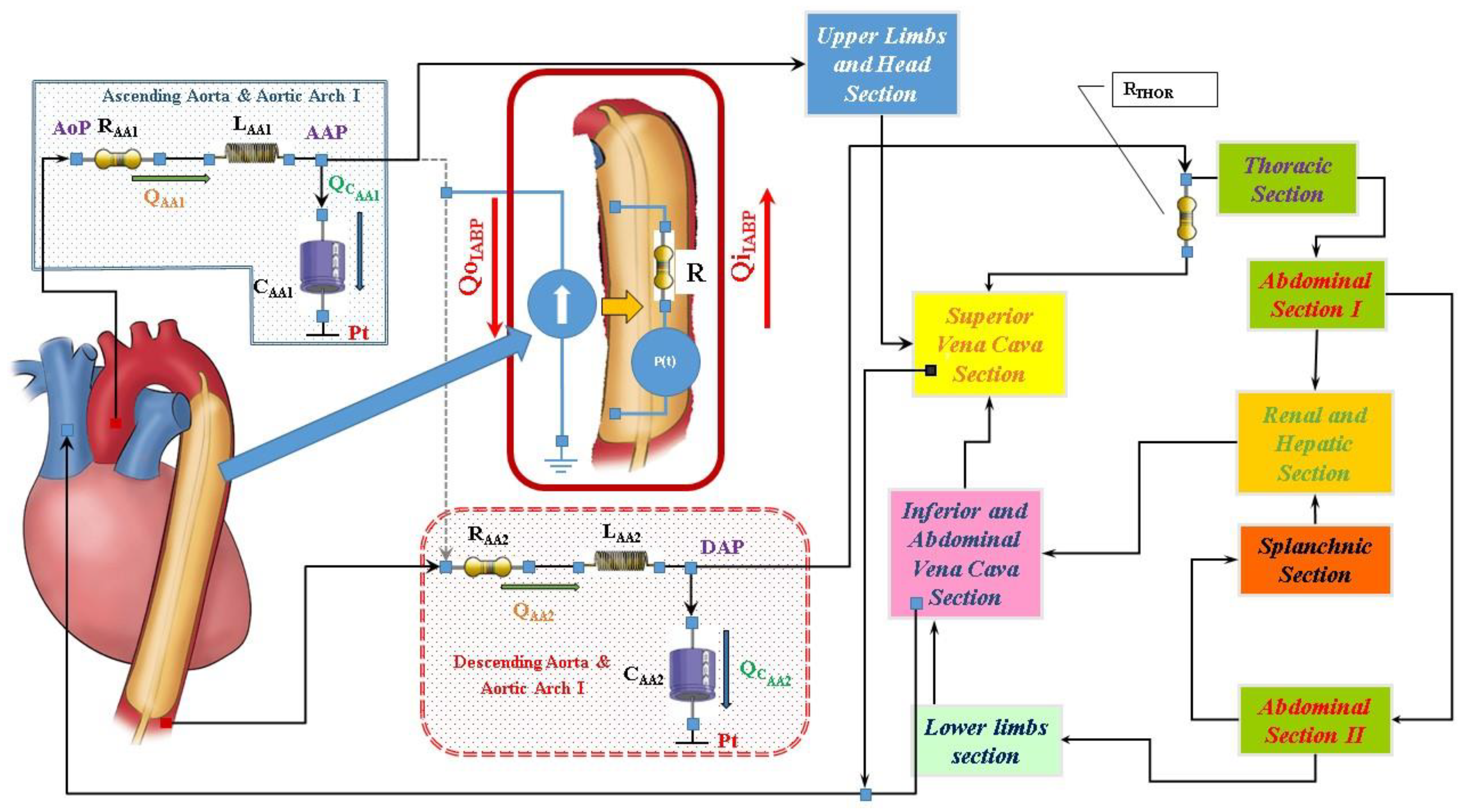
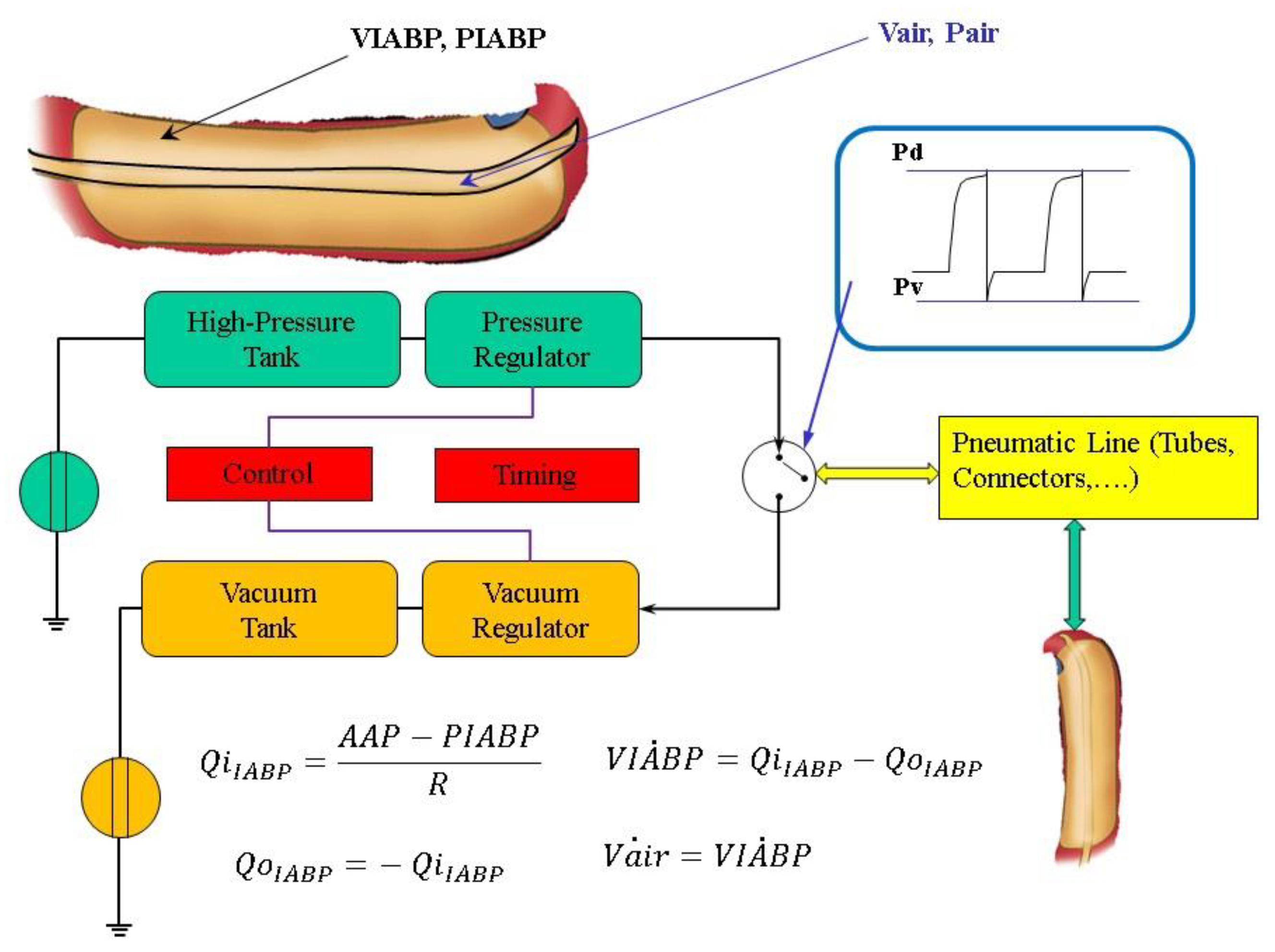
2.2. Intra-Aortic Balloon Pump Numerical Model
- the balloon inflates in diastole and the flow is positive;
- the balloon deflates in the following systole and the flow is negative.
- the air outflow from the high-pressure tank connected to the pressure source;
- the air outflow from the lower-pressure tank connected to the vacuum source (Figure 2).
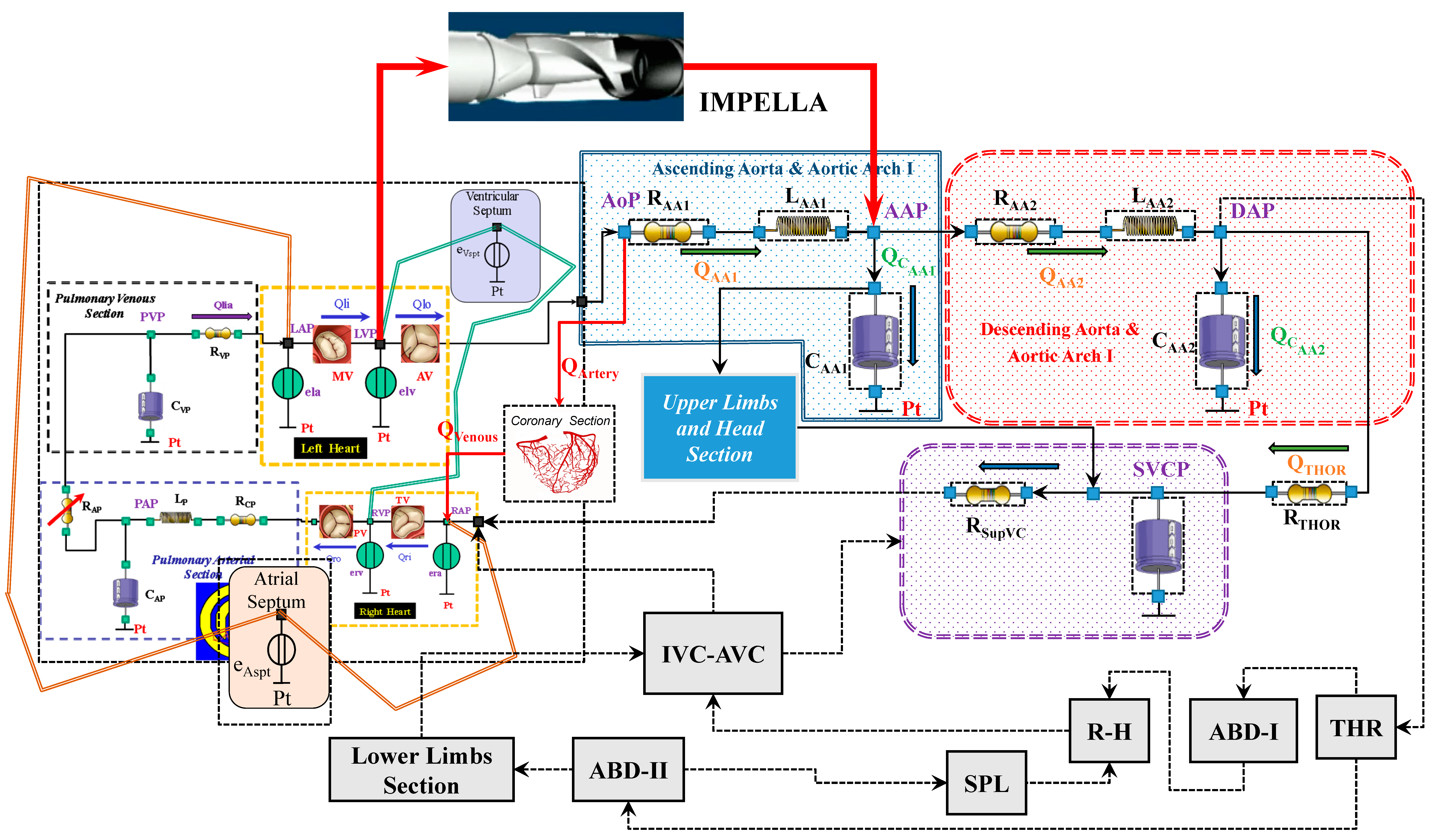
2.3. Impella 2.5 Numerical Model
2.4. Simulation Protocol
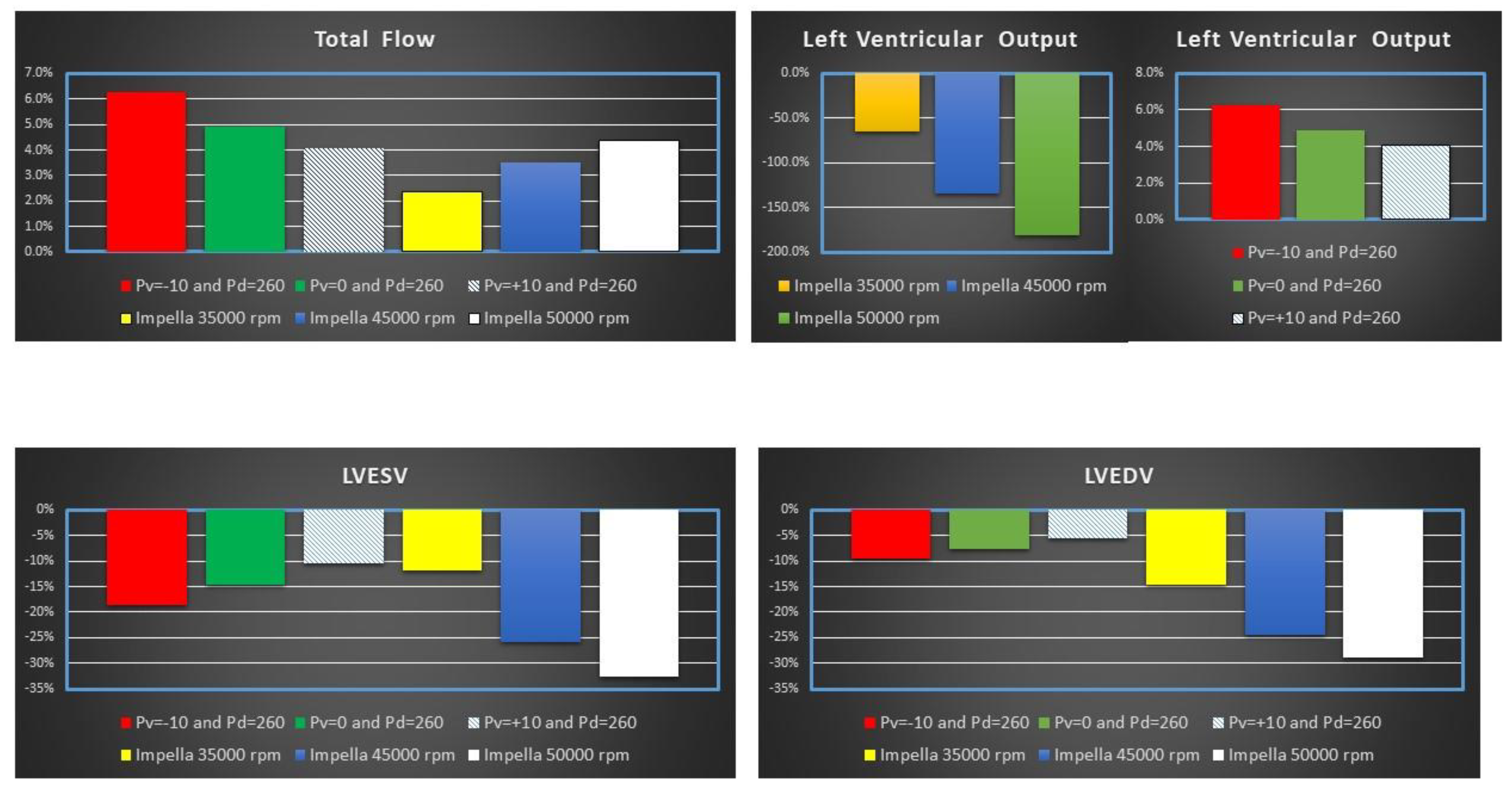
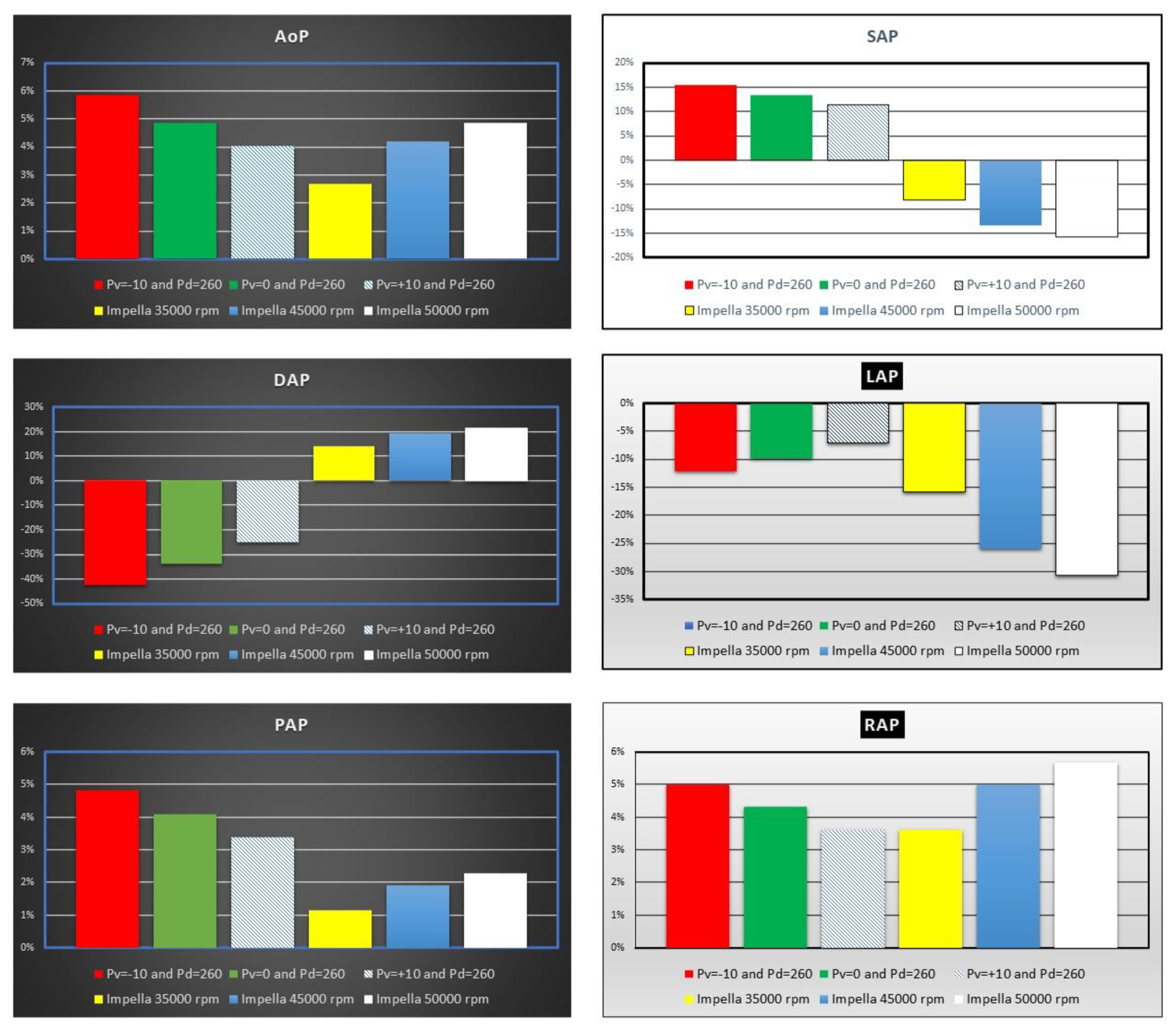
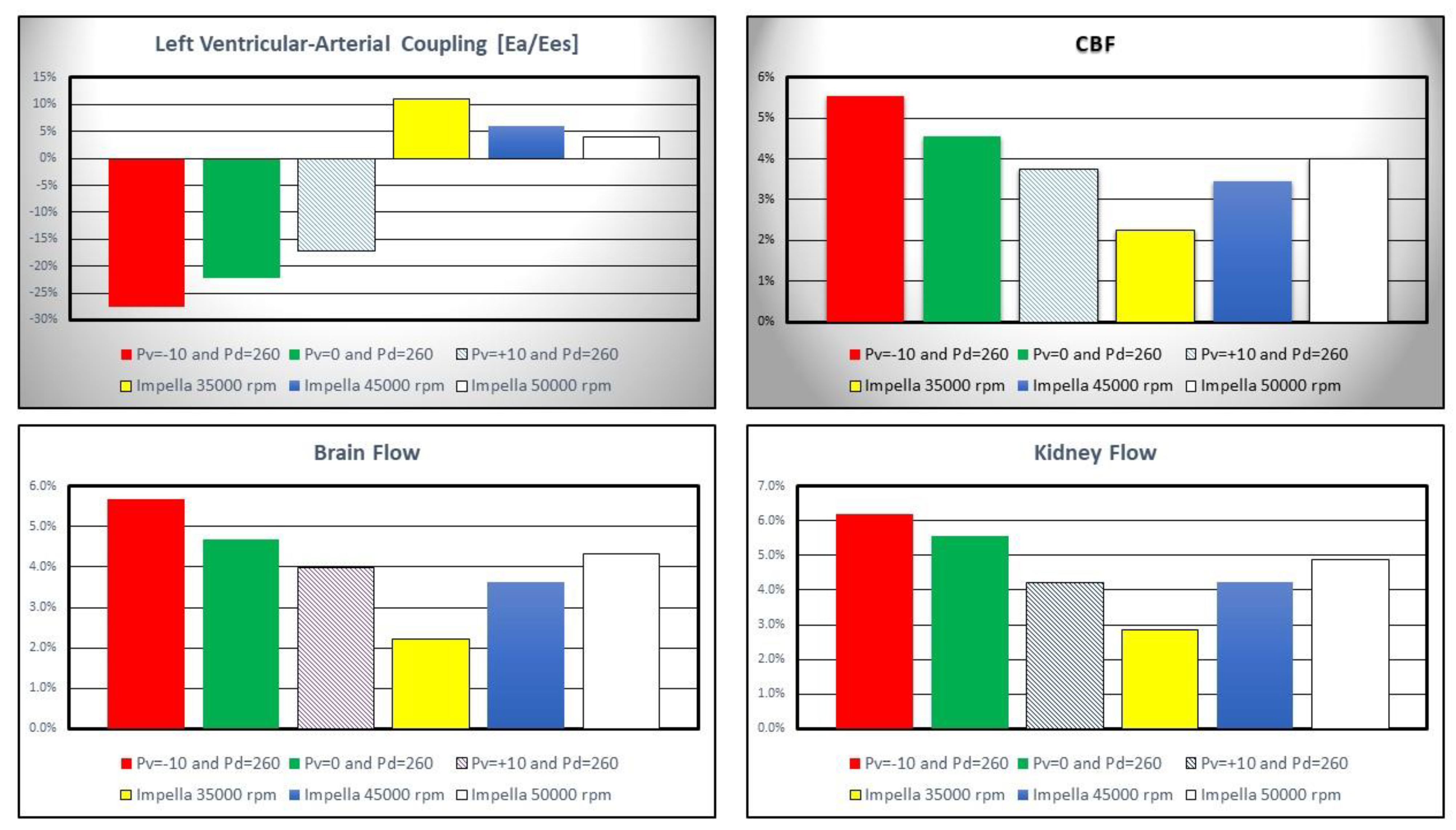
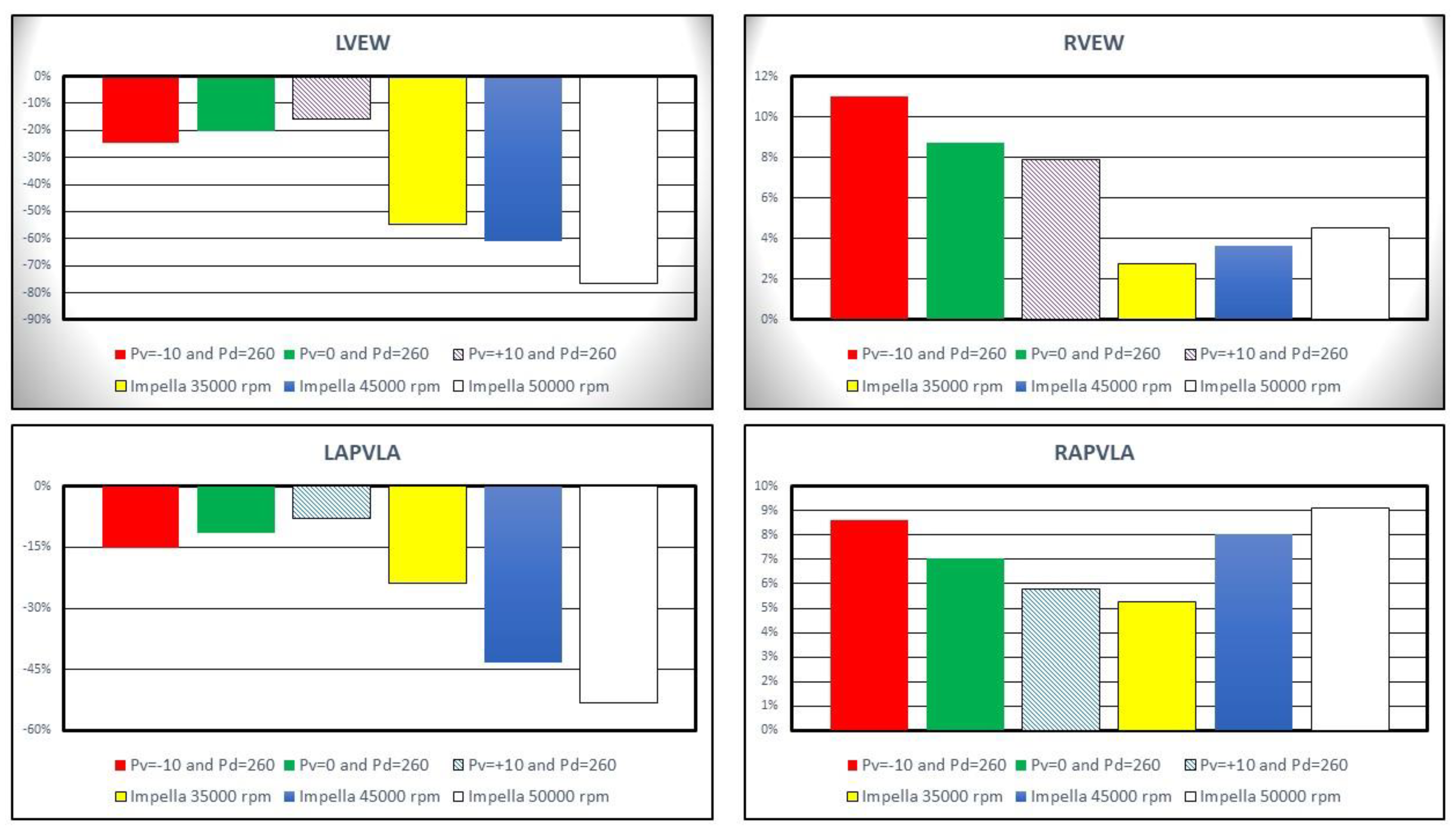
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Katz, A.M. Physiology of the Heart, 4th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006; pp. 209–210. [Google Scholar]
- Schurtz, G.; Rousse, N.; Saura, O.; Balmette, V.; Vincent, F.; Lamblin, N.; Porouchani, S.; Verdier, B.; Puymirat, E.; Robin, E.; et al. IMPELLA® or Extracorporeal Membrane Oxygenation for Left Ventricular Dominant Refractory Cardiogenic Shock. J. Clin. Med. 2021, 10, 759. [Google Scholar] [CrossRef] [PubMed]
- Abiomed, Inc. Impella® Recover® LP 2.5 System-U Instruction for Use; Abiomed, Inc.: Danvers, MA, USA, 2006. [Google Scholar]
- Frain, K.; Rees, P. Intra-aortic balloon pump versus percutaneous Impella© in emergency revascularisation for myocardial infarction and cardiogenic shock: Systematic review. Perfusion 2021. [Google Scholar] [CrossRef] [PubMed]
- Ouweneel, D.M.; Engstrom, A.E.; Sjauw, K.D.; Hirsch, A.; Hill, J.M.; Gockel, B.; Tuseth, V.; van der Schaaf, R.J.; Henriques, J.P.S. Experience from a randomized controlled trial with Impella 2.5 versus IABP in STEMI patients with cardiogenic pre-shock. Lessons learned from the IMPRESS in STEMI trial. Int. J. Cardiol. 2016, 202, 894–896. [Google Scholar] [CrossRef] [PubMed]
- Pieri, M.; Sorrentino, T.; Oppizzi, M.; Melisurgo, G.; Lembo, R.; Colombo, A.; Zangrillo, A.; Pappalardo, F. The role of different mechanical circulatory support devices and their timing of implantation on myocardial damage and mid-term recovery in acute myocardial infarction related cardiogenic shock. J. Interv. Cardiol. 2018, 31, 717–724. [Google Scholar] [CrossRef]
- De Lazzari, B.; Iacovoni, A.; Mottaghy, K.; Capoccia, M.; Badagliacca, R.; Vizza, C.D.; De Lazzari, C. ECMO Assistance During Mechanical Ventilation: Effects Induced on Energetic and Haemodynamic Variables. Comput. Methods Programs Biomed. 2021, 202, 106003. [Google Scholar] [CrossRef] [PubMed]
- De Lazzari, C. Interaction between the septum and the left (right) ventricular free wall in order to evaluate the effects on coronary blood flow: Numerical simulation. Comput. Methods Biomech. Biomed. Eng. 2012, 15, 1359–1368. [Google Scholar] [CrossRef] [PubMed]
- De Lazzari, B.; Iacovoni, A.; Capoccia, M.; Papa, S.; Badagliacca, R.; Filomena, D.; De Lazzari, C. Ventricular and Atrial Pressure—Volume Loops: Analysis of the Effects Induced by Right Centrifugal Pump Assistance. Bioengineering 2022, 9, 181. [Google Scholar] [CrossRef]
- Capoccia, M.; Marconi, S.; Singh, S.A.; Pisanelli, M.D.; De Lazzari, C. Simulation as a preoperative planning approach in advanced heart failure patients. A retrospective clinical analysis. BioMed. Eng. Online 2018, 17, 52. [Google Scholar]
- De Lazzari, C.; De Lazzari, B.; Iacovoni, A.; Marconi, S.; Papa, S.; Capoccia, M.; Badagliacca, R.; Vizza, C.D. Intra-Aortic Balloon Counterpulsation Timing: A New Numerical Model for Programming and Training in the Clinical Environment. Comput. Methods Programs Biomed. 2020, 194, 105537. [Google Scholar] [CrossRef]
- De Lazzari, C.; Stalteri, D. 2011–2019, CARDIOSIM© Website. Original Website Platform Regarding the Implementation of the Cardiovascular Software Simulator CARDIOSIM©. Available online: https://cardiosim.dsb.cnr.it/CirculatoryNetworks/fcn/fcn10 (accessed on 6 November 2022).
- De Lazzari, C.; Stalteri, D. 2011–2019, CARDIOSIM© Website. Original Website Platform Regarding the Implementation of the Cardiovascular Software Simulator CARDIOSIM©. Available online: https://cardiosim.dsb.cnr.it/CirculationModels/ncm2#ncm2 (accessed on 6 November 2022).
- De Lazzari, C. Coronary circulation models. In Modelling Cardiovascular System and Mechanical Circulatory Support; De Lazzari, C., Ed.; Consiglio Nazionale delle Ricerche (CNR): Roma, Italy, 2007; ISBN 978-88-8080-081-1. [Google Scholar]
- Jaron, D.; More, T.W.; He, P. Theoretical considerations regarding the optimization of cardiac assistance by intra-aortic balloon pumping. IEEE Tran. Biolog. Med. Eng. 1983, 30, 177–186. [Google Scholar] [CrossRef]
- Jaron, D.; More, T.W.; He, P. Control of intra-aortic balloon pumping: Theory and guidelines for clinical applications. Ann. Biomed. Eng. 1985, 13, 155–175. [Google Scholar] [CrossRef]
- Darowski, M.; De Lazzari, C.; Ferrari, G.; Clemente, F.; Guaragno, M. The influence of simultaneous intraaortic balloon pumping and mechanical ventilation on hemodynamic parameters—Numerical simulation. Front. Med. Biol. Eng. 1999, 9, 155–174. [Google Scholar] [PubMed]
- De Lazzari, C.; Darowski, M.; Ferrari, G.; Clemente, F.; Guaragno, M. Ventricular energetics during mechanical ventilation and intra-aortic balloon pumping—Computer simulation. J. Med. Eng. Technol. 2001, 25, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Trivella, M.G.; De Lazzari, C. Intra-aortic balloon pumping (IABP), ventricular assist device (VAD) and Hemopump numerical models. In Modelling Cardiovascular System and Mechanical Circulatory Support; De Lazzari, C., Ed.; Consiglio Nazionale delle Ricerche (CNR): Roma, Italy, 2007; ISBN 978-88-8080-081-1. [Google Scholar]
- Creigen, V.; Ferracina, L.; Hlod, A.; van Mourik, S.; Vellekoop, M.; Zegeling, P.A. Modeling a Heart Pump. In Proceedings of the 58th European Study Group Mathematics with Industry; Bisseling, R.H., Dajani, K., Dijkema, T.J., Eds.; Utrecht University: Utrecht, The Netherlands, 2007; pp. 7–25. [Google Scholar]
- Valgimigli, M.; Steendijk, P.; Sianos, G.; Onderwater, E.; Serruys, P.W. Left ventricular unloading and concomitant total cardiac output increase by the use of percutaneous Impella Recover LP 2.5 assist device during high-risk coronary intervention catheter. Cardiovasc. Interv. 2005, 65, 263–267. [Google Scholar] [CrossRef]
- Watanabe, S.; Fish, K.; Kovacic, J.C.; Bikou, O.; Leonardson, L.; Nomoto, K.; Aguero, J.; Kapur, N.K.; Hajjar, R.J.; Ishikawa, K. Left Ventricular Unloading Using an Impella CP Improves Coronary Flow and Infarct Zone Perfusion in Ischemic Heart Failure. J. Am. Heart Assoc. 2018, 7, e006462. [Google Scholar] [CrossRef]
- Donker, D.W.; Brodie, D.; Henriques, J.P.S.; Broom, M. Left Ventricular Unloading During Veno-Arterial ECMO: A Simulation Study. ASAIO J. 2019, 65, 11–20. [Google Scholar] [CrossRef]
- Schampaert, S.; van’t Veer, M.; van de Vosse, F.N.; Pijls, N.H.J.; de Mol, B.A.; Rutten, M.C.M. In vitro comparison of support capabilities of intra-aortic balloon pump and Impella 2.5 left percutaneous. Artif. Organs 2011, 35, 893–901. [Google Scholar] [CrossRef] [PubMed]
- Melmed, K.R.; Schlick, K.H.; Rinsky, B.; Dumitrascu, O.M.; Volod, O.; Nezhad, M.; Padrick, M.M.; Runyan, C.; Arabia, F.A.; Moriguchi, J.D.; et al. Assessing Cerebrovascular Hemodynamics Using Transcranial Doppler in Patients with Mechanical Circulatory Support Devices. J. Neuroimaging 2020, 30, 297–302. [Google Scholar] [CrossRef]
- Sauren, L.D.; Accord, R.E.; Hamzeh, K.; de Jong, M.; van der Nagel, T.; van der Veen, F.H.; Maessen, J.G. Combined Impella and intra-aortic balloon pump support to improve both ventricular unloading and coronary blood flow for myocardial recovery: An experimental study. Artif. Organs 2007, 31, 839–842. [Google Scholar] [CrossRef]
- Burzotta, F.; Trani, C.; Doshi, S.N.; Townend, J.; van Geuns, R.J.; Hunziker, P.; Schieffer, B.; Karatolios, K.; Møller, J.E.; Ribichini, F.L.; et al. Impella ventricular support in clinical practice: Collaborative viewpoint from a European expert user group. Int. J. Cardiol. 2015, 201, 684–691. [Google Scholar] [CrossRef]
- Thiele, H.; Schuler, G.; Neumann, F.J.; Hausleiter, J.; Olbrich, H.G.; Schwarz, B.; Hennersdorf, M.; Empen, K.; Fuernau, G.; Desch, S.; et al. Intraaortic balloon counterpulsation in acute myocardial infarction complicated by cardiogenic shock: Design and rationale of the Intraaortic Balloon Pump in Cardiogenic Shock II (IABP-SHOCK II) trial. Am. Heart J. 2012, 163, 938–945. [Google Scholar] [PubMed]
- Thiele, H.; Zeymer, U.; Neumann, F.J.; Ferenc, M.; Olbrich, H.G.; Hausleiter, J.; de Waha, A.; Richardt, G.; Hennersdorf, M.; Empen, K.; et al. Intraaortic Balloon Pump in cardiogenic shock II (IABP-SHOCK II) trial investigators. Intra-aortic balloon counterpulsation in acute myocardial infarction complicated by cardiogenic shock (IABP-SHOCK II): Final 12 month results of a randomised, open-label trial. Lancet 2013, 382, 1638–1645. [Google Scholar] [PubMed]
- Thiele, H.; Zeymer, U.; Thelemann, N.; Neumann, F.J.; Hausleiter, J.; Abdel-Wahab, M.; Meyer-Saraei, R.; Fuernau, G.; Eitel, I.; Hambrecht, R.; et al. IABPSHOCK II Trial (Intraaortic Balloon Pump in Cardiogenic Shock II) Investigators. Intraaortic Balloon Pump in Cardiogenic Shock Complicating Acute Myocardial Infarction: Long-Term 6-Year Outcome of the Randomized IABP-SHOCK II Trial. Circulation 2019, 139, 395–403. [Google Scholar] [PubMed]
- Lo, N.; Magnus Ohman, E. Mechanical Circulatory Support in ST-Elevation Myocardial Infarction. In Primary Angioplasty: A Practical Guide; Watson, T.J., Ong, P.J., Tcheng, J.E., Eds.; Springer: Singapore, 2018; ISBN 9789811311130. [Google Scholar]
- Guinot, P.-G.; Andrei, S.; Longrois, D. Ventriculo-Arterial Coupling: From Physiological Concept to Clinical Application in Peri-Operative Care and ICUs. Eur. J. Anaesth. Intensive Care 2022, 1, e004. [Google Scholar] [CrossRef]
- Ky, B.; French, B.; Khan, A.M.; Plappert, T.; Wang, A.; Chirinos, J.A.; Fang, J.C.; Sweitzer, N.K.; Borlaug, B.A.; Kass, D.A.; et al. Ventricular-Arterial Coupling, Remodeling, and Prognosis in Chronic Heart Failure. J. Am. Coll. Cardiol. 2013, 62, 1165–1172. [Google Scholar] [CrossRef]
- Brasseur, A.; Scolletta, S.; Lorusso, R.; Taccone, F.S. Hybrid extracorporeal membrane oxygenation. J. Thorac. Dis. 2018, 10, S707–S715. [Google Scholar] [CrossRef]
- Lüsebrink, E.; Orban, M.; Kupka, D.; Scherer, C.; Hagl, C.; Zimmer, S.; Luedike, P.; Thiele, H.; Westermann, D.; Massberg, S.; et al. Prevention and treatment of pulmonary congestion in patients undergoing venoarterial extracorporeal membrane oxygenation for cardiogenic shock. Eur. Heart J. 2020, 41, 3753–3761. [Google Scholar] [CrossRef]
- Li, Y.; Yan, S.; Gao, S.; Liu, M.; Lou, S.; Liu, G.; Ji, B.; Gao, B. Effect of an intra-aortic balloon pump with venoarterial extracorporeal membrane oxygenation on mortality of patients with cardiogenic shock: A systematic review and meta-analysis. Eur. J. Cardiothorac. Surg. 2019, 55, 395–404. [Google Scholar]
- Gupta, A.; Allaqaband, S.; Bajwa, T. Combined Use of Impella Device and Intra-Aortic Balloon Pump to Improve Survival in a Patient in Profound Cardiogenic Shock Post Cardiac Arrest. Catheter. Cardiovasc. Interv. 2009, 74, 975–976. [Google Scholar]
- Enezate, T.H.; Kumar, A.; Al-Dadah, A.; Balla, S.; Omran, J. Is Combined use of Impella 2.5L and Intra-Aortic Balloon Pump for Refractory Cardiogenic Shock Superior to Either Device Alone? Austin Cardio Cardiovasc. Case Rep. 2016, 1, 1012. [Google Scholar]
- Lemor, A.; Dehkordi, S.H.H.; Basir, M.B.; Villablanca, P.A.; Jain, T.; Koenig, G.C.; Alaswad, K.; Moses, J.W.; Kapur, N.K.; O’Neill, W. Impella Versus Extracorporeal Membrane Oxygenation for Acute Myocardial Infarction Cardiogenic Shock. Cardiovasc. Revasc. Med. 2020, 21, 1465–1471. [Google Scholar] [CrossRef] [PubMed]
- Nix, C.; Ishikawa, K.; Meyns, B.; Yasuda, S.; Adriaenssens, T.; Barth, S.; Zayat, R.; Leprince, P.; Lebreton, G. Comparison of Hemodynamic Support by Impella vs. Peripheral Extra-Corporeal Membrane Oxygenation: A Porcine Model of Acute Myocardial Infarction. Front. Cardiovasc. Med. 2020, 7, 99. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
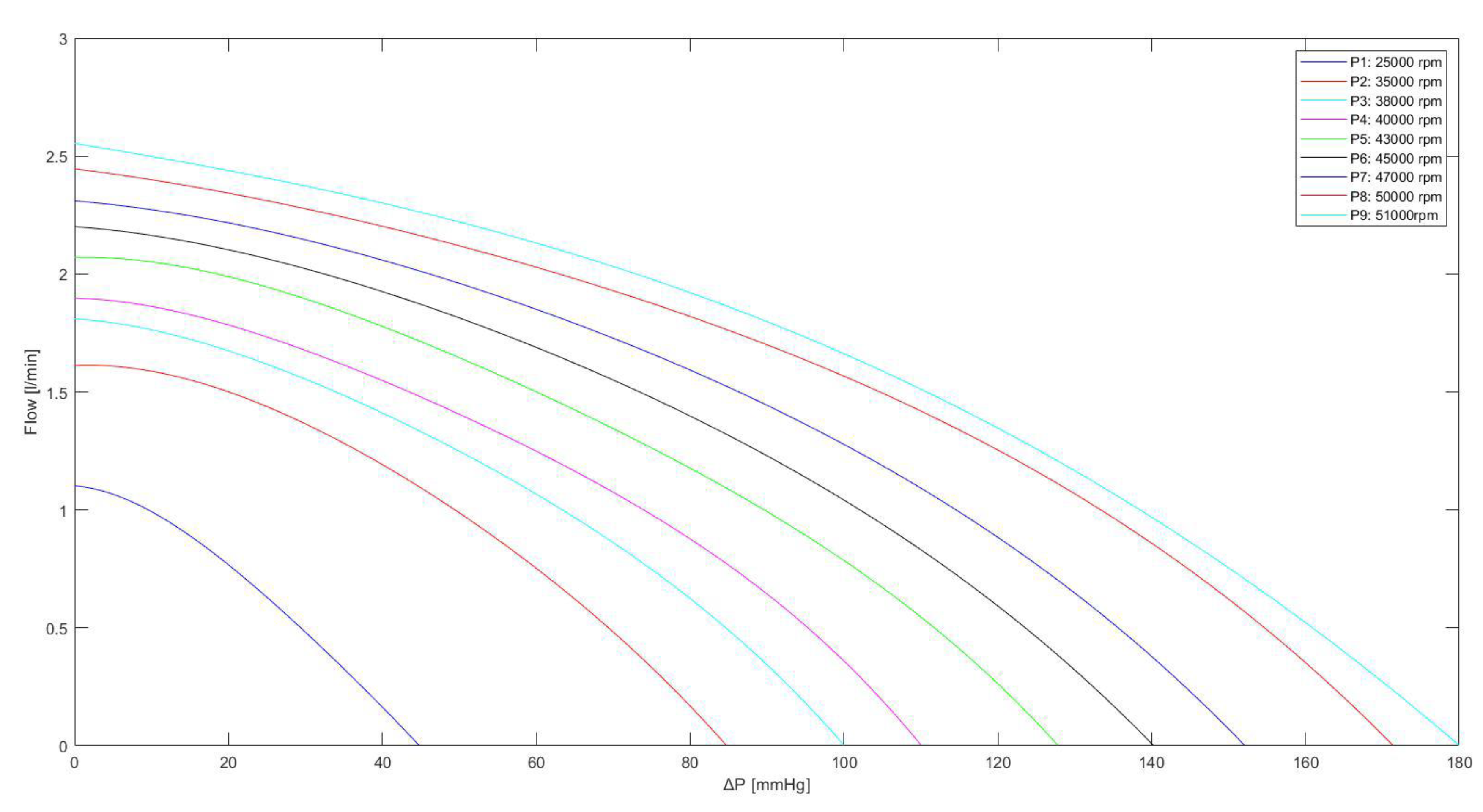
| Pump Rotational Speed (rpm) | K1 | K2 | K3 | K4 | K5 |
|---|---|---|---|---|---|
| 25,000 | −1.157·10−7 | 1.622·10−5 | −0.0009846 | −0.002613 | 1.102 |
| 35,000 | −2.065·10−8 | 3.849·10−6 | −0.0004192 | 0.001435 | 1.612 |
| 38,000 | −1.668·10−8 | 2.976·10−6 | −0.0002915 | 0.002004 | 1.812 |
| 40,000 | −1.497·10−8 | 3.849·10−6 | −0.000417 | 0.0005987 | 1.898 |
| 43,000 | −1.084·10−8 | 2.59·10−6 | −0.0002857 | 0.0006554 | 2.071 |
| 45,000 | −4.085·10−9 | 9.128·10−7 | −0.0001425 | −0.002385 | 2.201 |
| 47,000 | −3.011·10−9 | 6.504·10−7 | −0.0001116 | −0.0026555 | 2.31 |
| 50,000 | −1.742·10−9 | 3.015·10−7 | −6.007·10−5 | −0.004055 | 2.446 |
| 51,000 | −1.845·10−10 | −2.204·10−7 | −1.528·10−5 | −0.000537 | 2.554 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Lazzari, B.; Capoccia, M.; Badagliacca, R.; Bozkurt, S.; De Lazzari, C. IABP versus Impella Support in Cardiogenic Shock: “In Silico” Study. J. Cardiovasc. Dev. Dis. 2023, 10, 140. https://doi.org/10.3390/jcdd10040140
De Lazzari B, Capoccia M, Badagliacca R, Bozkurt S, De Lazzari C. IABP versus Impella Support in Cardiogenic Shock: “In Silico” Study. Journal of Cardiovascular Development and Disease. 2023; 10(4):140. https://doi.org/10.3390/jcdd10040140
Chicago/Turabian StyleDe Lazzari, Beatrice, Massimo Capoccia, Roberto Badagliacca, Selim Bozkurt, and Claudio De Lazzari. 2023. "IABP versus Impella Support in Cardiogenic Shock: “In Silico” Study" Journal of Cardiovascular Development and Disease 10, no. 4: 140. https://doi.org/10.3390/jcdd10040140