
Impact of Mitral Regurgitation Recurrence on Mitral Valve Repair for Secondary Ischemic Mitral Regurgitation
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Study Design
2.3. Study Procedure
- (1)
- Repositioning the PMs;
- (2)
- Standardized realignment of the subvalvular apparatus in one plane. This is achieved by the apico-lateral realignment of both PMs to eliminate apical tenting of the anterior leaflet;
- (3)
- Approximation of both PMs with the use of Goretex 4-0 stitch (CV-4 W.L. Gore & Associates Newark, Newark DE 19711, USA) for PMs for anatomy type 1–3 or with 4 mm Goretex graft (Gore & Associates Newark, city, DE, USA) for PMs anatomy type 4–5.
2.4. Interventions
2.5. Endpoints
2.6. Statistical Analysis
3. Results
3.1. Patients
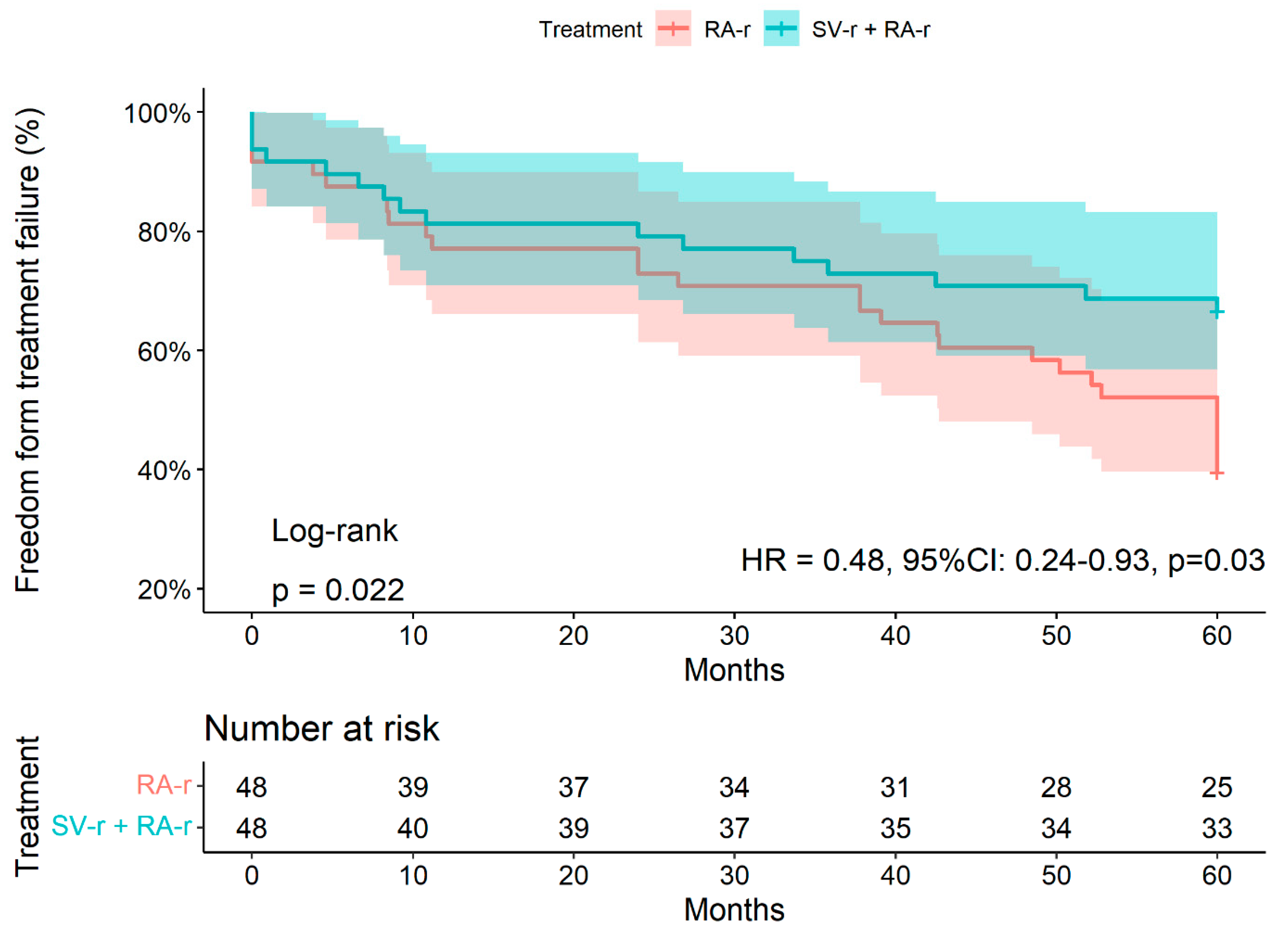
3.2. Treatment Failure at 5 Years
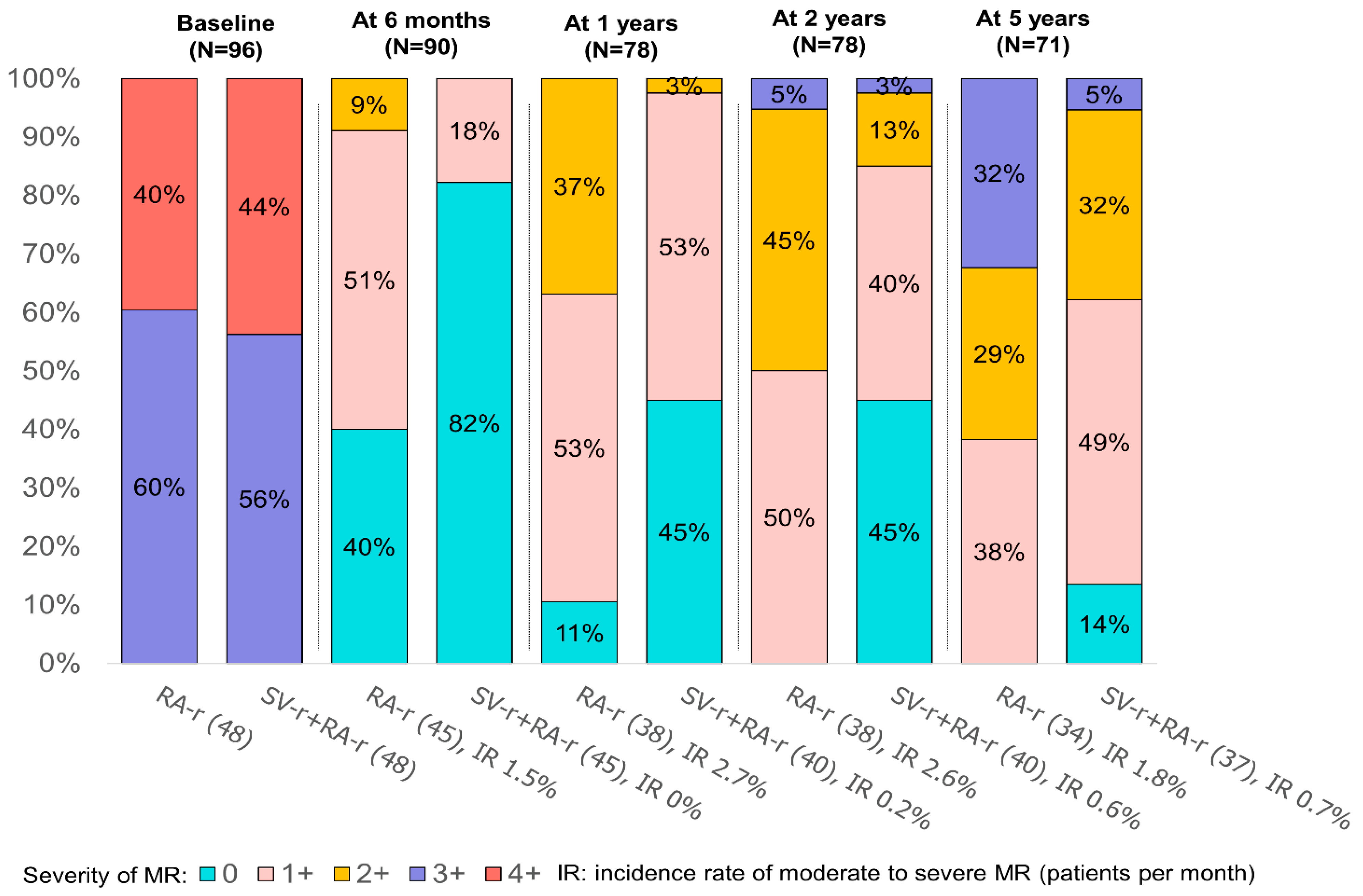
3.3. Influence of Residual MR
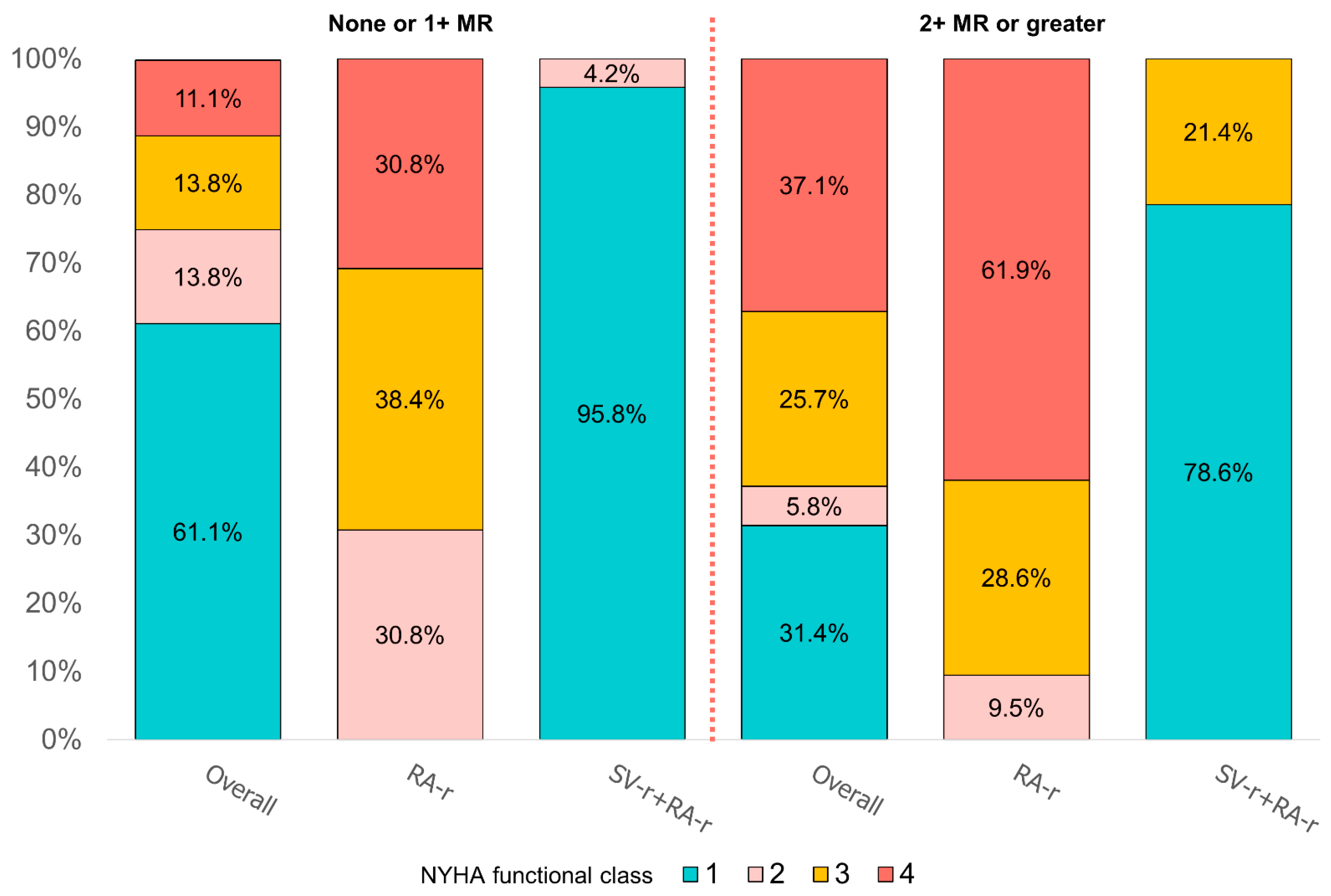
3.4. Left Ventricular Remodeling and NYHA Class
4. Discussion
4.1. Treatment-Based Differences in Outcomes after Mitral Valve Surgery for Secondary Mitral Regurgitation
4.2. Influence of Recurrent Mitral Regurgitation
4.3. Influence of LV Reverse Remodeling
4.4. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CABG | coronary artery bypass grafting |
| CTSN | Cardiothoracic Surgical Trials Network |
| EROA | effective regurgitant orifice area |
| ES-IPD | end-systolic interpapillary muscle distance |
| ETT | transthoracic echocardiography |
| HF | heart failure |
| IMR | ischemic mitral regurgitation |
| ITAs | internal thoracic arteries |
| LVEDD | left ventricular end-diastolic diameter |
| LVEF | left ventricular ejection fraction |
| LVESD | left ventricular end-systolic diameter |
| LVESVI | left ventricular end-systolic volume index |
| MI | myocardial infarction |
| MR | mitral regurgitation |
| MV | mitral valve |
| MVR | mitral valve replacement |
| NYHA | New York Heart Association |
| PMA | papillary muscle approximation |
| PMs | papillary muscles |
| QOL | decreased quality of life |
| RA-r | restrictive annuloplasty repair |
| RCTs | randomized clinical trials |
| SMR | secondary mitral regurgitation |
| SV-r | subvalvular repair |
| TH | tenting height |
References
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: Executive summary: A report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. J. Am. Coll. Cardiol. 2021, 77, 450–500. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 43, 561–623. [Google Scholar] [CrossRef] [PubMed]
- Nappi, F.; Lusini, M.; Spadaccio, C.; Nenna, A.; Covino, E.; Acar, C.; Chello, M. Papillary Muscle Approximation Versus Restrictive Annuloplasty Alone for Severe Ischemic Mitral Regurgitation. J. Am. Coll. Cardiol. 2016, 67, 2334–2346. [Google Scholar] [CrossRef] [PubMed]
- Nappi, F.; Spadaccio, C.; Nenna, A.; Lusini, M.; Fraldi, M.; Acar, C.; Chello, M. Is subvalvular repair worthwhile in severe ischemic mitral regurgitation? A Subanalysis of the Papillary Muscle Approximation trial. J. Thorac. Cardiovasc. Surg. 2017, 153, 286–295.e2. [Google Scholar] [CrossRef] [Green Version]
- Nappi, F.; Lusini, M.; Singh, S.S.A.; Santana, O.; Chello, M.; Mihos, C.G. Risk of Ischemic Mitral Regurgitation Recurrence After Combined Valvular and Subvalvular Repair. Ann. Thorac. Surg. 2019, 108, 536–543. [Google Scholar] [CrossRef]
- Harmel, E.; Pausch, J.; Gross, T.; Petersen, J.; Sinning, C.; Kubitz, J.; Reichenspurner, H.; Girdauskas, E. Standardized Subannular Repair Improves Outcomes in Type IIIb Functional Mitral Regurgitation. Ann. Thorac. Surg. 2019, 108, 1783–1792. [Google Scholar] [CrossRef]
- Fattouch, K.; Lancellotti, P.; Castrovinci, S.; Murana, G.; Sampognaro, R.; Corrado, E.; Caruso, M.; Speziale, G.; Novo, S.; Ruvolo, G. Papillary muscle relocation in conjunction with valve annuloplasty improve repair results in severe ischemic mitral regurgitation. J. Thorac. Cardiovasc. Surg. 2012, 143, 1352–1355. [Google Scholar] [CrossRef] [Green Version]
- Acker, M.A.; Parides, M.K.; Perrault, L.P.; Moskowitz, A.J.; Gelijns, A.C.; Voisine, P.; Smith, P.K.; Hung, J.W.; Blackstone, E.H.; Puskas, J.D.; et al. Mitral-Valve Repair versus Replacement for Severe Ischemic Mitral Regurgitation. N. Engl. J. Med. 2014, 370, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, D.; Moskowitz, A.J.; Gelijns, A.C.; Ailawadi, G.; Parides, M.K.; Perrault, L.P.; Hung, J.W.; Voisine, P.; Dagenais, F.; Gillinov, A.M.; et al. Two-Year Outcomes of Surgical Treatment of Severe Ischemic Mitral Regurgitation. N. Engl. J. Med. 2016, 374, 344–353. [Google Scholar] [CrossRef] [Green Version]
- Zoghbi, W.A.; Asch, F.M.; Bruce, C.; Gillam, L.D.; Grayburn, P.A.; Hahn, R.T.; Inglessis, I.; Islam, A.M.; Lerakis, S.; Little, S.H.; et al. Guidelines for the evaluation of valvular regurgitation after percutaneous valve repair or replacement: A report from the American Society of Echocardiography: Developed in collaboration with the Society for Cardiovascular Angiography and Interventions, Japanese Society of Echocardiography, and Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. 2019, 32, 431–475. [Google Scholar]
- Rama, A.; Nappi, F.; Praschker, B.G.L.; Gandjbakhch, I. Papillary Muscle Approximation for Ischemic Mitral Valve Regurgitation. J. Card. Surg. 2008, 23, 733–735. [Google Scholar] [CrossRef]
- Lancellotti, P.; Tribouilloy, C.; Hagendorff, A.; Popescu, B.A.; Edvardsen, T.; Pierard, L.A.; Badano, L.; Zamorano, J.L. Recommendations for the echocardiographic assessment of native valvular regurgitation: An executive summary from the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 611–644. [Google Scholar] [CrossRef] [Green Version]
- Packer, M.; Grayburn, P.A. New Evidence Supporting a Novel Conceptual Framework for Distinguishing Proportionate and Disproportionate Functional Mitral Regurgitation. JAMA Cardiol. 2020, 5, 469–475. [Google Scholar] [CrossRef]
- Grayburn, P.A.; Sannino, A.; Packer, M. Proportionate and Disproportionate Functional Mitral Regurgitation: A New Conceptual Framework That Reconciles the Results of the MITRA-FR and COAPT Trials. JACC Cardiovasc. Imaging 2019, 12, 353–362. [Google Scholar] [CrossRef]
- Hvass, U.; Joudinaud, T. The papillary muscle sling for ischemic mitral regurgitation. J. Thorac. Cardiovasc. Surg. 2010, 139, 418–423. [Google Scholar] [CrossRef] [Green Version]
- Kron, I.L.; Green, G.; Cope, J.T. Surgical relocation of the posterior papillary muscle in chronic ischemic mitral regurgitation. Ann. Thorac. Surg. 2002, 74, 600–601. [Google Scholar] [CrossRef]
- Roshanali, F.; Vedadian, A.; Shoar, S.; Naderan, M.; Mandegar, M.H. Efficacy of papillary muscle approximation in preventing functional mitral regurgitation recurrence in high-risk patients with ischaemic cardiomyopathy and mitral regurgitation. Acta Cardiol. 2013, 68, 271–278. [Google Scholar] [CrossRef]
- Langer, F.; Kunihara, T.; Hell, K.; Schramm, R.; Schmidt, K.I.; Aicher, D.; Kindermann, M.; Schäfers, H.J. RING+STRING: Successful repair technique for ischemic mitral regurgitation with severe leaflet tethering. Circulation 2009, 120 (Suppl. S11), S85–S91. [Google Scholar] [CrossRef] [Green Version]
- Kron, I.L.; Hung, J.; Overbey, J.R.; Bouchard, D.; Gelijns, A.C.; Moskowitz, A.; Voisine, P.; O’Gara, P.T.; Argenziano, M.; Michler, R.E.; et al. Predicting recurrent mitral regurgitation after mitral valve repair for severe ischemic mitral regurgitation. J. Thorac. Cardiovasc. Surg. 2015, 149, 752–761.e1. [Google Scholar] [CrossRef]
- Lancellotti, P.; Moura, L.; Pierard, L.A.; Agricola, E.; Popescu, B.A.; Tribouilloy, C.; Hagendorff, A.; Monin, J.L.; Badano, L.; Zamorano, J.L.; et al. European Association of Echocardiography recommendations for the assessment of valvular regurgitation. Part 2: Mitral and tricuspid regurgitation (native valve disease). Eur. J. Echocardiogr. 2010, 11, 307–332. [Google Scholar] [CrossRef] [Green Version]
- Nappi, F.; Nenna, A.; Mihos, C.; Spadaccio, C.; Gentile, F.; Chello, M.; Matzui, Y. Ischemic functional mitral regurgitation: From pathophysiological concepts to current treatment options. A systemic review for optimal strategy. Gen. Thorac. Cardiovasc. Surg. 2021, 69, 213–229. [Google Scholar] [CrossRef] [PubMed]
- Ciarka, A.; Braun, J.; Delgado, V.; Versteegh, M.; Boersma, E.; Klautz, R.; Dion, R.; Bax, J.J.; Van de Veire, N. Predictors of Mitral Regurgitation Recurrence in Patients With Heart Failure Undergoing Mitral Valve Annuloplasty. Am. J. Cardiol. 2010, 106, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Di Salvo, T.G.; Acker, M.A.; Dec, G.W.; Byrne, J.G. Mitral valve surgery in advanced heart failure. J. Am. Coll. Cardiol. 2010, 55, 271–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, J.; Papakostas, L.; Tahta, S. Mechanism of recurrent ischemic mitral regurgitation after annuloplasty: Continued LV remodeling as a moving target. Circulation 2004, 110 (Suppl. S1), 1185–1190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, R.A.; Schwammenthal, E. Ischemic mitral regurgitation on the threshold of a solution: From paradoxes to Unifying concepts. Circulation 2005, 112, 745–758. [Google Scholar] [CrossRef]
- Penicka, M.; Linkova, H.; Lang, O.; Fojt, R.; Kočka, V.; Vanderheyden, M.; Bartunek, J. Predictors of Improvement of Unrepaired Moderate Ischemic Mitral Regurgitation in Patients Undergoing Elective Isolated Coronary Artery Bypass Graft Surgery. Circulation 2009, 120, 1474–1481. [Google Scholar] [CrossRef] [Green Version]
- Fattouch, K.; Guccione, F.; Sampognaro, R.; Panzarella, G.; Corrado, E.; Navarra, E.; Calvaruso, D.; Ruvolo, G. POINT: Efficacy of adding mitral valve restrictive annuloplasty to coronary artery bypass grafting in patients with moderate ischemic mitral valve regurgitation: A randomized trial. J. Thorac. Cardiovasc. Surg. 2009, 138, 278–285. [Google Scholar] [CrossRef] [Green Version]
- Castleberry, A.W.; Williams, J.B.; Daneshmand, M.A.; Honeycutt, E.; Shaw, L.K.; Samad, Z.; Lopes, R.D.; Alexander, J.H.; Mathew, J.P.; Velazquez, E.J.; et al. Response to letter regarding article, “Surgical revascularization is associated with maximal survival in patients with ischemic mitral regurgitation: A 20-year experience”. Circulation 2014, 129, 2547–2565. [Google Scholar] [CrossRef] [Green Version]
- Kang, D.-H.; Kim, M.-J.; Kang, S.-J.; Song, J.-M.; Song, H.; Hong, M.-K.; Choi, K.-J.; Song, J.-K.; Lee, J.-W. Mitral Valve Repair Versus Revascularization Alone in the Treatment of Ischemic Mitral Regurgitation. Circulation 2006, 114 (Suppl. S1), 1499–1503. [Google Scholar] [CrossRef] [Green Version]
- Pausch, J.; Gross, T.S.; Müller, L.; von Stumm, M.; Kloth, B.; Reichenspurner, H.; Girdauskas, E. Subannular repair for functional mitral regurgitation type IIIb in patients with ischaemic versus dilated cardiomyopathy. Eur. J. Cardio-Thoracic Surg. 2021, 60, 122–130. [Google Scholar] [CrossRef]
- Nappi, F.; Singh, S.S.A. Subannular repair or transcatheter edge-to-edge repair for secondary mitral regurgitation? More data for international guidelines. JTCVS Open 2022, 10, 176–180. [Google Scholar] [CrossRef]
- Nappi, F.; Spadaccio, C.; Fraldi, M. Reply: Papillary Muscle Approximation Is an Anatomically Correct Repair for Ischemic Mitral Regurgitation. J. Am. Coll. Cardiol. 2016, 68, 1147–1148. [Google Scholar] [CrossRef]
- Nappi, F.; Singh, S.S.A.; Padala, M.; Attias, D.; Nejjari, M.; Mihos, C.G.; Benedetto, U.; Michler, R. The Choice of Treatment in Ischemic Mitral Regurgitation With Reduced Left Ventricular Function. Ann. Thorac. Surg. 2019, 108, 1901–1912. [Google Scholar] [CrossRef]
- Nappi, F.; Antoniou, G.A.; Nenna, A.; Michler, R.; Benedetto, U.; Singh, S.S.A.; Gambardella, I.C.; Chello, M. Treatment options for ischemic mitral regurgitation: A meta-analysis. J. Thorac. Cardiovasc. Surg. 2022, 163, 607–622.e14. [Google Scholar] [CrossRef]
- Sonne, C.; Sugeng, L.; Watanabe, N.; Weinert, L.; Saito, K.; Tsukiji, M.; Yoshida, K.; Takeuchi, M.; Mor-Avi, V.; Lang, R.M. Age and body surface area dependency of mitral valve and papillary apparatus parameters: Assessment by real-time three-dimensional echocardiography. Eur. J. Echocardiogr. 2009, 10, 287–294. [Google Scholar] [CrossRef] [Green Version]
- Nappi, F.; Nenna, A.; Spadaccio, C.; Lusini, M.; Chello, M.; Fraldi, M. Predictive factors of long-term results following valve repair in ischemic mitral valve prolapse. Int. J. Cardiol. 2016, 204, 218–228. [Google Scholar] [CrossRef]
- Nappi, F.; Cristiano, S.; Nenna, A.; Chello, M. Ischemic mitral valve prolapse. J. Thorac. Dis. 2016, 8, 3752–3761. [Google Scholar] [CrossRef] [Green Version]
- Nappi, F.; Spadaccio, C. Obstructive Cardiomyopathy and Tethering in Ischemic Mitral Regurgitation: Two Sides of the Coin. Ann. Thorac. Surg. 2019, 107, 1911–1912. [Google Scholar] [CrossRef]
- Jouan, J.; Tapia, M.; CCook, R.; Lansac, E.; Acar, C. Ischemic mitral valve prolapse: Mechanisms and implications for valve repair. Eur. J. Cardiothorac. Surg. 2004, 26, 1112–1117. [Google Scholar] [CrossRef]
- Watanabe, T.; Arai, H.; Nagaoka, E.; Oi, K.; Hachimaru, T.; Kuroki, H.; Fujiwara, T.; Mizuno, T. Influence of procedural differences on mitral valve configuration after surgical repair for functional mitral regurgitation: In which direction should the papillary muscle be relocated ? J. Cardiothorac. Surg. 2014, 9, 185. [Google Scholar] [CrossRef] [Green Version]
- Fattouch, K.; Castrovinci, S.; Murana, G.; Dioguardi, P.; Guccione, F.; Nasso, G.; Speziale, G. Papillary muscle relocation and mitral annuloplasty in ischemic mitral valve regurgitation: Midterm results. J. Thorac. Cardiovasc. Surg. 2014, 148, 1947–1950. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | No Treatment Failure within 5 Years (n = 51) | Treatment Failure within 5 Years (n = 45) | p Value * | ||
|---|---|---|---|---|---|
| SV-r + RA-r (n = 32) | RA-r (n = 19) | SV-r + RA-r (n = 16) | RA-r (n = 29) | ||
| Male sex | 23 (71.9) | 13 (68.4) | 5 (31.2) | 17 (58.6) | 0.05 |
| Age in years | 62.88 ± 7.32 | 62.05 ± 5.69 | 62.80 ± 6.58 | 66.24 ± 7.98 | 0.15 |
| Hypertension | 18 (56.2) | 5 (31.2) | 10 (52.6) | 13 (44.8) | 0.40 |
| Dyslipidemia | 12 (37.5) | 6 (37.5) | 6 (37.5) | 13 (44.8) | 0.92 |
| Diabetes | 11 (34.3) | 7 (36.8) | 7 (43.8) | 13 (44.8) | 0.83 |
| CKD, stage III+ | 4 (12.5) | 2 (10.5) | 5 (31.2) | 9 (31.0) | 0.14 |
| Family history of CVD | 8 (25.0) | 3 (15.8) | 4 (25.0) | 9 (31.0) | 0.70 |
| COPD | 3 (9.4) | 1 (5.3) | 4 (25.0) | 5 (17.2) | 0.29 |
| Atrial fibrillation | 5 (15.6) | 3 (15.8) | 4 (25.0) | 7 (24.1) | 0.76 |
| Preoperative MR | 0.97 | ||||
| grade 3 | 18 (56.2) | 11 (57.9) | 9 (56.2) | 18 (62.1) | |
| grade 4 | 14 (43.8) | 8 (42.1) | 7 (43.8) | 11 (37.9) | |
| Multivessel coronary disease | 23 (71.9) | 12 (63.2) | 13 (81.2) | 24 (82.8) | 0.42 |
| LVEF | 34.78 ± 4.68 | 37.26 ± 2.51 | 35.50 ± 6.58 | 36.31 ± 4.34 | 0.28 |
| Preoperative Values | SV-r + RA-r | RA-r | ||||
| MR grade | 3+/4+ | 3+/4+ | ||||
| LVEDD | 62.67 ± 3.41 | 61.44 ± 3.67 | ||||
| LVESD | 35.44 ± 3.54 | 52.23 ± 3.46 | ||||
| LVEF | 35.02 ± 5.33 | 36.69 ± 3.73 | ||||
| Tenting area (mm2) | 2.96 ± 0.36 | 2.84 ± 0.35 | ||||
| Tenting height (mm) | 1.21 ± 0.08 | 1.22 ± 0.16 | ||||
| ES IPD (mm) | 4.47 ± 0.42 | 4.42 ± 0.39 | ||||
| α angle (°) | 31.54 ± 2.27 | 31.61 ± 2.16 | ||||
| β angle (°) | 54.48 ± 5.00 | 54.10 ± 5.57 | ||||
| 6 months after the operation | SV-r + RA-r | RA-r | ||||
| MR grade | 0/1+ | 2+/3+ | p value | 0/1+ | 2+/3+ | p value |
| LVEDD | 62.064 ± 3.41 | 64.14 ± 3.03 | 0.05 | 61.04 ± 3.89 | 61.9 ± 3.44 | 0.44 |
| LVESD | 52.88 ± 3.42 | 54.79 ± 3.58 | 0.09 | 51.4 ± 3.25 | 53.1 ± 3.52 | 0.083 |
| LVEF | 35.32 ± 5.84 | 34.29 ± 3.91 | 0.50 | 36.32 ± 4.33 | 37.1 ± 2.98 | 0.48 |
| Tenting area (mm2) | 0.83 ± 0.23 | 0.96 ± 0.16 | 0.06 | 0.93 ± 0.30 | 0.98 ± 0.21 | 0.55 |
| Tenting height (mm) | 0.61 ± 0.17 | 0.76 ± 0.18 | 0.01 | 0.68 ± 0.15 | 0.70 ± 0.17 | 0.34 |
| ES IPD (mm) | 3.13 ± 0.37 | 3.37 ± 0.31 | 0.04 | 4.39 ± 0.46 | 4.45 ± 0.30 | 0.57 |
| α angle (°) | 19.59 ± 4.52 | 21.57 ± 3.65 | 0.20 | 27.16 ± 3.61 | 27.6 ± 3.12 | 0.65 |
| β angle (°) | 38.47 ± 4.17 | 40.36 ± 3.48 | 0.10 | 83.32 ± 10.50 | 84.9 ± 9.58 | 0.60 |
| 60 months after the operation | SV-r + RA-r | RA-r | ||||
| MR grade | 0/1+ | 2+/3+ | p value | 0/1+ | 2+/3+ | p value |
| LVEDD | 53.43 ± 1.73 | 61.43 ± 6.44 | <0.001 | 58.15 ± 3.95 | 62.2 ± 4.32 | 0.01 |
| LVESD | 44.13 ± 2.22 | 52.07 ± 6.79 | <0.001 | 47.62 ± 3.10 | 51.9 ± 4.24 | 0.004 |
| LVEF | 46.70 ± 4.24 | 39.79 ± 6.05 | <0.001 | 41.54 ± 4.07 | 38.9 ± 3.48 | 0.001 |
| Tenting area (mm2) | 0.89 ± 0.13 | 1.28 ± 0.36 | <0.001 | 1.9 ± 0.24 | 2.1 ± 0.40 | 0.11 |
| Tenting height (mm) | 0.64 ± 0.10 | 0.82 ± 0.20 | <0.001 | 0.72 ± 0.10 | 0.87 ± 0.14 | 0.87 |
| ES IPD (mm) | 3.75 ± 0.12 | 4.28 ± 0.49 | <0.001 | 4.1 ± 0.19 | 4.6 ± 0.61 | 0.007 |
| α angle (°) | 21.04 ± 2.78 | 23.21 ± 2.29 | 0.02 | 30.62 ± 1.26 | 32.6 ± 2.11 | 0.005 |
| β angle (°) | 37.04 ± 1.43 | 40.36 ± 3.48 | <0.001 | 78.77 ± 4.66 | 91.2 ± 9.33 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salsano, A.; Nenna, A.; Molinari, N.; Avtaar Singh, S.S.; Spadaccio, C.; Santini, F.; Chello, M.; Fiore, A.; Nappi, F. Impact of Mitral Regurgitation Recurrence on Mitral Valve Repair for Secondary Ischemic Mitral Regurgitation. J. Cardiovasc. Dev. Dis. 2023, 10, 124. https://doi.org/10.3390/jcdd10030124
Salsano A, Nenna A, Molinari N, Avtaar Singh SS, Spadaccio C, Santini F, Chello M, Fiore A, Nappi F. Impact of Mitral Regurgitation Recurrence on Mitral Valve Repair for Secondary Ischemic Mitral Regurgitation. Journal of Cardiovascular Development and Disease. 2023; 10(3):124. https://doi.org/10.3390/jcdd10030124
Chicago/Turabian StyleSalsano, Antonio, Antonio Nenna, Nicolas Molinari, Sanjeet Singh Avtaar Singh, Cristiano Spadaccio, Francesco Santini, Massimo Chello, Antonio Fiore, and Francesco Nappi. 2023. "Impact of Mitral Regurgitation Recurrence on Mitral Valve Repair for Secondary Ischemic Mitral Regurgitation" Journal of Cardiovascular Development and Disease 10, no. 3: 124. https://doi.org/10.3390/jcdd10030124