
Impact of Insulin-Treated Compared to Non-Insulin-Treated Diabetes Mellitus on Outcome of Percutaneous Coronary Intervention with Drug-Coated Balloons versus Drug-Eluting Stents in De Novo Coronary Artery Disease: The Randomized BASKET-SMALL 2 Trial
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population and Randomization
2.3. Procedures
2.4. Outcomes
2.5. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Levine, G.N.; Bates, E.R.; Blankenship, J.C.; Bailey, S.R.; Bittl, J.A.; Cercek, B.; Chambers, C.E.; Ellis, S.G.; Guyton, R.A.; Hollenberg, S.M.; et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J. Am. Coll. Cardiol. 2011, 58, e44–e122. [Google Scholar] [CrossRef] [Green Version]
- Jeger, R.V.; Farah, A.; Ohlow, M.A.; Mangner, N.; Möbius-Winkler, S.; Weilenmann, D.; Wöhrle, J.; Stachel, G.; Markovic, S.; Leibundgut, G.; et al. Long-term efficacy and safety of drug-coated balloons versus drug-eluting stents for small coronary artery disease (BASKET-SMALL 2): 3-year follow-up of a randomised, non-inferiority trial. Lancet 2020, 396, 1504–1510. [Google Scholar] [CrossRef]
- Jeger, R.V.; Farah, A.; Ohlow, M.A.; Mangner, N.; Möbius-Winkler, S.; Leibundgut, G.; Weilenmann, D.; Wöhrle, J.; Richter, S.; Schreiber, M.; et al. Drug-coated balloons for small coronary artery disease (BASKET-SMALL 2): An open-label randomised non-inferiority trial. Lancet 2018, 392, 849–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, Y.; Qiao, S.; Su, X.; Chen, Y.; Jin, Z.; Chen, H.; Xu, B.; Kong, X.; Pang, W.; Liu, Y.; et al. Drug-Coated Balloon Versus Drug-Eluting Stent for Small-Vessel Disease: The RESTORE SVD China Randomized Trial. JACC Cardiovasc. Interv. 2018, 11, 2381–2392. [Google Scholar] [CrossRef] [PubMed]
- Kleber, F.X.; Schulz, A.; Waliszewski, M.; Hauschild, T.; Böhm, M.; Dietz, U.; Cremers, B.; Scheller, B.; Clever, Y.P. Local paclitaxel induces late lumen enlargement in coronary arteries after balloon angioplasty. Clin. Res. Cardiol. 2015, 104, 217–225. [Google Scholar] [CrossRef]
- Megaly, M.; Ali, A.; Abraham, B.; Khalil, C.; Zordok, M.; Shaker, M.; Tawadros, M.; Hennawy, B.S.; Elbadawi, A.; Omer, M.; et al. Outcomes with Drug-Coated Balloons in Percutaneous Coronary Intervention in Diabetic Patients. Cardiovasc. Revasc. Med. 2020, 21, 78–85. [Google Scholar] [CrossRef]
- Van Belle, E.; Périé, M.; Braune, D.; Chmaït, A.; Meurice, T.; Abolmaali, K.; McFadden, E.P.; Bauters, C.; Lablanche, J.M.; Bertrand, M.E. Effects of coronary stenting on vessel patency and long-term clinical outcome after percutaneous coronary revascularization in diabetic patients. J. Am. Coll. Cardiol. 2002, 40, 410–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wöhrle, J.; Scheller, B.; Seeger, J.; Farah, A.; Ohlow, M.A.; Mangner, N.; Möbius-Winkler, S.; Weilenmann, D.; Stachel, G.; Leibundgut, G.; et al. Impact of Diabetes on Outcome with Drug-Coated Balloons Versus Drug-Eluting Stents: The BASKET-SMALL 2 Trial. JACC Cardiovasc. Interv. 2021, 14, 1789–1798. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.; Lu, W.; Han, Z.; Pan, S.; Wang, X.; Shan, Y.; Wang, X.; Zheng, X.; Li, R.; Zhou, Y.; et al. Clinical Outcomes of Drug-Coated Balloon in Coronary Patients with and without Diabetes Mellitus: A Multicenter, Propensity Score Study. J. Diabetes Res. 2021, 2021, 5495219. [Google Scholar] [CrossRef]
- Silber, S.; Serruys, P.W.; Leon, M.B.; Meredith, I.T.; Windecker, S.; Neumann, F.J.; Belardi, J.; Widimsky, P.; Massaro, J.; Novack, V.; et al. Clinical outcome of patients with and without diabetes mellitus after percutaneous coronary intervention with the resolute zotarolimus-eluting stent: 2-year results from the prospectively pooled analysis of the international global RESOLUTE program. JACC Cardiovasc. Interv. 2013, 6, 357–368. [Google Scholar] [CrossRef] [Green Version]
- Chandrasekhar, J.; Dangas, G.; Baber, U.; Sartori, S.; Qadeer, A.; Aquino, M.; Vogel, B.; Faggioni, M.; Vijay, P.; Claessen, B.E.; et al. Impact of insulin treated and non-insulin-treated diabetes compared to patients without diabetes on 1-year outcomes following contemporary PCI. Catheter Cardiovasc. Interv. 2020, 96, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Pi, S.H.; Rhee, T.M.; Lee, J.M.; Hwang, D.; Park, J.; Park, T.K.; Yang, J.H.; Song, Y.B.; Choi, J.H.; Hahn, J.Y.; et al. Outcomes in Patients with Diabetes Mellitus According to Insulin Treatment After Percutaneous Coronary Intervention in the Second-Generation Drug-Eluting Stent Era. Am. J. Cardiol. 2018, 121, 1505–1511. [Google Scholar] [CrossRef]
- Kalkman, D.N.; Woudstra, P.; den Heijer, P.; Menown, I.B.; Erglis, A.; Suryapranata, H.; Arkenbout, K.E.; Iñiguez, A.; van ‘t Hof, A.W.; Muller, P.; et al. One year clinical outcomes in patients with insulin-treated diabetes mellitus and non-insulin-treated diabetes mellitus compared to non-diabetics after deployment of the bio-engineered COMBO stent. Int. J. Cardiol. 2017, 226, 60–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voudris, V.; Karyofillis, P.; Thomopoulou, S.; Doulaptsis, C.; Manginas, A.; Pavlides, G.; Cokkinos, D.V. Long-term results after drug-eluting stent implantation in diabetic patients according to diabetic treatment. Hell. J. Cardiol. 2011, 52, 15–22. [Google Scholar]
- Gilgen, N.; Farah, A.; Scheller, B.; Ohlow, M.A.; Mangner, N.; Weilenmann, D.; Wöhrle, J.; Jamshidi, P.; Leibundgut, G.; Möbius-Winkler, S.; et al. Drug-coated balloons for de novo lesions in small coronary arteries: Rationale and design of BASKET-SMALL 2. Clin. Cardiol. 2018, 41, 569–575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeger, R.V.; Eccleshall, S.; Wan Ahmad, W.A.; Ge, J.; Poerner, T.C.; Shin, E.S.; Alfonso, F.; Latib, A.; Ong, P.J.; Rissanen, T.T.; et al. Drug-Coated Balloons for Coronary Artery Disease: Third Report of the International DCB Consensus Group. JACC Cardiovasc. Interv. 2020, 13, 1391–1402. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Simoons, M.L.; Chaitman, B.R.; White, H.D.; Joint ESC/ACCF/AHA/WHF Task Force for Universal Definition of Myocardial Infarction; Authors/Task Force Members Chairpersons; Thygesen, K.; Alpert, J.S.; et al. Third universal definition of myocardial infarction. J. Am. Coll. Cardiol. 2012, 60, 1581–1598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cutlip, D.E.; Windecker, S.; Mehran, R.; Boam, A.; Cohen, D.J.; van Es, G.A.; Steg, P.G.; Morel, M.A.; Mauri, L.; Vranckx, P.; et al. Clinical end points in coronary stent trials: A case for standardized definitions. Circulation 2007, 115, 2344–2351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abizaid, A.; Kornowski, R.; Mintz, G.S.; Hong, M.K.; Abizaid, A.S.; Mehran, R.; Pichard, A.D.; Kent, K.M.; Satler, L.F.; Wu, H.; et al. The influence of diabetes mellitus on acute and late clinical outcomes following coronary stent implantation. J. Am. Coll. Cardiol. 1998, 32, 584–589. [Google Scholar] [CrossRef] [PubMed]
- Bundhun, P.K.; Li, N.; Chen, M.H. Adverse cardiovascular outcomes between insulin-treated and non-insulin treated diabetic patients after percutaneous coronary intervention: A systematic review and meta-analysis. Cardiovasc. Diabetol. 2015, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Akin, I.; Bufe, A.; Eckardt, L.; Reinecke, H.; Senges, J.; Richardt, G.; Kuck, K.H.; Schneider, S.; Nienaber, C.A.; DES.DE Study Group. Comparison of outcomes in patients with insulin-dependent versus non-insulin dependent diabetes mellitus receiving drug-eluting stents (from the first phase of the prospective multicenter German DES.DE registry). Am. J. Cardiol. 2010, 106, 1201–1207. [Google Scholar] [CrossRef] [PubMed]
- Dangas, G.D.; Farkouh, M.E.; Sleeper, L.A.; Yang, M.; Schoos, M.M.; Macaya, C.; Abizaid, A.; Buller, C.E.; Devlin, G.; Rodriguez, A.E.; et al. Long-term outcome of PCI versus CABG in insulin and non-insulin-treated diabetic patients: Results from the FREEDOM trial. J. Am. Coll. Cardiol. 2014, 64, 1189–1197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Latib, A.; Ruparelia, N.; Menozzi, A.; Castriota, F.; Micari, A.; Cremonesi, A.; De Felice, F.; Marchese, A.; Tespili, M.; Presbitero, P.; et al. 3-Year Follow-Up of the Balloon Elution and Late Loss Optimization Study (BELLO). JACC Cardiovasc. Interv. 2015, 8, 1132–1134. [Google Scholar] [CrossRef] [Green Version]
- Cortese, B.; Di Palma, G.; Guimaraes, M.G.; Piraino, D.; Orrego, P.S.; Buccheri, D.; Rivero, F.; Perotto, A.; Zambelli, G.; Alfonso, F. Drug-Coated Balloon Versus Drug-Eluting Stent for Small Coronary Vessel Disease: PICCOLETO II Randomized Clinical Trial. JACC Cardiovasc. Interv. 2020, 13, 2840–2849. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Cho, Y.K.; Kim, S.W.; Hong, Y.J.; Koo, B.K.; Bae, J.W.; Lee, S.H.; Yang, T.H.; Park, H.S.; Choi, S.W.; et al. Clinical Results of Drug-Coated Balloon Treatment in a Large-Scale Multicenter Korean Registry Study. Korean Circ. J. 2022, 52, 444–454. [Google Scholar] [CrossRef]
- Nestelberger, T.; Jeger, R. Drug-coated Balloons for Small Coronary Vessel Interventions: A Literature Review. Interv. Cardiol. 2019, 14, 131–136. [Google Scholar] [CrossRef]
- Sinaga, D.A.; Ho, H.H.; Watson, T.J.; Sim, A.; Nyein, T.T.; Jafary, F.H.; Loh, J.K.; Ooi, Y.W.; Tan, J.K.; Ong, P.J. Drug-Coated Balloons: A Safe and Effective Alternative to Drug-Eluting Stents in Small Vessel Coronary Artery Disease. J. Interv. Cardiol. 2016, 29, 454–460. [Google Scholar] [CrossRef]
- Glagov, S.; Weisenberg, E.; Zarins, C.K.; Stankunavicius, R.; Kolettis, G.J. Compensatory enlargement of human ath- erosclerotic coronary arteries. N. Engl. J. Med. 1987, 316, 1371–1375. [Google Scholar] [CrossRef]
- Picard, F.; Doucet, S.; Asgar, A.W. Contemporary use of drug-coated balloons in coronary artery disease: Where are we now? Arch. Cardiovasc. Dis. 2017, 110, 259–272. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall | ITDM | NITDM | p-Value | |
|---|---|---|---|---|
| n | 252 | 95 | 157 | |
| age | 69.9 (9.5) | 70.9 (8.5) | 69.3 (9.9) | 0.1678 |
| sex = male | 178 (70.6) | 56 (58.9) | 122 (77.7) | 0.0025 |
| BMI | 29.8 (5.0) | 31.1 (5.2) | 29.0 (4.7) | 0.0012 |
| current smoker | 34 (13.5) | 10 (10.5) | 24 (15.2) | 0.5407 |
| former smoker | 98 (43.6) | 39 (41.1) | 59 (37.6) | |
| no | 116 (46.0) | 45 (47.4) | 71 (45.2) | |
| hypercholesterolemia | 187 (74.2) | 75 (78.9) | 112 (71.3) | 0.2663 |
| hypertension | 232 (92.1) | 91 (95.8) | 141 (89.8) | 0.1438 |
| family history | 93 (36.9) | 34 (35.8) | 59 (37.6) | 0.5411 |
| prev. anterior MI | 46 (18.3) | 19 (20.0) | 27 (17.2) | 0.6966 |
| prev. other MI | 58 (23.0) | 22 (23.2) | 36 (22.9) | 1.0000 |
| prev. any MI | 99 (39.3) | 39 (41.1) | 60 (38.2) | 0.7538 |
| prev. PCI | 160 (63.5) | 67 (70.5) | 93 (59.2) | 0.0951 |
| prev. CABG | 28 (11.1) | 13 (13.7) | 15 (9.6) | 0.4213 |
| heart failure | 41 (16.3) | 16 (16.8) | 25 (15.9) | 0.9877 |
| stroke | 16 (6.3) | 8 (8.4) | 8 (5.1) | 0.4601 |
| TIA | 11 (4.4) | 3 (3.2) | 8 (5.1) | |
| no | 225 (89.3) | 84 (88.4) | 141 (89.8) | |
| aortic aneurysm | 2 (0.8) | 2 (2.1) | 0 (0.0) | 0.2745 |
| PAOD | 21 (8.3) | 8 (8.4) | 13 (8.3) | 1.0000 |
| COPD | 26 (10.3) | 9 (9.5) | 17 (10.8) | 0.8975 |
| STEMI | 5 (2.0) | 3 (3.2) | 2 (1.3) | 0.6404 |
| NSTEMI | 35 (13.9) | 15 (15.8) | 20 (12.7) | |
| unstable | 26 (10.3) | 10 (10.5) | 16 (10.2) | |
| stable | 186 (73.8) | 67 (70.5) | 119 (75.8) | |
| acute coronary disease | 66 (26.2) | 28 (29.5) | 38 (24.2) | 0.4388 |
| liver disease | 12 (4.8) | 5 (5.3) | 7 (4.5) | 1.0000 |
| rheumatologic disorder | 9 (3.6) | 5 (5.3) | 4 (2.5) | 0.4381 |
| renal dysfunction | 82 (32.5) | 41 (43.2) | 41 (26.1) | 0.0078 |
| coronary LM | 8 (3.2) | 5 (5.3) | 3 (1.9) | 0.2712 |
| coronary LAD | 214 (84.9) | 87 (91.6) | 127 (80.9) | 0.0343 |
| coronary LCX | 195 (77.4) | 76 (80.0) | 119 (75.8) | 0.5368 |
| coronary RCA | 163 (64.7) | 60 (63.2) | 103 (65.6) | 0.7965 |
| multi-vessel coronary disease | 204 (81.0) | 80 (84.2) | 124 (79.0) | 0.3903 |
| ejection fraction % | 60.0 [50.0, 60.0] | 60.0 [50.0, 61.3] | 60.0 [49.3, 60.0] | 0.7926 |
| prev. clopidogrel | 65 (25.8) | 29 (30.5) | 36 (22.9) | 0.2351 |
| prev. ASS | 198 (78.6) | 79 (83.2) | 119 (75.8) | 0.2218 |
| prev. prasugrel | 18 (7.1) | 6 (6.3) | 12 (7.6) | 0.8853 |
| prev. ticagrelor | 38 (15.1) | 10 (10.5) | 28 (17.8) | 0.1647 |
| prev. statin | 176 (69.8) | 72 (75.8) | 104 (66.2) | 0.1647 |
| prev. anticoagulants | 26 (10.3) | 6 (6.3) | 20 (12.7) | 0.1641 |
| Type of Event | Subgroup | Study Arm | 1-y Events | 1-y HR [95% CI] | 2-y Events | 2-y HR [95% CI] | 3-y Events | 3-y HR [95% CI] |
|---|---|---|---|---|---|---|---|---|
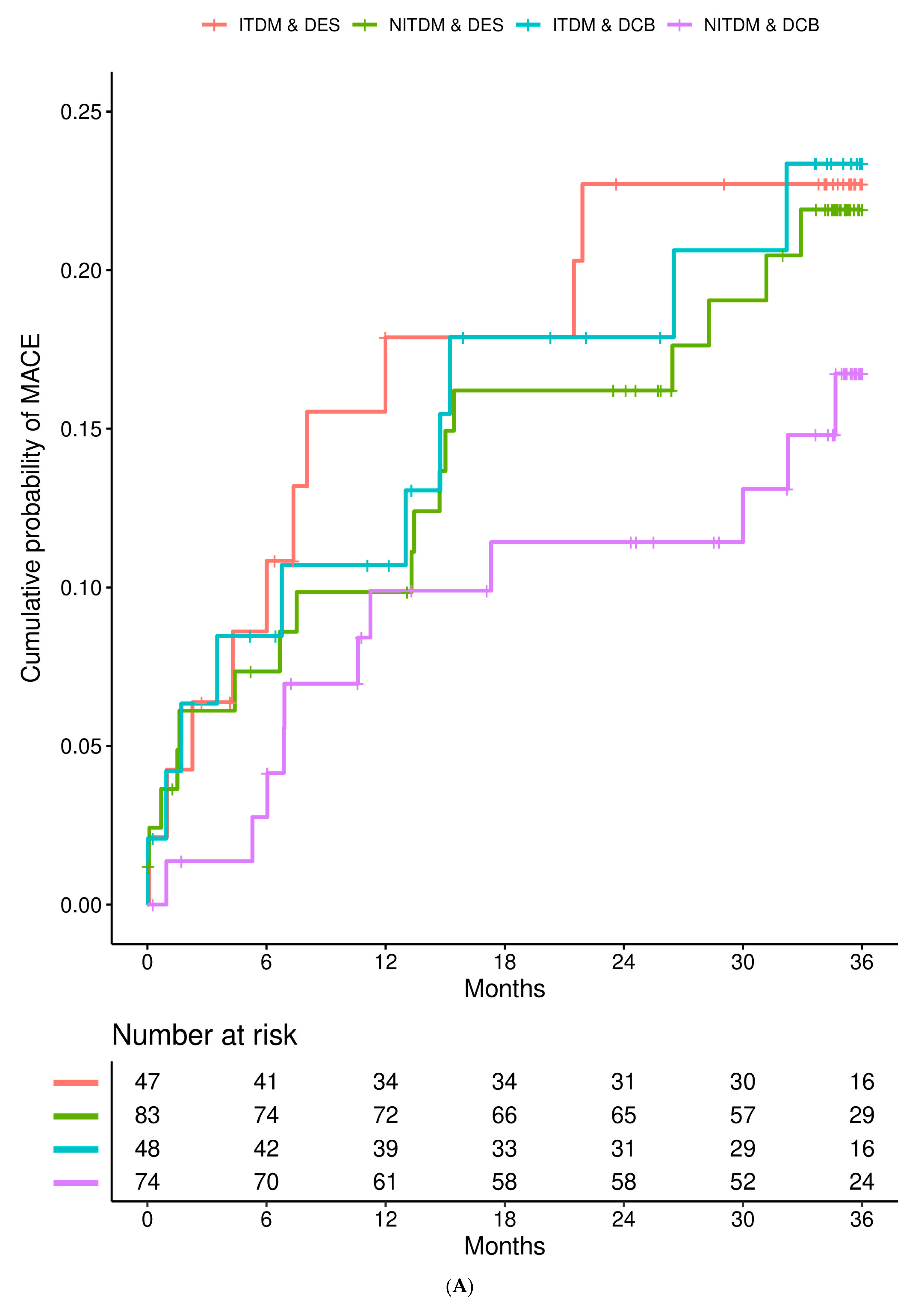
| MACE | ITDM | DES DCB | 8 (17.88%) 5 (10.70%) | 1—reference— 0.75 [0.24, 2.35] (p = 0.621) | 10 (22.71%) 8 (17.88%) | 1—reference – 0.89 [0.34, 2.31] (p = 0.813) | 10 (22.71%) 10 (23.36%) | 1—reference— 1.12 [0.46, 2.74] (p = 0.808) |
| MACE | NITDM | DES DCB | 8 (9.85%) 7 (9.90%) | 1—reference— 0.99 [0.32, 3.06] (p = 0.990] | 13 (16.20%) 8 (11.43%) | 1—reference— 0.70 [0.27, 1.85] (p = 0.476) | 17 (21.91%) 11 (16.74%) | 1—reference— 0.68 [0.29, 1.58] (p = 0.372) |
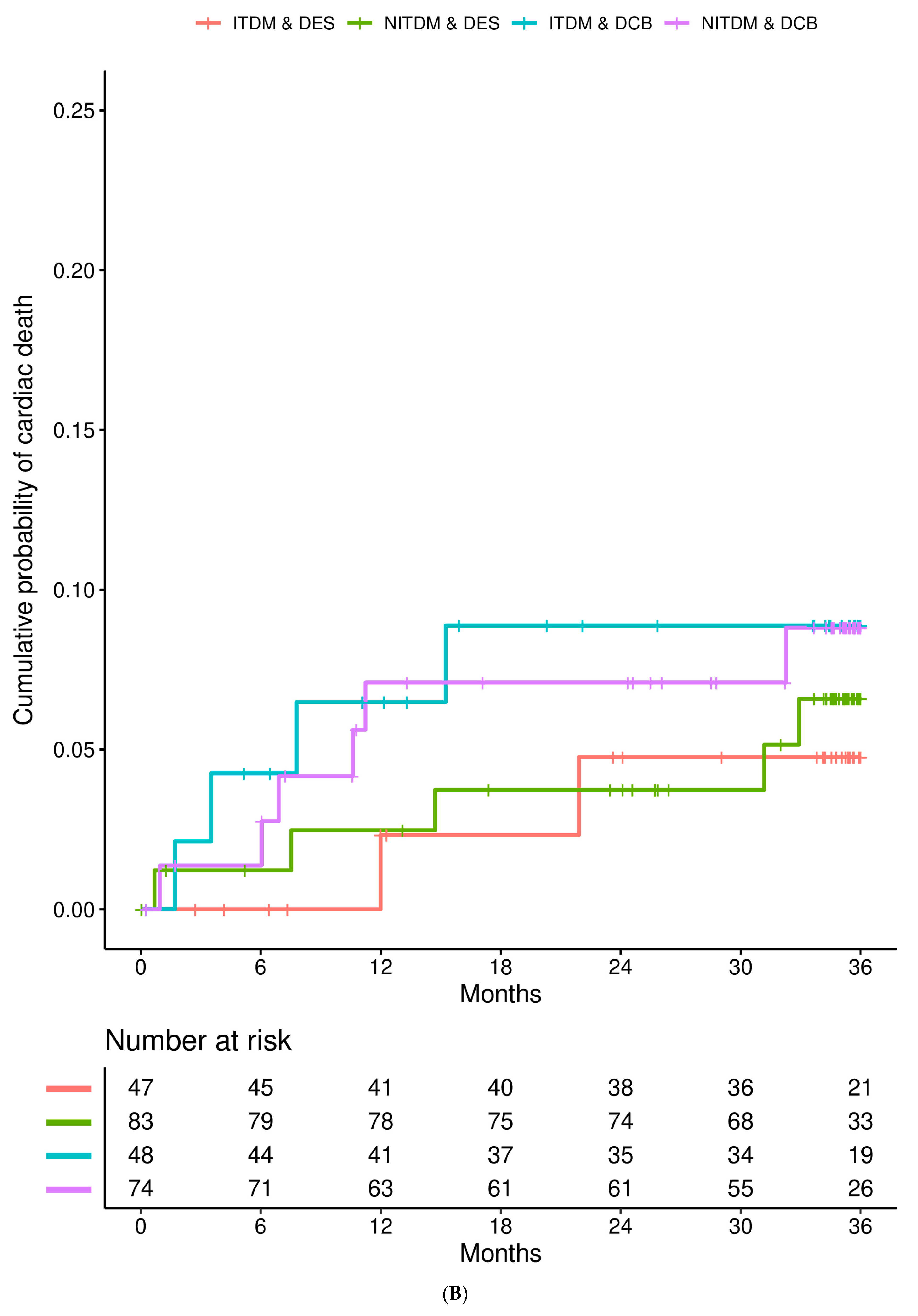
| cardiac death | ITDM | DES DCB | 1 (2.33%) 3 (6.48%) | 1—reference— 3.42 [0.35, 33.39] (p = 0.290) | 2 (4.77%) 4 (8.88%) | 1—reference— 2.25 [0.41, 12.37] (p = 0.353) | 2 (4.77%) 4 (8.88%) | 1—reference— 2.25 [0.41, 12.37] (p = 0.353) |
| cardiac death | NITDM | DES DCB | 2 (3.47%) 5 (7.09%) | 1—reference— 5.38 [1.02, 28.32] (p = 0.047) | 3 (3.74%) 5 (7.09%) | 1—reference— 3.47 [0.81,14.80] (p = 0.093) | 5 (6.59%) 6 (8.82%) | 1—reference— 2.47 [0.73, 8.34] (p = 0.145) |
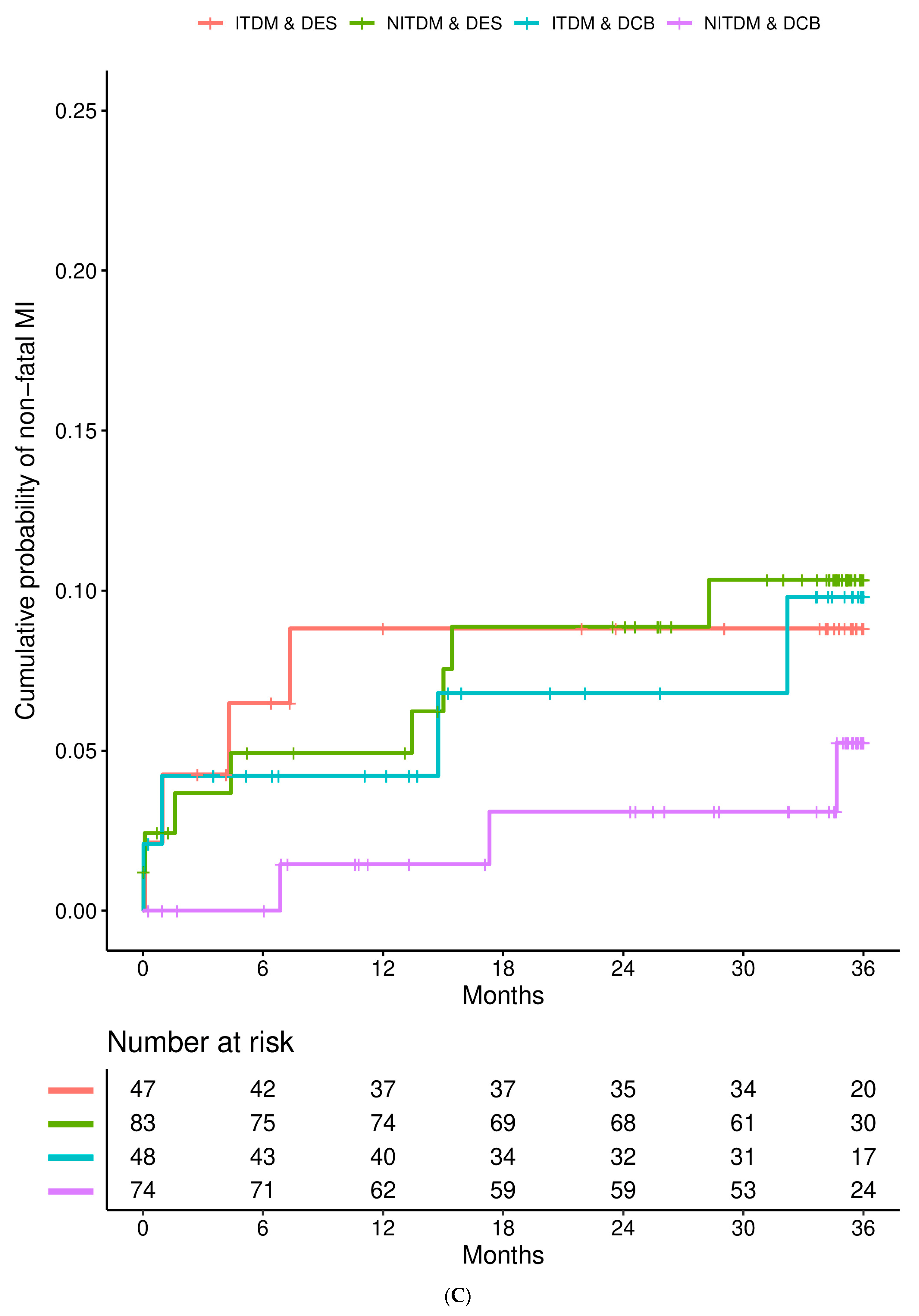
| non-fatal MI | ITDM | DES DCB | 4 (8.82%) 2 (4.21%) | 1—reference— 0.73 [0.13, 4.27] (p = 0.730) | 4 (8.82%) 2 (6.80%) | 1—reference— 1.00 [0.21, 4.80] (p = 0.999) | 4 (8.82%) 4 (9.81%) | 1—reference— 1.36 [0.32, 5.78] (p = 0.679) |
| non-fatal MI | NITDM | DES DCB | 4 (4.93%) 1 (1.45%) | 1—reference— 0.17 [0.02, 1.54] (p = 0.115) | 7 (8.87%) 2 (3.09%) | 1—reference— 0.10 [0.01, 1.00] (p = 0.050) | 8 (10.34%) 3 (5.25%) | 1—reference— 0.21 [0.04, 1.12] (p = 0.068) |
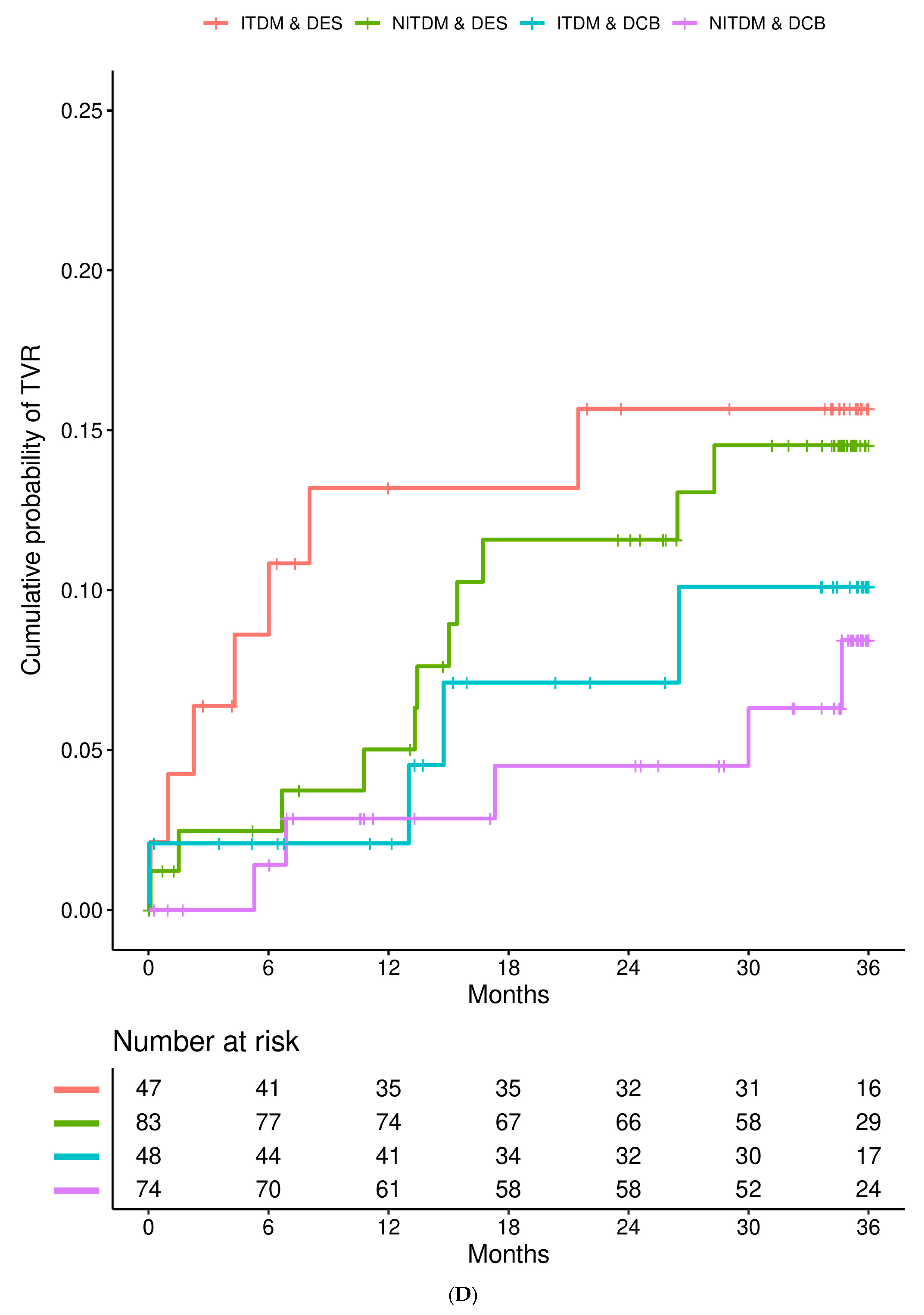
| TVR | ITDM | DES DCB | 6 (13.19%) 1 (2.08%) | 1—reference— 0.21 [0.02, 1.81] (p = 0.156) | 7 (15.67%) 3 (7.11%) | 1—reference— 0.48 [0.12, 1.92] (p = 0.297) | 7 (15.67%) 4 (10.11%) | 1—reference— 0.64 [0.18, 2.279. (p = 0.489) |
| TVR | NITDM | DES DCB | 4 (5.02%) 2 (2.86%) | 1—reference— 0.37 [0.06, 2.41] (p = 0.299) | 9 (11.58%) 3 (4.50%) | 1—reference— 0.25 [0.06, 1.08] (p = 0.063) | 11 (14.53%) 5 (8.44%) | 1—reference— 0.30 [0.09, 1.03] (p = 0.057) |
| all-causes death | ITDM | DES DCB | 2 (4.45%) 4 (8.56%) | 1—reference— 2.26 [0.41, 12.45] (p = 0.350) | 4 (9.11%) 7 (15.72%) | 1—reference— 2.19 [0.63, 7.60] (p = 0.217) | 5 (11.50%) 7 (15.72%) | 1—reference— 1.71 [0.53, 5.46] (p = 0.366) |
| all-causes death | NITDM | DES DCB | 3 (3.67%) 7 (9.75%) | 1—reference— 4.23 [1.05, 17.11] (p = 0.043) | 6 (7.38%) 8 (11.21%) | 1—reference— 1.79 [0.56, 5.70] (p = 0.324) | 10 (12.64%) 10 (14.41%) | 1—reference— 1.43 [0.55, 3.74] (p = 0.466) |
| Type of Event | Variable | 1-y HR [95% CI] (p-Value) | 2-y HR [95% CI] (p-Value) | 3-y HR [95% CI] (p-Value) |
|---|---|---|---|---|
| MACE | study arm: DCB vs. DES subgroup: NITDM vs. ITDM | 0.82 [0.38, 1.76] (p = 0.604) 0.59 [0.27, 1.28 0.(p = 0.183) | 0.77 [0.40, 1.49] (p = 0.442) 0.63 [0.33, 1.21] (p = 0.169) | 0.81 [0.45, 1.47] (p = 0.493) 0.75 [0.42, 1.36] (p = 0.348) |
| MACE | study arm: DCB vs. DES subgroup: NITDM vs. ITDM interaction: NITDM and DCB | 0.85 [0.39, 1.87] (p = 0.688) 0.61 [0.28, 1.33] (p = 0.215) 1.48 [0.31, 704] (p = 0.623) | 0.76 [0.39, 1.49] (p = 0.422) 0.63 [0.32, 1.21] (p = 0.163) 0.85 [0.23, 3.18] (p = 0.805) | 0.78 [0.43, 1.44] (p = 0.431) 0.73 [0.40, 1.34] (p = 0.314) 0.63 [0.19, 2.13] (p = 0.457) |
| cardiac death | study arm: DCB vs. DES subgroup: NITDM vs. ITDM | 3.93 [1.03, 15.04] (p = 0.046) 1.16 [0.33, 4.13] (p = 0.813) | 2.46 [0.82, 7.43] (p = 0.110) 0.89 [0.30, 2.63] (p = 0.830) | 2.06 [0.77, 5.50] (p = 0.150) 1.24 [0.45, 3.43] (p = 0.678) |
| cardiac death | study arm: DCB vs. DES subgroup: NITDM vs. ITDM interaction: NITDM and DCB | 3.85 [1.01, 14.63] (p = 0.048) 1.05 [0.25, 4.41] (p = 0.948) 1.50 [0.09, 25.19] (p = 0.779) | 2.49 [0.83, 7.49] (p = 0.105) 0.84 [0.27, 2.63] (p = 0.769) 1.37 [0.14, 12.90] (p = 0.786) | 2.06 [0.77, 5.50] (p = 0.151) 1.24 [0.43, 3.56] (p = 0.695) 1.03 [0.13, 8.39] (p = 0.977) |
| non-fatal MI | study arm: DCB vs. DES subgroup: NITDM vs. ITDM | 0.32 [0.08, 1.32] (p = 0.116) 0.42 [0.12, 1.44] (p = 167) | 0.45 [0.14, 1.37] (p = 0.157) 0.67 [0.24, 1.86] (p = 0.441) | 0.56 [0.21, 1.49] (p = 0.242) 0.75 [0.29, 1.91] (p = 0.546) |
| non-fatal MI | study arm: DCB vs. DES subgroup: NITDM vs. ITDM interaction: NITDM and DCB | 0.24 [0.05, 1.18] (p = 0.079) 0.30 [0.08, 1.24] (p = 0.096) 0.22 [0.01, 4.04] (p = 0.309) | 0.37 [0.11, 1.24] (p = 0.106) 0.52 [0.17, 1.58] (p = 0.248) 0.23 [0.02, 2.30] (p = 0.212) | 0.49 [0.17, 1.40] (p = 0.181) 0.65 [0.24, 1.75] (p = 0.392) 0.29 [0.04, 2.22] (p = 0.234) |
| TVR | study arm: DCB vs. DES subgroup: NITDM vs. ITDM | 0.28 [0.08, 1.04] (p = 0.058) 0.50 [0.16, 1.54] (p = 0.227) | 0.36 [0.14, 0.94] (p = 0.037) 0.67 [0.28, 1.60] (p = 0.368) | 0.41 [0.18, 0.95] (p = 0.038) 0.78 [0.35, 1.72] (p = 0.539) |
| TVR | study arm: DCB vs. DES subgroup: NITDM vs. ITDM interaction: NITDM and DCB | 0.30 [0.08, 1.16] (p = 0.081) 0.62 [0.16, 2.48] (p = 0.500) 2.28 [0.14, 36.22] (p = 0.560) | 0.34 [0.13, 0.93] (p = 0.035) 0.61 [0.23, 1.61] (p = 0.320) 0.66 [0.10, 4.57] (p = 0.673) | 0.39 [0.17, 0.92] (p = 0.032) 0.71 [0.31, 1.63] (p = 0.418) 0.55 [0.10, 3.09] (p = 0.493) |
| all-causes death | study arm: DCB vs. DES subgroup: NITDM vs. ITDM | 2.91 [0.99, 8.56] (p = 0.052) 0.99 [0.35, 2.80] (p = 0.981) | 1.71 [0.75, 3.88] (p = 0.201) 0.70 [0.31, 1.59] (p = 0.400) | 1.40 [0.68, 2.88] (p = 0.355) 0.92 [0.44, 1.93] (p = 0.832) |
| all-causes death | study arm: DCB vs. DES subgroup: NITDM vs. ITDM interaction: NITDM and DCB | 2.91 [1.00, 8.50] (p = 0.051) 0.88 [0.29, 2.68] (p = 0.822) 1.78 [0.20, 16.12] (p = 0.609) | 1.68 [0.73, 3.87] (p = 0.220) 0.72 [0.31, 1.66] (p = 0.437) 0.83 [0.16, 4.40] (p = 0.827) | 1.40 [0.68, 2.88] (p = 0.360) 0.93 [0.44, 1.95] (p = 0.846) 0.88 [0.20, 3.92] (p = 0.870) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seeger, J.; Wöhrle, J.; Scheller, B.; Farah, A.; Ohlow, M.-A.; Mangner, N.; Möbius-Winkler, S.; Weilenmann, D.; Stachel, G.; Leibundgut, G.; et al. Impact of Insulin-Treated Compared to Non-Insulin-Treated Diabetes Mellitus on Outcome of Percutaneous Coronary Intervention with Drug-Coated Balloons versus Drug-Eluting Stents in De Novo Coronary Artery Disease: The Randomized BASKET-SMALL 2 Trial. J. Cardiovasc. Dev. Dis. 2023, 10, 119. https://doi.org/10.3390/jcdd10030119
Seeger J, Wöhrle J, Scheller B, Farah A, Ohlow M-A, Mangner N, Möbius-Winkler S, Weilenmann D, Stachel G, Leibundgut G, et al. Impact of Insulin-Treated Compared to Non-Insulin-Treated Diabetes Mellitus on Outcome of Percutaneous Coronary Intervention with Drug-Coated Balloons versus Drug-Eluting Stents in De Novo Coronary Artery Disease: The Randomized BASKET-SMALL 2 Trial. Journal of Cardiovascular Development and Disease. 2023; 10(3):119. https://doi.org/10.3390/jcdd10030119
Chicago/Turabian StyleSeeger, Julia, Jochen Wöhrle, Bruno Scheller, Ahmed Farah, Marc-Alexander Ohlow, Norman Mangner, Sven Möbius-Winkler, Daniel Weilenmann, Georg Stachel, Gregor Leibundgut, and et al. 2023. "Impact of Insulin-Treated Compared to Non-Insulin-Treated Diabetes Mellitus on Outcome of Percutaneous Coronary Intervention with Drug-Coated Balloons versus Drug-Eluting Stents in De Novo Coronary Artery Disease: The Randomized BASKET-SMALL 2 Trial" Journal of Cardiovascular Development and Disease 10, no. 3: 119. https://doi.org/10.3390/jcdd10030119