
Effects of Intravenous Iron Replacement Therapy on Cardiovascular Outcomes in Patients with Heart Failure: A Systematic Review and Meta-Analysis
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Type of Studies, Outcomes and Inclusion and Exclusion Criteria
2.2. Search Methods
2.3. Data Collection and Analysis
2.4. Data Extraction and Management
2.5. Risk of Bias Assessment
2.6. Data Synthesis and Quantification
2.7. Subgroup Analysis and Sensitivity Analysis
3. Results
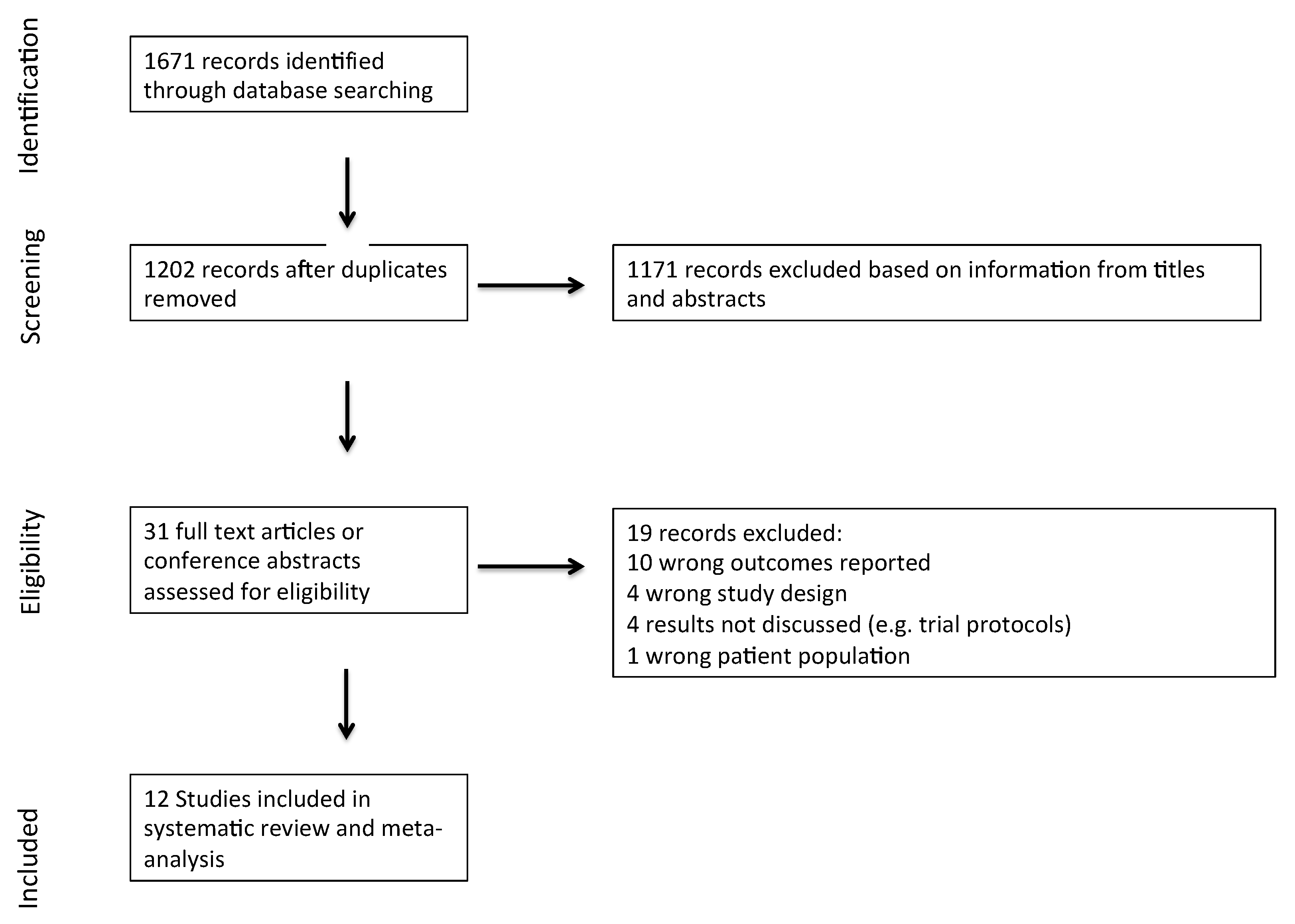
3.1. Search Strategy
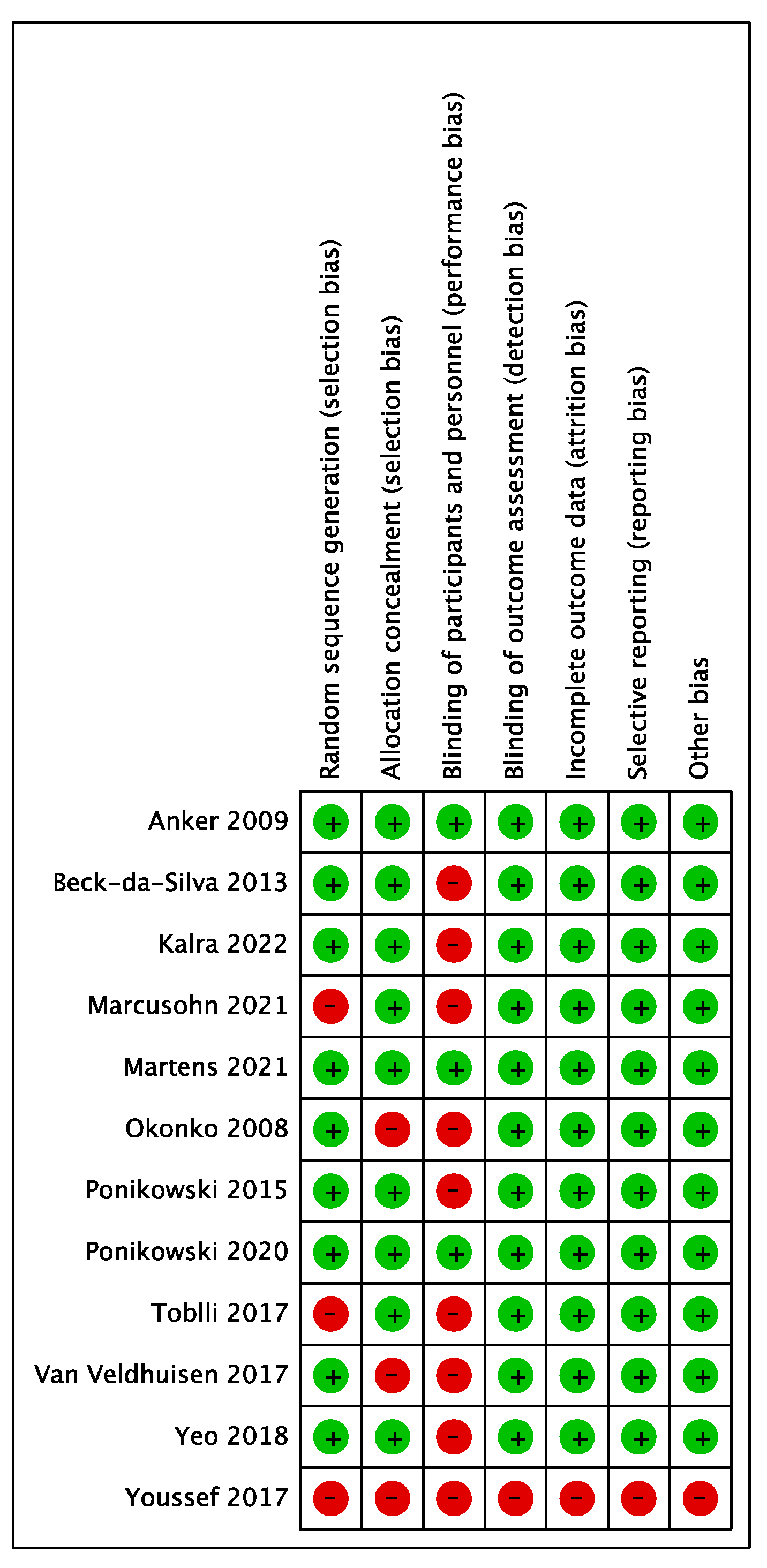
3.2. Characteristics of Included Studies and Risk of Bias Assessment
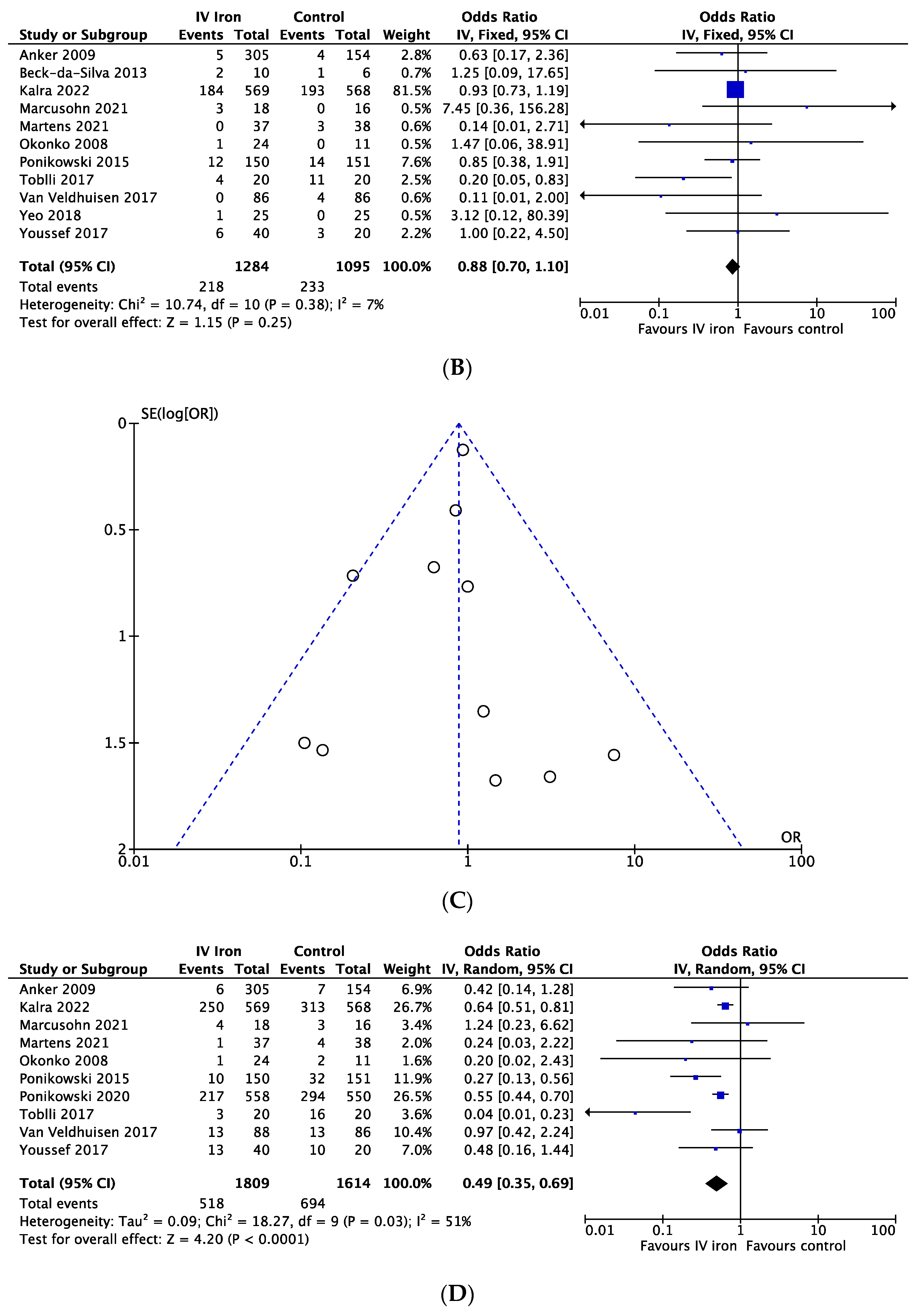
3.3. Primary Endpoint—Cardiovascular Mortality
3.4. Secondary Endpoints
3.4.1. All-Cause Mortality
3.4.2. Heart Failure Hospitalizations
3.4.3. Heart Failure Hospitalizations and Cardiovascular Death
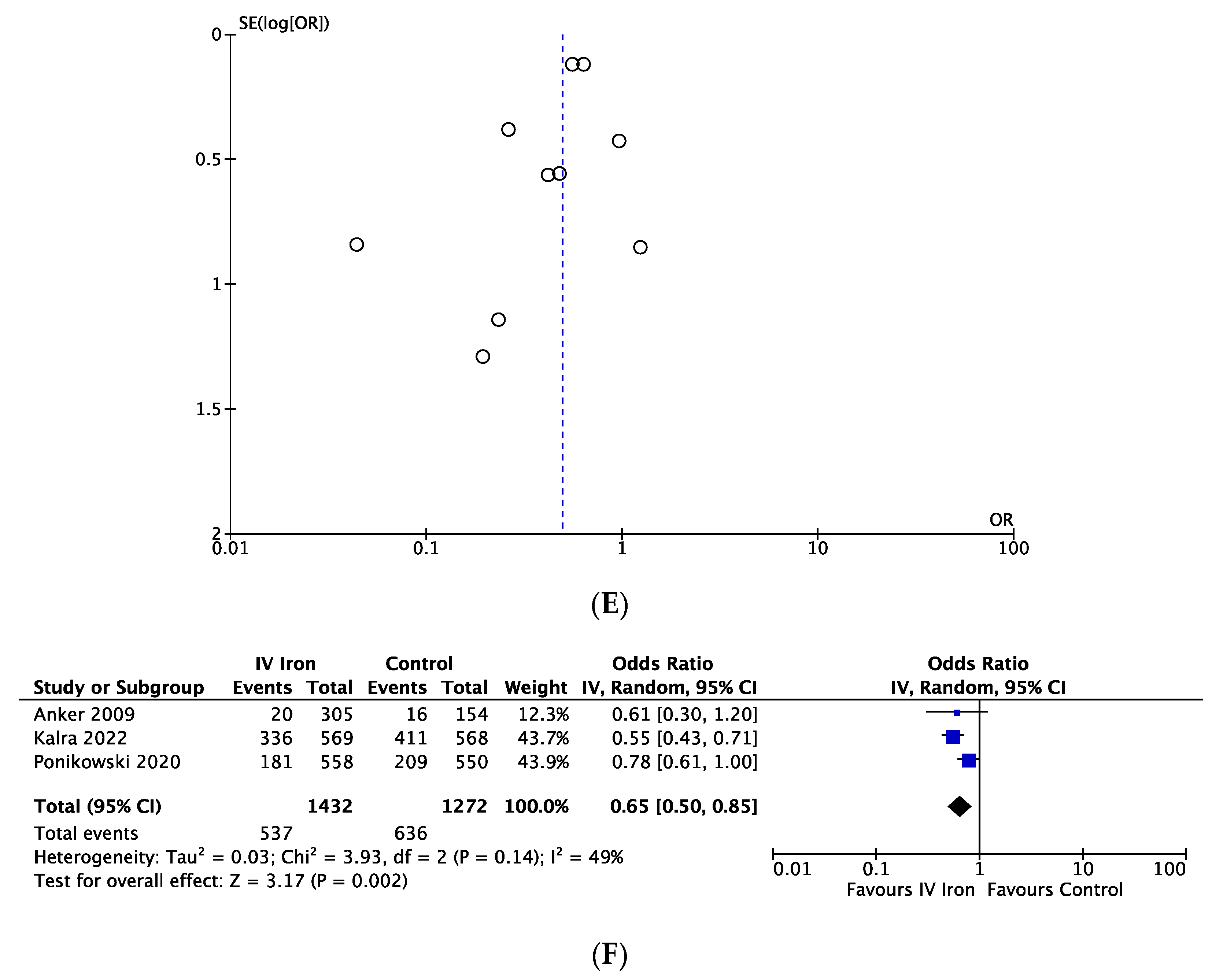
3.4.4. Endpoints in Chronic Heart Failure and Long Follow Up
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Andrews, N.C. Disorders of iron metabolism. N. Engl. J. Med. 1999, 341, 1986–1995. [Google Scholar] [CrossRef]
- Anderson, G.J.; Vulpe, C.D. Mammalian iron transport. Cell. Mol. Life Sci. 2009, 66, 3241–3261. [Google Scholar] [CrossRef] [PubMed]
- Jankowska, E.A.; von Haehling, S.; Anker, S.D.; Macdougall, I.C.; Ponikowski, P. Iron deficiency and heart failure: Diagnostic dilemmas and therapeutic perspectives. Eur. Heart J. 2013, 34, 816–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rouault, T.A.; Tong, W.-H. Iron–sulphur cluster biogenesis and mitochondrial iron homeostasis. Nat. Rev. Mol. Cell Biol. 2005, 6, 345–351. [Google Scholar] [CrossRef]
- Beard, J.L. Iron Biology in Immune Function, Muscle Metabolism and Neuronal Functioning. J. Nutr. 2001, 131, S568–S580. [Google Scholar] [CrossRef] [Green Version]
- Anker, S.D.; Comin Colet, J.; Filippatos, G.; Willenheimer, R.; Dickstein, K.; Drexler, H.; Lüscher, T.F.; Bart, B.; Banasiak, W.; Niegowska, J.; et al. Ferric Carboxymaltose in Patients with Heart Failure and Iron Deficiency. N. Engl. J. Med. 2009, 361, 2436–2448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponikowski, P.; Van Veldhuisen, D.J.; Comin-Colet, J.; Ertl, G.; Komajda, M.; Mareev, V.; McDonagh, T.; Parkhomenko, A.; Tavazzi, L.; Levesque, V.; et al. Beneficial effects of long-term intravenous iron therapy with ferric carboxymaltose in patients with symptomatic heart failure and iron deficiency. Eur. Heart J. 2015, 36, 657–668. [Google Scholar] [CrossRef]
- Van Veldhuisen, D.J.; Ponikowski, P.; van der Meer, P.; Metra, M.; Bohm, M.; Doletsky, A.; Voors, A.A.; MacDougal, I.C.; Anker, S.D.; Roubert, P.; et al. Effect of Ferric Car-boxymaltose on Exercise Capacity in Patients with Chronic Heart Failure and Iron Deficiency. Circulation 2017, 136, 1374–1383. [Google Scholar] [CrossRef]
- Grote Beverborg, N.; Klip, I.T.; Meijers, W.C.; Voors, A.A.; Vegter, E.L.; van der Wal, H.H.; Swinkels, D.V.; van Pelt, J.; Muldr, A.B.; Bulstra, J.K.; et al. Definition of Iron Deficiency Based on the Gold Standard of Bone Marrow Iron Staining in Heart Failure Patients. Circ. Heart Fail. 2018, 11, e004519. [Google Scholar] [CrossRef]
- Masini, G.; Graham, F.J.; Pellicori, P.; Cleland, J.G.; Cuthbert, J.J.; Kazmi, S.; Inciardi, R.M.; Clark, A.L. Criteria for Iron Deficiency in Patients with Heart Failure. J. Am. Coll. Cardiol. 2022, 79, 341–351. [Google Scholar] [CrossRef]
- Reinhold, J.; Papadopoulou, C.; Baral, R.; Vassiliou, V.S. Iron deficiency for prognosis in acute coronary syndrome—A systematic review and meta-analysis. Int. J. Cardiol. 2021, 328, 46–54. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.; Macdougall, I.C. Iron therapy for the treatment of iron deficiency in chronic heart failure: Intrave-nous or oral? Eur. J. Heart Fail. 2015, 17, 248–262. [Google Scholar] [CrossRef] [Green Version]
- Klip, I.T.; Comin-Colet, J.; Voors, A.A.; Ponikowski, P.; Enjuanes, C.; Banasiak, W.; Lok, D.J.; Rosentryt, P.; Torrens, A.; Polonski, L.; et al. Iron deficiency in chronic heart failure: An international pooled analysis. Am. Heart J. 2013, 165, 575–582.e3. [Google Scholar] [CrossRef] [PubMed]
- Van Veldhuisen, D.J.; Anker, S.D.; Ponikowski, P.; Macdougall, I.C. Anemia and iron deficiency in heart failure: Mechanisms and therapeutic approaches. Nat. Rev. Cardiol. 2011, 8, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Kalra, P.R.; Cleland, J.G.F.; Petrie, M.C.; A Thomson, E.; A Kalra, P.; Squire, I.B.; Ahmed, F.Z.; Al-Mohammad, A.; Cowburn, P.J.; Foley, P.W.X.; et al. Intravenous ferric derisomaltose in patients with heart failure and iron deficiency in the UK (IRONMAN): An investigator-initiated, prospective, randomised, open-label, blinded-endpoint trial. Lancet 2022, 400, 2199–2209. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef]
- Charles-Edwards, G.; Amaral, N.; Sleigh, A.; Ayis, S.; Catibog, N.; McDonagh, T.; Monaghan, M.; Amin-Youssef, G.; Kemp, G.J.; Shah, A.M.; et al. Effect of Iron Isomaltoside on Skeletal Muscle Energetics in Patients with Chronic Heart Failure and Iron Deficiency. Circulation 2019, 139, 2386–2398. [Google Scholar] [CrossRef]
- Papalia, F.; Jouhra, F.; Amin-Youssef, G.; Shah, A.M.; Charles-Edwards, G.; Okonko, D.O. Cardiac energetics in patients with chronic heart failure and iron deficiency: An in-vivo 31 P magnetic resonance spectroscopy study. Eur. J. Heart Fail. 2022, 24, 716–723. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and me-ta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Martens, P.; Dupont, M.; Dauw, J.; Nijst, P.; Herbots, L.; Dendale, P.; Vandervoort, P.; Bruckers, L.; Tang, W.H.W.; Mullens, W. The effect of intravenous ferric carboxymaltose on cardiac reverse remodelling following cardiac resynchronization therapy—The IRON-CRT trial. Eur. Heart J. 2021, 42, 4905–4914. [Google Scholar] [CrossRef]
- Ponikowski, P.; Kirwan, B.-A.; Anker, S.D.; McDonagh, T.; Dorobantu, M.; Drozdz, J.; Fabien, V.; Filippatos, G.; Göhring, U.M.; Keren, A.; et al. Ferric carboxymaltose for iron deficiency at discharge after acute heart failure: A multicentre, double-blind, randomised, controlled trial. Lancet 2020, 396, 1895–1904. [Google Scholar] [CrossRef] [PubMed]
- Yeo, T.J.; Yeo, P.S.D.; Hadi, F.A.; Cushway, T.; Lee, K.Y.; Yin, F.F.; Ching, A.; Li, R.; Loh, S.Y.; Lim, S.L.; et al. Single-dose intravenous iron in Southeast Asian heart failure patients: A pilot randomized placebo-controlled study (PRACTICE-ASIA-HF). ESC Heart Fail. 2018, 5, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Okonko, D.O.; Grzeslo, A.; Witkowski, T.; Mandal, A.K.; Slater, R.M.; Roughton, M.; Foldes, G.; Thum, T.; Majda, J.; Banasiak, W.; et al. Effect of intravenous iron sucrose on exercise tolerance in anemic and nonanemic patients with symptomatic chronic heart failure and iron defi-ciency FERRIC-HF: A randomized, controlled, observer-blinded trial. J. Am. Coll. Cardiol. 2008, 51, 103–112. [Google Scholar] [CrossRef] [Green Version]
- Marcusohn, E.; Borreda, I.; Hellman, Y.; Habib, M.; Bahouth, F.; Epstein, D.; Zukermann, R. IV Sodium Ferric Gluconate Complex in Patients with Iron Deficiency Hospitalized due to Acute Heart Failure-Investigator Initiated, Randomized Con-trolled Trial. J. Cardiovasc. Pharmacol. 2022, 80, 194–196. [Google Scholar] [CrossRef]
- Toblli, J.E.; Di Gennaro, F.P. Long-Term Effect of Intravenous Iron on Overall Survival and Hospitalization in Patients with Heart Failure with Reduced Ejection Fraction, Iron Deficiency and Mild Renal Impairment: An Open-Label 5-Year Follow Up Observation. J. Clin. Diagn. Res. 2017, 11, OC18–OC24. [Google Scholar] [CrossRef]
- Youssef, G.; Kamal, A.; Diab, R.; Hamid, M.A. P5825Intravenous iron therapy in acute decompensated heart failure patients with iron deficiency anaemia. Eur. Heart J. 2017, 38, ehx493.P5825. [Google Scholar] [CrossRef] [Green Version]
- Beck-Da-Silva, L.; Piardi, D.; Soder, S.; Rohde, L.E.; Pereira-Barretto, A.C.; Albuquerque, D.; Bocchi, E.; Vilas-Boas, F.; Moura, L.Z.; Montera, M.W.; et al. IRON-HF study: A randomized trial to assess the effects of iron in heart failure patients with anemia. Int. J. Cardiol. 2013, 168, 3439–3442. [Google Scholar] [CrossRef]
- Hoes, M.F.; Grote Beverborg, N.; Kijlstra, J.D.; Kuipers, J.; Swinkels, D.W.; Giepmans, B.N.G.; Rodenburg, R.J.; Van Veldhuisen, D.J.; De Boer, R.A.; Van Der Meer, P. Iron deficiency impairs contractility of human cardiomyocytes through decreased mitochondrial function. Eur. J. Heart Fail. 2018, 20, 910–919. [Google Scholar] [CrossRef] [Green Version]
- Johnson, B.B.; Reinhold, J.; Holmes, T.L.; Moore, J.A.; Cowell, V.; Bernardo, A.S.; Rushworth, S.A.; Vassiliou, V.; Smith, J.G.W. Modelling Metabolic Shifts during Cardiomyocyte Differentiation, Iron Deficiency and Transferrin Rescue Using Human Pluripotent Stem Cells. Metabolites 2021, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- Stewart, L.A.; Tierney, J.F. To IPD or not to IPD? Advantages and disadvantages of systematic reviews using indi-vidual patient data. Eval. Health Prof. 2002, 25, 76–97. [Google Scholar] [CrossRef] [PubMed]
- Núñez, J.; Miñana, G.; Cardells, I.; Palau, P.; Llàcer, P.; Fácila, L.; Almenar, L.; López-Lereu, M.P.; Monmeneu, J.V.; Amiguet, M.; et al. Noninvasive Imaging Estimation of Myocardial Iron Repletion Following Administration of Intravenous Iron: The Myocardial-IRON Trial. J. Am. Heart Assoc. 2020, 9, e014254. [Google Scholar] [CrossRef]
- Alam, M.H.; Auger, D.; Smith, G.C.; He, T.; Vassiliou, V.; Baksi, A.J.; Wage, R.; Drivas, P.; Feng, Y.; Firmin, D.N.; et al. T1 at 1.5T and 3T compared with conventional T2* at 1.5T for cardiac siderosis. J. Cardiovasc. Magn. Reson. 2015, 17, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/Year | Study Name | Countries | Number of Patients | Blinding | Definition of ID | IV Iron Form | Main Inclusion Criteria | Age (years) | Female (%) | LVEF (%) | Ischemic Cardiomyopathy (%) | NYHA III-IV (%) | eGFR (ml/min/1.73m2) | Follow Up Duration (weeks) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Anker 2009 [6] | FAIR-HF | 11 countries (Europe and Argentina) | 459 | Double | Guideline definition | FCM | Ambulatory NYHA II-III LVEF < 45% Hb 95–135g/L + ID | 67.8 (10.3) (FCM) 67.4 (11.1) (placebo) | 159 (52.3) (FCM) 85 (54.4) (placebo) | 31.9 (5.5) (FCM) 33 (6.1) (placebo) | 245 (80.6) (FCM) 123 (79.4) (placebo) | 251 (82.6) (FCM) 126 (81.3) (placebo) (NHA IV excl) | 63.8 (21.2) (FCM) 64.8 (25.3) (placebo) | 26 |
| Beck-da-Silva 2013 [28] | IRON-HF | Brazil | 23 | Double | Ferritin < 500 µg/L AND TSAT < 20% | IS | LVEF < 40% NYHA II-IV Able to perform ergospirometry | 66.9 (8.3) (IS) 68.9 (10.1) (placebo) | 30.4 | 25.2 (8.6) (IS) 30.7 (7.4) (placebo) | 39.1% | NA | NA | 12 |
| Kalra 2022 [15] | IRONMAN | UK | 1137 | Single (masked outcomes). Open label administration | Ferritin < 100 or TSAT < 20% | FDM | LVEF < 45% Iron deficient Symptomatic HF | 73·2 (66·7–80·1) (FDM) 73·5 (67·1–79·1) (usual care) | 142 (25%) (FDM) 158 (28%) (usual care) | 32 (25–37) (FDM) 35 (26–38) (usual care) | 331 (58%) (FDM) 316 (56%) (usual care) | 241 (42) (FDM) 248 (44) (usual care) | 51·7 (38·1–68·1) (FDM) 50·1 (37·8–68·6) (usual care) | 117 |
| Marcusohn 2021 [25] | Israel | 34 | Single | Guideline definition | SFGC | Acute admission with: -Hb 8–14 -ID -NT-proBNP > 300 pg/mL -IV loop diuretics | 71.5 (66.0 to 78.0) | 11 (32.4) | 35 (20 to 55) | N/A | N/A | N/A | 24 | |
| Martens 2021 [21] | IRON-CRT | Belgium | 75 | Double | Guideline definition | FCM | NYHA II-IV CRT > 6 months with ≥98% biventricular pacing LVEF ≤ 45% ID | 72 (12) (FCM) 73 (9) (placebo) | 11 (30) (FCM) 13 (34) (placebo) | 33 (8) (FCM) 34 (7) (placebo) | 19 (51) (FCM) 24 (63) (placebo) | 15 (41) (FCM) | 56 (25) (FCM) 51 (22) (placebo) | 13 |
| Okonko 2008 [24] | FERRIC-HF | Poland, UK | 35 | No | Guideline definition | IS | NYHA II-III LVEF ≤ 45% pVO2/kg ≤ 18 mL/kg/min ID | 64 (14) (IS) 62 (11) (control) | 7 (29) (IS) 3 (27) (control) | N/A | 18 (75) (IS) 8 (73) (control) | 11 (46) (IS) 5 (45) (control) | N/A | 18 |
| Ponikowski 2015 [7] | CONFIRM-HF | Austria, Italy, Poland, Portugal, Russia, Spain, Sweden, UK, and Ukraine | 304 | Double | Guideline definition | FCM | NYHA II-III LVEF ≤ 45% ID and Hb < 15 g/dl Able to complete 6 min walking test | 68.8 (9.5) (FCM) 69.5 (9.3) (placebo) | 67(45) FCM 74 (49) (placebo) | 37.1 (7.5) (FCM) 36.5 (7.3) (placebo) | 125 (83) (FCM) 126 (83) (placebo) | 70 (47) (FCM) 60 (40) (placebo) | 66.4 (21.7) (FCM) 63.5 (20.9) (placebo) | 52 |
| Ponikowski 2020 [22] | AFFIRM-AHF | 121 sites in Europe, South America, and Singapore | 1132 | Double | Guideline definition | FCM | ADHF LVEF ≤ 50% | 71.2 (10.8) (FCM) 70.9 (11.1) (placebo) | 244 (44%) (FCM) 250 (45%) (placebo) | 32.6 (9.6) (FCM) 32.7 (10.0) (placebo) | 265 (47%) (FCM) 257 (47%) (placebo) | 286 (51) (FCM) 299 (54) (placebo) | <60: 292 (52%) (FCM) 288 (52%) (placebo) | 52 |
| Toblli 2017 [26] | N/A | Argentina | 40 | Single | serum ferritin < 100 µg/L and/or TSAT ≤ 20% | IS | NYHA II-IV LVEF ≤ 35% ID and anemia | 76 (7) (IS) 74 (8) (saline) | 7 (35%) (IS) 8 (40%) (saline) | 31.3 (3.7) (IS) 30.8 (1.7) (saline) | ? | 2.9 (0.7) (IS) 2.9 (0.6) (saline) | ? | 260 |
| Van Veldhuisen 2017 [8] | EFFECT-HF | Australia, Belgium, France, Germany, Italy, The Netherlands, Poland, Russia, and Spain | 174 | No | Guideline definition | FCM | NYHA II-III. Optimized HF medications, LVEF ≤ 45%, ID | 63 (12) (FCM) 64 (11) (standard care) | 26 (30%) (FCM) 17 (20%) (standard care) | 33 (9) (FCM) 31 (8) (standard care) | ? | 25 (29) (FCM) 32 (37) (standard care) | 52 (13) (FCM) 51 (12) (standard care) | 24 |
| Yeo 2018 [23] | PRACTICE-ASIA-HF | Singapore | 50 | Single | ferritin < 300 µg/L and TSAT < 20% | FCM | ADHF, anemia and ID, able to do 6 min walk test, age > 21 years | 61.1 (10.8) (FCM) 64 (10) (Saline) | 6 (25%) (FCM), 5 (20%) (Saline) | 38.8 (17.5) 33.2 (14.8) | ? | ? | ? | 12 |
| Youssef 2017 [27] | N/A | Egypt | 60 | Single | Guideline definition | IS | ADHF NYHA III-IV, LVEF < 40, Anemia and ID | ? | ? | <40% | ? | 100% | ? | 13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reinhold, J.; Burra, V.; Corballis, N.; Tsampasian, V.; Matthews, G.; Papadopoulou, C.; Vassiliou, V.S. Effects of Intravenous Iron Replacement Therapy on Cardiovascular Outcomes in Patients with Heart Failure: A Systematic Review and Meta-Analysis. J. Cardiovasc. Dev. Dis. 2023, 10, 116. https://doi.org/10.3390/jcdd10030116
Reinhold J, Burra V, Corballis N, Tsampasian V, Matthews G, Papadopoulou C, Vassiliou VS. Effects of Intravenous Iron Replacement Therapy on Cardiovascular Outcomes in Patients with Heart Failure: A Systematic Review and Meta-Analysis. Journal of Cardiovascular Development and Disease. 2023; 10(3):116. https://doi.org/10.3390/jcdd10030116
Chicago/Turabian StyleReinhold, Johannes, Vyas Burra, Natasha Corballis, Vasiliki Tsampasian, Gareth Matthews, Charikleia Papadopoulou, and Vassilios S. Vassiliou. 2023. "Effects of Intravenous Iron Replacement Therapy on Cardiovascular Outcomes in Patients with Heart Failure: A Systematic Review and Meta-Analysis" Journal of Cardiovascular Development and Disease 10, no. 3: 116. https://doi.org/10.3390/jcdd10030116