
Impact of Medical Specialties on Diagnostic and Therapeutic Management of Elderly Cancer Patients
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
- Patient’s age, gender, lifestyle, and home support.
- Medical information: allergies, medical history, comorbidities, and number of medications prescriptions.
- The cancer history with the different para-clinical examinations performed.
- A standardized geriatric assessment including: Karnofsky/ECOG performance status score, ADL/IADL score, MMSE, mini-GDS/GDS, assessment of neurosensory deficits, number of falls in the previous year, nutritional assessment, sleep/asthenia assessment, physical activity evaluation, muscle strength assessment, mobility assessment, motor performance assessment.
- G8 score.
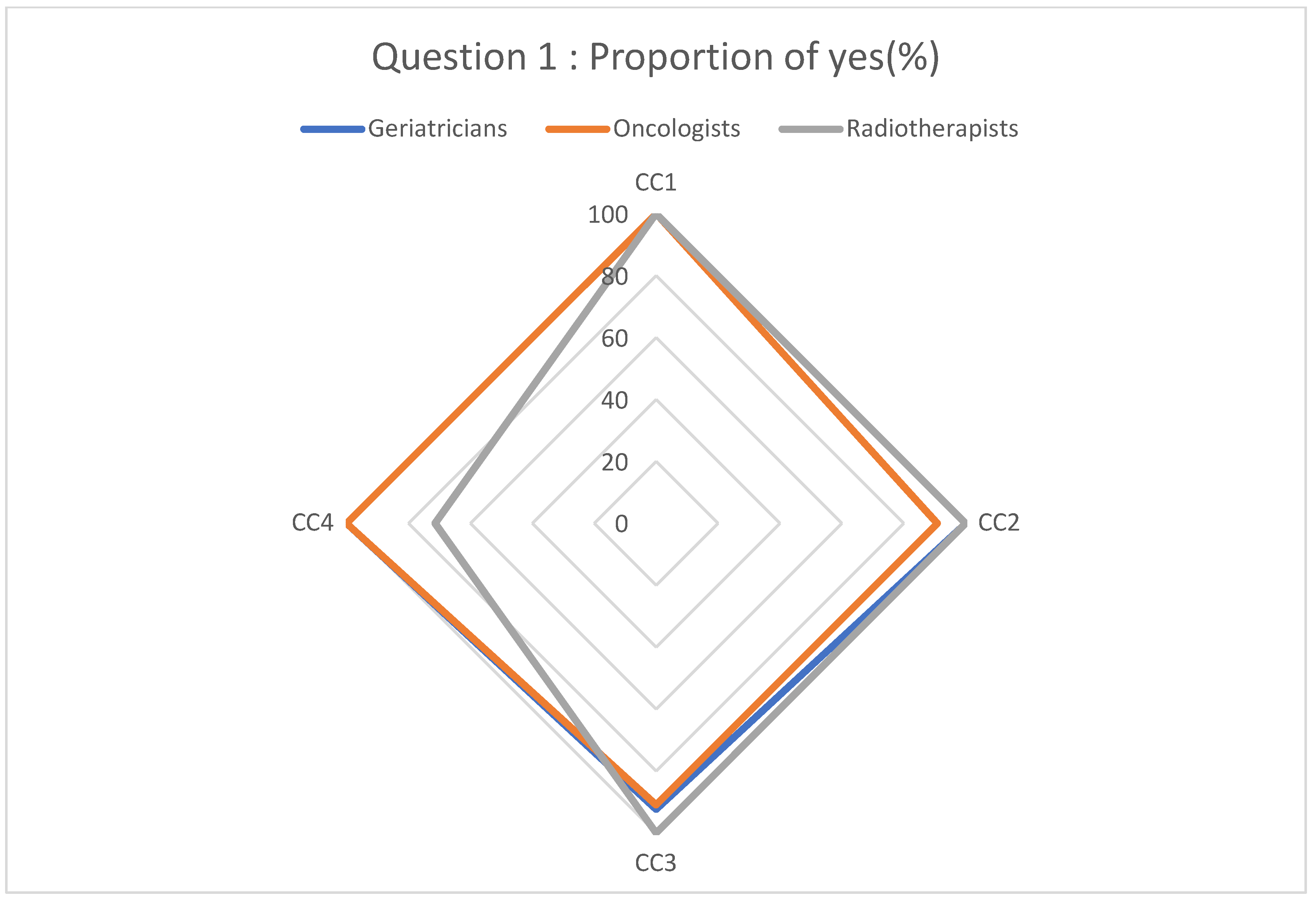
- Question 1: Would you have carried out diagnostic for cancer in this patient (biopsies, complementary exams...); Does a diagnostic approach seem reasonable to you?
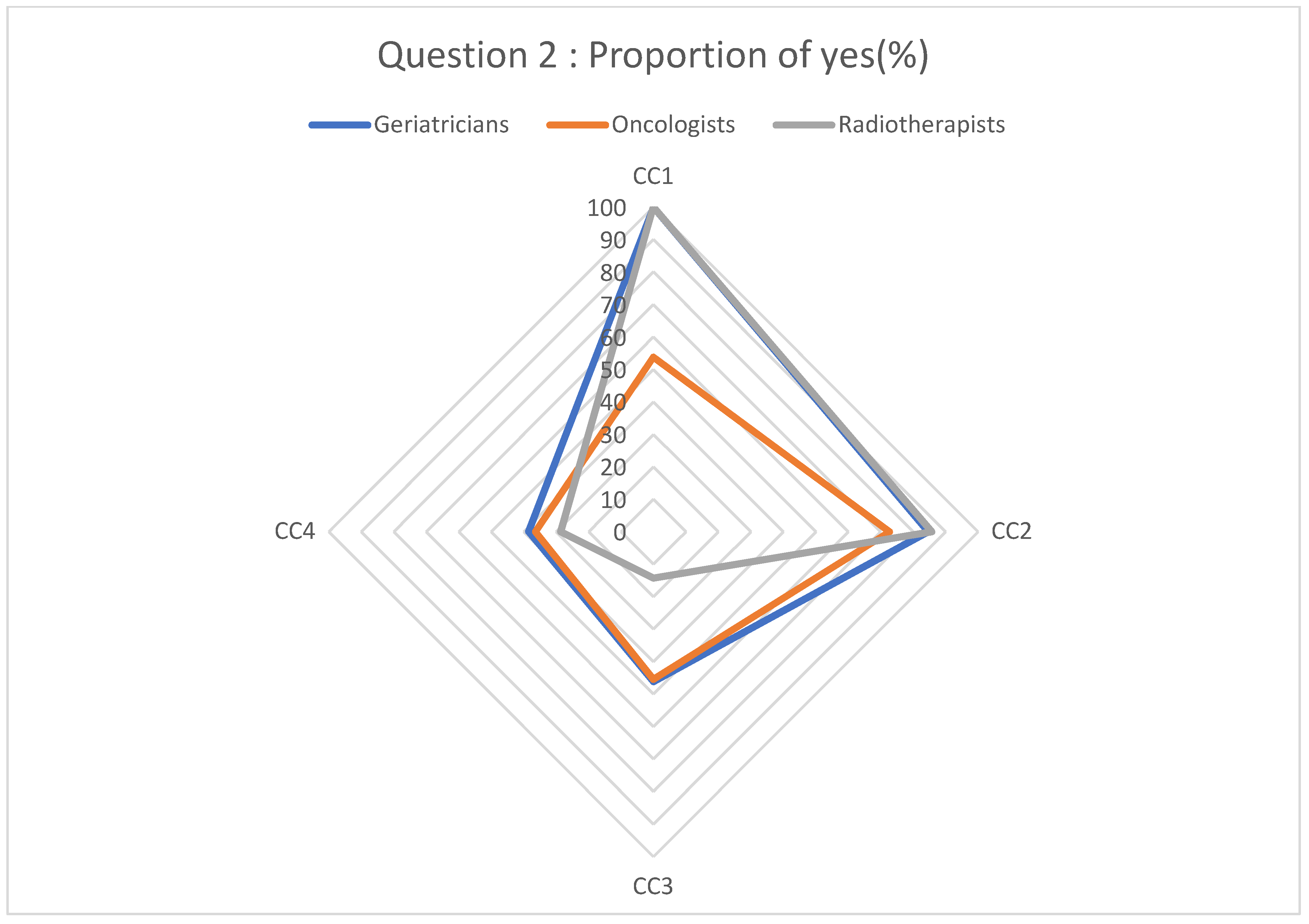
- Question 2: Would you perform surgery if it were necessary for this patient?
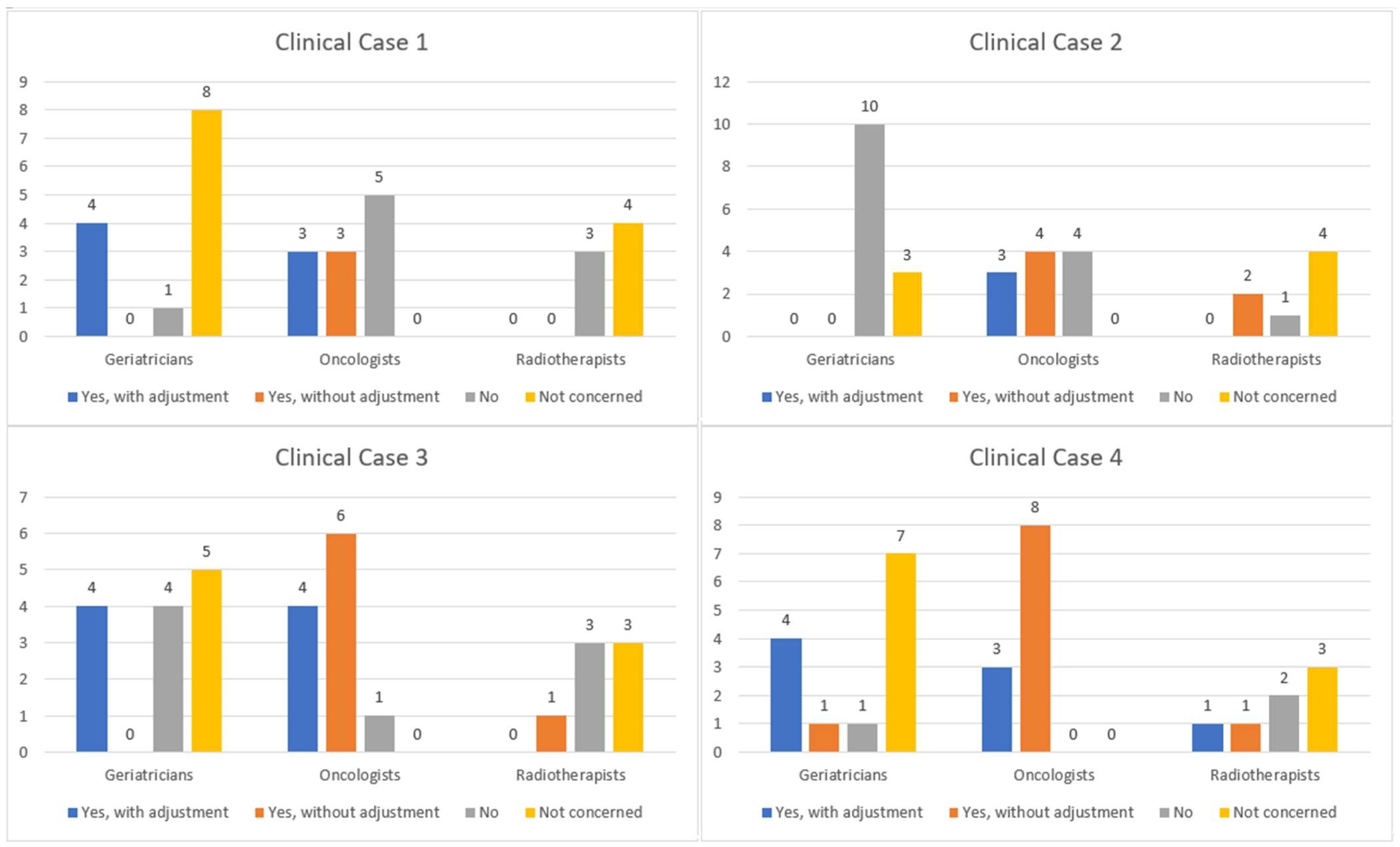
- Question 3: Would you agree to prescribe chemotherapy for this patient (if chemotherapy was indicated)?
- Question 4: Would you consider adjusting the dose of chemotherapy for this patient (if chemotherapy was indicated)?
- Question 5: What are the criteria that would guide your diagnostic approach of this clinical case?
- Question 6: What are the criteria that would affect your therapeutic approach of this clinical situation?
3. Results
3.1. Respondent Characteristics
3.2. Analysis Clinical Cases
3.3. Analysis of Question 5: What Are the Criteria That Would Guide Your Diagnostic Approach to This Clinical Case?
3.4. Analysis of Question 6: What Are the Criteria That Would Affect Your Therapeutic Approach to This Clinical Situation?
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Direction de la Recherche, des Etudes, de L’évaluation et des Statistiques/Santé Publique France. Principales causes de décès et de morbidité. In L’état De de la Population en France Rapport. 2017. Available online: https://drees.solidarites-sante.gouv.fr/publications-documents-de-reference/rapports/letat-de-sante-de-la-population-en-france-rapport-2017 (accessed on 1 March 2023).
- INSEE. Tableaux de l’Economie Française; INSEE: Paris, France, 2016. Available online: https://www.insee.fr/fr/statistiques/1906743 (accessed on 1 March 2023).
- INCa. Incidence et Mortalité Nationale; Institut National Du Cancer: Boulogne, France, 2017. [Google Scholar]
- Registre des cancers du Tarn 2010-2013 Réseau Oncomip. Available online: https://onco-occitanie.fr/registre-des-cancers-du-tarn/ (accessed on 1 March 2023).
- Baban, C.K.; Devane, L.; Geraghty, J. Change of paradigm in treating elderly with breast cancer: Are we undertreating elderly patients? Ir. J. Med. Sci. 2019, 188, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Swaminathan, D.; Swaminathan, V. Geriatric oncology: Problems with under-treatment within this population. Cancer Biol. Med. 2015, 12, 275–283. [Google Scholar]
- Ginoux, M.; Turquier, S.; Chebib, N.; Glerant, J.C.; Traclet, J.; Philit, F.; Sénéchal, A.; Mornex, J.-F.; Cottin, V. Impact of comorbidities and delay in diagnosis in elderly patients with pulmonary hypertension. ERJ Open Res. 2018, 4, 00100-2018. [Google Scholar] [CrossRef] [PubMed]
- Sarfati, D.; Koczwara, B.; Jackson, C. The impact of comorbidity on cancer and its treatment. CA Cancer J. Clin. 2016, 66, 337–350. [Google Scholar] [CrossRef]
- Delbaldo, C.; Caillet, P.; Pouessel, D.; Paillaud, E.; Culine, S. Spécificités de la prise en charge par chimiothérapie chez le sujet âgé. Prog. En Urol. 2009, 19, S100–S105. [Google Scholar] [CrossRef]
- Mangerel, K.; Armand-Branger, S.; Rhalimi, M. Spécificités de la personne âgée et leurs conséquences sur la prise en charge médicamenteuse. J. Pharm. Clin. 2011, 30, 167–173. [Google Scholar]
- Balducci, L.; Extermann, M. Cancer chemotherapy in the older patient: What the medical oncologist needs to know. Cancer 1997, 80, 1317–1322. [Google Scholar] [CrossRef]
- Balducci, L.; Extermann, M. Management of Cancer in the Older Person: A Practical Approach. Oncologist 2000, 5, 224–237. [Google Scholar] [CrossRef] [PubMed]
- Extermann, M.; Aapro, M.; Bernabei, R.; Cohen, H.J.; Droz, J.P.; Lichtman, S.; Mor, V.; Monfardini, S.; Repetto, L.; Sørbye, L.; et al. Use of comprehensive geriatric assessment in older cancer patients: Recommendations from the task force on CGA of the International Society of Geriatric Oncology (SIOG). Crit. Rev. Oncol. Hematol. 2005, 55, 241–252. [Google Scholar] [CrossRef]
- Soubeyran, P.; Bellera, C.; Goyard, J.; Heitz, D.; Cure, H.; Rousselot, H.; Albrand, G.; Servent, V.; Jean, O.S.; Roy, C.; et al. Validation of the screening tool in geriatric oncology: The ONCODAGE project. J. Clin. Oncol. 2011, 29, 9001. [Google Scholar] [CrossRef]
- Brunello, A.; Fontana, A.; Zafferri, V.; Panza, F.; Fiduccia, P.; Basso, U.; Copetti, M.; Lonardi, S.; Roma, A.; Falci, C.; et al. Development of an oncological-multidimensional prognostic index (Onco-MPI) for mortality prediction in older cancer patients. J. Cancer Res. Clin. Oncol. 2016, 142, 1069–1077. [Google Scholar] [CrossRef]
- Wildiers, H.; Heeren, P.; Puts, M.; Topinkova, E.; Janssen-Heijnen, M.L.G.; Extermann, M.; Falandry, C.; Artz, A.; Brain, E.; Colloca, G.; et al. International Society of Geriatric Oncology consensus on geriatric assessment in older patients with cancer. J. Clin. Oncol. Off J. Am. Soc. Clin. Oncol. 2014, 32, 2595–2603. [Google Scholar] [CrossRef]
- Caillet, P.; Canoui-Poitrine, F.; Vouriot, J.; Berle, M.; Reinald, N.; Krypciak, S.; Bastuji-Garin, S.; Culine, S.; Paillaud, E. Comprehensive geriatric assessment in the decision-making process in elderly patients with cancer: ELCAPA study. J. Clin. Oncol. Off J. Am. Soc. Clin. Oncol. 2011, 29, 3636–3642. [Google Scholar] [CrossRef]
- Aliamus, V.; Adam, C.; Druet-Cabanac, M.; Dantoine, T.; Vergnenegre, A. Impact de l’évaluation gériatrique sur la décision de traitement en oncologie thoracique. Rev. Mal. Respir. 2011, 28, 1124–1130. [Google Scholar] [CrossRef]
- Brugel, L.; Laurent, M.; Caillet, P.; Radenne, A.; Durand-Zaleski, I.; Martin, M.; Baron, M.; De Kermadec, H.; Bastuji-Garin, S.; Canouï-Poitrine, F.; et al. Impact of comprehensive geriatric assessment on survival, function, and nutritional status in elderly patients with head and neck cancer: Protocol for a multicentre randomised controlled trial (EGeSOR). BMC Cancer 2014, 14, 427. [Google Scholar] [CrossRef]
- Kalsi, T.; Babic-Illman, G.; Ross, P.J.; Maisey, N.R.; Hughes, S.; Fields, P.; Martin, F.C.; Wang, Y.; Harari, D. The impact of comprehensive geriatric assessment interventions on tolerance to chemotherapy in older people. Br. J. Cancer 2015, 112, 1435–1444. [Google Scholar] [CrossRef]
- Damhuis, R.A.M.; Meurs, C.J.C.; Meijer, W.S. Postoperative mortality after cancer surgery in octogenarians and nonagenarians: Results from a series of 5390 patients. World J. Surg. Oncol. 2005, 3, 71. [Google Scholar] [CrossRef] [PubMed]
- Paruch, J.L.; Ko, C.Y.; Bilimoria, K.Y. An opportunity to improve informed consent and shared decision making: The role of the ACS NSQIP Surgical Risk Calculator in oncology. Ann. Surg. Oncol. 2014, 21, 5–7. [Google Scholar] [CrossRef] [PubMed]
- Shahrokni, A.; Tin, A.L.; Sarraf, S.; Alexander, K.; Sun, S.; Kim, S.J.; McMillan, S.; Yulico, H.; Amirnia, F.; Downey, R.J.; et al. Association of Geriatric Comanagement and 90-Day Postoperative Mortality Among Patients Aged 75 Years and Older with Cancer. JAMA Netw. Open. 2020, 3, e209265. [Google Scholar] [CrossRef] [PubMed]
- Repetto, L. Greater risks of chemotherapy toxicity in elderly patients with cancer. J. Support Oncol. 2003, 1 (4 Suppl. 2), 18–24. [Google Scholar]
- Hall, P.S.; Swinson, D.; Waters, J.S.; Wadsley, J.; Falk, S.; Roy, R.; Tillett, T.; Nicoll, J.; Cummings, S.; Grumett, S.A.; et al. Optimizing Chemotherapy for Frail and Elderly Patients with Advanced Gastroesophageal Cancer: The GO2 Phase III Trial; Abstract 4006. In Proceedings of the 2019 ASCO, Annual Meeting, Chicago, IL, USA, 2 June 2019. [Google Scholar]
- Duverger, C.; Tardy, B.; Richard, A.; Célarier, T.; Bayle, S.; Cambou, M.; Perrot, J.L.; Cathebras, P.; Gonthier, R.; Fédération de Soins Palliatifs de Saint Etienne. Prophylactic treatment of venous thromboembolic disease in palliative care. A survey about four different clinical cases. Presse Med. 2009, 38, 1235–1239. [Google Scholar] [CrossRef] [PubMed]
- Boyle, H.; Girre, V.; Mertens, C.; Falandry, C.; Gouttenoire, F.; Freyer, G.; Brain, E.G.C. Recherche clinique en oncogériatrie. Oncologie 2009, 11, 331–336. [Google Scholar] [CrossRef]
- Pallis, A.G.; Ring, A.; Fortpied, C.; Penninckx, B.; Van Nes, M.C.; Wedding, U.; Vonminckwitz, G.; Johnson, C.D.; Wyld, L.; Timmer-Bonte, A.; et al. EORTC workshop on clinical trial methodology in older individuals with a diagnosis of solid tumors. Ann. Oncol. Off J. Eur. Soc. Med. Oncol. 2011, 22, 1922–1926. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Case 1 | Clinical Case 2 | Clinical Case 3 | Clinical Case 4 | |
|---|---|---|---|---|
| Cancer | Multifocal infiltrating ductal carcinoma of the right breast, SBR III, RO+ 100%, RP+ 80%, Her2++ with negative FISH, Ki67 at 60% | Well-differentiated Lieberkuhnian adenocarcinoma of the middle rectum | Adenocarcinoma of the pancreas with peritoneal carcinosis | Locally advanced middle-lobe bronchial adenocarcinoma, stage 3A N2cT2b |
| Sex | Female | Male | Female | Male |
| Age | 84 | 76 | 80 | 78 |
| Technical aids | Cane | Rollator | None | None |
| Home care | None | Wireless caregiver pager Nurse Homemaker service | None | Homemaker service |
| Allergy | None | Penicillin | None | None |
| Toxics | 2 glasses of alcohol per day | Tobacco 30PA | None | Tobacco 50 PA; 3 glasses of alcohol per day |
| Antecedents | Hysterectomy on fibroids | Bilateral total hip replacement Appendectomy | Left breast cancer treated in 1999 (mastectomy and radiotherapy) Right total hip replacement | Cholecystectomy Tonsillectomy |
| Comorbidities | Hypertension Gonarthrosis Anxiety and depression syndrome Age-related macular degeneration Chronic glaucoma Chronic renal failure Restrictive respiratory disorders | Obliterating arteriopathy of the lower limbs Anxiety and depression syndrome Alzheimer’s disease | Hypertension Migraines Rheumatoid arthritis Atrial fibrillation | Hypertension Hypothyroidism Chronic obstructive pulmonary disease |
| Number of medicines | 7 | 2 | 10 | 3 |
| Karnofsky(%)/ECOG performance status | K80-PS1 | K50-PS2 | K80-PS1 | K90-PS1 |
| ADL | 6/6 | 3/6 | 6/6 | 6/6 |
| IADL | 2/4 | 0/4 | 4/4 | 3/4 |
| MMS | 27/30 | 18/30 | 26/30 | 24/30 |
| Mini GDS–GDS | 0/4–Not realized | 3/4–12/15 | 0/4–Not realized | 1/4–6/15 |
| Neurosensory deficit | Blindness | None | Presbyopia + Myopia | Presbyopia + Presbycusis |
| Fall | None | 3 in the last year | None | 1 in the last year |
Nutritional assessment:
| 20.32 kg/m2 10/14 18/30 33 g/L | 23.66 kg/m2 12/14 Not realized 38.2 g/L | 22.03 kg/m2 13/14 Not realized 39 g/L | 24.4 kg/m2 12/14 Not realized 38 g/L |
| Sleep | Disturbed | Correct | Correct | Correct |
| Physical activity | 1.0 m/s | 0.7 m/s | 0.9 m/s | 0.9 m/s |
| Muscular strength | Normal | Significantly reduced | Normal | Normal |
| Mobility: TUG | 11 s | 23 s | 20 s | 14 s |
| Motor performance | 6/10 | 4/10 | 8/10 | 9/10 |
| G8 score | 8/17 | 7.5/17 | 12/17 | 10/17 |
| Geriatricians n = 13 | Oncologists n = 11 | Radiotherapists n = 7 | |
|---|---|---|---|
| -Gender: | |||
|
|
|
|
|
|
|
|
| -Years of professional experience | |||
|
|
|
|
|
|
|
|
| Geriatricians | Oncologists | Radiotherapists |
|---|---|---|
| Cognitive assessment (81%) | Comorbidities (75%) | Comorbidities (71%) |
| ADL score (75%) | Cognitive assessment (75%) | Karnofsky and ECOG performance status scoring (68%) |
| Comorbidities (73%) | Karnofsky and ECOG performance status scoring (71%) | Antecedents (46%) |
| IADL score (60%) | Antecedents (50%) | G8 score (39%) |
| Nutritional assessment (60%) | Nutritional assessment (46%) | Age (32%) |
| Assessment of mobility (56%) | Age (39%) | Cognitive assessment (32%) |
| Physical activity assessment (42%) | G8 score (36%) | None (25%) |
| Age (39%) | Number of falls during the year (34%) | Nutritional assessment (21%) |
| Karnofsky and ECOG performance status scoring (31%) | Home care aids (25%) | Number of falls during the year (18%) |
| Assessment of motor performance (31%) | Assessment of muscle strength (23%) | ADL score (11%) |
| Number of falls during the year (29%) | Neurosensory deficit (18%) | IADL score (11%) |
| Assessment of muscle strength (27%) | None (18%) | Neurosensory deficit (4%) |
| Antecedents (14%) | IADL score (16%) | Sleep assessment (4%) |
| Number of medicines (14%) | Assessment of mobility (16%) | Sex (0%) |
| Neurosensory deficit (14%) | ADL score (14%) | Number of medicines (0%) |
| Mini-GDS/GDS (12%) | Physical activity assessment (14%) | Mini-GDS/GDS (0%) |
| Home care aids (12%) | Mini-GDS/GDS (11%) | Home care aids (0%) |
| None (12%) | Assessment of motor performance (9%) | Physical activity assessment (0%) |
| G8 score (8%) | Number of medicines (7%) | Assessment of muscle strength (0%) |
| Sleep assessment (8%) | Sleep assessment (5%) | Assessment of mobility (0%) |
| Sex (0%) | Sex (2%) | Assessment of motor performance (0%) |
| Geriatricians | Oncologists | Radiotherapists |
|---|---|---|
| Comorbidities (87%) | Karnofsky and ECOG performance status scoring (89%) | Comorbidities (100%) |
| Cognitive assessment (79%) | Comorbidities (86%) | Karnofsky and ECOG performance status scoring (96%) |
| Nutritional assessment (77%) | Cognitive assessment (80%) | Antecedents (79%) |
| ADL score (73%) | Nutritional assessment (80%) | G8 score (75%) |
| Assessment of mobility (65%) | Antecedents (59%) | Cognitive assessment (64%) |
| IADL score (58%) | Age (55%) | Nutritional assessment (64%) |
| Number of falls during the year (56%) | Home care aids (55%) | Age (57%) |
| Physical activity assessment (52%) | Number of falls during the year (50%) | Home care aids (14%) |
| Karnofsky and ECOG performance status scoring (44%) | Assessment of mobility (43%) | Assessment of mobility (14%) |
| Assessment of motor performance (44%) | G8 score (41%) | IADL score (14%) |
| Age (42%) | IADL score (36%) | ADL score (14%) |
| Number of medicines (42%) | ADL score (34%) | Number of falls during the year (11%) |
| Home care aids (39%) | Assessment of motor performance (32%) | Neurosensory deficit (11%) |
| Assessment of muscle strength (37%) | Assessment of muscle strength (27%) | Number of medicines (11%) |
| G8 score (29%) | Neurosensory deficit (27%) | Mini-GDS/GDS (4%) |
| Neurosensory deficit (27%) | Physical activity assessment (25%) | Sex (4%) |
| Mini-GDS/GDS (23%) | Number of medicines (21%) | Assessment of motor performance (0%) |
| Sleep assessment (19%) | Mini-GDS / GDS (21%) | Assessment of muscle strength (0%) |
| Antecedents (12%) | Sleep assessment (9%) | Physical activity assessment (0%) |
| None (6%) | None (2%) | Sleep assessment (0%) |
| Sex (0%) | Sex (0%) | None (0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lafaie, L.; Chanelière-Sauvant, A.-F.; Magné, N.; Bouleftour, W.; Tinquaut, F.; Célarier, T.; Bertoletti, L. Impact of Medical Specialties on Diagnostic and Therapeutic Management of Elderly Cancer Patients. Geriatrics 2023, 8, 62. https://doi.org/10.3390/geriatrics8030062
Lafaie L, Chanelière-Sauvant A-F, Magné N, Bouleftour W, Tinquaut F, Célarier T, Bertoletti L. Impact of Medical Specialties on Diagnostic and Therapeutic Management of Elderly Cancer Patients. Geriatrics. 2023; 8(3):62. https://doi.org/10.3390/geriatrics8030062
Chicago/Turabian StyleLafaie, Ludovic, Anne-Françoise Chanelière-Sauvant, Nicolas Magné, Wafa Bouleftour, Fabien Tinquaut, Thomas Célarier, and Laurent Bertoletti. 2023. "Impact of Medical Specialties on Diagnostic and Therapeutic Management of Elderly Cancer Patients" Geriatrics 8, no. 3: 62. https://doi.org/10.3390/geriatrics8030062