

Associations between Physical Activity and Health-Related Quality of Life among Community-Dwelling Older Adults: A Cross-Sectional Study in Urban Greece
 , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Objective
3. Materials and Methods
3.1. Study Materials
3.2. Ethical Approval
3.3. Data Collection
3.4. Instruments
3.4.1. Short-Form Health Survey (SF-36)
3.4.2. International Physical Activity Questionnaire (IPAQ)
3.5. Data Analysis
4. Results
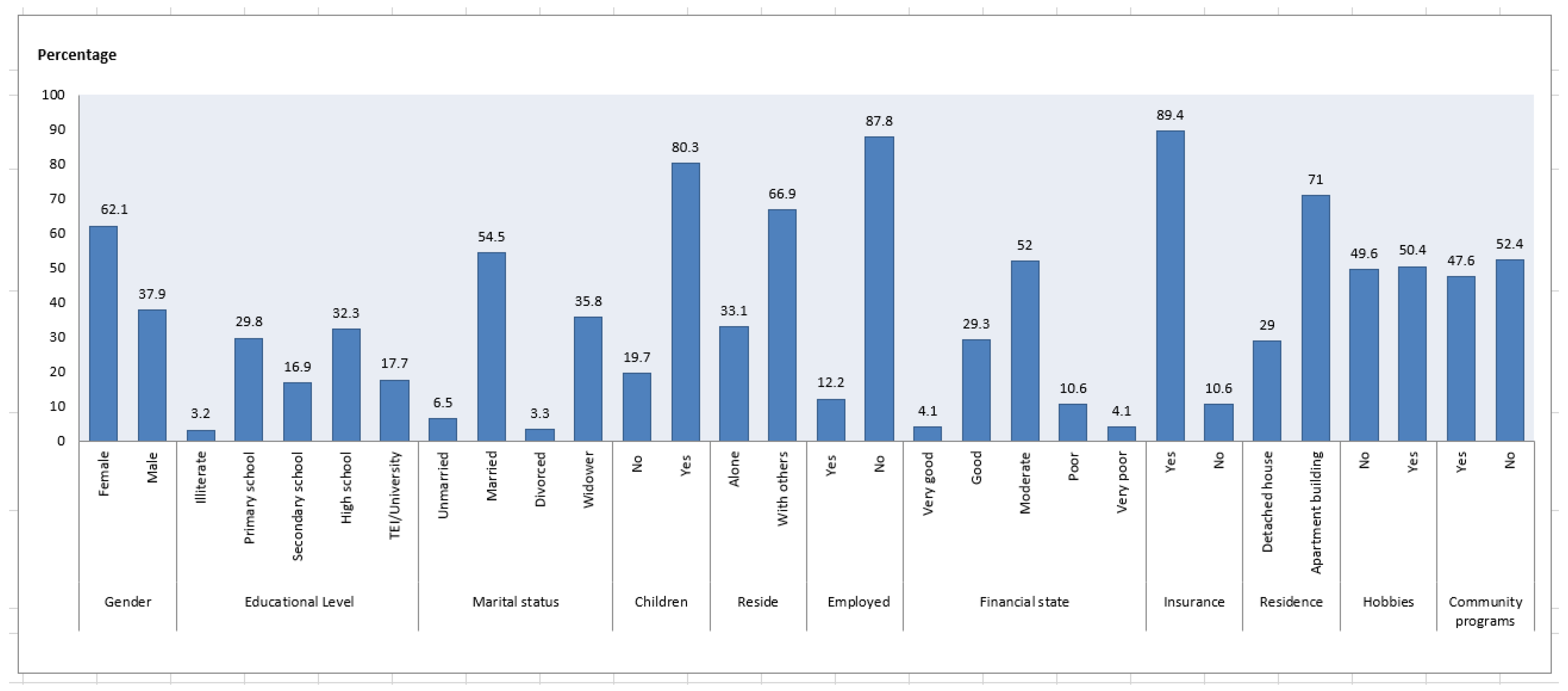
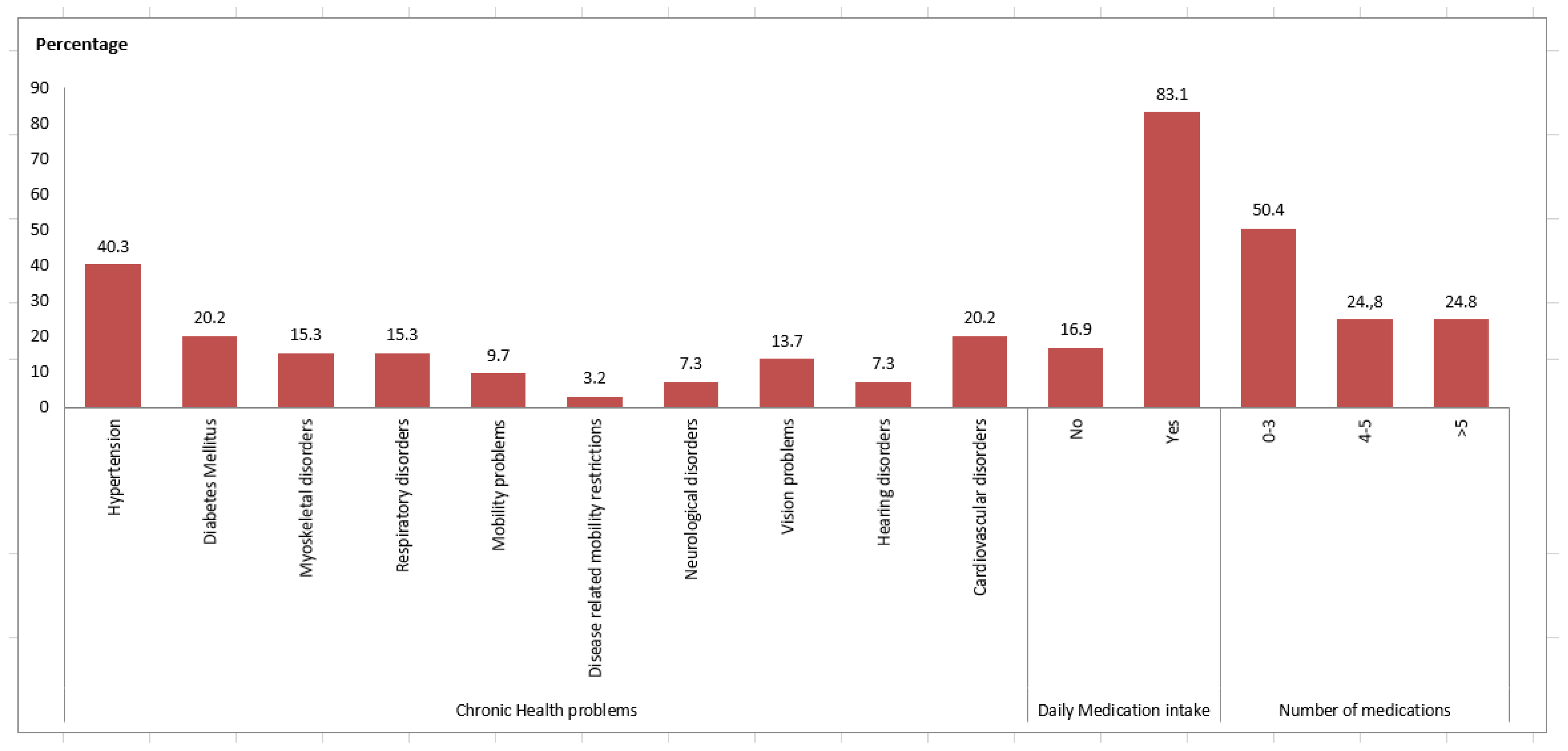
Demographic and Clinical Characteristics
5. Discussion
Study Limitations
6. Conclusions and Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gkouvas, K.C.; Soulis, G.; Panagiotakos, D.B. The Multiple Dimensions of the Ageing Process; What Do We Know about Them? Arch. Hell. Med. 2018, 35, 757–764. [Google Scholar]
- WHO. Healthy Ageing and Functional Ability. 2020. Available online: https://www.who.int/news-room/questions-and-answers/item/healthy-ageing-and-functional-ability (accessed on 23 March 2023).
- Balboa-Castillo, T.; León-Muñoz, L.M.; Graciani, A.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. Longitudinal Association of Physical Activity and Sedentary Behavior during Leisure Time with Health-Related Quality of Life in Community-Dwelling Older Adults. Health Qual. Life Outcomes 2011, 9, 47. [Google Scholar] [CrossRef]
- Makino, K.; Ihira, H.; Mizumoto, A.; Shimizu, K.; Ishida, T.; Furuna, T. Associations between the Settings of Exercise Habits and Health-Related Outcomes in Community-Dwelling Older Adults. J. Phys. Ther. Sci. 2015, 27, 2207–2211. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.R.; Bredin, S.S.D. Health Benefits of Physical Activity: A Systematic Review of Current Systematic Reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef] [PubMed]
- Daimiel, L.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Schröder, H.; Vioque, J.; Romaguera, D.; Martínez, J.A.; Wärnberg, J.; Lopez-Miranda, J.; et al. Physical Fitness and Physical Activity Association with Cognitive Function and Quality of Life: Baseline Cross-Sectional Analysis of the PREDIMED-Plus Trial. Sci. Rep. 2020, 10, 3472. [Google Scholar] [CrossRef] [PubMed]
- Lepsy, E.; Radwańska, E.; Żurek, G.; Żurek, A.; Kaczorowska, A.; Radajewska, A.; Kołcz, A. Association of Physical Fitness with Quality of Life in Community-Dwelling Older Adults Aged 80 and over in Poland: A Cross-Sectional Study. BMC Geriatr. 2021, 21, 491. [Google Scholar] [CrossRef] [PubMed]
- Psarrou, A.; Adamakidou, T.; Plakas, S.; Mastrogiannis, D.; Drakopoulou, M.; Mantzorou, M. Physical Activity and Quality of Life in Community-Dwelling Older Adults. Eur. Geriatr. Med. 2022, 13 (Suppl. S1), 299. [Google Scholar]
- Pinheiro, M.B.; Oliveira, J.S.; Baldwin, J.N.; Hassett, L.; Costa, N.; Gilchrist, H.; Wang, B.; Kwok, W.; Albuquerque, B.S.; Pivotto, L.R.; et al. Impact of Physical Activity Programs and Services for Older Adults: A Rapid Review. Int. J. Behav. Nutr. Phys. Act. 2022, 19, 87. [Google Scholar] [CrossRef]
- Hills, A.P.; Street, S.J.; Byrne, N.M. Physical Activity and Health. In Advances in Food and Nutrition Research; Elsevier: Amsterdam, The Netherlands, 2015; Volume 75, pp. 77–95. [Google Scholar] [CrossRef]
- Hamer, M.; Lavoie, K.L.; Bacon, S.L. Taking up Physical Activity in Later Life and Healthy Ageing: The English Longitudinal Study of Ageing. Br. J. Sports Med. 2014, 48, 239–243. [Google Scholar] [CrossRef]
- Park, S.-A.; Son, S.Y.; Lee, A.-Y.; Park, H.-G.; Lee, W.-L.; Lee, C.H. Metabolite Profiling Revealed That a Gardening Activity Program Improves Cognitive Ability Correlated with BDNF Levels and Serotonin Metabolism in the Elderly. IJERPH 2020, 17, 541. [Google Scholar] [CrossRef]
- Scott, T.L.; Masser, B.M.; Pachana, N.A. Positive Ageing Benefits of Home and Community Gardening Activities: Older Adults Report Enhanced Self-Esteem, Productive Endeavours, Social Engagement and Exercise. SAGE Open. Med. 2020, 8, 205031212090173. [Google Scholar] [CrossRef]
- Leyland, L.-A.; Spencer, B.; Beale, N.; Jones, T.; Van Reekum, C.M. The Effect of Cycling on Cognitive Function and Well-Being in Older Adults. PLoS ONE 2019, 14, e0211779. [Google Scholar] [CrossRef]
- Cornwell, B.; Laumann, E.O. The Health Benefits of Network Growth: New Evidence from a National Survey of Older Adults. Soc. Sci. Med. 2015, 125, 94–106. [Google Scholar] [CrossRef] [PubMed]
- Zilidou, B.; Duka, S.; Tsolaki, M. The Results of an Intervention Program of Traditional Dances, as a Recreational Activity, Improving the Quality of Life of Senior Citizens at the Municipality of Thessaloniki. Hell. J. Sport. Recreat. Manag. 2015, 12, 13–25. [Google Scholar]
- Douka, S.; Zilidou, V.I.; Lilou, O.; Tsolaki, M. Greek Traditional Dances: A Way to Support Intellectual, Psychological, and Motor Functions in Senior Citizens at Risk of Neurodegeneration. Front. Ageing Neurosci. 2019, 11, 6. [Google Scholar] [CrossRef] [PubMed]
- Moustakopoulou, L. Study of Fear, Loneliness and Depression in Older Adults during the COVID-19 Pandemic. Master’s Thesis, University of West Attica, Athens, Greece, 2022. Available online: https://polynoe.lib.uniwa.gr/xmlui/handle/11400/3539?locale-attribute=en (accessed on 1 March 2023).
- Liu, Y.; Tamura, R.; Song, Y. Constructing a Smart Home for Future Elders toward All-around Happiness: Taking Connectivity as the Core Element. Appl. Sci. 2020, 10, 5690. [Google Scholar] [CrossRef]
- Scarabottolo, C.C.; Cyrino, E.S.; Nakamura, P.M.; Tebar, W.R.; da Canhin, D.S.; Gobbo, L.A.; Christofaro, D.G.D. Relationship of Different Domains of Physical Activity Practice with Health-Related Quality of Life among Community-Dwelling Older People: A Cross-Sectional Study. BMJ Open 2019, 9, e027751. [Google Scholar] [CrossRef]
- Bădicu, G. Physical Activity and Health-Related Quality of Life in Adults from Braşov, Romania. Educ. Sci. 2018, 8, 52. [Google Scholar] [CrossRef]
- Subramaniam, M.; Zhang, Y.; Lau, J.H.; Vaingankar, J.A.; Abdin, E.; Chong, S.A.; Lee, E.S. Patterns of Physical Activity and Health-Related Quality of Life amongst Patients with Multimorbidity in a Multi-Ethnic Asian Population. BMC Public Health 2019, 19, 1612. [Google Scholar] [CrossRef]
- Dechamps, A. Effects of Exercise Programs to Prevent Decline in Health-Related Quality of Life in Highly Deconditioned Institutionalized Elderly Persons: A Randomized Controlled Trial. Arch Intern. Med. 2010, 170, 162. [Google Scholar] [CrossRef]
- Taguchi, N.; Higaki, Y.; Inoue, S.; Kimura, H.; Tanaka, K. Effects of a 12-Month Multicomponent Exercise Program on Physical Performance, Daily Physical Activity, and Quality of Life in Very Elderly People With Minor Disabilities: An Intervention Study. J. Epidemiol. 2010, 20, 21–29. [Google Scholar] [CrossRef]
- Mavrovouniotis, F.H.; Argiriadou, E.A.; Papaioannou, C.S. Greek Traditional Dances and Quality of Old People’s Life. J. Bodyw. Mov. Ther. 2010, 14, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Tzonichaki, I.; Malikiosi-Loizos, M.; Kleftaras, G. The Role of Level of Functioning, Life Satisfaction and Leisure Activities in Elderly Depressive Symptomatology. Rostrum Asclepius 2013, 12, 409–427. [Google Scholar]
- Hall, G.; Laddu, D.R.; Phillips, S.A.; Lavie, C.J.; Arena, R. A Tale of Two Pandemics: How Will COVID-19 and Global Trends in Physical Inactivity and Sedentary Behavior Affect One Another? Prog. Cardiovasc. Dis. 2021, 64, 108–110. [Google Scholar] [CrossRef]
- Ware, J.Ε.; Sherbourne, C.D. The MOS 36-Item Short-Form Health Survey (SF-36): I. Conceptual Framework and Item Selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E. The SF-36 Health Survey. A Manual and Interpretation Guide; The Health Institute, New England Medical Center: Boston, MA, USA, 1993. [Google Scholar]
- Anagnostopoulos, F.; Niakas, D.; Pappa, E. Construct Validation of the Greek SF-36 Health Survey. Qual. Life Res. 2005, 14, 1959–1965. [Google Scholar] [CrossRef]
- Pappa, E.; Kontodimopoulos, N.; Niakas, D. Validating and Norming of the Greek SF-36 Health Survey. Qual. Life Res. 2005, 14, 1433–1438. [Google Scholar] [CrossRef]
- Talwar, A.; Sahni, S.; Kim, E.J.; Verma, S.; Kohn, N. Dyspnea, Depression and Health Related Quality of Life in Pulmonary Arterial Hypertension Patients. J. Exerc. Rehabil. 2015, 11, 259–265. [Google Scholar] [CrossRef]
- Taft, C.; Karlsson, J.; Sullivan, M. Do SF-36 Summary Component Scores Accurately Summarize Subscale Scores? Qual. Life Res. 2001, 10, 395–404. [Google Scholar] [CrossRef]
- Ware, J. SF-36 Health Survey Update. Spine 2000, 25, 3130–3139. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sport. Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Papathanasiou, G.; Georgoudis, G.; Papandreou, M.; Spyropoulos, P.; Georgakopoulos, D.; Kalfakakou, V.; Evangelou, A. Reliability Measures of the Short International Physical Activity Questionnaire (IPAQ) in Greek Young Adults. Hell. J. Cardiol. 2009, 50, 283–294. [Google Scholar]
- IPAQ Research Committee Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ)—Short form. Physiopedia. 2004. Available online: https://www.physiopedia.com/images/c/c7/Quidelines_for_interpreting_the_IPAQ.pdf (accessed on 15 April 2023).
- Kolbe-Alexander, T.L.; Lambert, E.V.; Harkins, J.B.; Ekelund, U. Comparison of Two Methods of Measuring Physical Activity in South African Older Adults. J. Aging Phys. Act. 2006, 14, 98–114. [Google Scholar] [CrossRef] [PubMed]
- Van Holle, V.; De Bourdeaudhuij, I.; Deforche, B.; Van Cauwenberg, J.; Van Dyck, D. Assessment of Physical Activity in Older Belgian Adults: Validity and Reliability of an Adapted Interview Version of the Long International Physical Activity Questionnaire (IPAQ-L). BMC Public Health 2015, 15, 433. [Google Scholar] [CrossRef] [PubMed]
- Tomioka, K.; Iwamoto, J.; Saeki, K.; Okamoto, N. Reliability and Validity of the International Physical Activity Questionnaire (IPAQ) in Elderly Adults: The Fujiwara-Kyo Study. J. Epidemiol. 2011, 21, 459–465. [Google Scholar] [CrossRef]
- Cerin, E.; Barnett, A.; Cheung, M.; Sit, C.H.P.; Macfarlane, D.J.; Chan, W. Reliability and Validity of the IPAQ-L in a Sample of Hong Kong Urban Older Adults: Does Neighborhood of Residence Matter? J. Aging Phys. Act. 2012, 20, 402–420. [Google Scholar] [CrossRef]
- Cleland, C.; Ferguson, S.; Ellis, G.; Hunter, R.F. Validity of the International Physical Activity Questionnaire (IPAQ) for Assessing Moderate-to-Vigorous Physical Activity and Sedentary Behaviour of Older Adults in the United Kingdom. BMC Med. Res. Methodol. 2018, 18, 176. [Google Scholar] [CrossRef] [PubMed]
- Heesch, K.C.; Van Uffelen, J.G.; Hill, R.L.; Brown, W.J. What Do IPAQ Questions Mean to Older Adults? Lessons from Cognitive Interviews. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 35. [Google Scholar] [CrossRef]
- Karapanou, O.; Papadopoulos, A.; Vlassopoulou, B.; Vassilopoulos, C.; Pappa, E.; Tsagarakis, S.; Niakas, D. Health status of Greek thyroid cancer patients after radioiodine administration compared to a demographically matched general population sample. Hell. J. Nucl. Med. 2012, 15, 98–102. [Google Scholar] [CrossRef]
- Sun, W.; Aodeng, S.; Tanimoto, Y.; Watanabe, M.; Han, J.; Wang, B.; Yu, L.; Kono, K. Quality of Life (QOL) of the Community-Dwelling Elderly and Associated Factors: A Population-Based Study in Urban Areas of China. Arch. Gerontol. Geriatr. 2015, 60, 311–316. [Google Scholar] [CrossRef]
- Attafuah, P.Y.A.; Everink, I.; Abuosi, A.A.; Lohrmann, C.; Schols, J.M.G.A. Quality of Life of Older Adults and Associated Factors in Ghanaian Urban Slums: A Cross-Sectional Study. BMJ Open 2022, 12, e057264. [Google Scholar] [CrossRef]
- García-Fernández, L.; Romero-Ferreiro, V.; López-Roldán, P.D.; Padilla, S.; Rodriguez-Jimenez, R. Mental Health in Elderly Spanish People in Times of COVID-19 Outbreak. Am. J. Geriatr. Psychiatry 2020, 28, 1040–1045. [Google Scholar] [CrossRef] [PubMed]
- Webb, L.M.; Chen, C.Y. The COVID-19 Pandemic’s Impact on Older Adults’ Mental Health: Contributing Factors, Coping Strategies, and Opportunities for Improvement. Int. J. Geriat. Psychiatry 2022, 37. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.C.; Tou, N.X.; Low, J.A. A Comparative Study on Mental Health and Adaptability between Older and Younger Adults during the COVID-19 Circuit Breaker in Singapore. BMC Public Health 2022, 22, 507. [Google Scholar] [CrossRef]
- Koma, W.; True, S.; Fuglesten Biniek, J.; Cubanski, J.; Orgera, K.; Garfield, R. One in Four Older Adults Report Anxiety or Depression Amid the COVID-19 Pandemic. Medicare. 2020. Available online: https://www.kff.org/medicare/issue-brief/one-in-four-older-adults-report-anxiety-or-depression-amid-the-covid-19-pandemic/ (accessed on 5 April 2022).
- Meng, H.; Xu, Y.; Dai, J.; Zhang, Y.; Liu, B.; Yang, H. Analyze the Psychological Impact of COVID-19 among the Elderly Population in China and Make Corresponding Suggestions. Psychiatry Res. 2020, 289, 112983. [Google Scholar] [CrossRef] [PubMed]
- Tsekoura, M.; Kalampakos, N.; Fousekis, K.; Mylonas, K.; Angelopoulos, P.; Matzaroglou, C.; Bita, T.; Gliatis, J.; Tsepis, E.; Billis, E. Risk of Sarcopenia, Fear of COVID-19, Anxiety, Depression and Physical Activity Levels: Associations across Patients on Hemodialysis within Greece. JFSF 2023, 8, 32–37. [Google Scholar] [CrossRef]
- Roukounaki, M. Activity Levels of the Elderly in the COVID-19 Pandemic: A Research Study. Bachelor’s Thesis, University of Patras, Aigio, Greece, 2022. Available online: http://repository.library.teiwest.gr/xmlui/bitstream/handle/123456789/9904/%CE%A1%CE%9F%CE%A5%CE%9A%CE%9F%CE%A5%CE%9D%CE%91%CE%9A%CE%97.pdf?sequence=1&isAllowed=y (accessed on 6 April 2022).
- WHO Guidelines on Physical Activity and Sedentary Behaviour: At a Glance. 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/337001/9789240014886-eng.pdf?sequence=1&isAllowed=y (accessed on 25 March 2022).
- Babatsikou, F.; Gerogianni, G.; Zyga, S.; Koutis, C. Physical Activity in a Sample of Elderly Greek People: A Research Study. Health Sci. J. 2012, 6, 518–533. [Google Scholar]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical Activity in Older Age: Perspectives for Healthy Ageing and Frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical Activity and Public Health in Older Adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sport. Exerc. 2007, 39, 1435–1445. [Google Scholar] [CrossRef]
- Oliveira, M.R.; Sudati, I.P.; Konzen, V.D.M.; De Campos, A.C.; Wibelinger, L.M.; Correa, C.; Miguel, F.M.; Silva, R.N.; Borghi-Silva, A. COVID-19 and the Impact on the Physical Activity Level of Elderly People: A Systematic Review. Exp. Gerontol. 2022, 159, 111675. [Google Scholar] [CrossRef]
- Kahn, J.R.; McGill, B.S.; Bianchi, S.M. Help to Family and Friends: Are There Gender Differences at Older Ages? J. Marriage Fam. 2011, 73, 77–92. [Google Scholar] [CrossRef]
- Souza, A.M.R.; Fillenbaum, G.G.; Blay, S.L. Prevalence and Correlates of Physical Inactivity among Older Adults in Rio Grande Do Sul, Brazil. PLoS ONE 2015, 10, e0117060. [Google Scholar] [CrossRef] [PubMed]
- Sepúlveda-Loyola, W.; Rodríguez-Sánchez, I.; Pérez-Rodríguez, P.; Ganz, F.; Torralba, R.; Oliveira, D.V.; Rodríguez-Mañas, L. Impact of Social Isolation Due to COVID-19 on Health in Older People: Mental and Physical Effects and Recommendations. J. Nutr. Health Ageing 2020, 24, 938–947. [Google Scholar] [CrossRef]
- Ghram, A.; Briki, W.; Mansoor, H.; Al-Mohannadi, A.S.; Lavie, C.J.; Chamari, K. Home-Based Exercise Can Be Beneficial for Counteracting Sedentary Behavior and Physical Inactivity during the COVID-19 Pandemic in Older Adults. Postgrad. Med. 2021, 133, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D. Physical Activity Is Medicine for Older Adults. Postgrad. Med. J. 2014, 90, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, P.D.; Davis, R.E. Bouted and Non-Bouted Moderate-to-Vigorous Physical Activity with Health-Related Quality of Life. Prev. Med. Rep. 2016, 3, 46–48. [Google Scholar] [CrossRef]
- Van Leeuwen, K.M.; Van Loon, M.S.; Van Nes, F.A.; Bosmans, J.E.; De Vet, H.C.W.; Ket, J.C.F.; Widdershoven, G.A.M.; Ostelo, R.W.J.G. What Does Quality of Life Mean to Older Adults? A Thematic Synthesis. PLoS ONE 2019, 14, e0213263. [Google Scholar] [CrossRef]
- Gopinath, B.; Kifley, A.; Flood, V.M.; Mitchell, P. Physical Activity as a Determinant of Successful Ageing over Ten Years. Sci. Rep. 2018, 8, 10522. [Google Scholar] [CrossRef]
- Tricco, A.C.; Thomas, S.M.; Veroniki, A.A.; Hamid, J.S.; Cogo, E.; Strifler, L.; Khan, P.A.; Robson, R.; Sibley, K.M.; MacDonald, H.; et al. Comparisons of Interventions for Preventing Falls in Older Adults: A Systematic Review and Meta-Analysis. JAMA 2017, 318, 1687. [Google Scholar] [CrossRef]
- Fielding, R.A.; Guralnik, J.M.; King, A.C.; Pahor, M.; McDermott, M.M.; Tudor-Locke, C.; Manini, T.M.; Glynn, N.W.; Marsh, A.P.; Axtell, R.S.; et al. Dose of Physical Activity, Physical Functioning and Disability Risk in Mobility-Limited Older Adults: Results from the LIFE Study Randomized Trial. PLoS ONE 2017, 12, e0182155. [Google Scholar] [CrossRef]
- Zisopoulou, S.; Plakas, S.; Mastrogiannis, D.; Adamakidou, T.; Mantzorou, M. The Effect of E-Health Literacy on Adherence with Medication in Chronically Ill Patients. Intersci. Healthc. 2020, 12, 45–55. [Google Scholar]
- Shrestha, M.; Kc, H.; Bhattarai, P.; Mishra, A.; Parajuli, S.B. Quality of Life of Elderly People Living with Family and in Old Age Home in Morang District, Nepal. BIBECHANA 2018, 16, 221–227. [Google Scholar] [CrossRef]
- Conde-Sala, J.L.; Portellano-Ortiz, C.; Calvó-Perxas, L.; Garre-Olmo, J. Quality of Life in People Aged 65+ in Europe: Associated Factors and Models of Social Welfare—Analysis of Data from the SHARE Project (Wave 5). Qual. Life Res. 2017, 26, 1059–1070. [Google Scholar] [CrossRef] [PubMed]
- De Labra, C.; Maseda, A.; Lorenzo-López, L.; López-López, R.; Buján, A.; Rodríguez-Villamil, J.L.; Millán-Calenti, J.C. Social Factors and Quality of Life Aspects on Frailty Syndrome in Community-Dwelling Older Adults: The VERISAÚDE Study. BMC Geriatr. 2018, 18, 66. [Google Scholar] [CrossRef] [PubMed]
- Ha, N.T.; Duy, H.T.; Le, N.H.; Khanal, V.; Moorin, R. Quality of Life among People Living with Hypertension in a Rural Vietnam Community. BMC Public Health 2014, 14, 833. [Google Scholar] [CrossRef] [PubMed]
- Skevington, S.M. Qualities of Life, Educational Level and Human Development: An International Investigation of Health. Soc. Psychiat. Epidemiol. 2010, 45, 999–1009. [Google Scholar] [CrossRef] [PubMed]
- Marques, L.P.; Schneider, I.J.C.; d’Orsi, E. Quality of Life and Its Association with Work, the Internet, Participation in Groups and Physical Activity among the Elderly from the EpiFloripa Survey, Florianópolis, Santa Catarina State, Brazil. Cad. Saúde Pública 2016, 32, e00143615. [Google Scholar] [CrossRef] [PubMed]
- Cutler, D.M.; Lleras-Muney, A. Understanding Differences in Health Behaviors by Education. J. Health Econ. 2010, 29, 1–28. [Google Scholar] [CrossRef]
- Doležalová, J.; Tóthová, V.; Neugebauer, J.; Sadílek, P. Impact of Selected Geriatric Syndromes on the Quality of Life in the Population Aged 60 and Older. Healthcare 2021, 9, 657. [Google Scholar] [CrossRef]
- Ponirou, P.; Diomidous, M.; Kalokairinou, A.; Mantas, J.; Tsimahidou, C.; Tzavara, C. Document Details—Health Related Quality of Life in a Sample of Older People Who Are Members of Open Care Centers for the Elderly. In Studies in Health Technology and Informatics; Elsevier: Athens, Greece, 2014; Volume 202, pp. 269–272. [Google Scholar]
- Chin, Y.R.; Lee, I.S.; Lee, H.Y. Effects of Hypertension, Diabetes, and/or Cardiovascular Disease on Health-Related Quality of Life in Elderly Korean Individuals: A Population-Based Cross-Sectional Survey. Asian Nurs. Res. 2014, 8, 267–273. [Google Scholar] [CrossRef]
- Camelo, L.D.V.; Giatti, L.; Barreto, S.M. Qualidade de Vida Relacionada à Saúde Em Idosos Residentes Em Região de Alta Vulnerabilidade Para Saúde de Belo Horizonte, Minas Gerais. Rev. Bras. Epidemiol. 2016, 19, 280–293. [Google Scholar] [CrossRef]
- Joshi, M.R. Factors Determining Quality of Life of Elderly People in Rural Nepal. J. Gerontol. Geriatr. Res. 2020, 9, 1–7. [Google Scholar] [CrossRef]
- Crouch, A.; Champion, V.L.; Von Ah, D. Comorbidity, Cognitive Dysfunction, Physical Functioning, and Quality of Life in Older Breast Cancer Survivors. Support. Care Cancer 2022, 30, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Sadrollahi, A.; Hosseinian, M.; Masoudi Alavi, N.; Khalili, Z.; Esalatmanesh, S. Physical Activity Patterns in the Elderly Kashan Population. Iran. Red. Crescent Med. J. 2016, 18, e25008. [Google Scholar] [CrossRef] [PubMed]
- López-Sánchez, G.F.; López-Bueno, R.; Gil-Salmerón, A.; Zauder, R.; Skalska, M.; Jastrzębska, J.; Jastrzębski, Z.; Schuch, F.B.; Grabovac, I.; Tully, M.A.; et al. Comparison of Physical Activity Levels in Spanish Adults with Chronic Conditions before and during COVID-19 Quarantine. Eur. J. Public Health 2021, 31, 161–166. [Google Scholar] [CrossRef]
- Kwan, R.Y.C.; Liu, J.Y.W.; Yin, Y.-H.; Lee, P.H.; Ng, S.Y.; Cheung, D.S.K.; Kor, P.P.K.; Lam, S.C.; Lo, S.K.L.; Yang, L.; et al. Sarcopenia and Its Association with Objectively Measured Life-Space Mobility and Moderate-to-Vigorous Physical Activity in the Oldest-Old amid the COVID-19 Pandemic When a Physical Distancing Policy Is in Force. BMC Geriatr. 2022, 22, 250. [Google Scholar] [CrossRef] [PubMed]
- Harada, N.D.; Chiu, V.; King, A.C.; Stewart, A.L. An Evaluation of Three Self-Report Physical Activity Instruments for Older Adults. Med. Sci. Sports Exerc. 2001, 33, 962–970. [Google Scholar] [CrossRef]
- Stewart, A.L.; Mills, K.M.; King, A.C.; Haskell, W.L.; Gillis, D.; Ritter, P.L. CHAMPS Physical Activity Questionnaire for Older Adults: Outcomes for Interventions. Med. Sci. Sports Exerc. 2001, 33, 1126–1141. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Level | Ν | % |
|---|---|---|
| Low | 104 | 83.9 |
| Moderate | 11 | 8.9 |
| High | 9 | 7.3 |
| Subscales | Mean | Standard Deviation | Median | Lowest Value | Highest Value | Cronbach’s α |
|---|---|---|---|---|---|---|
| Physical Functioning (PF) | 69.7 | 30.8 | 75 | 0 | 100 | 0.94 |
| Role Functioning/Physical (RP) | 64.1 | 28.1 | 69 | 0 | 100 | 0.76 |
| Bodily Pain (BP) | 58.1 | 25.4 | 62 | 0 | 100 | 0.73 |
| General Health (GH) | 56.2 | 19.8 | 57 | 5 | 97 | 0.86 |
| Vitality (VT) | 57.7 | 20.6 | 63 | 6 | 100 | 0.89 |
| Social Functioning (SF) | 67.8 | 26.6 | 68 | 12.5 | 100 | 0.84 |
| Role Functioning/Emotional (RE) | 68.2 | 28.2 | 75 | 0 | 100 | 0.81 |
| Mental Health (MH) | 59.2 | 22 | 58 | 5 | 100 | 0.86 |
| Physical Component Summary (PCS) | 52.4 | 14.7 | 55.3 | 14.3 | 62.8 | 0.88 |
| Mental Component Summary (MCS) | 63.1 | 16.7 | 63.8 | 23.3 | 97.2 | 0.91 |
| Subscales | Physical Activity a (Low vs. Moderate/High) p Value |
|---|---|
| Physical Functioning (PF) | 0.03 |
| Role Functioning/Physical (RP) | 0.03 |
| Bodily Pain (BP) | 0.1 |
| General Health (GH) | 0.01 |
| Vitality (VT) | 0.02 |
| Social Functioning (SF) | 0.1 |
| Role Functioning/Emotional (RE) | 0.1 |
| Mental Health (MH) | 0.1 |
| Physical Component Summary (PCS) | 0.6 |
| Mental Component Summary (MCS) | 0.6 |
| Independent Variable | B Coefficient | 95% Confidence Interval of b | p Value | Collinearity Diagnostics | |
|---|---|---|---|---|---|
| Tolerance | VIF | ||||
| Mental Component Summary (MCS) as Dependent Variable R2 = 0.188 | |||||
| High school compared to primary school/illiterate | 13.9 | 5.6–22.2 | 0.001 | 0.88 | 1.13 |
| Secondary school compared to primary school/illiterate | 10.9 | 0.6–21.1 | 0.038 | 0.90 | 1.11 |
| Comorbidity | −3.6 | −6.4–−0.8 | 0.013 | 0.97 | 1.02 |
| Physical Functioning (PF)as Dependent Variable R2 = 0.238 | |||||
| High school compared to primary school/illiterate | 13.6 | 2.3–24.9 | 0.004 | 0.83 | 1.21 |
| Married | 11.9 | 2.1–21.8 | 0.019 | 0.97 | 1.03 |
| Comorbidity | −8.2 | −12.1–−4.3 | <0.001 | 0.88 | 1.14 |
| Role Functioning/Physical (RE)as Dependent Variable R2 = 0.30 | |||||
| Married | 10.6 | 1.8–19.4 | 0.018 | 0.94 | 1.06 |
| Comorbidity | −7.8 | −11.1–−4.6 | <0.001 | 0.97 | 1.03 |
| Hobby | 13.2 | 4.6–21.7 | 0.003 | 0.98 | 1.02 |
| Bodily Pain (BP)as Dependent Variable R2 = 0.17 | |||||
| Comorbidity | −5.5 | −8.9–−2.1 | 0.002 | 0.88 | 1.14 |
| General Health (GH)as Dependent Variable R2 = 0.243 | |||||
| High school compared to primary school/illiterate | 7.8 | 0.6–15.1 | 0.035 | 0.83 | 1.21 |
| Higher education compared to primary school/illiterate | 8.9 | 0.07–17.9 | 0.048 | 0.81 | 0.123 |
| Hobby | 1.4 | 5.1–17.6 | <0.001 | 0.88 | 1.14 |
| Comorbidity | −3.8 | −6.3–−1.3 | 0.003 | 0.87 | 1.14 |
| Number of children | 3.0 | 0.2–5.9 | 0.039 | 0.99 | 1.01 |
| Vitalityas Dependent Variable R2 = 0.20 | |||||
| Married | 8.2 | 1.5–15 | 0.017 | 0.95 | 1.05 |
| Comorbidity | −5.5 | −8.1–−3.1 | <0.001 | 0.97 | 1.02 |
| Social Functioning (SF)as Dependent Variable R2 = 0.19 | |||||
| Male | 9.9 | 0.4–19.4 | 0.041 | 0.89 | 1.11 |
| Participation in community programs | 13.9 | 5.1–22.6 | 0.002 | 0.99 | 1.01 |
| Comorbidity | −5.3 | −9.1–−2.4 | 0.001 | 0.96 | 1.04 |
| Role Functioning/Emotional (RE)as Dependent Variable R2 = 0.21 | |||||
| Married | 17.7 | 8.5–26.8 | <0.001 | 0.99 | 1.00 |
| Comorbidity | −7.2 | −10.7–−3.8 | <0.001 | 0.99 | 1.00 |
| Mental Health (MH)as Dependent Variable R2 = 0.146 | |||||
| Comorbidity | −4.1 | −7.1–−1.3 | 0.005 | 1.00 | 1.00 |
| Physical Activity as Dependent Variable R2 = 0.19 | |||
|---|---|---|---|
| Odds Ratio | 95% Confidence Interval | p Value | |
| Hobby | 3.5 | 1.1–11.1 | 0.03 |
| Comorbidities | 0.6 | 0.3–0.9 | 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Psarrou, A.; Adamakidou, T.; Apostolara, P.; Koreli, A.; Drakopoulou, M.; Plakas, S.; Mastrogiannis, D.; Mantoudi, A.; Parissopoulos, S.; Zartaloudi, A.; et al. Associations between Physical Activity and Health-Related Quality of Life among Community-Dwelling Older Adults: A Cross-Sectional Study in Urban Greece. Geriatrics 2023, 8, 61. https://doi.org/10.3390/geriatrics8030061
Psarrou A, Adamakidou T, Apostolara P, Koreli A, Drakopoulou M, Plakas S, Mastrogiannis D, Mantoudi A, Parissopoulos S, Zartaloudi A, et al. Associations between Physical Activity and Health-Related Quality of Life among Community-Dwelling Older Adults: A Cross-Sectional Study in Urban Greece. Geriatrics. 2023; 8(3):61. https://doi.org/10.3390/geriatrics8030061
Chicago/Turabian StylePsarrou, Anna, Theodoula Adamakidou, Paraskevi Apostolara, Alexandra Koreli, Marianna Drakopoulou, Sotirios Plakas, Dimos Mastrogiannis, Alexandra Mantoudi, Stelios Parissopoulos, Afroditi Zartaloudi, and et al. 2023. "Associations between Physical Activity and Health-Related Quality of Life among Community-Dwelling Older Adults: A Cross-Sectional Study in Urban Greece" Geriatrics 8, no. 3: 61. https://doi.org/10.3390/geriatrics8030061