

Colombian Stakeholder Perceptions and Recommendations Regarding Fall Detection Systems for Older Adults

Abstract
:1. Introduction
- User-activated or personal emergency response systems (PERS) are FDSs featuring an alert button which the user can activate manually. Upon activation, a text message is sent or an alert call is made to a specific caregiver, providing them with the user’s geopositioning [28].
- Automatic FDSs detect a fall without requiring activation by the user, while having the advantages of the previous system [28].
2. Methods
2.1. Setting and Participants
2.2. Participant Recruitment
2.3. Ethics Approval
2.4. Data Collection Procedure
2.5. Data Collection Instruments
2.5.1. Overview
2.5.2. Fall Characteristics
2.5.3. Wearable Fall Detection Technology
2.6. Data Analysis
3. Results
3.1. Samples and Sociodemographic Data
3.2. Findings
3.2.1. Overview
3.2.2. Findings for Fall Characteristics
Fall Frequency or Fear of Falling
Factors That Influence Falls, Such as Fall Type, Movements during a Fall, or Recovery Movements




ADLs, in Which Some Older Adults Need Help or Comfort, and Request Support from Their Caregivers or Family Members

Factors That Influence the Assessment of and Research into Falls
3.2.3. Monitoring Technology Findings
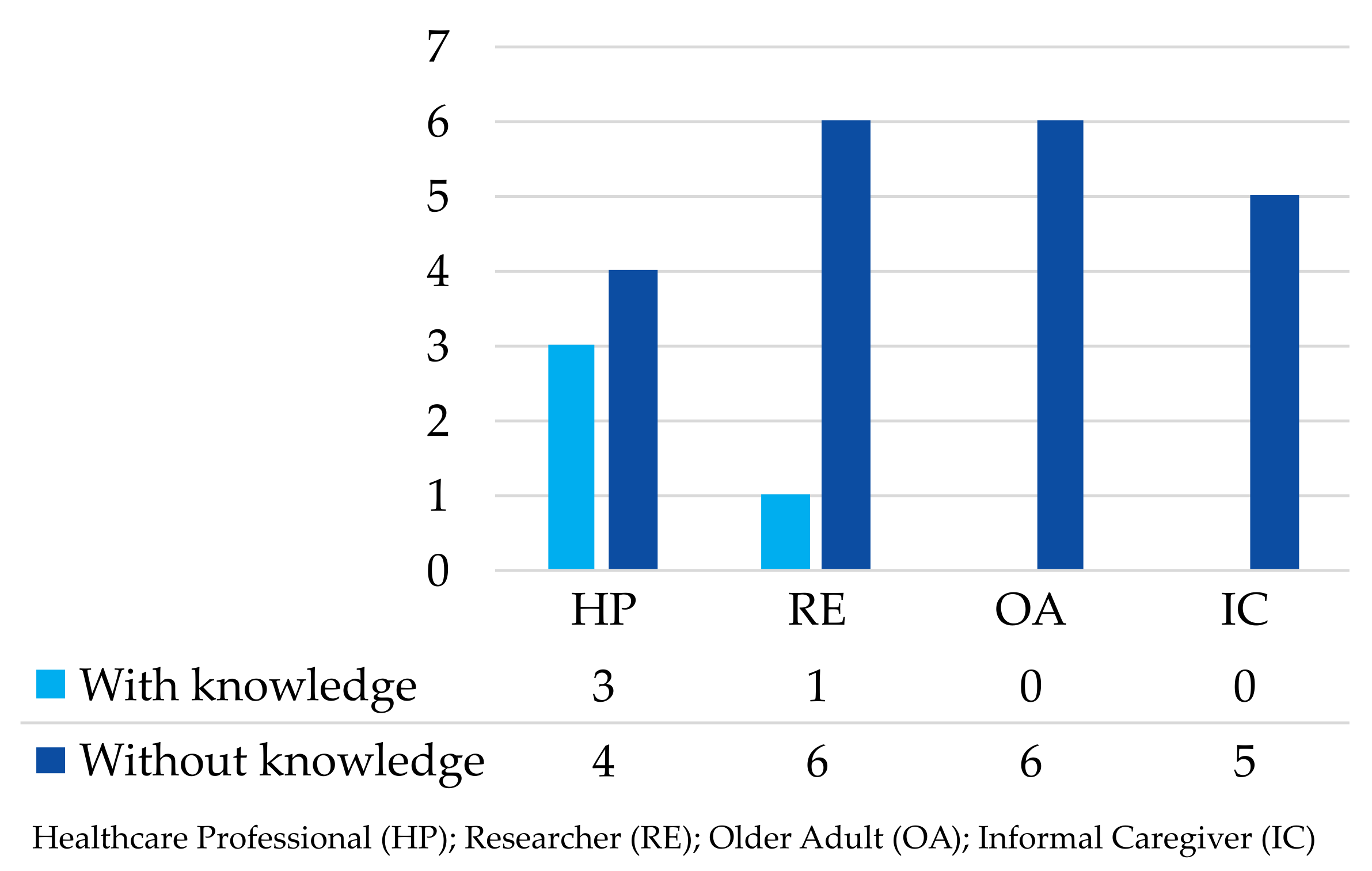
Knowledge of Fall Detection Systems

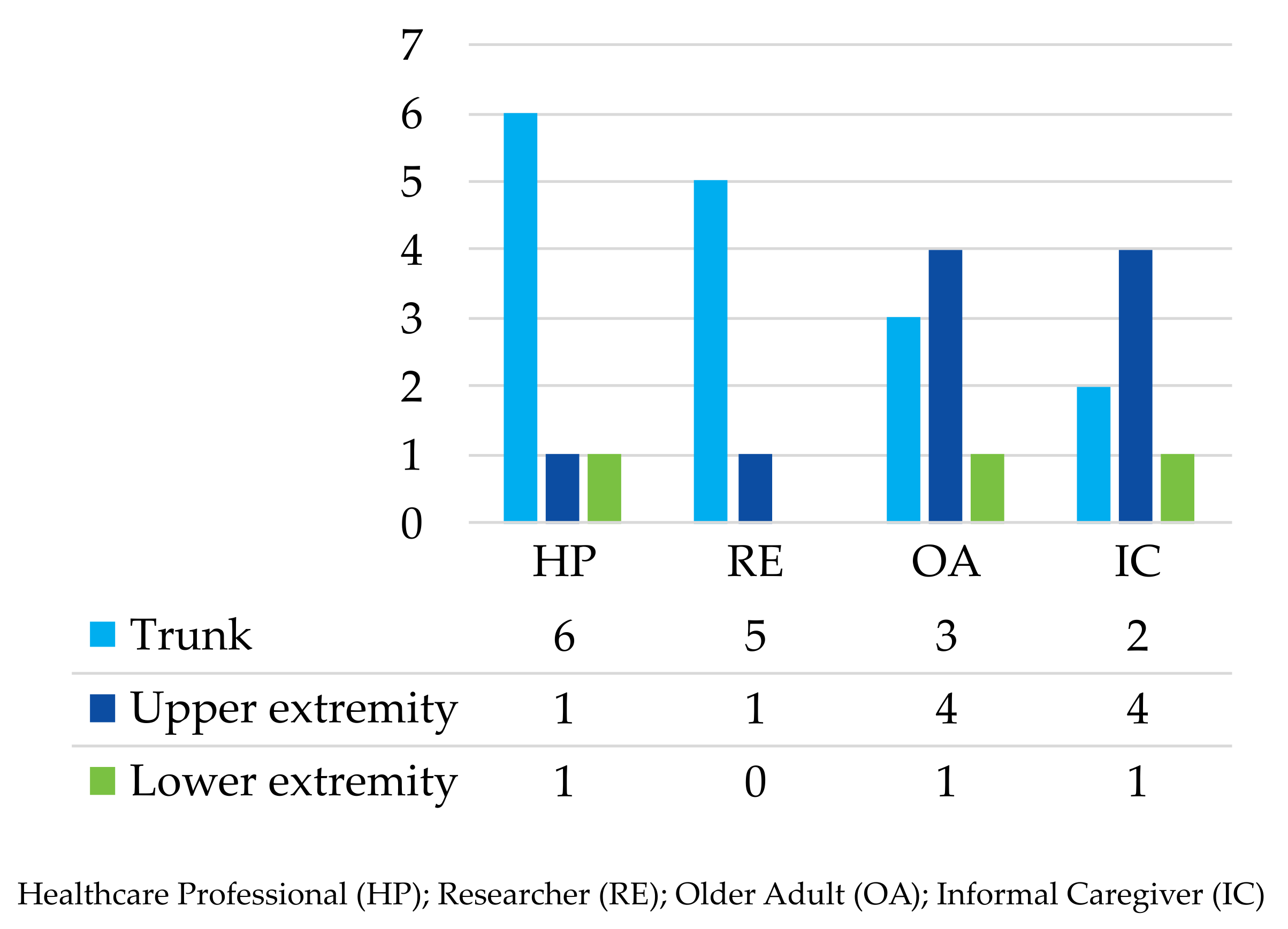
Elements That Respond to the Needs of Stakeholders







4. Discussion
4.1. Overview
4.2. Falls and the Fall Detector Importance
4.3. Existing and Approval of Fall Detectors
4.4. Stakeholder Fall Detector Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations, Department of Economic and Social Affairs. World Population Prospects 2022; United Nations, Department of Economic and Social Affairs: New York, NY, USA, 2022. [Google Scholar]
- United Nations, Department of Economic and Social Affairs. World Population Ageing 2019: Highlights (ST/ESA/SER.A/430); Technical Report; United Nations, Department of Economic and Social Affairs: New York, NY, USA, 2019. [Google Scholar]
- Chatterji, S.; Byles, J.; Cutler, D.; Seeman, T.; Verdes, E. Health, functioning, and disability in older adults–present status and future implications. Lancet 2015, 385, 563–575. [Google Scholar] [CrossRef] [PubMed]
- Observatorio Nacional de Envejecimiento y Vejez. Indicadores Demográficos (Indice de Envejecimiento, Tasa de Dependencia y Razón de Sexo); Ministerio de Salud y Protección Social, Colombia: Bogotá, Colombia, 2022. [Google Scholar]
- The World Bank. Life Expectancy at Birth, Total (Years)—Colombia; The World Bank: Washington, DC, USA, 2020. [Google Scholar]
- Departamento Administrativo Nacional de Estadística—DANE, Colombia. Adulto Mayor en Colombia—Características Generales; Technical Report; Departamento Administrativo Nacional de Estadística—DANE, Colombia: Bogotá, Colombia, 2020. [Google Scholar]
- Esteve, A.; Zueras, P. La estructura de los hogares de las personas mayores en América Latina y el Caribe. Rev. Panam. Salud Pública 2021, 45, e115. [Google Scholar] [CrossRef] [PubMed]
- Astorquiza Bustos, B.A.; Chingal, Ó.A. ¿Cómo están nuestros ancianos? Una exploración empírica de la calidad de vida del adulto mayor para el caso de Colombia. Rev. CEPAL 2019, 129, 139–161. [Google Scholar]
- Erkkola, R.U.; Vasankari, T.; Erkkola, R.A. Opinion paper: Exercise for healthy aging. Maturitas 2021, 144, 45–52. [Google Scholar] [CrossRef]
- Ferreira, G.R.O.N.; Chagas, T.D.N.D.C.E.; Gonçalves, L.H.T.; de Oliveira, M.D.F.V.; Botelho, E.P.; Polaro, S.H.I. Fall-Related Hospitalizations in Elderly People: Temporal Trend and Spatial Distribution in Brazil. Geriatrics 2023, 8, 30. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Falls; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization (WHO). Step Safely: Strategies for Preventing and Managing Falls across the Life-Course; World Health Organization (WHO): Geneva, Switzerland, 2021; pp. 1–194. [Google Scholar]
- Pan American Health Organization. Proportional Mortality in Older Adults and Leading Causes of Death 2019; Pan American Health Organization: Washington, DC, USA, 2019. [Google Scholar]
- Vesga Ferreira, J.C.; Contreras Higuera, M.F.; Vesga Barrera, J.A. Nuevos desafíos en el desarrollo de soluciones para e-health en Colombia, soportados en Internet de las Cosas (IoT). Rev. EIA 2021, 18, 1–19. [Google Scholar] [CrossRef]
- Muñoz García, Z.M. La Incorporación del Adulto Mayor en el Uso de las TICS y su Repercusión en las Tecnologías de Servicio de las Organizaciones; Specialisit; Universidad Militar Nueva Granada: Cajicá, Colombia, 2019. [Google Scholar]
- World Health Organization (WHO). Global Report on Assistive Technology; Technical Report; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Tanwar, R.; Nandal, N.; Zamani, M.; Manaf, A.A. Pathway of Trends and Technologies in Fall Detection: A Systematic Review. Healthcare 2022, 10, 172. [Google Scholar] [CrossRef]
- Bet, P.; Castro, P.C.; Ponti, M.A. Fall detection and fall risk assessment in older person using wearable sensors: A systematic review. Int. J. Med. Inform. 2019, 130, 103946. [Google Scholar] [CrossRef]
- Silva Fhon, J.R.; Partezani Rodrigues, R.A. Caída y factores demográficos y clínicos en adultos mayores: Estudio de seguimiento. Enfermería Glob. 2021, 20, 139–171. [Google Scholar] [CrossRef]
- Moreland, B.L.; Kakara, R.; Haddad, Y.K.; Shakya, I.; Bergen, G. A Descriptive Analysis of Location of Older Adult Falls That Resulted in Emergency Department Visits in the United States, 2015. Am. J. Lifestyle Med. 2021, 15, 590–597. [Google Scholar] [CrossRef]
- Mamdiwar, S.D.; R, A.; Shakruwala, Z.; Chadha, U.; Srinivasan, K.; Chang, C.Y. Recent Advances on IoT-Assisted Wearable Sensor Systems for Healthcare Monitoring. Biosensors 2021, 11, 372. [Google Scholar] [CrossRef] [PubMed]
- Camp, N.; Johnston, J.; Lewis, M.G.C.; Zecca, M.; Di Nuovo, A.; Hunter, K.; Magistro, D. Perceptions of In-home Monitoring Technology for Activities of Daily Living: Semistructured Interview Study With Community-Dwelling Older Adults. JMIR Aging 2022, 5, e33714. [Google Scholar] [CrossRef] [PubMed]
- Santoyo-Ramón, J.A.; Casilari-Pérez, E.; Cano-García, J.M. A study on the impact of the users’ characteristics on the performance of wearable fall detection systems. Sci. Rep. 2021, 11, 23011. [Google Scholar] [CrossRef] [PubMed]
- Talukder, M.S.; Sorwar, G.; Bao, Y.; Ahmed, J.U.; Palash, M.A.S. Predicting antecedents of wearable healthcare technology acceptance by elderly: A combined SEM-Neural Network approach. Technol. Forecast. Soc. Chang. 2020, 150, 119793. [Google Scholar] [CrossRef]
- Karar, M.E.; Shehata, H.I.; Reyad, O. A Survey of IoT-Based Fall Detection for Aiding Elderly Care: Sensors, Methods, Challenges and Future Trends. Appl. Sci. 2022, 12, 3276. [Google Scholar] [CrossRef]
- Xefteris, V.R.; Tsanousa, A.; Meditskos, G.; Vrochidis, S.; Kompatsiaris, I. Performance, Challenges, and Limitations in Multimodal Fall Detection Systems: A Review. IEEE Sens. J. 2021, 21, 18398–18409. [Google Scholar] [CrossRef]
- Ponce, H.; Martínez-Villaseñor, L.; Brieva, J.; Moya-Albor, E. Studies in Systems, Decision and Control. In Challenges and Trends in Multimodal Fall Detection for Healthcare, 1st ed.; Springer International Publishing: Cham, Switzerland, 2020; Volume 273, pp. 1–259. [Google Scholar] [CrossRef]
- Wang, L.; Peng, M.; Zhou, Q. Pre-Impact Fall Detection Based on Multi-Source CNN Ensemble. IEEE Sens. J. 2020, 20, 5442–5451. [Google Scholar] [CrossRef]
- Abdul Rahman, K.; Ahmad, S.A.; Che Soh, A.; Ashari, A.; Wada, C.; Gopalai, A.A. The Association of Falls with Instability: An Analysis of Perceptions and Expectations toward the Use of Fall Detection Devices Among Older Adults in Malaysia. Front. Public Health 2021, 9, 612538. [Google Scholar] [CrossRef]
- Moore, K.; O’Shea, E.; Kenny, L.; Barton, J.; Tedesco, S.; Sica, M.; Crowe, C.; Alamäki, A.; Condell, J.; Nordström, A.; et al. Older Adults’ Experiences with Using Wearable Devices: Qualitative Systematic Review and Meta-synthesis. JMIR MHealth UHealth 2021, 9, e23832. [Google Scholar] [CrossRef]
- Chaudhuri, S.; Kneale, L.; Le, T.; Phelan, E.; Rosenberg, D.; Thompson, H.; Demiris, G. Older Adults’ Perceptions of Fall Detection Devices. J. Appl. Gerontol. 2017, 36, 915–930. [Google Scholar] [CrossRef]
- Thilo, F.J.; Hahn, S.; Halfens, R.J.; Heckemann, B.; Schols, J.M. Facilitating the use of personal safety alerting device with older adults: The views, experiences and roles of relatives and health care professionals. Geriatr. Nurs. 2021, 42, 935–942. [Google Scholar] [CrossRef] [PubMed]
- Iancu, I.; Iancu, B. Designing mobile technology for elderly. A theoretical overview. Technol. Forecast. Soc. Chang. 2020, 155, 119977. [Google Scholar] [CrossRef]
- Thilo, F.J.S.; Hahn, S.; Halfens, R.J.G.; Schols, J.M.G.A. Usability of a wearable fall detection prototype from the perspective of older people—A real field testing approach. J. Clin. Nurs. 2019, 28, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Sidhu, K.; Jones, R.; Stevenson, F. Publishing qualitative research in medical journals. Br. J. Gen. Pract. 2017, 67, 229–230. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Medical Devices: Managing the Mismatch, an Outcome of the Priority Medical Devices Project; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Wiltshire, G.; Ronkainen, N. A realist approach to thematic analysis: Making sense of qualitative data through experiential, inferential and dispositional themes. J. Crit. Realism 2021, 20, 159–180. [Google Scholar] [CrossRef]
- Fadrique, L.X.; Rahman, D.; Vaillancourt, H.; Boissonneault, P.; Donovska, T.; Morita, P.P. Overview of Policies, Guidelines, and Standards for Active Assisted Living Data Exchange: Thematic Analysis. JMIR MHealth UHealth 2020, 8, e15923. [Google Scholar] [CrossRef]
- Suurmeijer, T.P.; Doeglas, D.M.; Moum, T.; Briançon, S.; Krol, B.; Sanderman, R.; Guillemin, F.; Bjelle, A.; van den Heuvel, W.J. The Groningen Activity Restriction Scale for measuring disability: Its utility in international comparisons. Am. J. Public Health 1994, 84, 1270–1273. [Google Scholar] [CrossRef]
- Capera-Peña, C.C.; Huertas-Prieto, T. Dispositivo IoT Detector de Caídas para las Personas de la Tercera Edad. Bachelor’s Thesis, Universidad Católica de Colombia, Bogotá, Colombia, 2021. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Section | Theme | Sub-Theme |
|---|---|---|
| Fall Characteristics | ADL | GARS |
| Assessment | Frequency | |
| Method | ||
| Rank | ||
| Fear | Injuries | |
| Form | Fall movements | |
| Recovery movements | ||
| Types | ||
| Quantity | ||
| Research | Area | |
| Time | ||
| Topic | ||
| Wearable Fall Detection Technology | Accessibility | Disadvantages |
| Affordability | Acceptance | |
| Advantages | ||
| Appropriateness | Additional suggestions | |
| Design | ||
| Disadvantages | ||
| Influencing factors | ||
| Availability | Existing knowledge | |
| Usability | Advantages | |
| Comfort | ||
| Influencing Factors | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Avella-Rodríguez, E.; Gómez, L.; Ramirez-Scarpetta, J.; Rosero, E. Colombian Stakeholder Perceptions and Recommendations Regarding Fall Detection Systems for Older Adults. Geriatrics 2023, 8, 51. https://doi.org/10.3390/geriatrics8030051
Avella-Rodríguez E, Gómez L, Ramirez-Scarpetta J, Rosero E. Colombian Stakeholder Perceptions and Recommendations Regarding Fall Detection Systems for Older Adults. Geriatrics. 2023; 8(3):51. https://doi.org/10.3390/geriatrics8030051
Chicago/Turabian StyleAvella-Rodríguez, Edna, Lessby Gómez, Jose Ramirez-Scarpetta, and Esteban Rosero. 2023. "Colombian Stakeholder Perceptions and Recommendations Regarding Fall Detection Systems for Older Adults" Geriatrics 8, no. 3: 51. https://doi.org/10.3390/geriatrics8030051