
Are Bubbles the Future of Dysphagia Rehabilitation: A Systematic Review Analysing Evidence on the Use of Carbonated Liquids in Dysphagia Rehabilitation

Abstract
:
1. Introduction
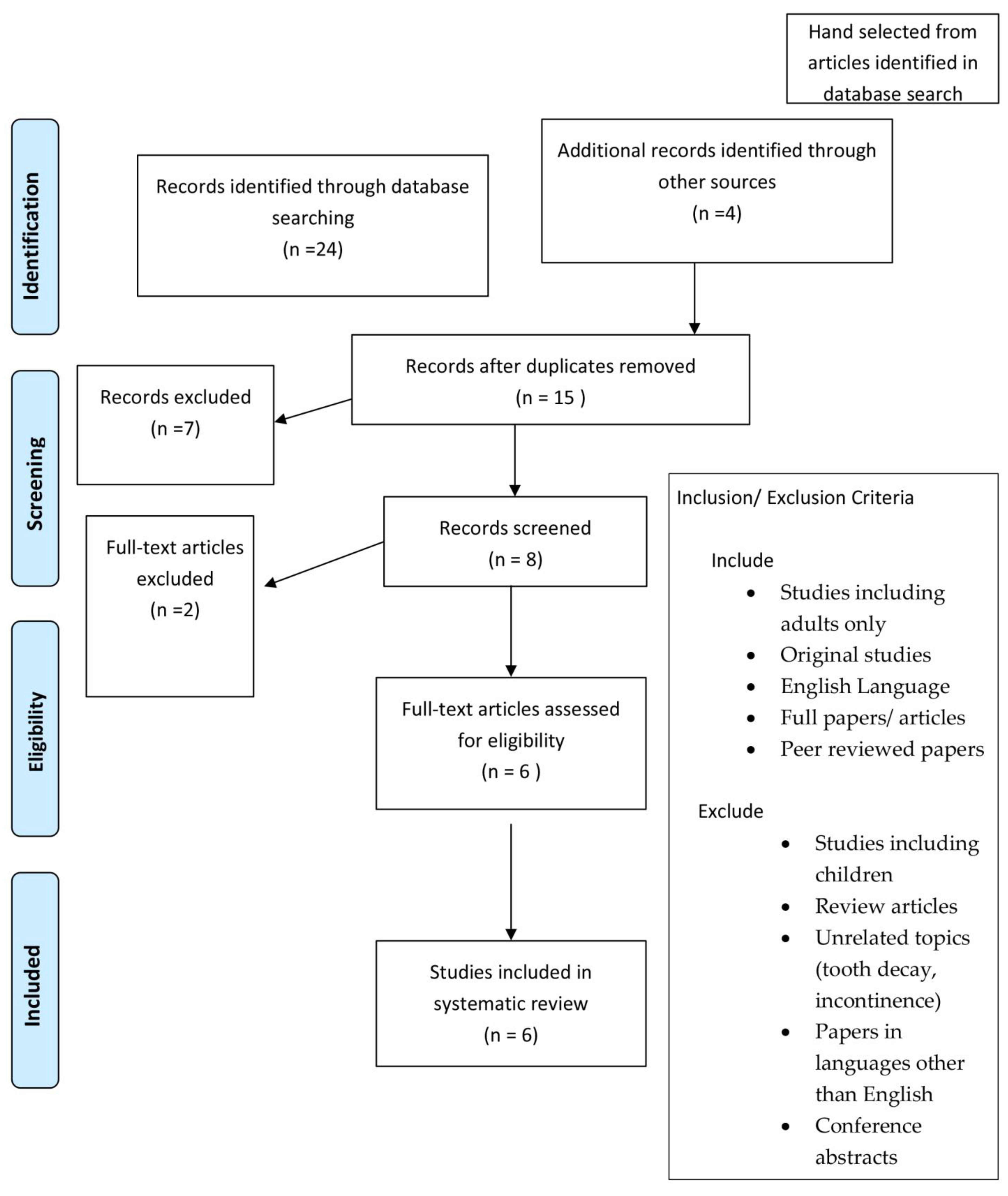
2. Materials and Methods
3. Results

{kind=link}
{kind=link}
| Author, Year | Title | Study Design | Participants | Method | Main Conclusions |
|---|---|---|---|---|---|
| Jennings et al., 1992 [14] | Swallowing problems after excision of tumors of the skull base: diagnosis and management in 12 patients. | Single centre retrospective observational study USA | N = 12 Post skull base surgery | Modified barium swallow (MBS), analysis via 2 authors. Several ½ teaspoons of different textures trialled. Use of swallowing manoeuvres | Overall 75% demonstrated evidence of aspiration. Vocal cord augmentation reduced aspiration. Carbonated beverage appeared beneficial to eliminate copious barium and secretions. No statistical breakdown of different liquids. |
| Bulow et al., 2003 [13] | Videoradiographic analysis of how carbonated thin liquids and thickened liquids affect the physiology of swallow in subjects with aspiration on thin liquids | Single centre prospective study Sweden | N = 40 36 were neurologically impaired and 4 were not. 19 had previously had a stroke | VFSS assessment of administration of 3 × 5 mL swallows of various textures with cued swallows | Significant reduction in penetration/aspiration and PTT with CTLs (p < 0.0001, p < 0.0001) compared to NCTL. Additionally, significantly reduced pharyngeal retention (p = 0.0013) with CTL compared to NCTL, and also compared to thickened liquids (p < 0.0001) |
| Sdarvou et al., 2012 [11] | Effects of carbonated liquids on oropharyngeal swallowing measures in people with neurogenic dysphagia | Single centre, Phase 1 study of treatment effect Greece | N = 17 18–80-year-olds with confirmed neurological disorder on CT/MRI, confirmed orophyngeal dysphagia with ability to tolerate VFSS and delayed pharyngeal response on NCTL seen on VFSS. Excluded peripheral nerve disorders. All participants had suffered stroke or traumatic brain injury | VFSS assessment of increasing quantities of NCTL then CTL (5-5-10-25 mL). Images analysed and subsequently 20% of studies re-analysed by two other raters to control interrater reliability. Participants rated palatability of CTL using the modified quartermaster hedonic scale. | CTL significantly decreased PEN/ASP scores of 5 and 10 mL swallows compared to NCTL (p = 0.028, p = 0.037), though not 25 mL swallows. CTL had no significant improvement in IPS, STD and PTT. CTL actually increased STD in 25 mL swallows. 58.8% participants liked or extremely liked CTL, 23.5% were not sure and 17.7% did not like CTL. |
| Larsson et al., 2017 [12] | Effects of carbonated liquid on swallowing dysfunction in dementia with Lewy bodies and Parkinson’s disease dementia | Single centre retrospective observational Sweden | N = 48 All participants had Lewy body dementia or Parkinson’s disease dementia and were referred from memory clinic for videofluoroscopy between 2006–2016 | Retrospective analysis of previous videofluoroscopy by two authors. Patients given 3–5 mL of various textured foods. Images assessed initially with descriptive analysis, then 25 patients included in quantitative analysis | Swallow improved in 87% individuals with carbonated liquid. Significantly reduced PTT with CTL compared to thick and thin liquids (p = 0.014 & p < 0.001) The severity of retention and depth of penetration was not significantly reduced with CTL. |
| Turkington et al., 2019 [15] | Impact of carbonation on neurogenic dysphagia and an exploration of the clinical predictors of a response to carbonation. | Single Centre Cohort study Australia | N = 29 Recruitment of individuals referred for VFSS with neurogenic dysphagia who could consent and had PAS score of ≥ 3 on VFSS. Varied diagnoses including stroke, progressive neurological disorders and brain injury | All participants underwent a clinical swallow examination, VFSS and genetic taste screening. With VFSS, participants prompted to take three discrete non-fixed volume sips on request, of non-carbonated liquid, then carbonated thin liquid. VFSS analysed using viduofluoroscopy dysphagia scale. VFSS interpretation by two assessors and if a disagreement then third assessor | Significant reduction (p = 0.01) in severity of PAS score with CTL vs. NCTL. Significant reduction in total VDS score with CTL but no reduction in PTT with CTL vs. NCTL Large variability in individual cases, some had worse PAS with CTL |
| Morishita et al., 2022 [10] | Effects of Carbonated Thickened Drinks on Pharyngeal Swallowing with a Flexible Endoscopic Evaluation of Swallowing in Older Patients with Oropharyngeal Dysphagia | Cross-sectional | N = 13 Adults who underwent FEES for diagnosis of dysphagia between 2021–2022 at Yokohama Izumidai Hospital.Mean age 79.6. Varied diagnoses, most common cause for dysphagia deconditioning | Patients took non-fixed volume swallows of cold (10°) CTL, NCTL, and CThL and uncarbonated thick liquids in a random order. 5 min intervals given between swallows. Swallows assessed using FEES. Secretion burden assessed using Murray secretion scale. Patient face scale was used to measure subjective difficultly in swallowing between liquids. | PAS lower with CThL than NCTL (p < 0.05). No significant difference in residue between liquids. No laryngeal penetration with CThL in comparison to NCTL in three patients. Subjectively swallow was reported to be easier with CThL than NCTL. Swallowing reflex initiation better with CThL compared to NCTL but no difference between CThL and thickened liquids Small sample size, varied aetiology of dysphagia |
4. Discussion
5. Future Work
- (1)
- Co-production with patient groups.
- (2)
- A minimum data set so that study results can be brought together to provide a larger data set.
- (3)
- Multicentre studies (single blind studies, cohort randomisation).
- (4)
- Short-, medium- and long-term outcomes (survival, dependency).
- (5)
- Simple, patient reported outcome measure, including secretion management, food intake (volume/consistency), nutritional assessments, hydration and quality of life assessment.
- (6)
- Carer stress.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Correction Statement
Abbreviations
| CTL | carbonated thin liquid |
| CThL | carbonated thickened liquids |
| inc | including |
| NCTL | non-carbonated thin liquids |
| PTT | pharyngeal transit time |
| PENASP/PAS | penetration/aspiration scale |
| IPS | initiation of the pharyngeal swallow |
| STD | stage transition duration |
| VDS | dysphagia scale |
References
- Greener, M. Dysphagia. Gastroenterol. GM J. 2009, 458, 1–7. Available online: https://www.gmjournal.co.uk/media/21598/aug2009p458.pdf (accessed on 21 July 2019).
- Adkins, C.; Takakura, W.; Spiegel, B.; Lu, M.; Vera-Llonch, M.; Williams, J.; Almario, C. Prevalence and Characteristics of Dysphagia Based on a Population-Based Survey. Clin. Gastroenterol. Hepatol. 2020, 18, 1970–1979. [Google Scholar] [CrossRef] [PubMed]
- Doo-Young, K.; Hyo-Sik, P.; Si-Woon, P.; Jae-Hyung, K. The impact of dysphagia on quality of life in stroke patients. Medicine 2020, 21, 21795. [Google Scholar]
- Kronenberger, M.B.; Meyers, A.D. Dysphagia following head and neck cancer surgery. Dysphagia. Fall 1994, 9, 236–244. [Google Scholar] [CrossRef]
- Porto de Toledo, I.; Pantoja, L.L.Q.; Luchesi, K.F.; Assad, D.X.; De Luca Canto, G.; Guerra, E.N.S. Deglutition disorders as a consequence of head and neck cancer therapies: A systematic review and meta-analysis. Support Care Cancer 2019, 27, 3681–3700. [Google Scholar] [CrossRef]
- Logemann, J.A. Pre swallow sensory input: Its potential importance to dysphagic patients and normal individuals. Dysphagia 1996, 11, 9–10. [Google Scholar] [CrossRef]
- Turkington, L.G.; Farrell, A.M.; Ward, E.C. Carbonation as a sensory enhancement strategy: A narrative synthesis of existing evidence. Disabil. Rehabil. 2017, 39, 1958–1967. [Google Scholar] [CrossRef] [PubMed]
- Carstens, E.; Carstens, M.; Dessirier, J.M.; O’Mahony, M.; Simons, C.; Sudo, S. It hurts so good: Oral irritation by spices and carbonated drinks and the underlying neural mechanisms. Food Qual. Prefer. 2002, 13, 431–443. [Google Scholar] [CrossRef]
- PRISMA. Transparent Reporting of Systematic Reviews and Meta-Analysis. Available online: http://www.prisma-statement.org/PRISMAStatement/ (accessed on 14 July 2019).
- Morishita, M.; Okubo, M.; Sekine, T. Effects of carbonated thickened drinks on pharyngeal swallowing with a flexible endoscopic evaluation of swallowing in older patients with oro-pharyngeal dysphagia. Healthcare 2022, 10, 1769. [Google Scholar] [CrossRef] [PubMed]
- Sdvarou, K.; Walshe, M.; Dagdilelis, L. Effects of Carbonated Liquids on Oropharyngeal Swallowing Measures in People with Neurogenic Dysphagia. Dysphagia 2012, 27, 240–250. [Google Scholar]
- Larsson, V.; Torisson, G.; Bülow, M.; Londos, E. Effects of carbonated liquid on swallowing dysfunction in dementia with Lewy bodies and Parkinson’s disease dementia. Clin. Interv. Ageing 2017, 12, 1215–1222. [Google Scholar] [CrossRef] [PubMed]
- Bulow, M. Videoradiographic Analysis of How Carbonated Thin Liquids and Thickened Liquids Affect the Physiology of Swallowing in Subjects with Aspiration on Thin Liquids. Acta Radiol. 2003, 44, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Jennings, S. Swallowing Problems after Excision of Tumors of the Skull Base: Diagnosis and Management in 12 Patients. Dysphagia 1992, 7, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Turkington, L.; Ward, E.C.; Farrell, A.; Porter, L.; Wall, L.R. Impact of carbonation on neurogenic dysphagia and an exploration of the clinical predictors of a response to carbonation. Int. J. Lang Commun. Disord. 2019, 54, 499–513. [Google Scholar] [CrossRef] [PubMed]
- Smithard, D.G. Dysphagia: A Geriatric Giant. Med. Clin. Rev. 2016, 2, 5. [Google Scholar] [CrossRef]
- Nagano, A.; Maeda, K.; Shimizu, A.; Murotani, K.; Mori, N. Effects of carbonation on swallowing: Systematic review and meta-analysis. Laryngosocpe 2022, 132, 1924–1933. [Google Scholar] [CrossRef] [PubMed]
- Barry, E.; Regan, J. An examination into the effect of genetic taste status and intensity of carbonation on swallowing and palatability in healthy young adults. Int. J. Lang Commun. Disord. 2021, 56, 812–825. [Google Scholar] [CrossRef] [PubMed]
- Wierenga, M.R.; Crawford, C.R.; Running, C.A. Older US adults like sweetened colas, but not other chemesthetic beverages. J. Texture Stud. 2020, 51, 722–732. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Price, K.; Isbister, G.; Long, S.; Mirams, J.; Smithard, D. Are Bubbles the Future of Dysphagia Rehabilitation: A Systematic Review Analysing Evidence on the Use of Carbonated Liquids in Dysphagia Rehabilitation. Geriatrics 2023, 8, 6. https://doi.org/10.3390/geriatrics8010006
Price K, Isbister G, Long S, Mirams J, Smithard D. Are Bubbles the Future of Dysphagia Rehabilitation: A Systematic Review Analysing Evidence on the Use of Carbonated Liquids in Dysphagia Rehabilitation. Geriatrics. 2023; 8(1):6. https://doi.org/10.3390/geriatrics8010006
Chicago/Turabian StylePrice, Kathryn, Grace Isbister, Susannah Long, John Mirams, and David Smithard. 2023. "Are Bubbles the Future of Dysphagia Rehabilitation: A Systematic Review Analysing Evidence on the Use of Carbonated Liquids in Dysphagia Rehabilitation" Geriatrics 8, no. 1: 6. https://doi.org/10.3390/geriatrics8010006