
Determinants of 1-Year Adverse Event Requiring Re-Hospitalization in COVID-19 Oldest Old Survivors

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
4.1. Prevalence and Causes of 12-Month Adverse Events Requiring Rehospitalization
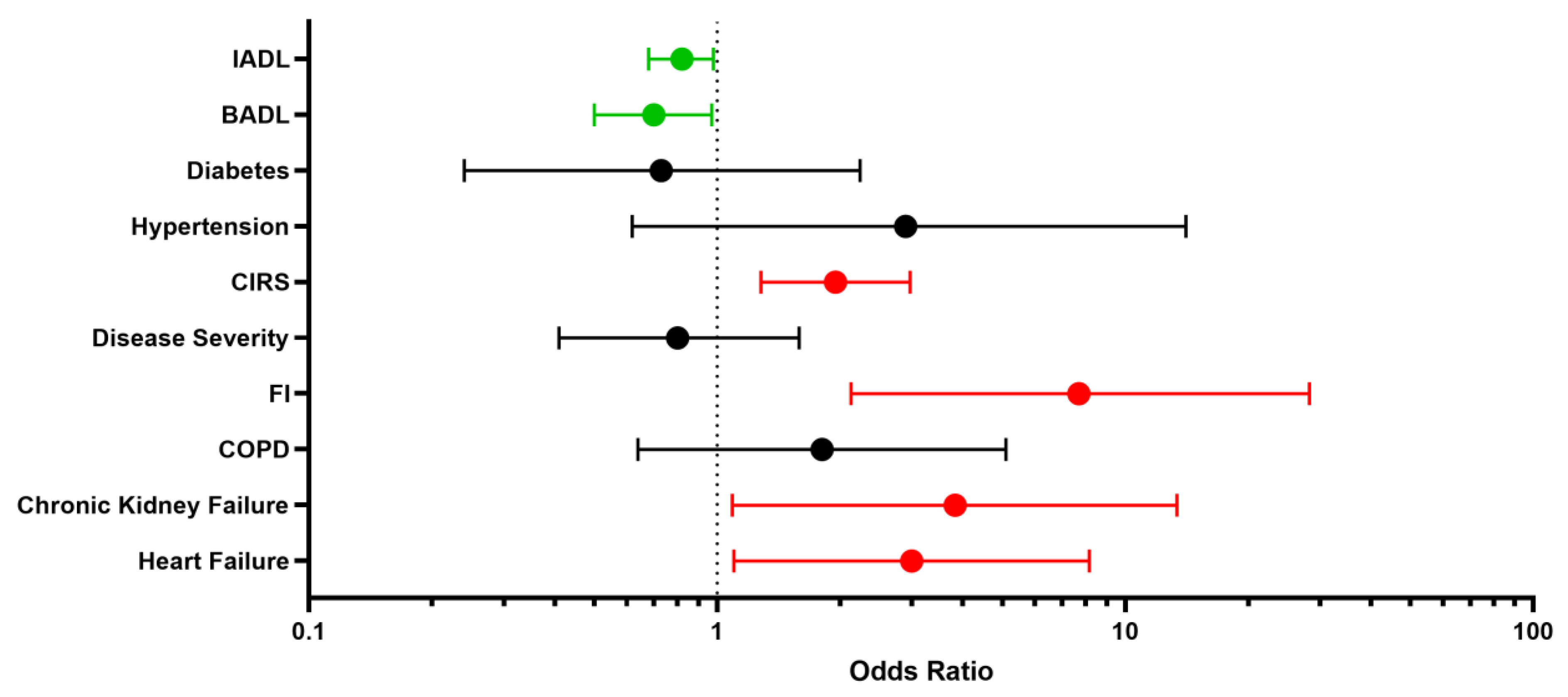
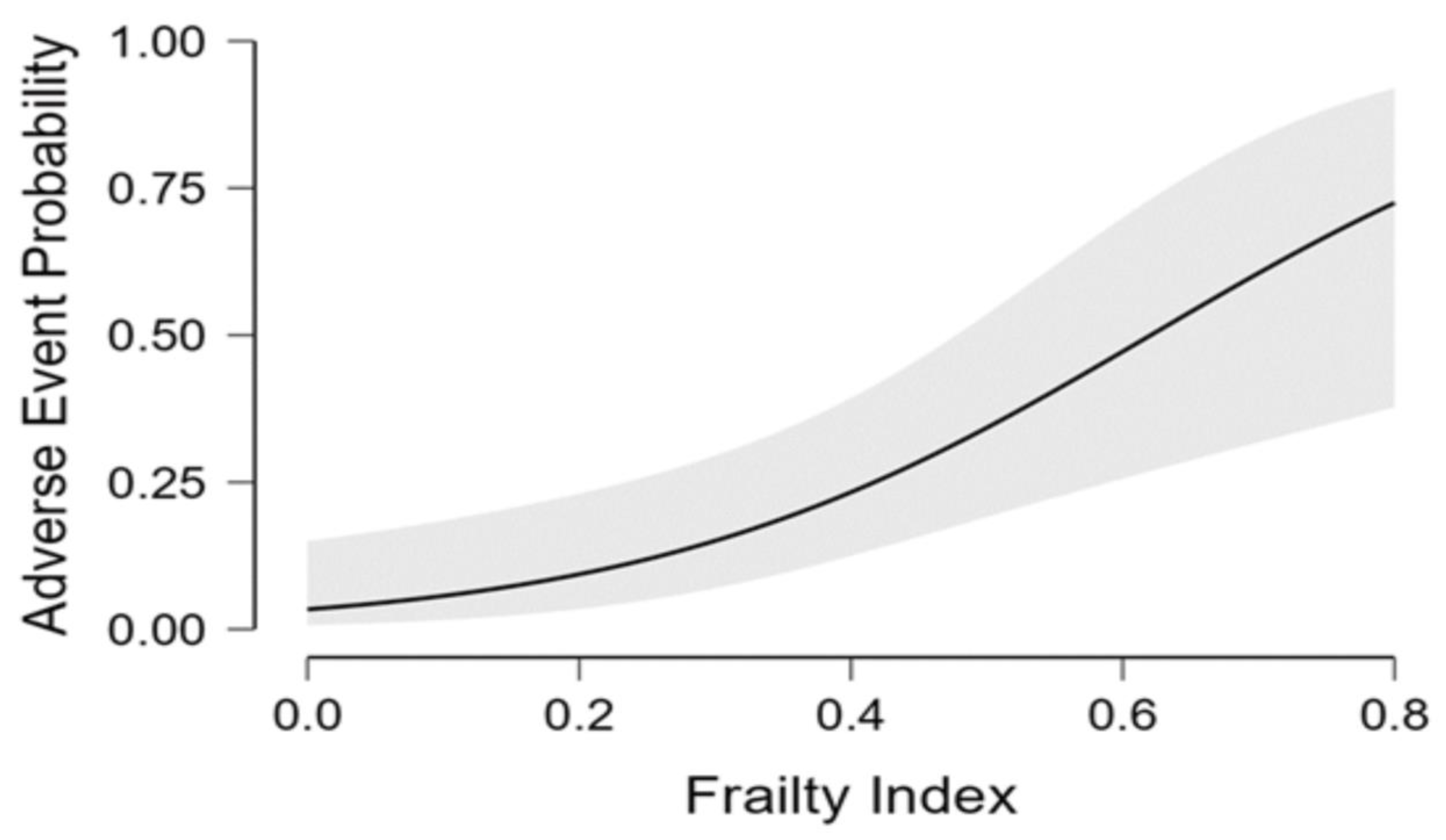
4.2. Risk Factors of Adverse Events Requiring Re-Hospitalization
4.3. Impact on Functional Performance
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Xiong, Q.; Xu, M.; Li, J.; Liu, Y.; Zhang, J.; Xu, Y.; Dong, W. Clinical sequelae of COVID-19 survivors in Wuhan, China: A single-centre longitudinal study. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2021, 27, 89–95. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F. Persistent Symptoms in Patients after Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Mandal, S.; Barnett, J.; Brill, S.E.; Brown, J.S.; Denneny, E.K.; Hare, S.S.; Heightman, M.; Hillman, E.T.; Jacob, J.; Jarvis, H.C.; et al. “Long-COVID”: A cross-sectional study of persisting symptoms, biomarker and imaging abnormalities following hospitalisation for COVID-19. Thorax 2021, 76, 396–398. [Google Scholar] [CrossRef]
- Wang, F.; Kream, R.M.; Stefano, G.B. Long-Term Respiratory and Neurological Sequelae of COVID-19. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e928996. [Google Scholar] [CrossRef]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 Long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef]
- Liu, Y.H.; Wang, Y.R.; Wang, Q.H.; Chen, Y.; Chen, X.; Li, Y.; Cen, Y.; Xu, C.; Hu, T.; Liu, X.-D.; et al. Post-infection cognitive impairments in a cohort of elderly patients with COVID-19. Mol. Neurodegener. 2021, 16, 48. [Google Scholar] [CrossRef]
- Bowles, K.H.; McDonald, M.; Barrón, Y.; Kennedy, E.; O’Connor, M.; Mikkelsen, M. Surviving COVID-19 After Hospital Discharge: Symptom, Functional, and Adverse Outcomes of Home Health Recipients. Ann. Intern. Med. 2021, 174, 316–325. [Google Scholar] [CrossRef] [PubMed]
- Ramzi, Z.S. Hospital readmissions and post-discharge all-cause mortality in COVID-19 recovered patients; A systematic review and meta-analysis. Am. J. Emerg. Med. 2022, 51, 267–279. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Wang, X.Q.; Iwashyna, T.J.; Prescott, H.C. Readmission and Death After Initial Hospital Discharge Among Patients With COVID-19 in a Large Multihospital System. JAMA 2021, 325, 304–306. [Google Scholar] [CrossRef] [PubMed]
- Stuck, A.E.; Siu, A.L.; Wieland, G.D.; Adams, J.; Rubenstein, L.Z. Comprehensive geriatric assessment: A meta-analysis of controlled trials. Lancet 1993, 342, 1032–1036. [Google Scholar] [CrossRef]
- Pfeiffer, E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J. Am. Geriatr. Soc. 1975, 23, 433–441. [Google Scholar] [CrossRef]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of ilness in the aged. The index of ADL: A standardized measure of biological and psycological function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Guigoz, Y.; Lauque, S.; Vellas, B.J. Identifying the elderly at risk for malnutrition. The Mini Nutritional Assessment. Clin. Geriatr. Med. 2002, 18, 737–757. [Google Scholar] [CrossRef]
- Parmelee, P.A.; Thuras, P.D.; Katz, I.R.; Lawton, M.P. Validation of the Cumulative Illness Rating Scale in a geriatric residential population. J. Am. Geriatr. Soc. 1995, 43, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Treacy, D.; Hassett, L. The Short Physical Performance Battery. J. Physiother. 2018, 64, 61. [Google Scholar] [CrossRef]
- Prem, K.; Liu, Y.; Russell, T.W.; Kucharski, A.J.; Eggo, R.M.; Davies, N.; Jit, M.; Klepac, P.; Flasche, S.; Clifford, S.; et al. The effect of control strategies to reduce social mixing on outcomes of the COVID-19 epidemic in Wuhan, China: A modelling study. Lancet Public Health 2020, 5, e261–e270. [Google Scholar] [CrossRef] [Green Version]
- Tosato, M.; Carfì, A.; Martis, I.; Pais, C.; Ciciarello, F.; Rota, E.; Tritto, M.; Salerno, A.; Zazzara, M.B.; Martone, A.M.; et al. Prevalence and Predictors of Persistence of COVID-19 Symptoms in Older Adults: A Single-Center Study. J. Am. Med. Dir. Assoc. 2021, 22, 1840–1844. [Google Scholar] [CrossRef]
- Hewitt, J.; Carter, B.; Vilches-Moraga, A.; Quinn, T.J.; Braude, P.; Verduri, A.; Pearce, L.; Stechman, M.; Short, R.; Price, A.; et al. The effect of frailty on survival in patients with COVID-19 (COPE): A multicentre, European, observational cohort study. Lancet Public Health 2020, 5, e444–e451. [Google Scholar] [CrossRef]
- Carrillo-Garcia, P.; Garmendia-Prieto, B.; Cristofori, G.; Montoya, I.L.; Hidalgo, J.J.; Feijoo, M.Q.; Cortés, J.J.B.; Gómez-Pavón, J. Health status in survivors older than 70 years after hospitalization with COVID-19: Observational follow-up study at 3 months. Eur. Geriatr. Med. 2021, 12, 1091–1094. [Google Scholar] [CrossRef] [PubMed]
- Welch, C. Age and frailty are independently associated with increased COVID-19 mortality and increased care needs in survivors: Results of an international multi-centre study. Age Ageing 2021, 50, 617–630. [Google Scholar] [CrossRef]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA 2020, 323, 1775–1776. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; He, W.; Yu, X.; Hu, D.; Bao, M.; Liu, H.; Zhou, J.; Jiang, H. Coronavirus disease 2019 in elderly patients: Characteristics and prognostic factors based on 4-week follow-up. J. Infect. 2020, 80, 639–645. [Google Scholar] [CrossRef]
- Rey, J.R.; Caro-Codón, J.; Rosillo, S.O.; Iniesta, M. Heart failure in COVID-19 patients: Prevalence, incidence and prognostic implications. Eur. J. Heart Fail 2020, 22, 2205–2215. [Google Scholar] [CrossRef]
- Yamamoto, K.; Takeshita, H.; Rakugi, H. ACE2, angiotensin 1-7 and skeletal muscle: Review in the era of COVID-19. Clin. Sci. 2020, 134, 3047–3062. [Google Scholar] [CrossRef] [PubMed]
- Braun, F.; Lütgehetmann, M.; Pfefferle, S.; Wong, M.N.; Carsten, A.; Lindenmeyer, M.T.; Nörz, D.; Heinrich, F.; Meißner, K.; Wichmann, D.; et al. SARS-CoV-2 renal tropism associates with acute kidney injury. Lancet 2020, 396, 597–598. [Google Scholar] [CrossRef]
- Perico, L.; Benigni, A.; Casiraghi, F.; Ng, L.F.P.; Renia, L.; Remuzzi, G. Immunity, endothelial injury and complement-induced coagulopathy in COVID-19. Nat. Rev. Nephrol. 2021, 17, 46–64. [Google Scholar] [CrossRef]
- Touyz, R.M.; Boyd, M.O.E.; Guzik, T.; Padmanabhan, S.; McCallum, L.; Delles, C.; Mark, P.B.; Petrie, J.R.; Rios, F.; Montezano, A.C.; et al. Cardiovascular and Renal Risk Factors and Complications Associated with COVID-19. CJC Open 2021, 3, 1257–1272. [Google Scholar] [CrossRef]
- Chan, L.; Chaudhary, K.; Saha, A.; Chauhan, K.; Vaid, A.; Zhao, S.; Paranjpe, I.; Somani, S.; Richter, F.; Miotto, R.; et al. AKI in Hospitalized Patients with COVID-19. J. Am. Soc. Nephrol. 2021, 32, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Ganz, D.A.; Latham, N.K. Prevention of Falls in Community-Dwelling Older Adults. N. Engl. J. Med. 2020, 382, 734–743. [Google Scholar] [CrossRef] [PubMed]
- Rossi, R.; Socci, V.; Talevi, D.; Mensi, S.; Niolu, C.; Pacitti, F.; Di Marco, A.; Rossi, A.; Siracusano, A.; Di Lorenzo, G. COVID-19 Pandemic and Lockdown Measures Impact on Mental Health Among the General Population in Italy. Front. Psychiatry 2020, 11, 790. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.L.; Steinman, L.E.; Casey, E.A. Combatting Social Isolation Among Older Adults in a Time of Physical Distancing: The COVID-19 Social Connectivity Paradox. Front. Public Health 2020, 8, 403. [Google Scholar] [CrossRef] [PubMed]
- Wostyn, P. COVID-19 and chronic fatigue syndrome: Is the worst yet to come? Med. Hypotheses 2021, 146, 110469. [Google Scholar] [CrossRef] [PubMed]
- Proal, A.; Marshall, T. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome in the Era of the Human Microbiome: Persistent Pathogens Drive Chronic Symptoms by Interfering with Host Metabolism, Gene Expression, and Immunity. Front. Pediatr. 2018, 6, 373. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Comprehensive Geriatric Assessment (CGA) | Whole Cohort (n = 100) | Patients with Adverse Events (n = 24) | Controls (n = 76) | p |
|---|---|---|---|---|
| Gender F (%) | 42 (42) | 10 (41.7) | 32 (42.1) | 0.97 |
| Age [mean years (SD)] | 85 (4) | 85.6 (4.1) | 84.8 (4) | 0.40 |
| BMI [mean (SD)] | 25.8 (3.9) | 25.8 (4.5) | 26.2 (3.8) | 0.67 |
| BADL [median (IQR)] | 5 (1) | 5 (3.25) | 6 (1) | 0.02 |
| IADL [median (IQR)] | 6.5 (5) | 4.5 (6) | 7 (4) | 0.03 |
| CIRS [median (IQR)] | 3 (2) | 4 (1.25) | 2 (2) | 0.002 |
| Frailty index [mean (SD)] | 0.32 (0.16) | 0.41 (0.14) | 0.29 (0.15) | 0.001 |
| Not frail (%) Frail (%) | 44 (44) 56 (56) | 3 (12.5) 21 (87.5) | 41 (54) 35 (46) | 0.001 |
| Hypertension (%) | 81 (81) | 22 (91.7) | 59 (77.6) | 0.12 |
| Heart failure (%) | 27 (27) | 11 (45.8) | 16 (21.1) | 0.01 |
| Ischemic heart disease (%) | 21 (21) | 6 (25) | 15 (19.7) | 0.58 |
| Diabetes (%) | 25 (25) | 5 (20.8) | 20 (26.3) | 0.58 |
| COPD (%) | 25 (25) | 8 (33) | 17 (22.3) | 0.28 |
| Stroke (%) | 12 (12) | 3 (12.5) | 9 (11.8) | 0.93 |
| Chronic renal failure (%) | 12 (12) | 6 (25) | 6 (7.9) | 0.02 |
| Previous cancer (%) | 30 (30) | 8 (33.3) | 22 (28.9) | 0.68 |
| COVID-19 severity No supplemental oxygen (%) Low flow oxygen (%) High flow oxygen (%) | 12 (12) 21 (21) 67 (67) | 4 (17.4) 4 (17.4) 16 (65.2) | 8 (9.4) 17 (22.3) 51 (67) | 0.56 |
| Total Adverse Events | 26 |
|---|---|
| Heart failure (%) | 4 (15.3) |
| Pneumonia (%) | 4 (15.3) |
| Bone fracture (%) | 4 (15.3) |
| Acute kidney failure (%) | 3 (11.5) |
| Neurological (%) | 3 (11.5) |
| Sepsis (%) | 2 (7.6) |
| Syncope (%) | 1 (3.8) |
| Hematuria (%) | 1 (3.8) |
| Pulmonary embolism (%) | 1 (3.8) |
| Subdural hematoma (%) | 1 (3.8) |
| Atrial Fibrillation (%) | 1 (3.8) |
| Pericarditis (%) | 1 (3.8) |
| Whole Cohort (n = 100) | Patients with Adverse Events (n = 24) | Controls (n = 76) | p | |
|---|---|---|---|---|
| Hand Grip Strength [mean Kg (SD)] | 20.7 (7.5) | 20 (6.9) | 21 (7.8) | 0.59 |
| MNA [mean (SD)] | 12.4 (1.7) | 11.79 (2.02) | 12.59 (1.5) | 0.04 |
| N° of drugs [median (IQR)] | 6 (4) | 8 (5) | 5 (4) | <0.001 |
| SPPB [median (IQR)] | 6 (8) | 5 (6) | 6.5 (8.25) | 0.04 |
| SPSMQ [median (IQR)] | 2 (3) | 2 (3.25) | 1.5 (2) | 0.15 |
| Loss of BADL (%) | 7 (7) | 3 (12.5) | 4 (5.2) | 0.23 |
| Dyspnea (%) | 37 (37) | 11 (45.8) | 26 (34.2) | 0.18 |
| Cough (%) | 9 (9) | 3 (12.5) | 6 (7.9) | 0.78 |
| Pharyngodynia (%) | 3 (3) | 2 (8.3) | 1 (1.3) | 0.21 |
| Muscle pain (%) | 6 (6) | 3 (12.5) | 3 (3.9) | 0.12 |
| Arthralgia (%) | 6 (6) | 2 (8.3) | 4 (5.2) | 0.85 |
| Fatigue (%) | 27 (27) | 9 (37.5) | 18 (23.8) | 0.35 |
| Heartburn (%) | 4 (4) | 1 (4.1) | 3 (3.9) | 0.96 |
| Loss of taste (%) | 9 (9) | 1 (4.1) | 8 (10.5) | 0.61 |
| Loss of smell (%) | 9 (9) | 2 (8.3) | 7 (9.2) | 0.91 |
| Deambulation impairment (%) | 15 (15) | 8 (33.3) | 7 (9.2) | 0.01 |
| Concentration impairment (%) | 9 (9) | 1 (4.1) | 8 (10.5) | 0.56 |
| Memory impairment (%) | 11 (11) | 3 (12.5) | 8 (10.5) | 0.91 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okoye, C.; Franchi, R.; Calabrese, A.M.; Morelli, V.; Peta, U.; Mazzarone, T.; Pompilii, I.M.; Coppini, G.; Rogani, S.; Calsolaro, V.; et al. Determinants of 1-Year Adverse Event Requiring Re-Hospitalization in COVID-19 Oldest Old Survivors. Geriatrics 2023, 8, 10. https://doi.org/10.3390/geriatrics8010010
Okoye C, Franchi R, Calabrese AM, Morelli V, Peta U, Mazzarone T, Pompilii IM, Coppini G, Rogani S, Calsolaro V, et al. Determinants of 1-Year Adverse Event Requiring Re-Hospitalization in COVID-19 Oldest Old Survivors. Geriatrics. 2023; 8(1):10. https://doi.org/10.3390/geriatrics8010010
Chicago/Turabian StyleOkoye, Chukwuma, Riccardo Franchi, Alessia Maria Calabrese, Virginia Morelli, Umberto Peta, Tessa Mazzarone, Igino Maria Pompilii, Giulia Coppini, Sara Rogani, Valeria Calsolaro, and et al. 2023. "Determinants of 1-Year Adverse Event Requiring Re-Hospitalization in COVID-19 Oldest Old Survivors" Geriatrics 8, no. 1: 10. https://doi.org/10.3390/geriatrics8010010