
Development of a Nomogram to Predict the Outcome for Patients with Soft Tissue Sarcoma

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Data
2.2. Patient Demographics and Risk Analysis of Individual Variables
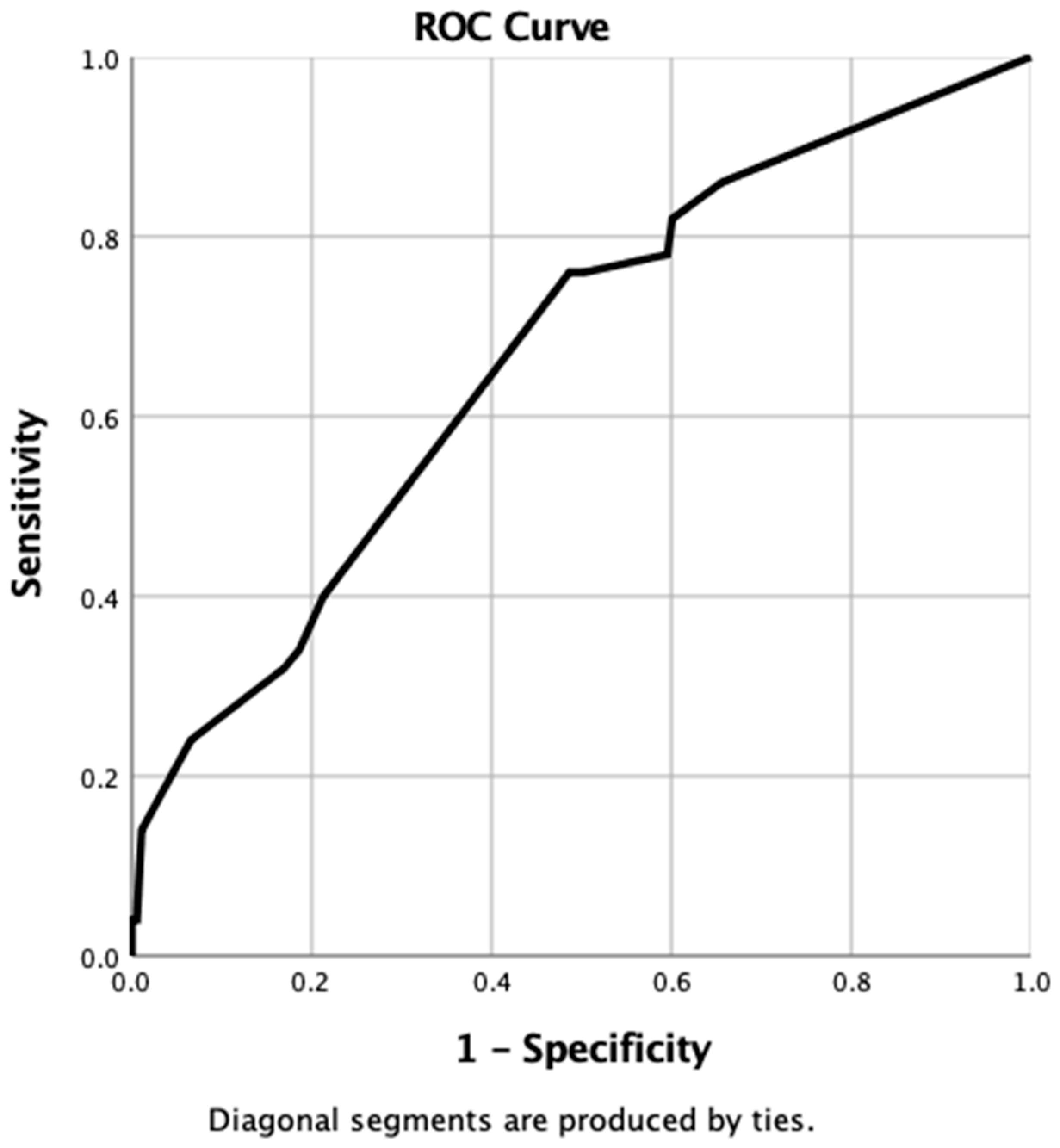
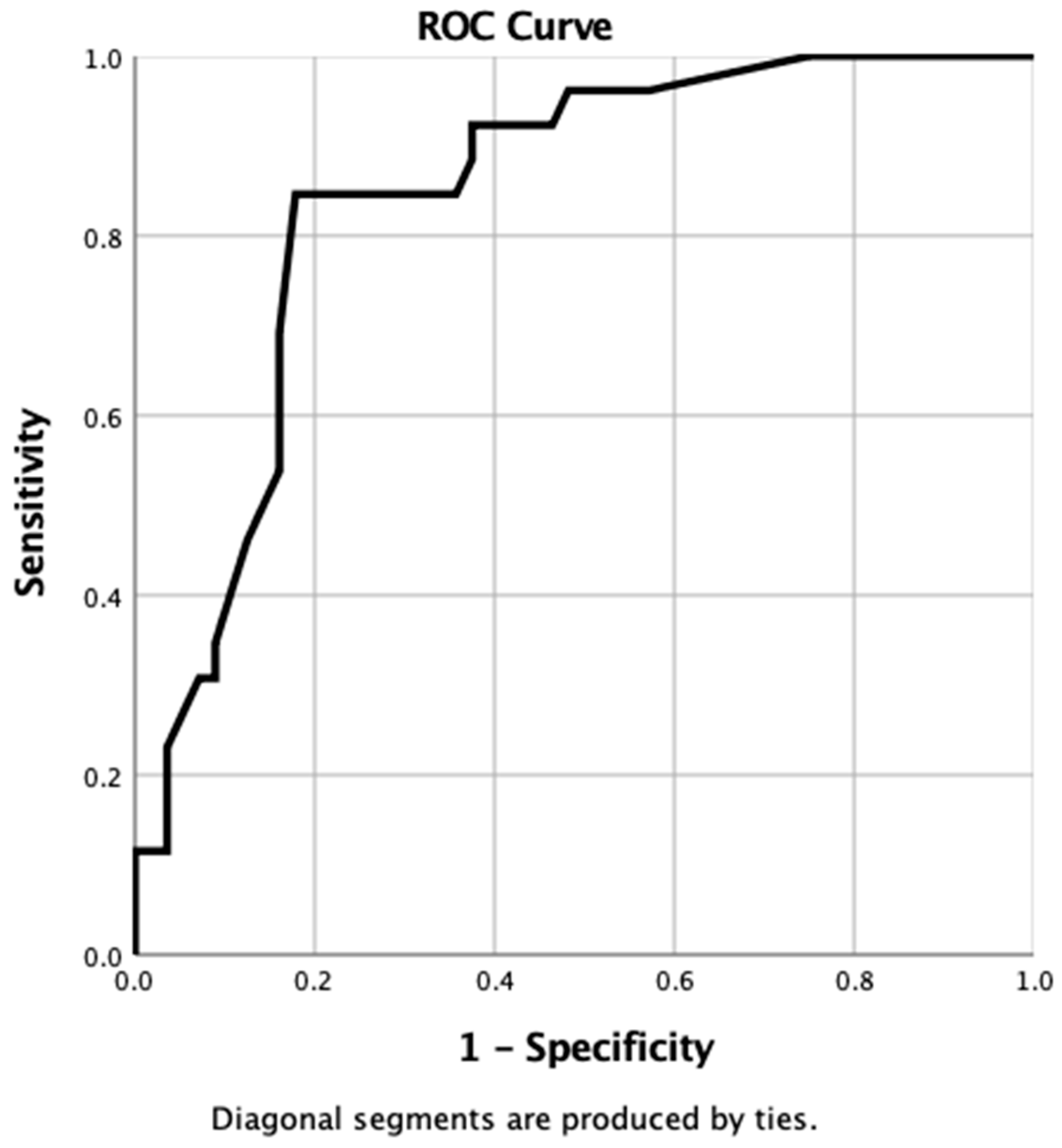
2.3. Using a ROC Curve to Evaluate the Predictive Accuracy of Individual Tumour Characteristics
2.4. Nomogram Construction
2.5. Statistical Validation of the Nomograms
2.6. Validation of the Nomograms Using an Independent Dataset
2.7. Nomogram Validation by Manual Calculation of Values
2.8. Sensitivity, Specificity and ROC Validation of the Nomograms
3. Results
3.1. Clinical Train Dataset
3.1.1. Patient Demographics
- Palpable characteristics: A true positive result was obtained in 21 patients, but a further 32 patients were wrongly predicted to experience recurrence when they did not (i.e., false positive). An accurate prediction of no recurrence was made in 43 patients (i.e., true negative), but tumours recurred in six patients when the test results suggested they would not (i.e., false negative). Overall, this gave a sensitivity of 78%, a specificity of 57%, a positive predictive value of 40%, and a negative predictive value of 88%;
- Grade: A true positive result was obtained in 15 patients, but a further 17 patients were wrongly predicted to experience recurrence when they did not. An accurate prediction of no recurrence was made in 58 patients, but tumours recurred in 12 patients when the test results suggested they would not. Overall, this gave a sensitivity of 56%, a specificity of 77%, a positive predictive value of 47%, and a negative predictive value of 83%.
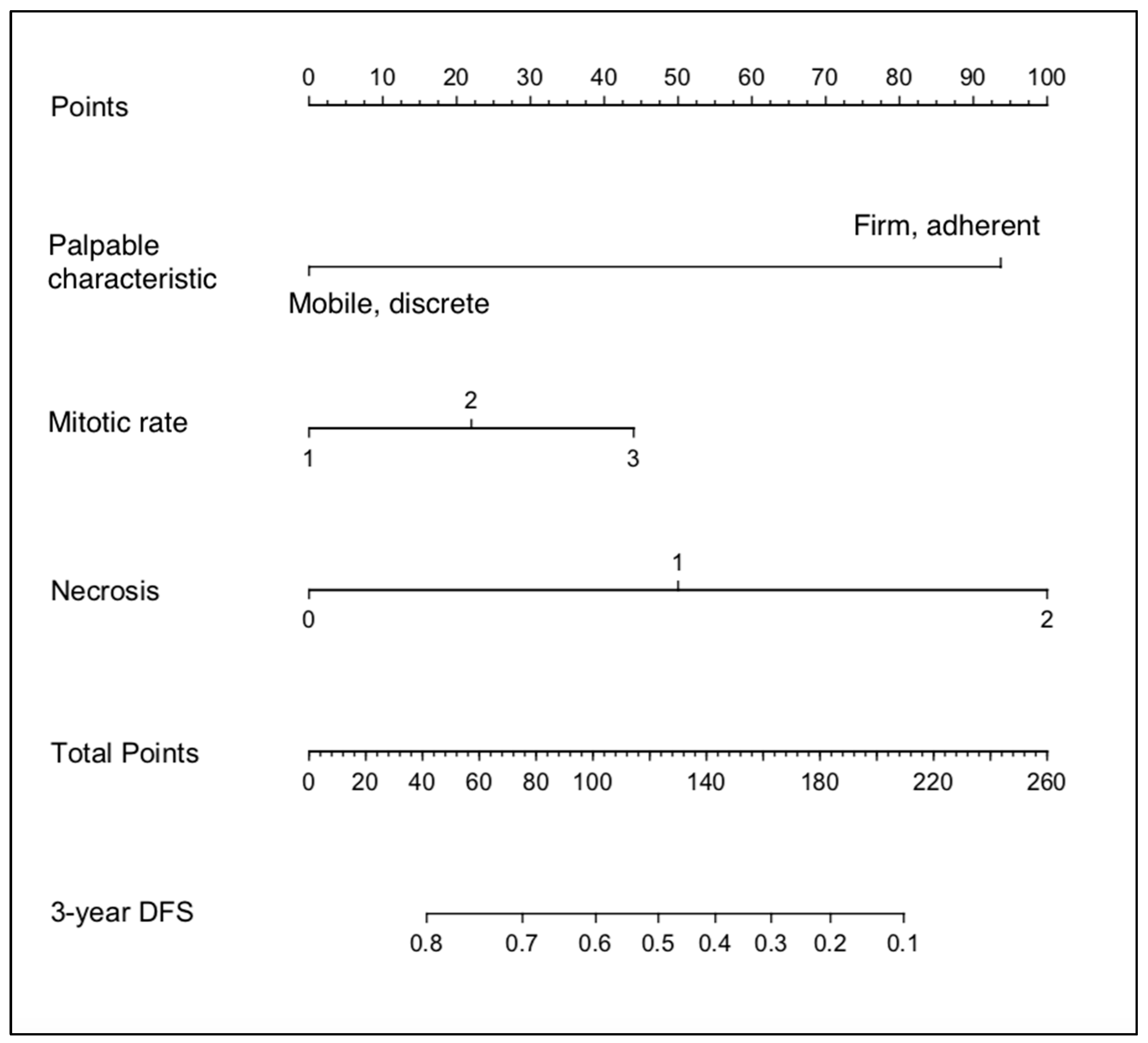
3.1.2. Nomogram Construction: Clinical
3.2. Statistical Validation of the Clinical Nomogram
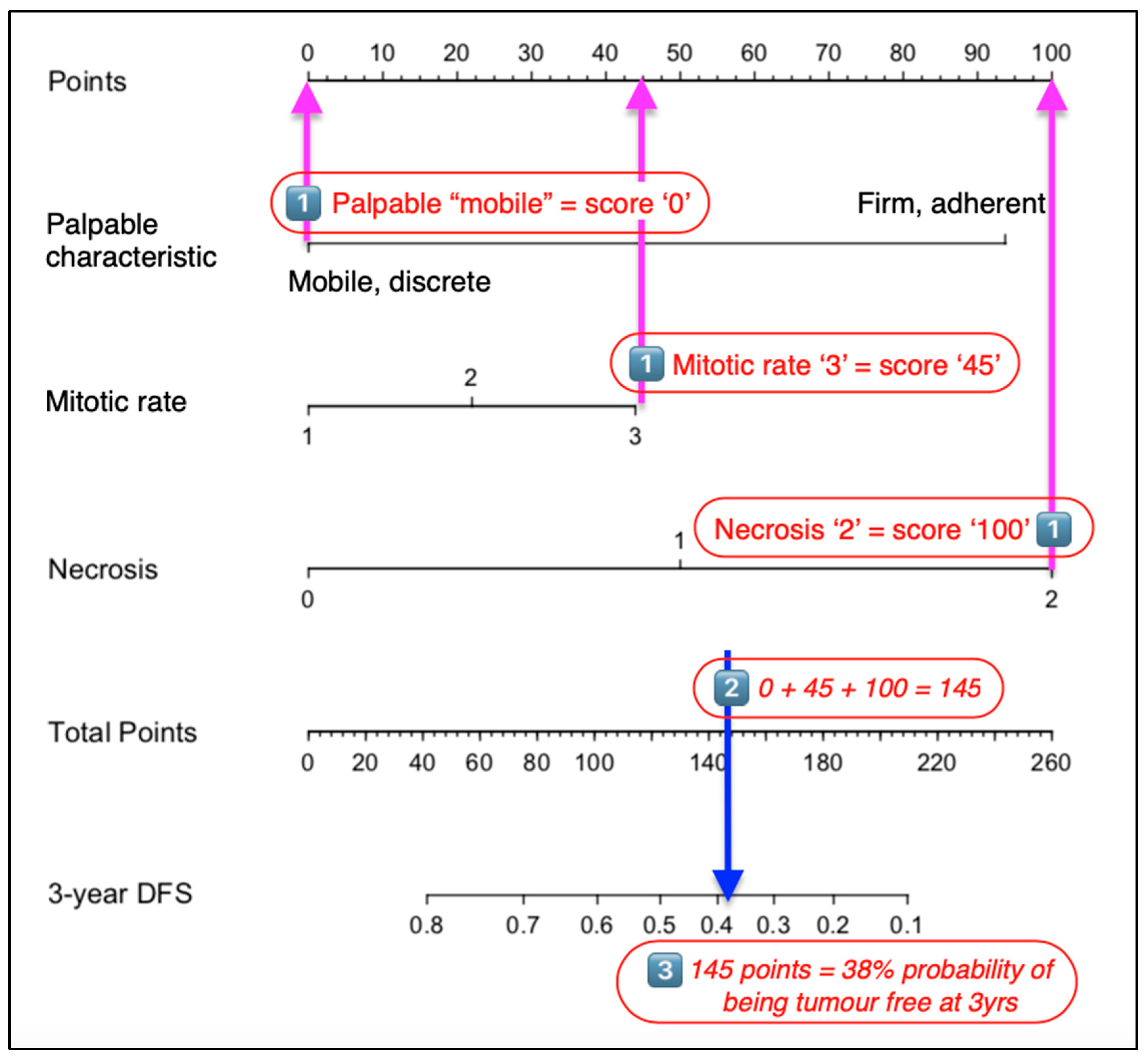
3.3. Manual Validation of the Clinical Nomogram
3.4. IHC Dataset
3.4.1. Patient Demographics
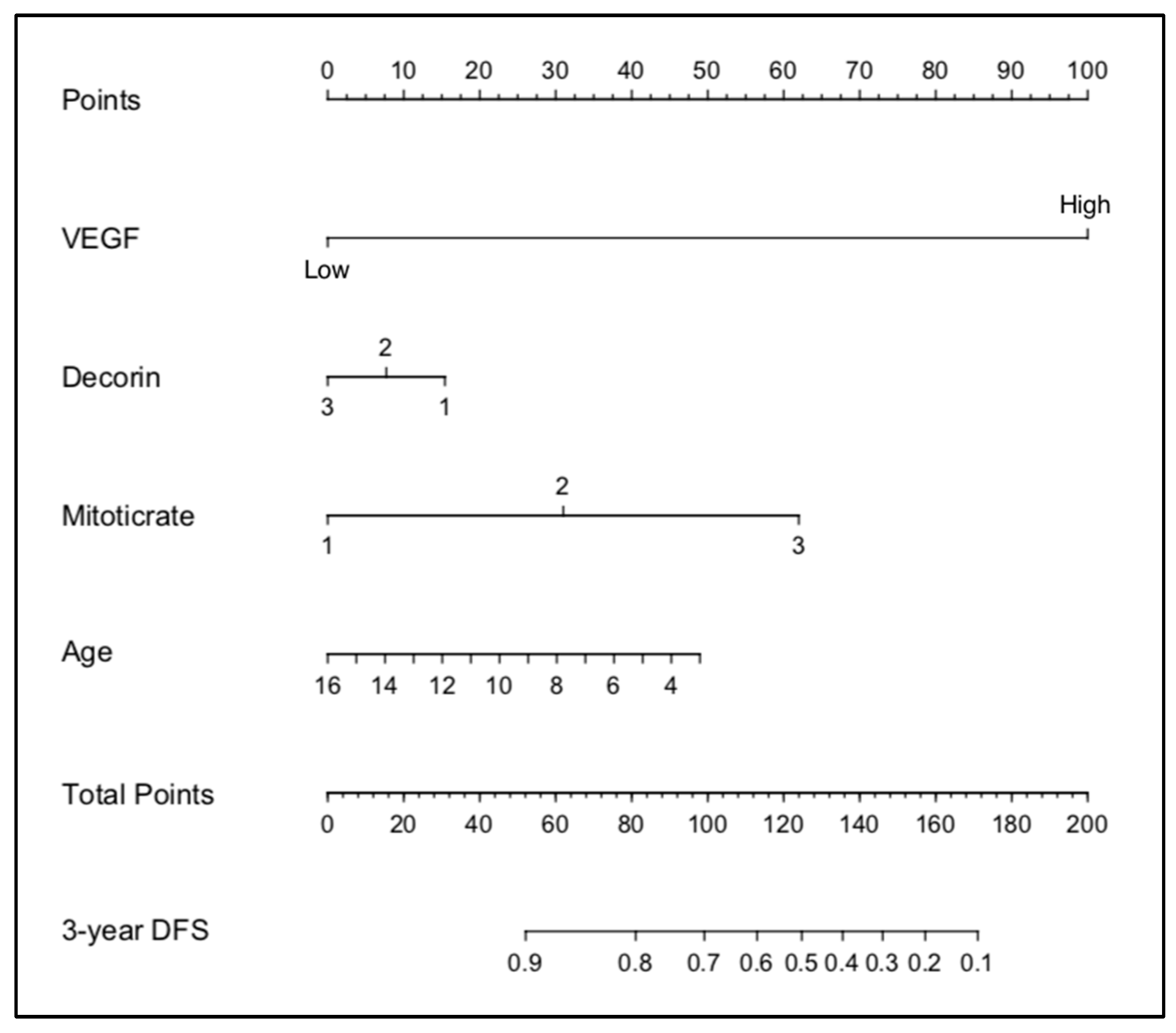
3.4.2. Nomogram Construction: IHC
3.4.3. Manual Validation of the IHC Nomogram
3.5. Summary of Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ehrhart, N. Soft-tissue sarcomas in dogs: A review. J. Am. Anim. Hosp. Assoc. 2005, 41, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Dennis, M.M.; McSporran, K.D.; Bacon, N.J.; Schulman, F.Y.; Foster, R.A.; Powers, B.E. Prognostic factors for cutaneous and subcutaneous soft tissue sarcomas in dogs. Vet. Pathol. 2011, 48, 73–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKnight, J.A.; Mauldin, G.N.; McEntee, M.C.; Meleo, K.A.; Patnaik, A.K. Radiation treatment for incompletely resected soft-tissue sarcomas in dogs. J. Am. Vet. Med. Assoc. 2000, 217, 205–210. [Google Scholar] [CrossRef]
- Bacon, N.J.; Dernell, W.S.; Ehrhart, N.; Powers, B.E.; Withrow, S.J. Evaluation of primary re-excision after recent inadequate resection of soft tissue sarcomas in dogs: 41 cases (1999–2004). J. Am. Vet. Med. Assoc. 2007, 230, 548–554. [Google Scholar] [CrossRef]
- Greene, F.L.; Sobin, L.H. The staging of cancer: A retrospective and prospective appraisal. CA Cancer J. Clin. 2008, 58, 180–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denoix, P.F. Nomenclature and classification of cancers based on an atlas. Acta Unio. Int. Contra. Cancrum. 1953, 9, 769–771. [Google Scholar] [PubMed]
- Owen, L.N. TNM Classification of Tumours in Domestic Animals; World Health Organization: Geneva, Switzerland, 1980.
- MacEwan, E.G.; Powers, B.; Macy, D.W.; Withrow, S. Soft Tissue Sarcomas. In Small Animal Clinical Oncology, 3rd ed.; Withrow, S., MacEwan, E.G., Eds.; Saunders: Philadelphia, PA, USA, 2001; pp. 283–304. [Google Scholar]
- Liptak, J.M.; Forrest, L.J. Soft tissue sarcomas. In Withrow & McEwen’s Small Animal Clinical Oncology, 5th ed.; Withrow, S.J., Vail, D.M., Page, R.L., Eds.; Elsevier: Maryland Heights, MO, USA, 2013; pp. 356–380. [Google Scholar]
- Kuntz, C.A.; Dernell, W.S.; Powers, B.E.; Devitt, C.; Straw, R.C.; Withrow, S.J. Prognostic factors for surgical treatment of soft-tissue sarcomas in dogs: 75 cases (1986–1996). J. Am. Vet. Med. Assoc. 1997, 211, 1147–1151. [Google Scholar]
- Monteiro, B.; Boston, S.; Monteith, G. Factors influencing complete tumor excision of mast cell tumors and soft tissue sarcomas: A retrospective study in 100 dogs. Can. Vet. J. 2011, 52, 1209–1214. [Google Scholar] [PubMed]
- Kamstock, D.A.; Ehrhart, E.J.; Getzy, D.M.; Bacon, N.J.; Rassnick, K.M.; Moroff, S.D.; Liu, S.M.; Straw, R.C.; McKnight, C.A.; Amorim, R.L.; et al. Recommended guidelines for submission, trimming, margin evaluation, and reporting of tumor biopsy specimens in veterinary surgical pathology. Vet. Pathol. 2011, 48, 19–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emmadi, R.; Wiley, E.L. Evaluation of Resection Margins in Breast Conservation Therapy: The Pathology Perspective—Past, Present, and Future. Int. J. Surg. Oncol. 2012, 2012, 180259. [Google Scholar] [CrossRef] [Green Version]
- Balachandran, V.P.; Gonen, M.; Smith, J.J.; DeMatteo, R.P. Nomograms in oncology: More than meets the eye. Lancet Oncol. 2015, 16, 173–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kattan, M.W.; Leung, D.H.Y.; Brennan, M.F. Postoperative nomogram for 12-year sarcoma-specific death. J. Clin. Oncol. 2002, 20, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Zivanovic, O.; Jacks, L.M.; Iasonos, A.; Leitao, M.M., Jr.; Soslow, R.A.; Veras, E.; Chi, D.S.; Abu-Rustum, N.R.; Barakat, R.R.; Brennan, M.F.; et al. A nomogram to predict postresection 5-year overall survival for patients with uterine leiomyosarcoma. Cancer 2012, 118, 660–669. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.J.; Lemieux, A.; Kalpathy-Cramer, J.; Ord, C.B.; Walker, G.V.; Fuller, C.D.; Kim, J.-S.; Thomas, C.R., Jr. Nomogram for predicting the benefit of adjuvant chemoradiotherapy for resected gallbladder cancer. J. Clin. Oncol. 2011, 29, 4627–4632. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.J.; Patel, S.G.; Shah, J.P.; Goldstein, D.P.; Irish, J.C.; Carvalho, A.L.; Kowalski, L.P.; Lockhart, J.L.; Holland, J.M.; Gross, N.D. An oral cavity carcinoma nomogram to predict benefit of adjuvant radiotherapy. JAMA Otolaryngol. Head Neck Surg. 2013, 139, 554–559. [Google Scholar]
- Abdollah, F.; Sun, M.; Suardi, N.; Gallina, A.; Bianchi, M.; Tutolo, M.; Passoni, N.; Tian, Z.; Salonia, A.; Colombo, R.; et al. Prediction of functional outcomes after nerve-sparing radical prostatectomy: Results of conditional survival analyses. Eur. Urol. 2012, 62, 42–52. [Google Scholar] [CrossRef]
- Chipman, J.J.; Sanda, M.G.; Dunn, R.L.; Wei, J.T.; Litwin, M.S.; Crociani, C.M.; Regan, M.M.; Chang, P. Measuring and predicting prostate cancer related quality of life changes using EPIC for clinical practice. J. Urol. 2014, 191, 638–645. [Google Scholar] [CrossRef]
- Weiser, M.R.; Landmann, R.G.; Kattan, M.W.; Gonen, M.; Shia, J.; Chou, J.; Paty, P.B.; Guillem, J.G.; Temple, L.K.; Schrag, D.; et al. Individualized prediction of colon cancer recurrence using a nomogram. J. Clin. Oncol. 2008, 26, 380–385. [Google Scholar] [CrossRef]
- Pleijhuis, R.G.; Kwast, A.B.; Jansen, L.; de Vries, J.; Lanting, R.; Bart, J.; Wiggers, T.; van Dam, G.M.; Siesling, S. A validated web-based nomogram for predicting positive surgical margins following breast-conserving surgery as a preoperative tool for clinical decision-making. Breast 2013, 22, 773–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayashi, Y.; Xiao, L.; Suzuki, A.; Blum, M.A.; Sabloff, B.; Taketa, T.; Maru, D.M.; Welsh, J.; Lin, S.H.; Weston, B.; et al. A nomogram associated with high probability of malignant nodes in the surgical specimen after trimodality therapy of patients with oesophageal cancer. Eur. J. Cancer 2012, 48, 3396–3404. [Google Scholar] [CrossRef] [Green Version]
- Gospodarowicz, M.; Benedet, L.; Hutter, R.V.; Fleming, I.; Henson, D.E.; Sobin, L.H. History and international developments in cancer staging. Cancer Prev. Control. 1998, 2, 262–268. [Google Scholar] [PubMed]
- Specht, M.C.; Kattan, M.W.; Gonen, M.; Fey, J.; Van Zee, K.J. Predicting nonsentinel node status after positive sentinel lymph biopsy for breast cancer: Clinicians versus nomogram. Ann. Surg. Oncol. 2005, 12, 654–659. [Google Scholar] [CrossRef] [PubMed]
- Bray, J.; Polton, G.; Mcsporran, K.; Bridges, J.; Whitbread, T. Soft Tissue Sarcoma Managed in First Opinion Practice: Outcome in 350 cases. Vet. Surg. 2014, 43, 774–782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, J. Understanding the Prognosis and Progression of Soft Tissue Sarcoma in the Dog: A Thesis presented in partial fulfilment of the requirements for the degree of Doctor of Philosophy at Massey University, Manawatū, New Zealand. Ph.D. Thesis, Massey University, Manawatū, New Zealand, 2020. [Google Scholar]
- Kattan, M.W.; Scardino, P.T. Prediction of progression: Nomograms of clinical utility. Clin. Prostate Cancer 2002, 1, 90–99. [Google Scholar] [CrossRef]
- Hoo, Z.H.; Candlish, J.; Teare, D. What is an ROC curve? Emerg. Med. J. 2017, 34, 357–359. [Google Scholar] [CrossRef] [Green Version]
- Harrell, F.J. Regression Modeling Strategies. Bios 2019, 330, 164. [Google Scholar]
- Bartlett, J. Adjusting for Optimism/Overfitting in Measures of Predictive Ability Using Bootstrapping. Available online: https://thestatsgeek.com/2014/10/04/adjusting-for-optimismoverfitting-in-measures-of-predictive-ability-using-bootstrapping/ (accessed on 25 August 2019).
- Demetriou, J.L.; Brearley, M.J.; Constantino-Casas, F.; Addington, C.; Dobson, J.M. Intentional marginal excision of canine limb soft tissue sarcomas followed by radiotherapy. J. Small Anim. Pract. 2012, 53, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Chase, D.; Bray, J.; Ide, A.; Polton, G. Outcome following removal of canine spindle cell tumours in first opinion practice: 104 cases. J. Small Anim. Pract. 2009, 50, 568–574. [Google Scholar] [CrossRef] [PubMed]
- Banks, T.; Straw, R.; Thomson, M.; Powers, B. Soft tissue sarcomas in dogs: A study correlating optimal surgical margin with tumour grade. Aust. Vet. Pract. 2004, 34, 158–163. [Google Scholar]
- Nurkin, S.J.; Kane Iii, J.M. Margin Status, Local Recurrence, and Survival: Correlation or Causation? Surg. Oncol. Clin. N. Am. 2012, 21, 255–267. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, Y.A.; Huddy, J.R.; Miller, J.D.; Strauss, D.C.; Thomas, J.M.; Hayes, A.J. Unplanned excision of soft tissue sarcoma results in increased rates of local recurrence despite full further oncological treatment. Ann. Surg. Oncol. 2012, 19, 871–877. [Google Scholar] [CrossRef] [PubMed]
- Scarpa, F.; Sabattini, S.; Marconato, L.; Capitani, O.; Morini, M.; Bettini, G. Use of histologic margin evaluation to predict recurrence of cutaneous malignant tumors in dogs and cats after surgical excision. J. Am. Vet. Med. Assoc. 2012, 240, 1181–1187. [Google Scholar] [CrossRef] [Green Version]
- Stojadinovic, A.; Leung, D.H.; Allen, P.; Lewis, J.J.; Jaques, D.P.; Brennan, M.F. Primary adult soft tissue sarcoma: Time-Dependent influence of prognostic variables. J. Clin. Oncol. 2002, 20, 4344–4352. [Google Scholar] [CrossRef]
- Dickinson, I.C.; Whitwell, D.J.; Battistuta, D.; Thompson, B.; Strobel, N.; Duggal, A.; Steadman, P. Surgical margin and its influence on survival in soft tissue sarcoma. ANZ J. Surg. 2006, 76, 104–109. [Google Scholar] [CrossRef]
- McSporran, K.D. Histologic grade predicts recurrence for marginally excised canine subcutaneous soft tissue sarcomas. Vet. Pathol 2009, 46, 928–933. [Google Scholar] [CrossRef] [PubMed]
- Stojadinovic, A.; Leung, D.H.; Hoos, A.; Jaques, D.P.; Lewis, J.J.; Brennan, M.F. Analysis of the prognostic significance of microscopic margins in 2,084 localized primary adult soft tissue sarcomas. Ann. Surg. 2002, 235, 424–434. [Google Scholar] [CrossRef]
- Neill, T.; Schaefer, L.; Iozzo, R.V. Decorin: A guardian from the matrix. Am. J. Pathol. 2012, 181, 380–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, S.; Birk, D.E. Focus on Molecules: Decorin. Exp. Eye Res. 2011, 92, 444. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | AUC | Significance | 95% Confidence Interval |
|---|---|---|---|
| Size | 0.581 | p = 0.215 | 0.45–0.711 |
| Palpable characteristics | 0.676 | p = 0.007 | 0.561–0.79 |
| Differentiation | 0.534 | p = 0.606 | 0.406–0.661 |
| Mitotic rate | 0.584 | p = 0.197 | 0.453–0.715 |
| Necrosis | 0.604 | p = 0.109 | 0.472–0.737 |
| Grade | 0.666 | p = 0.011 | 0.541–0.792 |
| Age | 0.488 | p = 0.856 | 0.376–0.6 |
| Mitoses | 0.629 | p = 0.047 | 0.501–0.757 |
| Clinical Characteristic | Significance (p Value) | HR | 95.0% CI for HR Lower Upper | ||
|---|---|---|---|---|---|
| 1 | Well-differentiated | 0.995 | - | - | - |
| Moderately differentiated | 0.949 | 0.967 | 0.346 | 2.7 | |
| Poorly differentiated | 0.966 | 1.054 | 0.096 | 11.595 | |
| 2 | Size (<1 cm) | 0.778 | - | - | - |
| Size (1–5 cm) | 0.329 | 1.623 | 0.613 | 4.296 | |
| Size (>5 cm) | 0.611 | 1.334 | 0.44 | 4.048 | |
| 3 | Age | 0.79 | 0.98 | 0.846 | 1.136 |
| 4 | Mitoses | 0.731 | 1.011 | 0.95 | 1.075 |
| 5 | Grade 1 | 0.657 | - | - | - |
| Grade 2 | 0.736 | 0.783 | 0.188 | 3.253 | |
| Grade 3 | 0.389 | 0.303 | 0.02 | 4.598 | |
| 6 | Palpable (discrete) | ||||
| Palpable (firm, immobile) | 0.035 | 2.403 | 1.065 | 5.421 | |
| Mitotic rate score 1 | 0.015 | - | - | - | |
| Mitotic rate score 2 | 0.11 | 2.141 | 0.841 | 5.446 | |
| Mitotic rate score 3 | 0.007 | 5.08 | 1.571 | 1422 | |
| Necrosis score 1 | 0.181 | - | - | - | |
| Necrosis score 2 | 0.156 | 0.49 | 0.183 | 1.313 | |
| Necrosis score 3 | 0.318 | 2.128 | 0.483 | 9.377 | |
| Parameter | AUC | Significance | 95% Confidence Interval |
|---|---|---|---|
| VEGF | 0.786 | p ≤ 0.001 | 0.677–0.895 |
| Decorin | 0.534 | p = 0.628 | 0.398–0.669 |
| Differentiation | 0.488 | p = 0.863 | 0.354–0.622 |
| Mitotic rate | 0.517 | p = 0.804 | 0.379–0.655 |
| Necrosis | 0.54 | p = 0.572 | 0.399–0.68 |
| Grade | 0.506 | p = 0.936 | 0.37–0.642 |
| Age | 0.626 | p = 0.072 | 0.5–0.752 |
| Size | 0.52 | p = 0.779 | −0.665 |
| Clinical Characteristic | Significance | HR | 95.0% CI for HR | ||
|---|---|---|---|---|---|
| (p Value) | Lower | Upper | |||
| 1 | Well-differentiated | 0.9 | - | - | 6 |
| Moderately differentiated | 0.7 | 1.3 | 0.314 | ||
| Poorly differentiated | 0.9 | 0.6 | 0.004 | ||
| 2 | Size (<1 cm) | 0.8 | - | - | - |
| Size (1–5 cm) | 0.3 | 1.623 | 0.613 | 4.296 | |
| Size (>5 cm) | 0.6 | 1.334 | 0.44 | 4.048 | |
| 3 | Grade 1 | 0.6 | - | - | - |
| Grade 2 | 0.7 | 0.723 | 0.135 | 3.882 | |
| Grade 3 | 0.3 | 0.231 | 0.014 | 3.786 | |
| 4 | Necrosis score 1 | 0.3 | - | - | - |
| Necrosis score 2 | 0.3 | 0.564 | 0.198 | 1.607 | |
| Necrosis score 3 | 0.4 | 1.842 | 0.437 | 7.764 | |
| 5 | Palpable (discrete) | - | - | - | |
| Palpable (firm, immobile) | 0.2 | 1.769 | 0.675 | 4.635 | |
| 6 | VEGF low | - | - | - | |
| VEGF high | <0.0001 | 31.25 | 5.197 | 187.903 | |
| Decorin type 1 | 0.1 | - | - | - | |
| Decorin type 2 | 0.9 | 1.097 | 0.394 | 3.06 | |
| Decorin type 3 | 0.1 | 0.397 | 0.134 | 1.18 | |
| Mitotic rate score 1 | 0.01 | - | - | - | |
| Mitotic rate score 2 | 0.6 | 0.727 | 0.207 | 2.551 | |
| Mitotic rate score 3 | 0.002 | 25.271 | 3.257 | 19062 | |
| Age | 0.1 | 0.856 | 0.71 | 1.031 | |
| C-Index | AUC of ROC Curve (95% CI) | Sens | Spec | PPV | NPV | |
|---|---|---|---|---|---|---|
| Individual Characteristics | ||||||
| Palpable | 0.68 | 78% | 57% | 40% | 88% | |
| Grade only | 0.67 | 56% | 77% | 47% | 83% | |
| VEGF | 0.79 | 84% | 70% | 56% | 90% | |
| Nomograms | ||||||
| Clinical nomogram | ||||||
| Training dataset | 71% | 0.67 (0.6–0.75) | 82% | 40% | 27% | 89% |
| Validation dataset | 51% | |||||
| IHC nomogram | 75% | 0.84 (0.76–0.93) | 96% | 45% | 45% | 96% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bray, J.P.; Munday, J.S. Development of a Nomogram to Predict the Outcome for Patients with Soft Tissue Sarcoma. Vet. Sci. 2023, 10, 266. https://doi.org/10.3390/vetsci10040266
Bray JP, Munday JS. Development of a Nomogram to Predict the Outcome for Patients with Soft Tissue Sarcoma. Veterinary Sciences. 2023; 10(4):266. https://doi.org/10.3390/vetsci10040266
Chicago/Turabian StyleBray, Jonathan P., and John S. Munday. 2023. "Development of a Nomogram to Predict the Outcome for Patients with Soft Tissue Sarcoma" Veterinary Sciences 10, no. 4: 266. https://doi.org/10.3390/vetsci10040266