

Automatic Localization of Seizure Onset Zone Based on Multi-Epileptogenic Biomarkers Analysis of Single-Contact from Interictal SEEG
 ,
,
Abstract
:
1. Introduction
- We presented a high-sensitivity SOZ localization method based on multiple epileptogenic biomarkers analysis of single contact;
- We demonstrated that normalized pathological ripple rate with the regional +10% threshold can significantly improve the ability of SOZ identification;
- Machine learning and deep learning algorithms, such as SEEG-Net, AM, and Focal loss, were employed in each stage of the entire process. Cross validation was performed for stronger generality and generalization;
- Consistency was maintained with real clinical settings of preoperative DRE assessment. Individual SOZ prediction and visualization on MRI was provided to make reliable and explainable support.
2. Methods
2.1. MEBM-SC Overview
2.2. Detection of Multiple Epileptogenic Biomarkers
| Algorithm 1: Preliminary Screening Algorithm | |
| Require: 1: sigfull: original signal; sigfiltered: bandpass filtered signal 2: env: Hilbert envelope of smoothed bandpass signal 3: stdata: sigfull 81–500 Hz Stockwell transform 4: : Sampling frequency; : any time; Eol: event of interest 5: threshold: ripple is 30, fastripple is 20 | |
| Ensure: | |
| 7: | ▷ Relative energy, the ratio of the energy occupied by a certain frequency at that moment |
| 8: | ▷ Signal energy entropy |
| 9: if , sigfull 0.9 & sigfiltered 10 | |
| 10: baselineenv(t); baselineFilteredsigfiltered(t) | |
| 11: thrbaseline experience accumulation function 95% threshold | |
| 12: thrFiltbaselineFiltered experience accumulation function 99% threshold | |
| 13: end if | |
| 14: if , env(t)0.99 & threshold | |
| 15: eventenv(t) | |
| 16: numberThe number of times each event crossed thrFilt | |
| 17: if 6 | |
| 18: Eolevent | |
| 19: end if | |
| 20: end if | |
| 21: for do | |
| 22: | |
| 23: end for | |
2.3. Multiple Features Extraction of Contacts
2.3.1. Signal Distribution of Contact
Spike Rate
Normalized Pathological Ripples (Rs) Rate
Fast Ripples (FRs) Rate
Ripples Co-Occurring with FRs(R&FRs) Rate
2.3.2. Signal Energy of Contact
Spike Energy
Ripples Energy
Fast Ripples Energy & R&FRs Complex Wave Energy
2.4. Feature Selection and Contact Classification
2.4.1. Feature Selection Based on ShapHT+
- (a)
- We used the tree SHAP method to determine local importance. The algorithm is:
- (b)
- Feature ’s global relevance is:
- (c)
- We provide an adaptable threshold for assessing the relevance of features. As a result, the possibility that a feature is irrelevant is determined by computing proportion of features in sequence whose local relevance is lower than adaptive threshold. Hence, the final threshold is expressed as follows:
- (d)
- In addition, hypothesis tests were conducted to rule out irrelevant features. All the relevant characteristics were gathered as the initial features are sorted into relevant and irrelevant groups. The ideal feature subset had a good association with the label and little redundancy among features.
2.4.2. Contact Classification Based on AM and Focal Loss
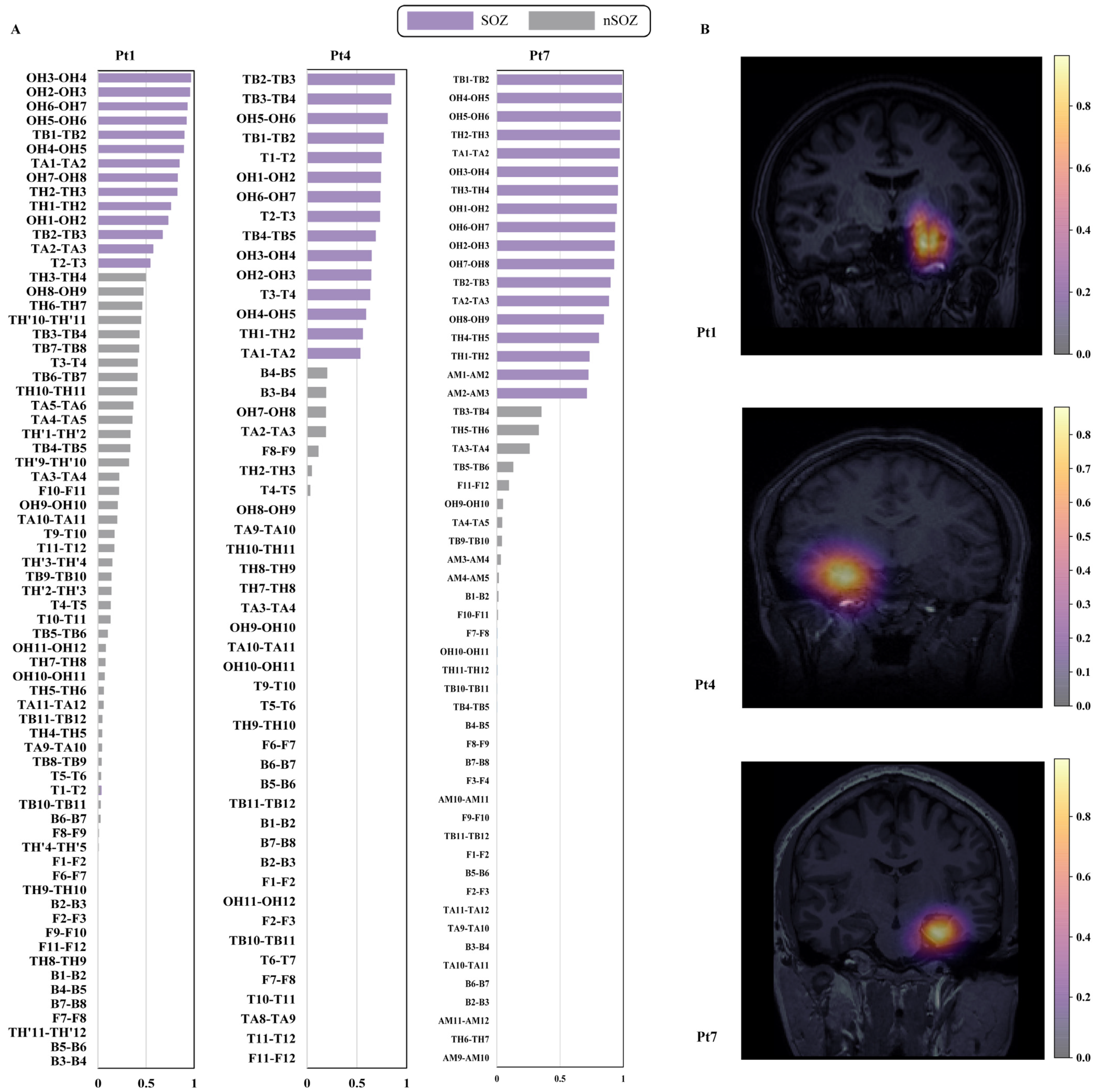
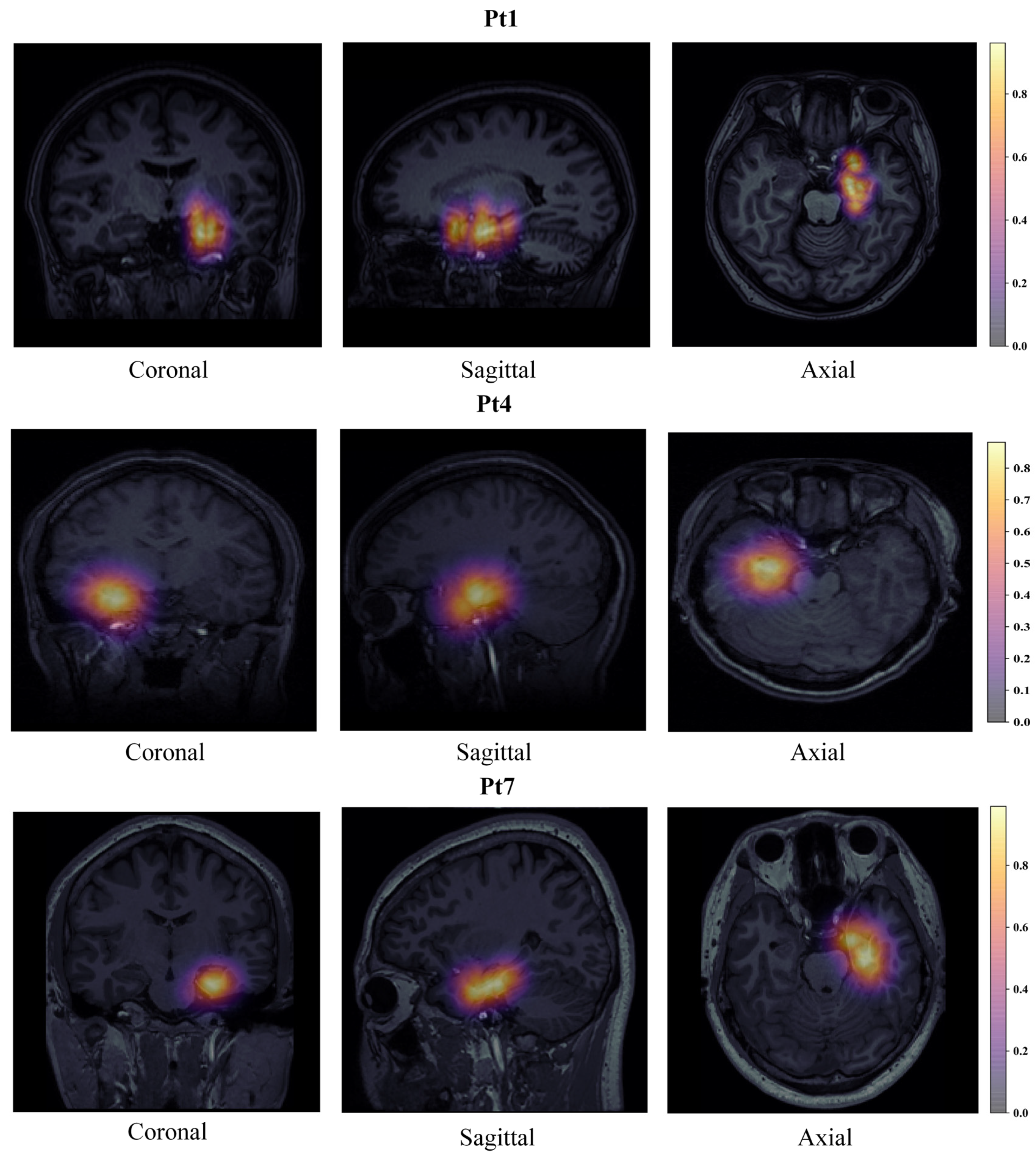
2.5. Individualized SOZ Prediction and Visualizaiton
- Considering the low correlation between brain boundary voxels and SOZ, this section set brain boundary voxels to the lowest quantified value;
- Considering the strong correlation between the SOZ surrounding voxels and SOZ contacts, we set SOZ contacts and their surrounding voxels to the predicted value corresponding to the contact;
- To further achieve whole-brain mapping, we used a 3D Gaussian kernel method to map all other voxels in the whole brain. The other voxels’ values are between the predicted values of the SOZ surrounding voxels and the quantified values of the brain boundary voxels;
- The predictive values of all voxels were calculated through the above interpolation method, ranging from 0 to 1. Then, we visualized the predictive values on the MRI. Thus, individualized SOZ prediction and visualization were obtained.
3. Experiments and Results
3.1. Patient Selection and Dataset Processing
- (a)
- the patient has focal DRE;
- (b)
- seizure free and outcome is Engel 1;
- (c)
- a curative epilepsy surgery has been conducted;
- (d)
- pathology is hippocampal sclerosis (HS);
- (e)
- long-term SEEG monitoring, and post-operative structural MRI are obtainable;
- (f)
- a minimum of six months of post-operative follow-up;
- (g)
- at least one recorded seizure exhibits rhythmic activity.
3.2. Experimental Protocols
3.2.1. Validation Protocols
3.2.2. Evaluation Metrics
3.2.3. Parameter Setting
3.3. Results for SOZ Localization Based on Cross Validation
3.4. Ablation Study
3.4.1. Multi Biomarkers Features of Contacts
- feature a (Multiple features of spike): we utilize the pathological signal distribution and energy of spike;
- feature b (Multiple features of HFOs): we employ the pathological signal distribution and energy of HFOs;
- feature c (Multiple features of spike and HFOs): we add the pathological signal distribution and energy of both biomarkers;
- feature d (Multiple features of spike and normalized pathological HFOs): add the normalization of ripples by the regional atlas threshold, based on feature c;
- feature e/MEBM-SC (Multiple features of spike and regional+10% based on normalized pathological HFOs): add the normalization of ripples by the regional + 10% threshold, based on feature c.
3.4.2. Feature Selection Methods
- selection a (XGBoost): exploit XGBoost as feature selection method and classifier;
- selection b (RFE-XGBoost): applie SVM-RFE as feature selection method and classifier;
- selection c (ShapHT++DNN): employ a shallow deep learning model, DNN as the feature selection method and classifier;
- selection d (ShapHT+self-AM+DNN): add self-attention machine based on selection c;
- selection e/MEBM-SC (ShapHT+AM+DNN): add attention machine based on selection c.
4. Discussion
4.1. Comparison with Other Methods
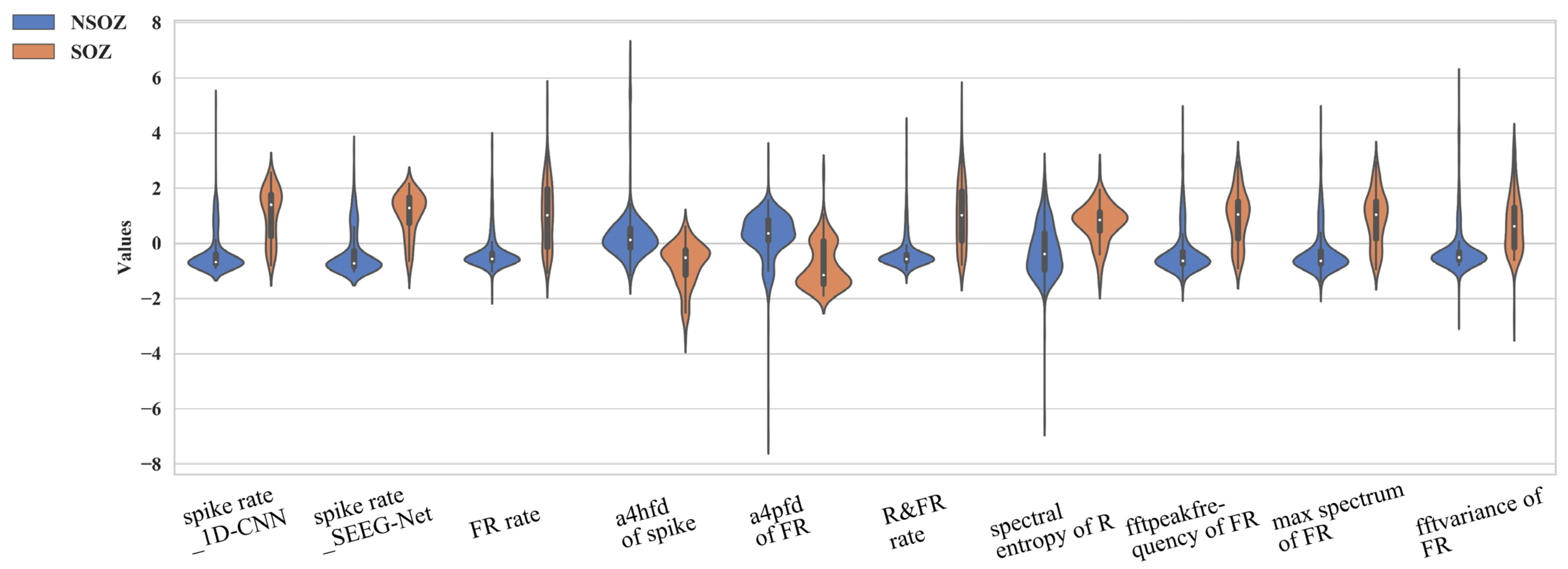
4.2. Significant Numerical Features of Epileptogenic Biomarkers
4.3. Extraction of Normalized Pathological HFOs Rate
4.4. Visualization of Electrodes with MRI
4.5. Limitations and Future Work
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Thijs, R.D.; Surges, R.; O’Brien, T.J.; Sander, J.W. Epilepsy in adults. Lancet 2019, 393, 689–701. [Google Scholar] [CrossRef] [PubMed]
- Dalic, L.; Cook, M.J. Managing drug-resistant epilepsy: Challenges and solutions. Neuropsychiatr. Dis. Treat. 2016, 12, 2605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, M.; Wan, T.; Wan, X.; Fang, Z.; Du, Y. A new localization method for epileptic seizure onset zones based on time-frequency and clustering analysis. Pattern Recognit. 2021, 111, 107687. [Google Scholar] [CrossRef]
- de Borman, A.; Vespa, S.; Tahry, R.E.; Absil, P.A. Estimation of seizure onset zone from ictal scalp EEG using independent component analysis in extratemporal lobe epilepsy. J. Neural. Eng. 2022, 19, 026005. [Google Scholar] [CrossRef]
- Foldes, S.T.; Munter, B.T.; Appavu, B.L.; Kerrigan, J.F.; Adelson, P.D. Shift in electrocorticography electrode locations after surgical implantation in children. Epilepsy Res. 2020, 167, 106410. [Google Scholar] [CrossRef]
- Pellegrino, G.; Hedrich, T.; Chowdhury, R.; Hall, J.A.; Lina, J.M.; Dubeau, F.; Kobayashi, E.; Grova, C. Source localization of the seizure onset zone from ictal EEG/MEG data. Hum. Brain Mapp. 2016, 37, 2528–2546. [Google Scholar] [CrossRef] [Green Version]
- McGonigal, A.; Bartolomei, F.; Regis, J.; Guye, M.; Gavaret, M.; Trebuchon-Da Fonseca, A.; Dufour, H.; Figarella-Branger, D.; Girard, N.; Peragut, J.C.; et al. Stereoelectroencephalography in presurgical assessment of MRI-negative epilepsy. Brain 2007, 130, 3169–3183. [Google Scholar] [CrossRef]
- Zhao, B.; Hu, W.; Zhang, C.; Wang, X.; Wang, Y.; Liu, C.; Mo, J.; Yang, X.; Sang, L.; Ma, Y.; et al. Integrated Automatic Detection, Classification and Imaging of High Frequency Oscillations With Stereoelectroencephalography. Front. Neurosci. 2020, 14, 546. [Google Scholar] [CrossRef]
- Frauscher, B.; von Ellenrieder, N.; Zelmann, R.; Rogers, C.; Nguyen, D.K.; Kahane, P.; Dubeau, F.; Gotman, J. High-Frequency Oscillations in the Normal Human Brain. Ann. Neurol. 2018, 84, 374–385. [Google Scholar] [CrossRef]
- Johnson, G.W.; Cai, L.Y.; Doss, D.J.; Jiang, J.W.; Negi, A.S.; Narasimhan, S.; Paulo, D.L.; González, H.F.J.; Roberson, S.W.; Bick, S.K.; et al. Localizing temporal lobe seizure onset zones using deep learning on SEEG cortico-cortical evoked potentials. bioRxiv 2022. [Google Scholar] [CrossRef]
- Jiang, H.; Kokkinos, V.; Ye, S.; Urban, A.; Bagić, A.; Richardson, M.; He, B. Interictal SEEG resting-state connectivity localizes seizure onset zone and predicts seizure outcome. Adv. Sci. 2022, 9, 2200887. [Google Scholar] [CrossRef] [PubMed]
- Klimes, P.; Cimbalnik, J.; Brazdil, M.; Hall, J.; Dubeau, F.; Gotman, J.; Frauscher, B. NREM sleep is the state of vigilance that best identifies the epileptogenic zone in the interictal electroencephalogram. Epilepsia 2019, 60, 2404–2415. [Google Scholar] [CrossRef] [PubMed]
- Xiao, L.; Li, C.; Wang, Y.; Chen, J.; Si, W.; Yao, C.; Li, X.; Duan, C.; Heng, P.-A. Automatic Localization of Seizure Onset Zone From High-Frequency SEEG Signals: A Preliminary Study. IEEE J. Transl. Eng. Health Med. 2021, 9, 1–10. [Google Scholar] [CrossRef]
- Li, J.; Grinenko, O.; Mosher, J.C.; Gonzalez-Martinez, J.; Leahy, R.M.; Chauvel, P. Learning to define an electrical biomarker of the epileptogenic zone. Hum. Brain Mapp. 2020, 41, 429–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinkovic, L.; Hecimovic, H.; Sulc, V.; Marecek, R.; Marusic, P. Modern techniques of epileptic focus localization. Int. Rev. Neurobiol. 2014, 114, 245–278. [Google Scholar] [CrossRef]
- Liu, S.; Sha, Z.; Sencer, A.; Aydoseli, A.; Bebek, N.; Abosch, A.; Henry, T.; Gurses, C.; Ince, N.F. Exploring the time-frequency content of high frequency oscillations for automated identification of seizure onset zone in epilepsy. J. Neural. Eng. 2016, 13, 026026. [Google Scholar] [CrossRef]
- Grinenko, O.; Li, J.; Mosher, J.C.; Wang, I.Z.; Bulacio, J.C.; Gonzalez-Martinez, J.; Nair, D.; Najm, I.; Leahy, R.M.; Chauvel, P. A fingerprint of the epileptogenic zone in human epilepsies. Brain 2018, 141, 117–131. [Google Scholar] [CrossRef] [Green Version]
- Zweiphenning, W.; von Ellenrieder, N.; Dubeau, F.; Martineau, L.; Minotti, L.; Hall, J.A.; Chabardes, S.; Dudley, R.; Kahane, P.; Gotman, J.; et al. Correcting for physiological ripples improves epileptic focus identification and outcome prediction. Epilepsia 2021, 63, 483–496. [Google Scholar] [CrossRef]
- Krikid, F.; Karfoul, A.; Chaibi, S.; Kachenoura, A.; Nica, A.; Kachouri, A.; Jeannès, R.L.B. Classification of High Frequency Oscillations in intracranial EEG signals based on coupled time-frequency and image-related features. Biomed. Signal Process. Control 2022, 73, 103418. [Google Scholar] [CrossRef]
- Wan, X.; Fang, Z.; Wu, M.; Du, Y. Automatic detection of HFOs based on singular value decomposition and improved fuzzy c-means clustering for localization of seizure onset zones. Neurocomputing 2020, 400, 1–10. [Google Scholar] [CrossRef]
- Cimbalnik, J.; Klimes, P.; Sladky, V.; Nejedly, P.; Jurak, P.; Pail, M.; Roman, R.; Daniel, P.; Guragain, H.; Brinkmann, B.; et al. Multi-feature localization of epileptic foci from interictal, intracranial EEG. Clin. Neurophysiol. 2019, 130, 1945–1953. [Google Scholar] [CrossRef] [PubMed]
- Akter, M.S.; Islam, M.R.; Iimura, Y.; Sugano, H.; Fukumori, K.; Wang, D.; Tanaka, T.; Cichocki, A. Multiband entropy-based feature-extraction method for automatic identification of epileptic focus based on high-frequency components in interictal iEEG. Sci. Rep. 2020, 10, 7044. [Google Scholar] [CrossRef]
- An, N.; Ye, X.; Liu, Q.; Xu, J.; Zhang, P. Localization of the epileptogenic zone based on ictal stereo-electroencephalogram: Brain network and single-channel signal feature analysis. Epilepsy Res. 2020, 167, 106475. [Google Scholar] [CrossRef]
- Wang, Y.; Dai, Y.; Liu, Z.; Guo, J.; Cao, G.; Ouyang, M.; Liu, D.; Shan, Y.; Kang, G.; Zhao, G. Computer-Aided Intracranial EEG Signal Identification Method Based on a Multi-Branch Deep Learning Fusion Model and Clinical Validation. Brain Sci. 2021, 11, 615. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Yang, Y.; Cao, G.; Guo, J.; Wei, P.; Feng, T.; Dai, Y.; Huang, J.; Kang, G.; Zhao, G. SEEG-Net: An explainable and deep learning-based cross-subject pathological activity detection method for drug-resistant epilepsy. Comput. Biol. Med. 2022, 148, 105703. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Wei, P.; Wang, Y.; Yang, Y.; Dai, Y.; Cao, G.; Kang, G.; Shan, Y.; Liu, D.; Xie, Y. Automatic Detection of High-Frequency Oscillations Based on an End-to-End Bi-Branch Neural Network and Clinical Cross-Validation. Comput. Intell. Neurosci. 2021, 2021, 7532241. [Google Scholar] [CrossRef]
- Liu, Z. Localization of Epileptic Seizure Onset Zone Based on High Frequency Oscillations Signal Detection; Beijing University of Post and Telecommunications: Beijing, China, 2021. [Google Scholar]
- Jacobs, J.; Wu, J.Y.; Perucca, P.; Zelmann, R.; Mader, M.; Dubeau, F.; Mathern, G.W.; Schulze-Bonhage, A.; Gotman, J. Removing high-frequency oscillations: A prospective multicenter study on seizure outcome. Neurology 2018, 91, e1040–e1052. [Google Scholar] [CrossRef]
- Liu, S.; Parvizi, J. Cognitive refractory state caused by spontaneous epileptic high-frequency oscillations in the human brain. Sci. Transl. Med. 2019, 11, eaax7830. [Google Scholar] [CrossRef]
- Miao, Y.; Iimura, Y.; Sugano, H.; Fukumori, K.; Shoji, T.; Tanaka, T. Seizure Onset Zone Identification Based on Phase-Amplitude Coupling of Interictal Electrocorticogram. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Guadalajara, Mexico, 1–5 November 2021; pp. 587–590. [Google Scholar]
- Yin, D.; Chen, D.; Tang, Y.; Dong, H.; Li, X. Adaptive feature selection with shapley and hypothetical testing: Case study of EEG feature engineering. Inf. Sci. 2022, 586, 374–390. [Google Scholar] [CrossRef]
- Lin, T.Y.; Goyal, P.; Girshick, R.; He, K.; Dollár, P. Focal loss for dense object detection. In Proceedings of the IEEE international Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 2980–2988. [Google Scholar]
- Burnos, S.; Frauscher, B.; Zelmann, R.; Haegelen, C.; Sarnthein, J.; Gotman, J. The morphology of high frequency oscillations (HFO) does not improve delineating the epileptogenic zone. Clin. Neurophysiol. 2016, 127, 2140–2148. [Google Scholar] [CrossRef]
- Lundberg, S.M.; Erion, G.; Chen, H.; DeGrave, A.; Prutkin, J.M.; Nair, B.; Katz, R.; Himmelfarb, J.; Bansal, N.; Lee, S.-I. From local explanations to global understanding with explainable AI for trees. Nat. Mach. Intell. 2020, 2, 56–67. [Google Scholar] [CrossRef] [PubMed]
- Murphy, P.M.; von Paternos, A.J.; Santaniello, S. A novel HFO-based method for unsupervised localization of the seizure onset zone in drug-resistant epilepsy. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Republic of Korea, 11–15 July 2017; pp. 1054–1057. [Google Scholar]
- Fang, Z.; Wan, X.; Wan, T. Fast automatic localization of epileptic seizure onset zones using complex Morlet wavelet transform-based singular value decomposition. In Proceedings of the 2018 37th Chinese Control Conference (CCC), Wuhan, China, 25–27 July 2018; pp. 4330–4334. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Multiple Features | Signal Distribution | Signal Energy | |
|---|---|---|---|
| Biomarkers | |||
| Spikes | Rate/min (Feature based,1D-CNN, SEEG-Net) | Media value of DWT (Kraskov entropy, Renyi entropy, Permutation entropy, Sample entropy, Shannon entropy, Energy, SVD entropy, Petrosan Fractal Dimension (PFD), Katz Fractal Dimension (KFD), Higuchi Fractal Dimension (HFD) | |
| Hfos | Ripples | Rate/min Normalized pathological ripples rate/min | Media value of Time (Energy, Time) Media value of FT (Maximum, Mean, Minimum, Peak frequency, Power, Power spectral density (Psd), Spectral entropy, Spectrum, Variance) Media value of DWT (Kraskov entropy, Renyi entropy, Permutation entropy, Sample entropy, Shannon entropy, Energy, SVD entropy, PFD, KFD, HFD) |
| Fast Ripples | Rate/min | Same as ripples | |
| Ripples co-occurring with FRs | Rate/min | Media value of Time (Energy, Time) Media value of FT (Maximum, Mean, Minimum, Peak frequency, Power, Power spectral density (Psd), Spectral entropy, Spectrum, Variance) Media value of DWT (Permutation entropy, Sample entropy, Shannon entropy, Energy, SVD entropy, PFD, KFD, HFD) | |
| Index | Region | 95th Percentile |
|---|---|---|
| 2 | Medial and basal temporal region | 19.5 |
| 7 | Superior, middle, and orbital frontal gyri and anterior part of inferior frontal gyrus | 3.5 |
| 8 | Middle and inferior temporal gyrus, temporal pole, and planum polare | 2.7 |
| 9 | Anterior and middle cingulate | 2 |
| Patient Id | Age | Sex | Number of SEEG Electrodes | Surgery Type | Outcome (Engel) | Follow-Up (Months) | Number of SOZ Contacts | Number of nSOZ Contacts |
|---|---|---|---|---|---|---|---|---|
| 1 | 38 | F | 8 | RF-TC | I | 33 | 15 | 55 |
| 2 | 35 | M | 7 | RF-TC | I | 32 | 13 | 45 |
| 3 | 34 | F | 8 | RF-TC | I | 16 | 11 | 43 |
| 4 | 27 | F | 7 | RF-TC | I | 12 | 15 | 36 |
| 5 | 22 | M | 7 | ATL | I | 12 | 4 | 29 |
| 6 | 20 | F | 6 | RF-TC | I | 9 | 14 | 34 |
| 7 | 34 | M | 6 | RF-TC | I | 9 | 14 | 40 |
| 8 | 22 | F | 6 | RF-TC | I | 9 | 12 | 18 |
| 9 | 30 | M | 7 | RF-TC | I | 12 | 8 | 26 |
| 10 | 21 | F | 7 | RF-TC | I | 18 | 14 | 23 |
| Total | - | - | - | - | - | - | 120 | 349 |
| Random Forest | Num of Estimators | Max Depth | Learning Rate | Class Weight |
|---|---|---|---|---|
| 100 | 3 | 0.1 | Balanced | |
| DNN classifier | Layer | In | Out | Dropout |
| Fully Connected (FC)1 | Feature num | 128 | 0.3 | |
| FC2 | 128 | 128 | - | |
| FC3 | 128 | 128 | 0.3 | |
| FC4 | 128 | Class num | - | |
| Training Epochs | Batch Size | Optimizer | Learning Rate | |
| Trainer | 20 | 4 | NAdam | 1 × 10−4 |
| Patient ID | Training & Valid/Testing ID | TP | TN | FP | FN | SEN [%] | SPE [%] | ACC [%] | PPV [%] | NPV [%] |
|---|---|---|---|---|---|---|---|---|---|---|
| Pt1 | Pt2-10/Pt1 | 14 | 55 | 0 | 1 | 93.33 | 100 | 98.57 | 100 | 98.21 |
| Pt2 | Pt1,3-10/Pt2 | 13 | 39 | 6 | 0 | 100 | 86.67 | 89.66 | 68.42 | 100 |
| Pt3 | Pt1-2,4-10/Pt3 | 8 | 42 | 1 | 3 | 72.73 | 97.67 | 92.59 | 88.89 | 93.33 |
| Pt4 | Pt1-3,5-10/Pt4 | 14 | 33 | 3 | 1 | 93.33 | 91.67 | 92.16 | 82.35 | 97.06 |
| Pt5 | Pt1-4,6-10/Pt5 | 3 | 29 | 0 | 1 | 75 | 100 | 96.97 | 100 | 96.67 |
| Pt6 | Pt1-5,7-10/Pt6 | 14 | 27 | 7 | 0 | 100 | 79.41 | 85.42 | 66.67 | 100 |
| Pt7 | Pt1-6,8-10/Pt7 | 14 | 36 | 4 | 0 | 100 | 90 | 92.59 | 77.78 | 100 |
| Pt8 | Pt1-7,9-10/Pt8 | 10 | 15 | 3 | 2 | 83.33 | 83.33 | 83.33 | 76.92 | 88.24 |
| Pt9 | Pt1-8,10/Pt9 | 6 | 24 | 2 | 2 | 75 | 92.31 | 88.24 | 75 | 92.31 |
| Pt10 | Pt1-9/Pt10 | 14 | 19 | 4 | 0 | 100 | 82.61 | 89.19 | 77.78 | 100 |
| Mean | - | - | - | - | 89.27 | 90.37 | 90.87 | 81.38 | 96.58 |
| Multi Biomarkers Features | Spike | HFOs | Pathological HFOs | Regional+10% Based Pathological HFOs | SEN [%] | SPE [%] | ACC [%] | PPV [%] | NPV [%] |
|---|---|---|---|---|---|---|---|---|---|
| feature a | √ | 78.80 | 89.95 | 87.74 | 72.89 | 93.37 | |||
| feature b | √ | 74.91 | 91.22 | 88.34 | 68.74 | 93.08 | |||
| feature c | √ | √ | 82.89 | 89.66 | 88.93 | 73.82 | 95.21 | ||
| feature d | √ | √ | 87.93 | 89.92 | 90.71 | 71.43 | 93.18 | ||
| feature e/ MEBM-SC | √ | √ | 89.27 | 90.37 | 90.87 | 81.38 | 96.58 |
| Feature Selection Methods | SEN [%] | SPE [%] | ACC [%] | PPV [%] | NPV [%] |
|---|---|---|---|---|---|
| XGBoost | 56.52 | 95.89 | 84.91 | 71.63 | 86.13 |
| RFE-XGBoost | 65.81 | 95.02 | 87.89 | 79.75 | 89.54 |
| ShapHT++DNN | 86.91 | 89.64 | 89.63 | 75.97 | 95.64 |
| ShapHT++self-AM+DNN | 88.94 | 86.13 | 88.20 | 72.32 | 96.25 |
| MEBM-SC (ShapHT++AM+DNN) | 89.27 | 90.37 | 90.87 | 81.38 | 96.58 |
| Authors | Methods | SEN [%] | SPE [%] | ACC [%] | PPV [%] | NPV [%] |
|---|---|---|---|---|---|---|
| Mruphy et al. [35] | HFOs-based contact ranking index | - | - | 70 | - | - |
| Su Liu et al. [16] | HFOs-based clinical analyses | 81 | 82.2 | - | - | - |
| Zelin Fang et al. [36] | HFOs-Based Quantity Deviation and Semi-Maximum | 60.0 | 96.3 | - | - | - |
| Jian Li et al. [14] | “fingerprint”, fast activity and SVM | 13.59 | 99.64 | 76.38 | 89.36 | 75.84 |
| Zweiphenning et al. [18] | physiological ripples correction and thresholds | 27 | 97.1 | 77.3 | 80.6 | 78.2 |
| Proposed | DL-based multi biomarkers detection and contact classification | 89.27 | 90.37 | 90.87 | 81.38 | 96.58 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Yang, Y.; Li, S.; Su, Z.; Guo, J.; Wei, P.; Huang, J.; Kang, G.; Zhao, G. Automatic Localization of Seizure Onset Zone Based on Multi-Epileptogenic Biomarkers Analysis of Single-Contact from Interictal SEEG. Bioengineering 2022, 9, 769. https://doi.org/10.3390/bioengineering9120769
Wang Y, Yang Y, Li S, Su Z, Guo J, Wei P, Huang J, Kang G, Zhao G. Automatic Localization of Seizure Onset Zone Based on Multi-Epileptogenic Biomarkers Analysis of Single-Contact from Interictal SEEG. Bioengineering. 2022; 9(12):769. https://doi.org/10.3390/bioengineering9120769
Chicago/Turabian StyleWang, Yiping, Yanfeng Yang, Si Li, Zichen Su, Jinjie Guo, Penghu Wei, Jinguo Huang, Guixia Kang, and Guoguang Zhao. 2022. "Automatic Localization of Seizure Onset Zone Based on Multi-Epileptogenic Biomarkers Analysis of Single-Contact from Interictal SEEG" Bioengineering 9, no. 12: 769. https://doi.org/10.3390/bioengineering9120769