
Personalised 3D Printed Medicines: Which Techniques and Polymers Are More Successful?

Abstract
:
1. Overview
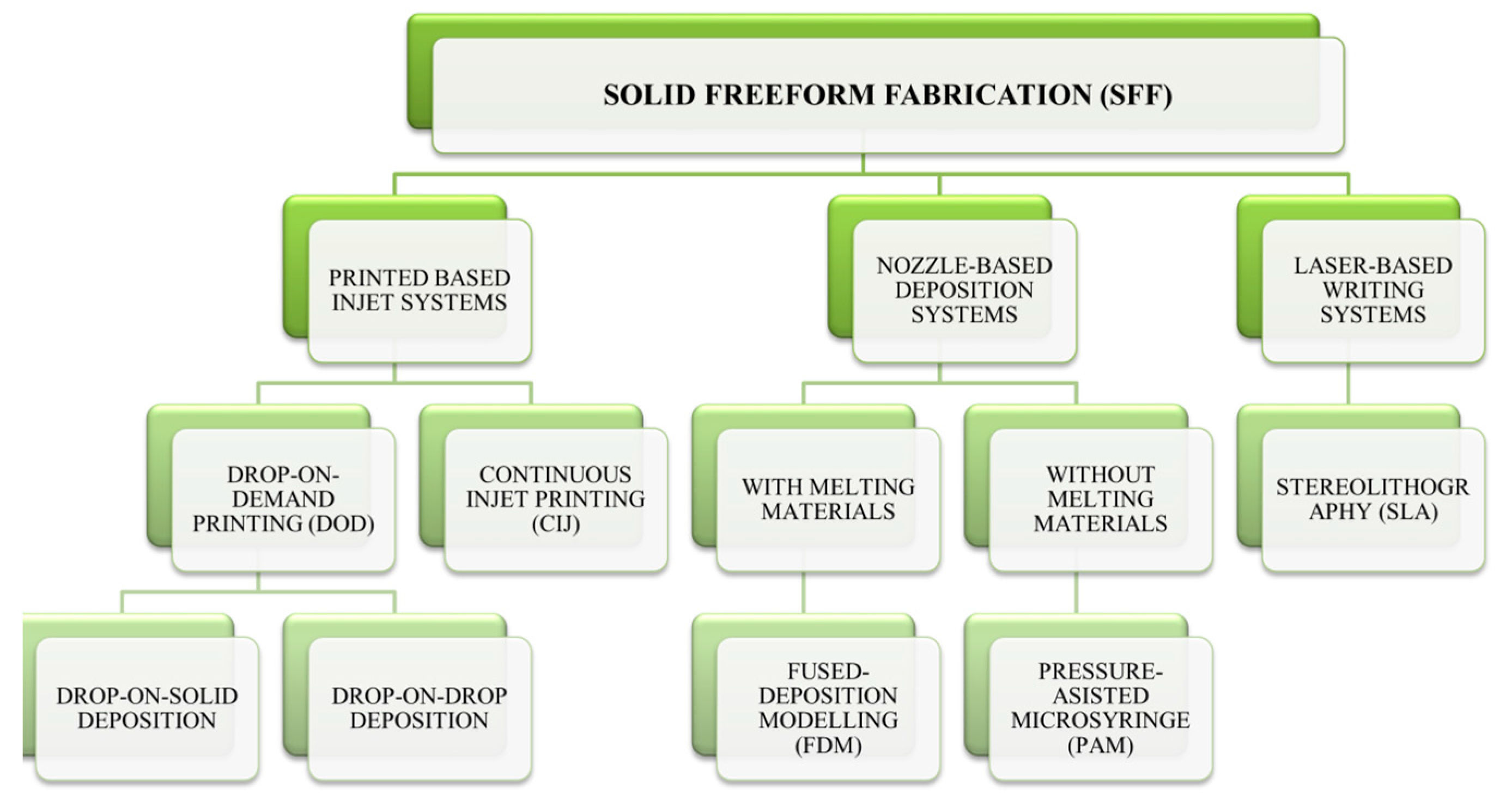
2. Current 3D Printing Techniques
2.1. Printing-Based Inkjet Systems
2.2. Nozzle-Based Deposition Systems
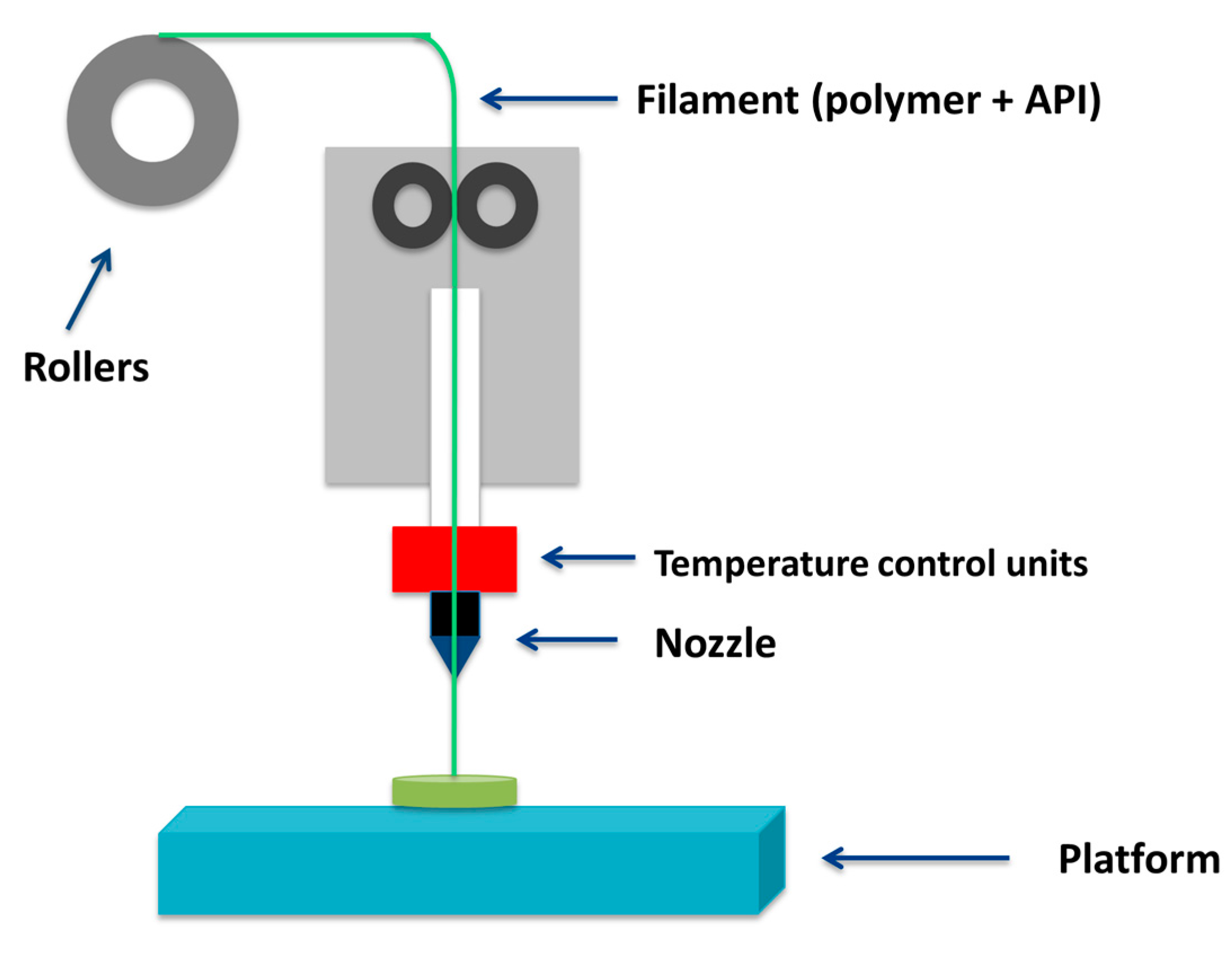
2.2.1. Fused Deposition Modelling (FDM)
2.2.2. PAM Technology
2.3. Laser-Based Writing System
3. Polymers Used in 3D Printing for Medical Purpouses
3.1. Polyvinyl Alcohol (PVA)
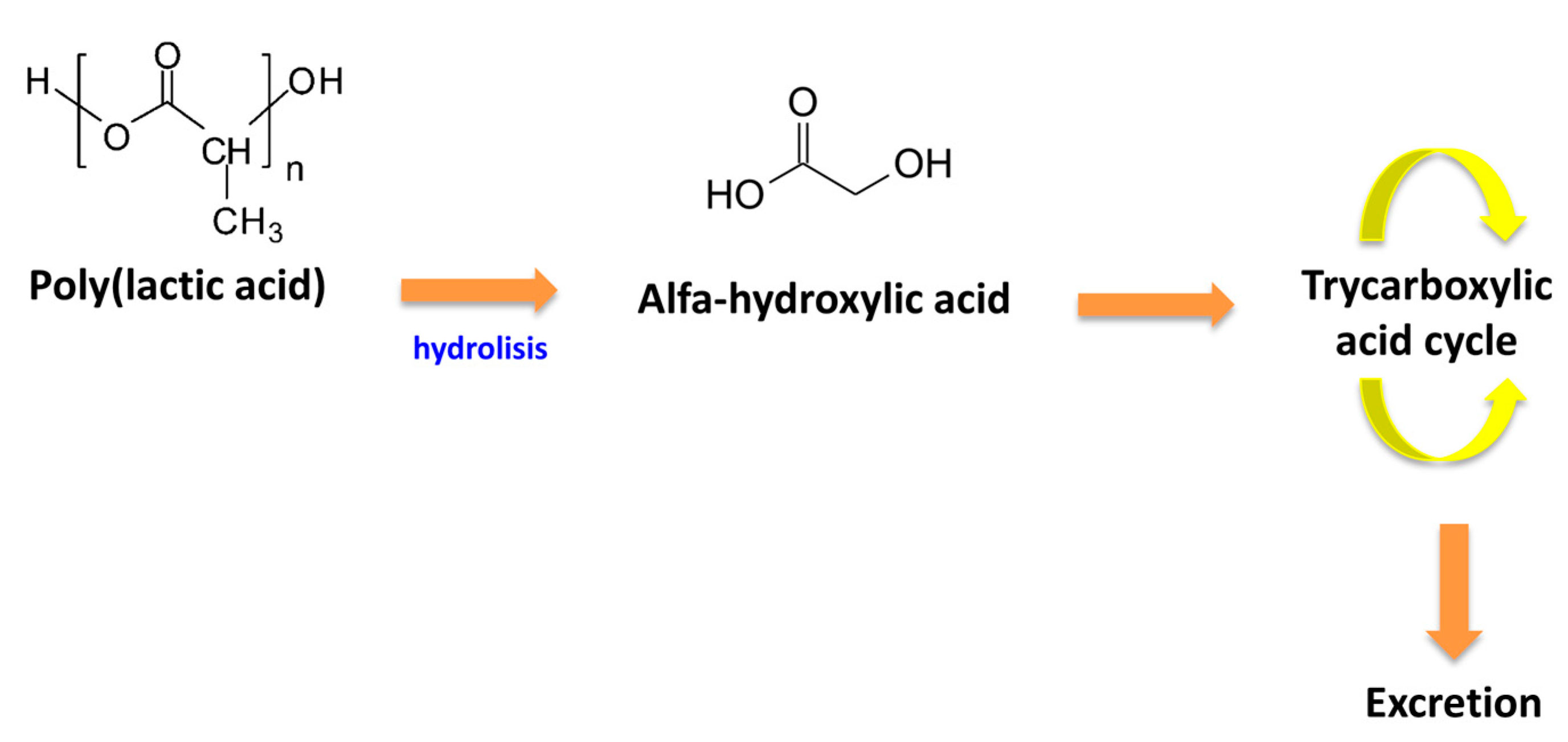
3.2. Poly(Lactic Acid) (PLA)
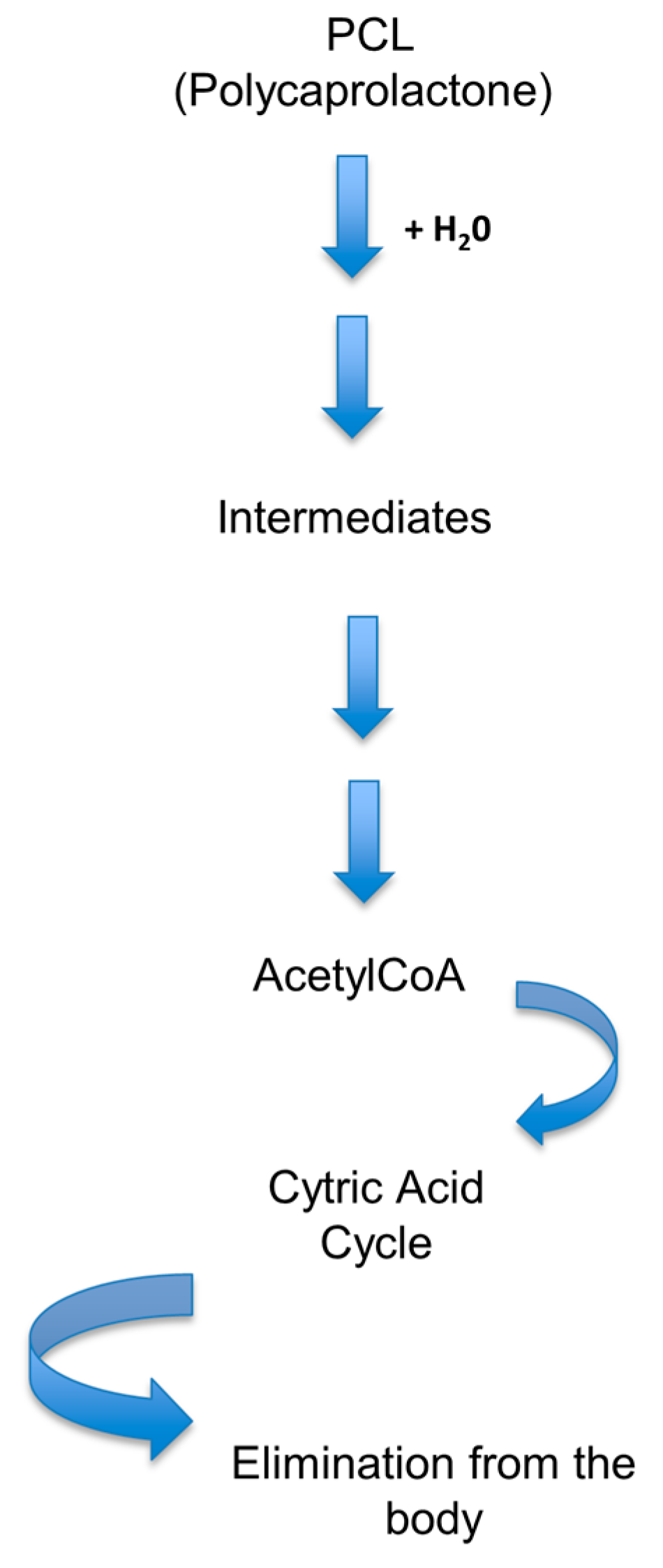
3.3. Poly(Caprolactone) (PCL)
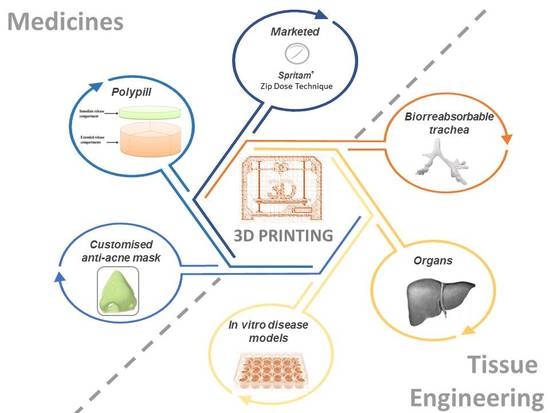
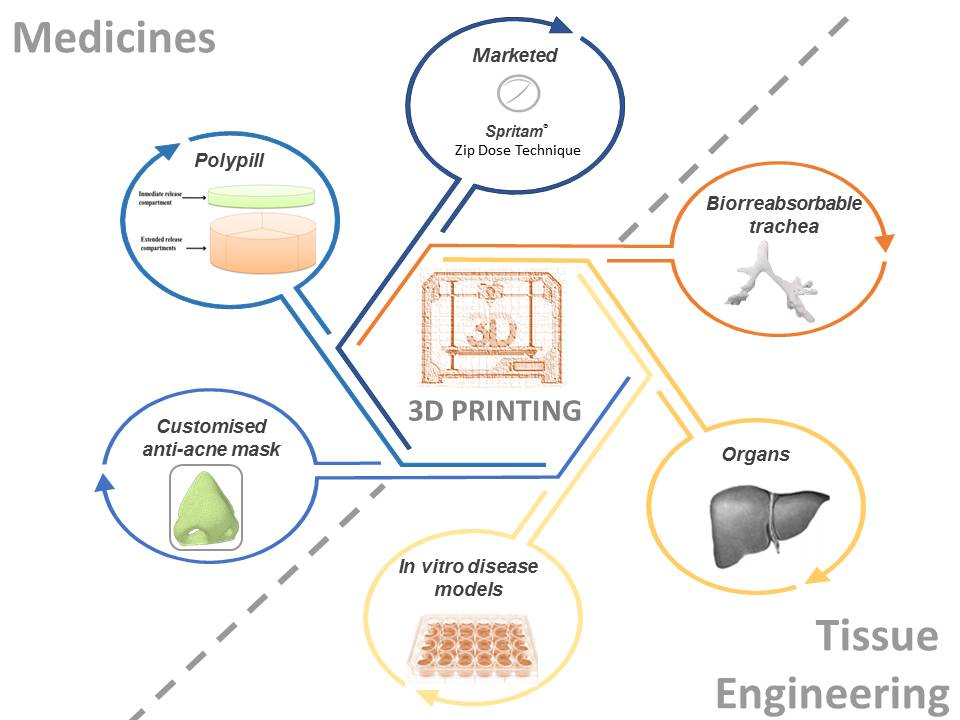
4. Applications of 3D Printed Drugs
4.1. Commercially Available 3D Printed Drugs: Spritam®
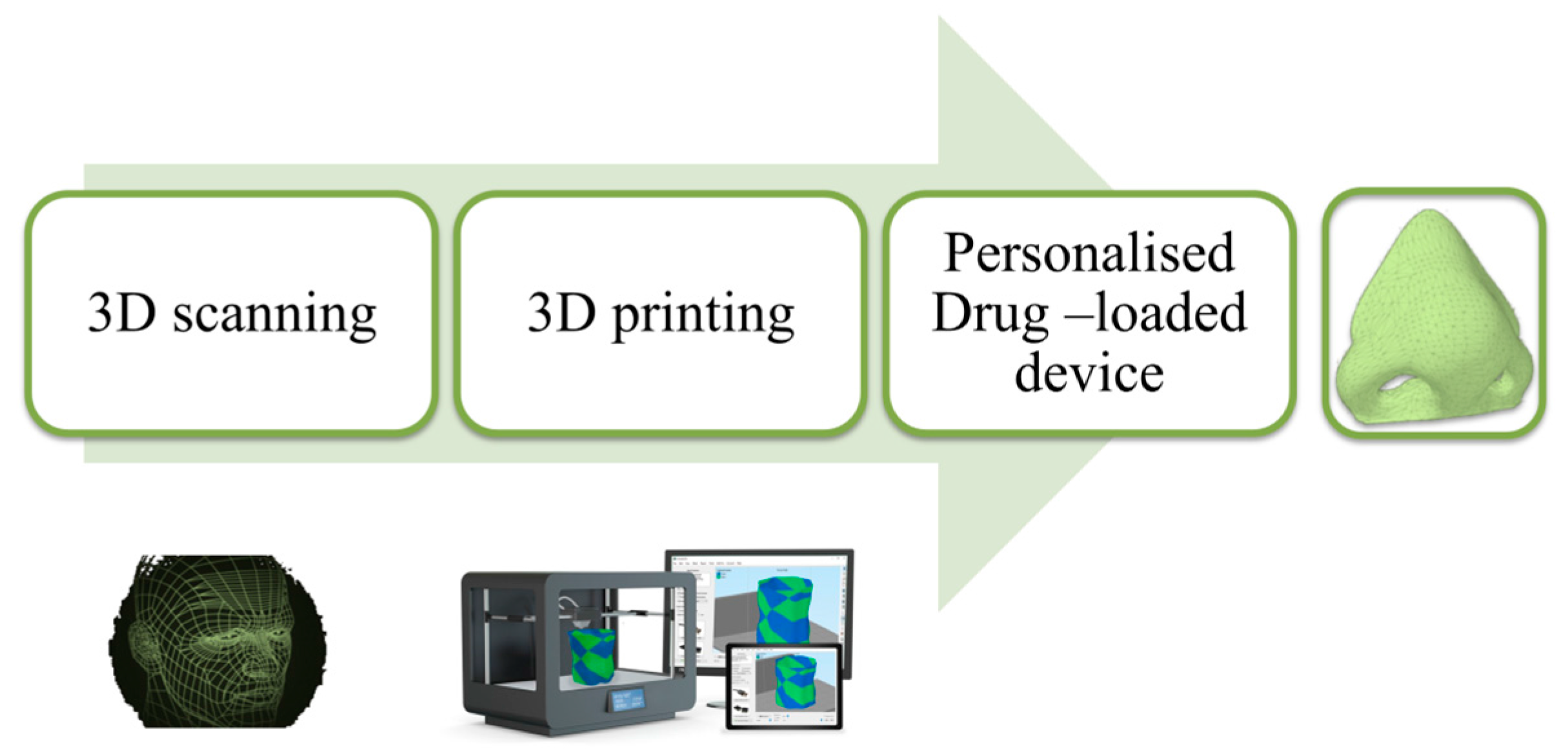
4.2. Personalized Topical Treatment Devices
4.3. 3D Printing for Cancer Treatment
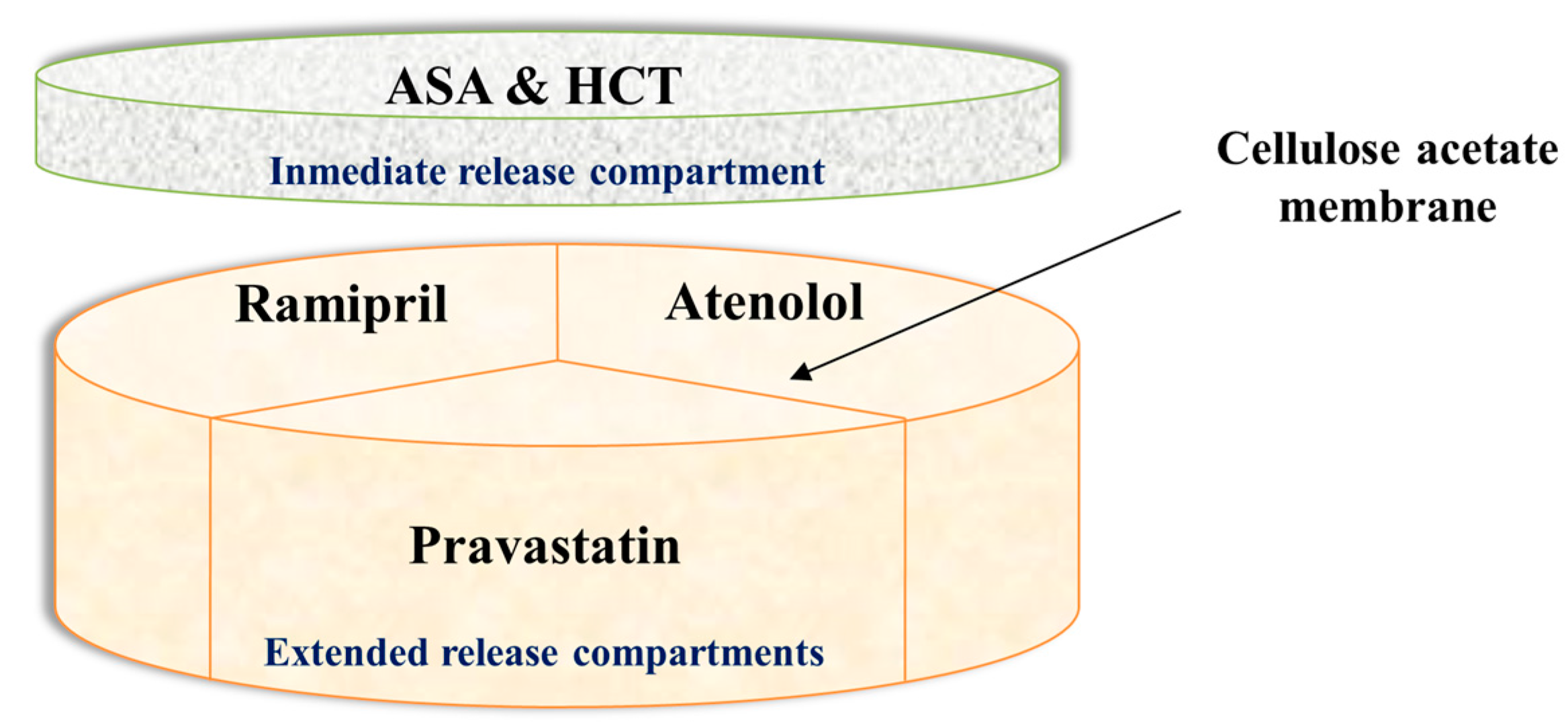
4.4. 3D Printed Polypill
4.5. Applications in Tissue Engineering
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Shastry, B.S. Pharmacogenetics and the concept of individualized medicine. Pharmacogenom. J. 2006, 6, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Preis, M.; Oblom, H. 3D-printed drugs for children—Are we ready yet? AAPS PharmSciTech 2017, 18, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Khaled, S.A.; Burley, J.C.; Alexander, M.R.; Yang, J.; Roberts, C.J. 3D printing of five-in-one dose combination polypill with defined immediate and sustained release profiles. J. Control. Release 2015, 217, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Jonathan, G.; Karim, A. 3D printing in pharmaceutics: A new tool for designing customized drug delivery systems. Int. J. Pharm. 2016, 499, 376–394. [Google Scholar]
- Wang, J.; Goyanes, A.; Gaisford, S.; Basit, A.W. Stereolithographic (SLA) 3D printing of oral modified-release dosage forms. Int. J. Pharm. 2016, 503, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Prasad, L.K.; Smyth, H. 3D printing technologies for drug delivery: A review. Drug Dev. Ind. Pharm. 2016, 42, 1019–1031. [Google Scholar] [CrossRef] [PubMed]
- Kolakovic, R.; Viitala, T.; Ihalainen, P.; Genina, N.; Peltonen, J.; Sandler, N. Printing technologies in fabrication of drug delivery systems. Expert Opin. Drug Deliv. 2013, 10, 1711–1723. [Google Scholar] [CrossRef] [PubMed]
- Acosta-Vélez, G.F.; Wu, B.M. 3D pharming: Direct printing of personalized pharmaceutical tablets. Polym. Sci. 2016. [Google Scholar] [CrossRef]
- Fina, F.; Goyanes, A.; Gaisford, S.; Basit, A.W. Selective laser sintering (SLS) 3D printing of medicines. Int. J. Pharm. 2017, 529, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Sandler, N.; Määttänen, A.; Ihalainen, P.; Kronberg, L.; Meierjohann, A.; Viitala, T.; Peltonen, J. Inkjet printing of drug substances and use of porous substrates-towards individualized dosing. J. Pharm. Sci. 2011, 100, 3386–3395. [Google Scholar] [CrossRef] [PubMed]
- Pardeike, J.; Strohmeier, D.M.; Schrödl, N.; Voura, C.; Gruber, M.; Khinast, J.G.; Zimmer, A. Nanosuspensions as advanced printing ink for accurate dosing of poorly soluble drugs in personalized medicines. Int. J. Pharm. 2011, 420, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Wonjin Jo, K.S.C.; Lee, H.J.; Myoung-Woon, M. 3D and 4D Printing Technologies: An Overview. Materials Matters. 2016. Available online: http://www.sigmaaldrich.com/technical-documents/articles/material-matters/3d-and-4d-printing-technologies.html (accessed on 20 July 2017).
- Van Wijk, A.J.M.; van Wijk, I. 3D Printing with Biomaterials: Towards a Sustainable and Circular Economy; IOS Press: Amsterdam, The Netherlands, 2015; p. 86. [Google Scholar]
- CFR-Code of Federal Regulations Title 21. Available online: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfCFR/CFRSearch.cfm?fr=178.3400 (accessed on 2 April 2017).
- Inactive Ingredients Database Download. 2017. Available online: https://www.fda.gov/drugs/informationondrugs/ucm113978.htm (accessed on 15 August 2017).
- Thakral, S.; Thakral, N.K.; Majumdar, D.K. Eudragit: A technology evaluation. Expert Opin. Drug Deliv. 2013, 10, 131–149. [Google Scholar] [CrossRef] [PubMed]
- Cleaver, G.; Agilent Technologies, Inc. Biodegradable Polymers. Available online: https://www.agilent.com/cs/library/applications/US5990-6920EN.pdf (accessed on 25 April 2017).
- Ulery, B.D.; Nair, L.S.; Laurencin, C.T. Biomedical applications of biodegradable polymers. J. Polym. Sci. Part B Polym. Phys. 2011, 49, 832–864. [Google Scholar] [CrossRef] [PubMed]
- Preis, M.; Breitkreutz, J.; Sandler, N. Perspective: Concepts of printing technologies for oral film formulations. Int. J. Pharm. 2015, 494, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Goyanes, A.; Det-Amornrat, U.; Wang, J.; Basit, A.W.; Gaisford, S. 3D scanning and 3D printing as innovative technologies for fabricating personalized topical drug delivery systems. J. Control. Release 2016, 234, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Marson, N.; Nocera, A.D.; Real, J.P.; Palma, S. Las impresoras 3D y el diseño de medicamentos. Bitácoradigital 2016, 3, 7. [Google Scholar]
- Chia, H.N.; Wu, B.M. Recent advances in 3D printing of biomaterials. J. Biol. Eng. 2015, 9, 4. [Google Scholar] [CrossRef] [PubMed]
- Ventola, C.L. Medical applications for 3D printing: Current and projected uses. Pharm. Ther. 2014, 39, 704. [Google Scholar]
- Impresión 3D por Estereolitografía, te Explicamos Todo. Available online: http://www.3dnatives.com/es/impresion-3d-por-estereolitografia-les-explicamos-todo/ (accessed on 28 January 2017).
- Boehm, R.D.; Miller, P.R.; Daniels, J.; Stafslien, S.; Narayan, R.J. Inkjet printing for pharmaceutical applications. Mater. Today 2014, 17, 247–252. [Google Scholar] [CrossRef]
- Kochhar, J.S.; Zou, S.; Chan, S.Y.; Kang, L. Protein encapsulation in polymeric microneedles by photolithography. Int. J. Nanomed. 2012, 7, 3143–3154. [Google Scholar]
- Baker, M.I.; Walsh, S.P.; Schwartz, Z.; Boyan, B.D. A review of polyvinyl alcohol and its uses in cartilage and orthopedic applications. J. Biomed. Mater. Res. Part B Appl. Biomater. 2012, 100B, 1451–1457. [Google Scholar] [CrossRef] [PubMed]
- Marin, E.; Rojas, J.; Yhors Ciro, Y. A review of polyvinil alcohol derivatives: Promising materials for pharmaceutical and biomedical applications. Afr. J. Pharm. Pharm. 2014, 8, 674–684. [Google Scholar]
- Salaoru, I.; Zhou, Z.; Morris, P.; Gibbons, G.J. Inkjet printing of polyvinyl alcohol multilayers for additive manufacturing applications. J. Appl. Polym. Sci. 2016, 133, 43572. [Google Scholar] [CrossRef]
- Goyanes, A.; Kobayashi, M.; Martínez-Pacheco, R.; Gaisford, S.; Basit, A.W. Fused-filament 3d printing of drug products: Microstructure analysis and drug release characteristics of pva-based caplets. Int. J. Pharm. 2016, 514, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Farah, S.; Anderson, G.D.; Robert Langer, R. Physical and mechanical properties of pla, and their functions in widespread applications—A comprehensive review. Adv. Drug Deliv. Rev. 2016, 107, 367–392. [Google Scholar] [CrossRef] [PubMed]
- Sin, L.T.; Rahmat, A.R.; Rahman, W.A.W.A. Degradation and stability of poly(lactic acid). In Polylactic Acid: PLA Biopolymer Tehcnology and Applications, 1st ed.; Elsevier Inc.: Oxford, UK, 2012; pp. 247–299. [Google Scholar]
- Sin, L.T.; Rahmat, A.R.; Rahman, W.A.W.A. Overview of poly(lactic Acid). In Polylactic Acid: PLA Biopolymer Tehcnology and Applications, 1st ed.; Elsevier Inc.: Oxford, UK, 2012; pp. 1–70. [Google Scholar]
- Woodruff, M.A.; Hutmacher, W.D. The return of a forgotten polymer—Polycaprolactone in the 21st Century. Prog. Polym. Sci. 2010, 35, 1217–1256. [Google Scholar] [CrossRef] [Green Version]
- Abedalwafa, M.; Wang, F.; Wang, L.; Li, C. Biodegradable poly-epsilon-caprolactone (PCL) for tissue engineering applications: A review. Rev. Adv. Mater. Sci. 2012, 34, 123–140. [Google Scholar]
- Labet, M.; Wim Thielemans, W. Synthesis of polycaprolactone: A review. Chem. Soc. Rev. 2009, 38, 3484. [Google Scholar] [CrossRef] [PubMed]
- Muwaffak, Z.; Goyanes, A.; Clark, V.; Basit, A.W.; Hilton, S.T.; Gaisford, S. Patient-specific 3D scanned and 3D printed antimicrobial polycaprolactone wound dressings. Int. J. Pharm. 2017, 527, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Beck, R.C.R.; Chaves, P.S.; Goyanez, A.; Vukosavljevic, B.; Buanz, A.; Windbergs, M.; Basit, A.W.; Gaisford, S. 3D Printed tablets loaded with polymeric nanocapsules: An innovative approach to produce customized drug delivery systems. Int. J. Pharm. 2017, 528, 268–279. [Google Scholar] [CrossRef] [PubMed]
- FDA SPRITAM (Levetiracetam) Tablets. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2015/207958Orig1s000TOC.cfm (accessed on 27 April 2017).
- Pharmaceuticals, A. 3D Printing. Available online: https://www.aprecia.com/zipdose-platform/3d-printing.php (accessed on 29 April 2017).
- Yi, H.G.; Choi, Y.J.; Kang, K.S.; Hong, J.M.; Pati, R.G.; Park, M.N.; Shim, I.K.; Lee, C.M.; Kim, S.C.; Cho, D.W. A 3D-printed local drug delivery patch for pancreatic cancer growth suppression. J. Control. Release Off. J. Control. Release Soc. 2016, 238, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Ji, S.; Guvendiren, M. Recent advances in bioink design for 3D bioprinting of tissues and organs. Front. Bioeng. Biotechnol. 2017, 5, 23. [Google Scholar] [CrossRef] [PubMed]
- Vanderburgh, J.; Sterling, J.A.; Guelcher, S.A. 3D printing of tissue engineered constructs for in vitro modeling of disease progression and drug screening. Ann. Biomed. Eng. 2017, 45, 164–179. [Google Scholar] [CrossRef] [PubMed]
- Technical Considerations for Additive Manufactured Devices. Available online: https://www.fda.gov/downloads/MedicalDevices/DeviceRegulationandGuidance/GuidanceDocuments/UCM499809.pdf (accessed on 14 September 2017).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 3D Printer | CIJ | FDM | PAM | SLA |
|---|---|---|---|---|
| Polymer | Polymer Stabilizer Liquid | Material heat-resistant as melted metals, photo-polymerizable resin and thermoplastic materials | Semi-liquid viscous material | Liquid photopolymer which rapidly solidifies with UV light, as low molecular weight polyacrylate macromers |
| Polymer Example | Tween 20 | PVA, PLA, Nylon, ABS, Polyvinyl chloride | Hydroxypropyl methylcellulose (HPMC), Polyacrylate Methocel® E5 | Epoxy Resin Acrylic resin PEGDA (liquid photosensitive resin), Propiophenone 2-hydroxy-2-methyl (initiator) |
| Drug Type | Slightly soluble in water and organic solvents | Thermorresistant molecule | Wide variety Non-specific type | Proteins and Peptides |
| Drug Example | Folic Acid | Prednisone, Theophylline, 5-ASA | Nifedipine, Glipizide | BSA (Bovine Serum Albumin) |
| Pros | Works in continuous | Lowest cost, Good mechanical resistance | Manufacture of complex drug delivery systems | Smooth surface due to the use of liquid photopolymers, Manufacture of micro-structures |
| Cons | High energy expenditure and waste generation | Low adequate thermoplastic materials., API degradation due to high temperatures | Use of organic solvents, toxicity and loss of stability | Lack of FDA-approved photosensitive polymers |
| Reference | [4,7,10,11] | [8] | [4] | [4,12] |
| Polymer | FDA Approval | Bio-Degradable Polymer | Characteristics | Technique Commonly Employed | Reference |
|---|---|---|---|---|---|
| Tween 20 (Polysorbate 20) | ✓ | ✓ | GRAS status—Good surfactant properties | CIJ | [10,11,14,15] |
| Eudragit E100 (Cationic methacrylic ester copolymer) | ✓ | ✓ | Soluble under acidic conditions (<pH 5) | Powder Bed Fusion | [4,15,16] |
| Eudragit RLPO (Copolymer of methacrylic ammonium acid) | ✓ | ✓ | Insoluble in permeable water regardless of pH | Powder Bed Fusion | [4,15,16] |
| MCC (Microcrystalline cellulose) | ✓ | ✓ | Used as a disintegrator | FDM | [15,17] |
| Polyacrylic acid (PAA) | ✓ | ✓ | Used as a hydrophilic matrix | FDM | [15,17] |
| Polyvinyl alcohol (PVA) | ✓ | ✓ | Biocompatible water-soluble synthetic polymer capable of swelling upon contact with aqueous fluids. | FDM | [4,12,15,17] |
| Polyacid-L-lactic (PLLA) | ✓ | ✓ | Biodegradable aliphatic polyester that comes from renewable resources such as corn starch, tapioca roots or sugar cane | FDM | [12,15,17,18] |
| Polyetherimide (PEI) | X | X | Remains unchanged after autoclaving | FDM | [17,19] |
| Polyphenylsulfone (PPSF) | X | X | Known as RADEL. High heat and chemical resistance. | FDM | [15,19] |
| Policaprolactone (PCL) | ✓ | ✓ | Biocompatible polyester, used in wound dressings, tissue engineering and drug administration | FDM | [15,18,20] |
| NinjaFlex® (NF) | ✓ | ✓ | Thermoplastic polyurethane widely used for regeneration, bone substitution and drug delivery | FDM | [15,20] |
| PLA flexible variety (FPLA) | ✓ | ✓ | Aliphatic polyester with adequate mechanical strength and low toxicity | FDM | [15,18,20] |
| Methocel® E5 (matrix gel) | ✓ | ✓ | Used for immediate release tablets | PAM | [4,15] |
| Hydroxypropyl Methylcellulose (HPMC) | ✓ | ✓ | Used for drug released tablets and polypills | PAM | [4,15,17] |
| Carbopol® 974P (Polymer crosslinked acrylic acid) | ✓ | ✓ | Used for sustained release purposes | PAM | [15,17] |
| Polyethylene glycol diacrylate (PEGDA) | X | ✓ | Used as liquid photopolymer | SLA | [4,15,18,20] |
| Polyethylene glycol (PEG) | ✓ | ✓ | Solidifies with the action of a laser beam | SLA | [15,17,20] |
| Tm (˚C) | Tm’ (˚C) | Tg (˚C) | Td (˚C) | Viscosity (mPa·s) | Viscosity’ (mPa·s) | LD50 (g/kg) | Drug Loading Examples (% w/w) | Reference | |
|---|---|---|---|---|---|---|---|---|---|
| PVA | 180 | 220 | 85 | 350–450 | 3.4–52 | 4.0–60 | 15–20 | 0,24; 1,9; 3,9; 8,2 | [4,27,28,30] |
| Tm (°C) | Tg (°C) | Td (°C) | Melt Viscosity (Pa·s) | Melt Viscosity’ (Pa·s) | Pd 50% Mass Loss (Months) | Pd 100% Mass Loss (Months) | Deg. Rate of Copolymer (PLA + Polyglicolide) (Months) | Process. T. (°C) | Drug Loading Examples (% w/w) | Reference | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| PLA | 150–175 | 55 | 325–500 | 1000 | 5100 | 6–12 | >36 | 5–6 | 185–190 | 0,4; 1,9 | [7,31,32,33] |
| Good Solubility | Low Solubility | Insoluble | |
|---|---|---|---|
| PVA | Water | Ethanol | Other Organic Solvents |
| PLA | Dioxane, acetonitrile, chloroform, methylene chloride, 1,1,2-trichloroethane and dichloroacetic acid | Ethyl benzene, toluene, acetone and tetrahydrofuran (when cold) | Water, methanol, ethanol, propylene glycol and unsubtituted hydrocarbons |
| PCL | Chloroform, dichloromethane, carbon tetrachloride, benzene, toluene, cyclohexanone and 2-nitropropane | Acetone, 2-butanone, ethyl acetate, dimethylformamide and acetonitrile | Alcohol, petroleum ether and diethyl ether |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Konta, A.A.; García-Piña, M.; Serrano, D.R. Personalised 3D Printed Medicines: Which Techniques and Polymers Are More Successful? Bioengineering 2017, 4, 79. https://doi.org/10.3390/bioengineering4040079
Konta AA, García-Piña M, Serrano DR. Personalised 3D Printed Medicines: Which Techniques and Polymers Are More Successful? Bioengineering. 2017; 4(4):79. https://doi.org/10.3390/bioengineering4040079
Chicago/Turabian StyleKonta, Andrea Alice, Marta García-Piña, and Dolores R. Serrano. 2017. "Personalised 3D Printed Medicines: Which Techniques and Polymers Are More Successful?" Bioengineering 4, no. 4: 79. https://doi.org/10.3390/bioengineering4040079