

A Review of Voice-Based Pain Detection in Adults Using Artificial Intelligence
 , , and
, , and
Abstract
:1. Introduction
1.1. Background
1.2. Research Question and Objectives
1.3. Methodology
1.3.1. Inclusion and Exclusion Criteria
1.3.2. Search Strategy
1.3.3. Data Extraction and Analysis
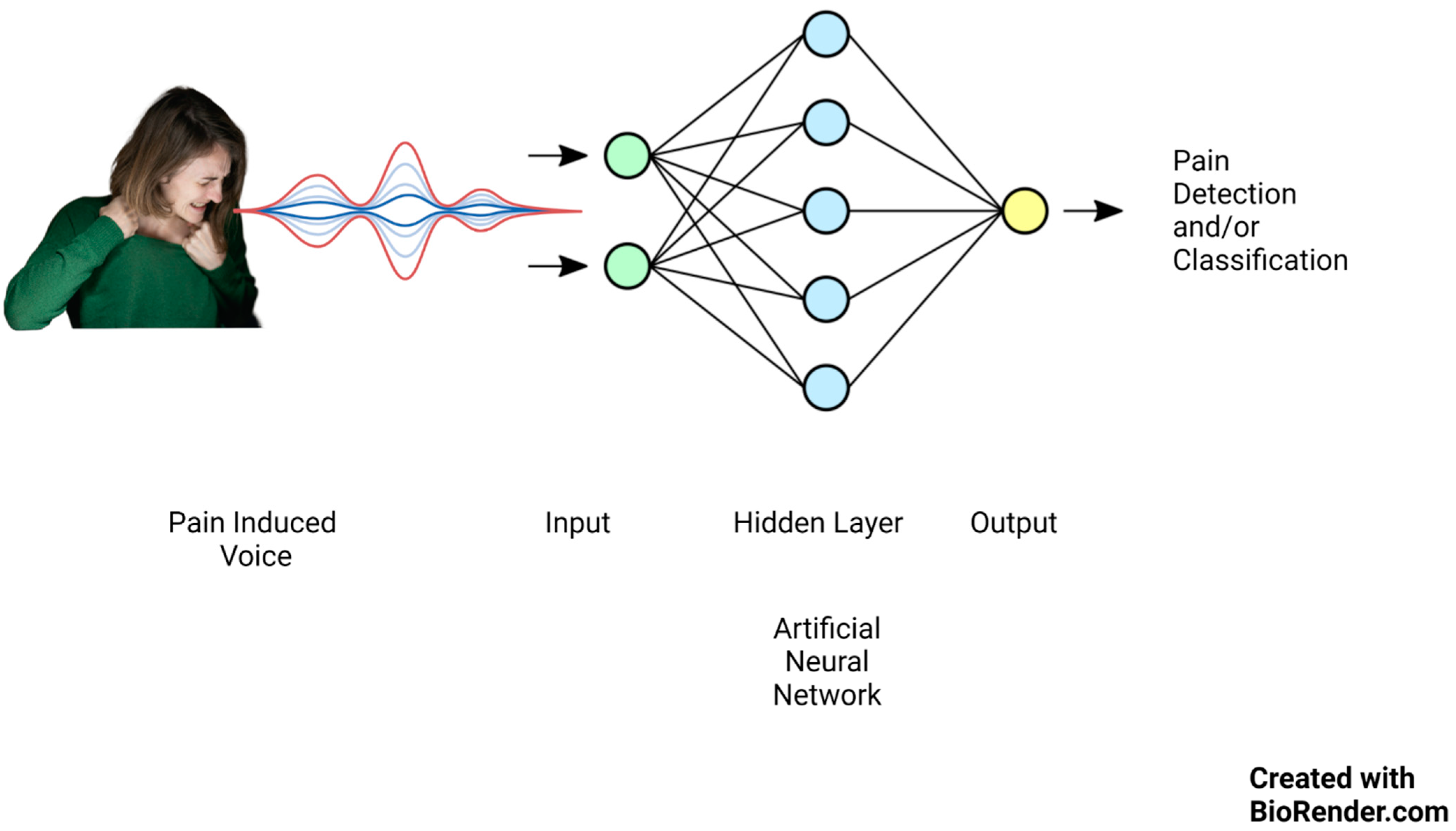
2. Voice, Pain, and Artificial Intelligence
Using Voice to Detect Pain
3. Artificial Intelligence in Pain Detection
3.1. AI Techniques Used in Pain Detection
3.2. AI Models Used in Pain Detection from Voice
- (1)
- Recurrent Artificial Neural Networks (RNNs).
- (2)
- Feed-Forward Artificial Neural Networks (FNNs).
- (3)
- Convolutional Neural Networks (CNNs): These use multiple layers to automatically learn features from the input data.
- (4)
- Long Short-Term Memory (LSTMs): It can handle vanishing and exploding gradients, which are common problems in the training of RNNs.
- (5)
- Multitask Neural Network (MT-NN): This employs the sharing of representations across associated tasks to yield a more advanced generalization model.
4. Review of the Studies
4.1. AI and Pain Triage
4.2. Pain as a Complex Affection
4.3. Can the Speech Prosody Act as a Biosignal?
4.4. Age, Gender, and Pain
5. Limitations and Challenges of AI Models in Pain Detection from Voice
6. Conclusions
6.1. Summary of Findings
6.2. Clinical Applications
6.3. Potential Areas for Future Research
6.4. Limitations
6.5. Final Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Keskinarkaus, A.; Yang, R.; Fylakis, A.; Mostafa, S.E.; Hautala, A.; Hu, Y.; Peng, J.; Zhao, G.; Seppänen, T.; Karppinen, J. Pain fingerprinting using multimodal sensing: Pilot study. Multimed. Tools Appl. 2021, 81, 5717–5742. [Google Scholar] [CrossRef]
- Tsai, F.-S.; Weng, Y.-M.; Ng, C.-J.; Lee, C.-C. Pain versus Affect? An Investigation in the Relationship between Observed Emotional States and Self-Reported Pain. In Proceedings of the 2019 Asia-Pacific Signal and Information Processing Association Annual Summit and Conference (APSIPA ASC), Lanzhou, China, 18–21 November 2019. [Google Scholar]
- Duca, L.M.; Helmick, C.G.; Barbour, K.E.; Nahin, R.L.; Von Korff, M.; Murphy, L.B.; Theis, K.; Guglielmo, D.; Dahlhamer, J.; Porter, L.; et al. A Review of Potential National Chronic Pain Surveillance Systems in the United States. J. Pain 2022, 23, 1492–1509. [Google Scholar] [CrossRef] [PubMed]
- Shu, L.; Xie, J.; Yang, M.; Li, Z.; Li, Z.; Liao, D.; Xu, X.; Yang, X. A Review of Emotion Recognition Using Physiological Signals. Sensors 2018, 18, 2074. [Google Scholar] [CrossRef] [PubMed]
- Nazari, R.; Sharif, S.P.; Allen, K.; Nia, H.S.; Yee, B.-L.; Yaghoobzadeh, A. Behavioral Pain Indicators in Patients with Traumatic Brain Injury Admitted to an Intensive Care Unit. J. Caring Sci. 2018, 7, 197. [Google Scholar] [CrossRef]
- Berger, S.E.; Baria, A.T. Assessing Pain Research: A Narrative Review of Emerging Pain Methods, Their Technosocial Implications, and Opportunities for Multidisciplinary Approaches. Front. Pain Res. 2022, 3, 896276. [Google Scholar] [CrossRef]
- Li, J.-L.; Weng, Y.-M.; Ng, C.-J.; Lee, C.-C. Learning Conditional Acoustic Latent Representation with Gender and Age Attributes for Automatic Pain Level Recognition. In Proceedings of the Interspeech 2018, Hyderabad, India, 2–6 September 2018. [Google Scholar] [CrossRef]
- Han, J.S.; Bird, G.C.; Li, W.; Jones, J.; Neugebauer, V. Computerized analysis of audible and ultrasonic vocalizations of rats as a standardized measure of pain-related behavior. J. Neurosci. Methods 2005, 141, 261–269. [Google Scholar] [CrossRef]
- Ren, Z.; Cummins, N.; Han, J.; Schnieder, S.; Krajewski, J.; Schuller, B. Evaluation of the pain level from speech: Introducing a novel pain database and benchmarks. In Proceedings of the 13th ITG-Symposium, Oldenburg, Germany, 10–12 October 2018. Speech Communication. [Google Scholar]
- Werner, P.; Lopez-Martinez, D.; Walter, S.; Al-Hamadi, A.; Gruss, S.; Picard, R.W. Automatic Recognition Methods Supporting Pain Assessment: A Survey. IEEE Trans. Affect. Comput. 2019, 13, 530–552. [Google Scholar] [CrossRef]
- Breau, L.M.; McGrath, P.; Camfield, C.; Rosmus, C.; Finley, G.A. Preliminary validation of an observational checklist for persons with cognitive impairments and inability to communicate verbally. Dev. Med. Child Neurol. 2000, 42, 609–616. [Google Scholar] [CrossRef]
- Gruss, S.; Geiger, M.; Werner, P.; Wilhelm, O.; Traue, H.C.; Al-Hamadi, A.; Walter, S. Multi-modal signals for analyzing pain responses to thermal and electrical stimuli. JoVE (J. Vis. Exp.) 2019, 146, e59057. [Google Scholar]
- Takai, Y.; Yamamoto-Mitani, N.; Ko, A.; Heilemann, M.V. Differences in Pain Measures by Mini-Mental State Examination Scores of Residents in Aged Care Facilities: Examining the Usability of the Abbey Pain Scale–Japanese Version. Pain Manag. Nurs. 2014, 15, 236–245. [Google Scholar] [CrossRef]
- Tsai, F.-S.; Weng, Y.-M.; Ng, C.-J.; Lee, C.-C. Embedding stacked bottleneck vocal features in a LSTM architecture for automatic pain level classification during emergency triage. In Proceedings of the 2017 Seventh International Conference on Affective Computing and Intelligent Interaction (ACII), San Antonio, TX, USA, 23–26 October 2017. [Google Scholar] [CrossRef]
- Helmer, L.M.; Weijenberg, R.A.; de Vries, R.; Achterberg, W.P.; Lautenbacher, S.; Sampson, E.L.; Lobbezoo, F. Crying out in pain—A systematic review into the validity of vocalization as an indicator for pain. Eur. J. Pain 2020, 24, 1703–1715. [Google Scholar] [CrossRef] [PubMed]
- Roulin, M.-J.; Ramelet, A.-S. Generating and Selecting Pain Indicators for Brain-Injured Critical Care Patients. Pain Manag. Nurs. 2015, 16, 221–232. [Google Scholar] [CrossRef]
- Manfredi, P.L.; Breuer, B.; Meier, D.E.; Libow, L. Pain Assessment in Elderly Patients with Severe Dementia. J. Pain Symptom Manag. 2003, 25, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Hong, H.-T.; Li, J.-L.; Weng, Y.-M.; Ng, C.-J.; Lee, C.-C. Investigating the Variability of Voice Quality and Pain Levels as a Function of Multiple Clinical Parameters. Age 2019, 762, 6. [Google Scholar]
- Lotan, M.; Icht, M. Diagnosing Pain in Individuals with Intellectual and Developmental Disabilities: Current State and Novel Technological Solutions. Diagnostics 2023, 13, 401. [Google Scholar] [CrossRef]
- Gkikas, S.; Tsiknakis, M. Automatic assessment of pain based on deep learning methods: A systematic review. Comput. Methods Programs Biomed. 2023, 231, 107365. [Google Scholar] [CrossRef]
- Dave, N. Feature extraction methods LPC, PLP and MFCC in speech recognition. Int. J. Adv. Res. Eng. Technol. 2013, 1, 1–4. [Google Scholar]
- Htet, Y.; Zin, T.T.; Tin, P.; Tamura, H.; Kondo, K.; Chosa, E. HMM-Based Action Recognition System for Elderly Healthcare by Colorizing Depth Map. Int. J. Environ. Res. Public Health 2022, 19, 12055. [Google Scholar] [CrossRef]
- Mahmut, E.-E.; Nicola, S.; Stoicu-Tivadar, V. Support-Vector Machine-Based Classifier of Cross-Correlated Phoneme Segments for Speech Sound Disorder Screening. Stud. Health Technol. Inform. 2022, 294, 455–459. [Google Scholar] [CrossRef]
- Liang, Y.-C.; Wijaya, I.; Yang, M.-T.; Juarez, J.R.C.; Chang, H.-T. Deep Learning for Infant Cry Recognition. Int. J. Environ. Res. Public Health 2022, 19, 6311. [Google Scholar] [CrossRef]
- Hitchcock, E.R.; Ochs, L.C.; Swartz, M.T.; Leece, M.C.; Preston, J.L.; McAllister, T. Tutorial: Using Visual–Acoustic Biofeedback for Speech Sound Training. Am. J. Speech-Lang. Pathol. 2023, 32, 18–36. [Google Scholar] [CrossRef] [PubMed]
- Icht, M.; Ressis-Tal, H.W.; Lotan, M. Can the Vocal Expression of Intellectually Disabled Individuals Be Used as a Pain Indicator? Initial Findings Supporting a Possible Novice Assessment Method. Front. Psychol. 2021, 12, 655202. [Google Scholar] [CrossRef]
- Lautenbacher, S.; Salinas-Ranneberg, M.; Niebuhr, O.; Kunz, M. Phonetic characteristics of vocalizations during pain. Pain Rep. 2017, 2, e597. [Google Scholar] [CrossRef] [PubMed]
- Raine, J.; Pisanski, K.; Simner, J.; Reby, D. Vocal communication of simulated pain. Bioacoustics 2018, 28, 404–426. [Google Scholar] [CrossRef]
- Carter, B.; McArthur, E.; Cunliffe, M. Dealing with uncertainty: Parental assessment of pain in their children with profound special needs. J. Adv. Nurs. 2002, 38, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Salinas-Ranneberg, M.; Niebuhr, O.; Kunz, M.; Lautenbacher, S.; Barbosa, P. Effects of pain on vowel production–Towards a new way of pain-level estimation based on acoustic speech-signal analyses. In Proceedings of the 43 Deutsche Jahrestagung für Akustik, Kiel, Germany, 6–9 March 2017. [Google Scholar]
- Corbett, A.; Achterberg, W.P.; Husebo, B.S.; Lobbezoo, F.; de Vet, H.; Kunz, M.; Strand, L.I.; Constantinou, M.; Tudose, C.; Kappesser, J.; et al. An international road map to improve pain assessment in people with impaired cognition: The development of the Pain Assessment in Impaired Cognition (PAIC) meta-tool. BMC Neurol. 2014, 14, 229. [Google Scholar] [CrossRef]
- Nagireddi, J.N.; Vyas, A.K.; Sanapati, M.R.; Soin, A.; Manchikanti, L. The Analysis of Pain Research through the Lens of Artificial Intelligence and Machine Learning. Pain Physician 2022, 25, e211. [Google Scholar]
- Mundial, F.E.; Schwab, K. The Fourth Industrial Revolution: What it means, how to respond. In Proceedings of the 2016 World Economic Forum, Dubai, United Arab Emirates, 11–12 November 2016. [Google Scholar]
- House of Lords Select Committee A. AI in the UK: Ready, Willing and Able; House of Lords: London, UK, 2018; p. 36. [Google Scholar]
- De Neufville, R.; Baum, S.D. Collective action on artificial intelligence: A primer and review. Technol. Soc. 2021, 66, 101649. [Google Scholar] [CrossRef]
- Cornet, G. Chapter 4. Robot companions and ethics: A pragmatic approach of ethical design. J. Int. Bioéth. 2013, 24, 49–58. [Google Scholar] [CrossRef]
- Hamet, P.; Tremblay, J. Artificial intelligence in medicine. Metabolism 2017, 69, S36–S40. [Google Scholar] [CrossRef]
- Jung, W.; Lee, K.E.; Suh, B.J.; Seok, H.; Lee, D.W. Deep learning for osteoarthritis classification in temporomandibular joint. Oral Dis. 2023, 29, 1050–1059. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; He, M.; Jiang, Z.; Wu, Z.; Dai, H.; Zhang, L.; Luo, S.; Han, T.; Li, X.; Jiang, X.; et al. Survey on natural language processing in medical image analysis. Zhong Nan Da Xue Xue Bao Yi Xue Ban 2022, 47, 981–993. [Google Scholar] [PubMed]
- Theofilatos, K.; Pavlopoulou, N.; Papasavvas, C.; Likothanassis, S.; Dimitrakopoulos, C.; Georgopoulos, E.; Moschopoulos, C.; Mavroudi, S. Predicting protein complexes from weighted protein–protein interaction graphs with a novel unsupervised methodology: Evolutionary enhanced Markov clustering. Artif. Intell. Med. 2015, 63, 181–189. [Google Scholar] [CrossRef]
- Qin, K.; Chen, W.; Cui, J.; Zeng, X.; Li, Y.; Li, Y.; You, X. The influence of time structure on prediction motion in visual and auditory modalities. Atten. Percept. Psychophys. 2022, 84, 1994–2001. [Google Scholar] [CrossRef] [PubMed]
- Thiam, P.; Kessler, V.; Amirian, M.; Bellmann, P.; Layher, G.; Zhang, Y.; Velana, M.; Gruss, S.; Walter, S.; Traue, H.C.; et al. Multi-Modal Pain Intensity Recognition Based on the SenseEmotion Database. IEEE Trans. Affect. Comput. 2019, 12, 743–760. [Google Scholar] [CrossRef]
- Walter, S.; Gruss, S.; Ehleiter, H.; Tan, J.; Traue, H.C.; Crawcour, S.; Werner, P.; Al-Hamadi, A.; Andrade, A.O. The biovid heat pain database data for the advancement and systematic validation of an automated pain recognition system. In Proceedings of the 2013 IEEE International Conference on Cybernetics (CYBCO), Lausanne, Switzerland, 13–15 June 2013. [Google Scholar] [CrossRef]
- Lucey, P.; Cohn, J.F.; Prkachin, K.M.; Solomon, P.E.; Matthews, I. Painful data: The UNBC-McMaster shoulder pain expression archive database. In Proceedings of the 2011 IEEE International Conference on Automatic Face & Gesture Recognition (FG), Santa Barbara, CA, USA, 21–23 March 2011. [Google Scholar]
- Rodriguez, P.; Cucurull, G.; Gonzalez, J.; Gonfaus, J.M.; Nasrollahi, K.; Moeslund, T.B.; Roca, F.X. Deep Pain: Exploiting Long Short-Term Memory Networks for Facial Expression Classification. IEEE Trans. Cybern. 2022, 52, 3314–3324. [Google Scholar] [CrossRef]
- Gouverneur, P.; Li, F.; Shirahama, K.; Luebke, L.; Adamczyk, W.M.; Szikszay, T.M.; Luedtke, K.; Grzegorzek, M. Explainable Artificial Intelligence (XAI) in Pain Research: Understanding the Role of Electrodermal Activity for Automated Pain Recognition. Sensors 2023, 23, 1959. [Google Scholar] [CrossRef]
- Krenker, A.; Bešter, J.; Kos, A. Introduction to the artificial neural networks. In Artificial Neural Networks: Methodological Advances and Biomedical Applications; InTech: Rijeka, Croatia, 2011; pp. 1–18. [Google Scholar]
- O’Shea, K.; Nash, R. An introduction to convolutional neural networks. arXiv 2015, arXiv:151108458. [Google Scholar]
- Tsai, S.-T.; Fields, E.; Xu, Y.; Kuo, E.-J.; Tiwary, P. Path sampling of recurrent neural networks by incorporating known physics. Nat. Commun. 2022, 13, 7231. [Google Scholar] [CrossRef]
- Mohan, H.M.; Anitha, S. Real Time Audio-Based Distress Signal Detection as Vital Signs of Myocardial Infarction Using Convolutional Neural Networks. J. Adv. Inf. Technol. 2022, 13, 106–116. [Google Scholar] [CrossRef]
- Zehetner, A.; Hagmüller, M.; Pernkopf, F. Wake-up-word spotting for mobile systems. In Proceedings of the 2014 22nd European Signal Processing Conference (EUSIPCO), Lisbon, Portugal, 1–5 September 2014. [Google Scholar]
- Hou, J.; Xie, L.; Zhang, S. Two-stage streaming keyword detection and localization with multi-scale depthwise temporal convolution. Neural Netw. 2022, 150, 28–42. [Google Scholar] [CrossRef] [PubMed]
- Qin, H.; Ma, X.; Ding, Y.; Li, X.; Zhang, Y.; Ma, Z.; Wang, J.; Luo, J.; Liu, X. BiFSMNv2: Pushing Binary Neural Networks for Keyword Spotting to Real-Network Performance. IEEE Trans. Neural Netw. Learn. Syst. 2023, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Oshrat, Y.; Bloch, A.; Lerner, A.; Cohen, A.; Avigal, M.; Zeilig, G. Speech prosody as a biosignal for physical pain detection. In Proceedings of the 8th Conference on Speech Prosody, Boston, MA, USA, 31 May–3 June 2016. [Google Scholar]
- Kinoshita, M.; Nascimento, I.J.B.D.; Styrmisdóttir, L.; Bruschettini, M. Systemic opioid regimens for postoperative pain in neonates. Cochrane Database Syst. Rev. 2023, 4, Cd015016. [Google Scholar] [CrossRef] [PubMed]
- Carroll, C.P.; Brandow, A.M. Chronic Pain: Prevalence and Management. Hematol. Oncol. Clin. N. Am. 2022, 36, 1151–1165. [Google Scholar] [CrossRef]
- Tsai, F.-S.; Hsu, Y.-L.; Chen, W.-C.; Weng, Y.-M.; Ng, C.-J.; Lee, C.-C. Toward Development and Evaluation of Pain Level-Rating Scale for Emergency Triage based on Vocal Characteristics and Facial Expressions. In Proceedings of the Interspeech 2016, San Francisco, CA, USA, 8–12 September 2016. [Google Scholar] [CrossRef]
- Lavand’homme, P.M.; Kehlet, H.; Rawal, N.; Joshi, G.P. Pain Management after Total Knee Arthroplasty: Procedure Specific Postoperative Pain Management Recommendations. Eur. J. Anaesthesiol. 2022, 39, 743–757. [Google Scholar] [CrossRef]
- Ganguly, A.; Michael, M.; Goschin, S.; Harris, K.; McFarland, D.C. Cancer Pain and Opioid Use Disorder. Oncology 2022, 36, 535–541. [Google Scholar]
- Grezl, F.; Karafiat, M.; Vesely, K. Adaptation of multilingual stacked bottle-neck neural network structure for new language. In Proceedings of the 2014 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Florence, Italy, 4–9 May 2014. [Google Scholar]
- Wu, Z.; Valentini-Botinhao, C.; Watts, O.; King, S. Deep neural networks employing multi-task learning and stacked bottleneck features for speech synthesis. In Proceedings of the 2015 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), South Brisbane, Australia, 19–24 April 2015. [Google Scholar] [CrossRef]
- Zhang, Y.; Chuangsuwanich, E.; Glass, J.R. Language ID-based training of multilingual stacked bottleneck features. In Proceedings of the Interspeech 2014, Singapore, 14–18 September 2014. [Google Scholar] [CrossRef]
- Smith, K.L.; Cameron, P.; Meyer, A.; McNeil, J.J. Knowledge of heart attack symptoms in a community survey of Victoria. Emerg. Med. Australas. 2002, 14, 255–260. [Google Scholar] [CrossRef]
- Carter, L.; McNeil, D.W.; Vowles, K.; Sorrell, J.T.; Turk, C.L.; Ries, B.J.; Hopko, D.R. Effects of Emotion on Pain Reports, Tolerance and Physiology. Pain Res. Manag. 2002, 7, 21–30. [Google Scholar] [CrossRef]
- Keefe, F.J.; Lumley, M.; Anderson, T.; Lynch, T.; Carson, K.L. Pain and emotion: New research directions. J. Clin. Psychol. 2001, 57, 587–607. [Google Scholar] [CrossRef]
- Melzack, R. Wall PD the Challenge of Pain; Basic Books: New York, NY, USA, 1982. [Google Scholar]
- Robinson, M.E.; Riley, J.L., III. The role of emotion in pain. In Psychosocial Factors in Pain: Critical Perspectives; The Guilford Press: New York, NY, USA, 1999. [Google Scholar]
- Loggia, M.L.; Juneau, M.; Bushnell, C.M. Autonomic responses to heat pain: Heart rate, skin conductance, and their relation to verbal ratings and stimulus intensity. Pain 2011, 152, 592–598. [Google Scholar] [CrossRef]
- Möltner, A.; Hölzl, R.; Strian, F. Heart rate changes as an autonomic component of the pain response. Pain 1990, 43, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Robinson, B.F. Relation of Heart Rate and Systolic Blood Pressure to the Onset of Pain in Angina Pectoris. Circulation 1967, 35, 1073–1083. [Google Scholar] [CrossRef] [PubMed]
- Storm, H. Changes in skin conductance as a tool to monitor nociceptive stimulation and pain. Curr. Opin. Anaesthesiol. 2008, 21, 796–804. [Google Scholar] [CrossRef] [PubMed]
- Ledowski, T.; Bromilow, J.; Wu, J.; Paech, M.J.; Storm, H.; Schug, S.A. The assessment of postoperative pain by monitoring skin conductance: Results of a prospective study. Anaesthesia 2007, 62, 989–993. [Google Scholar] [CrossRef]
- Rivasi, G.; Menale, S.; Turrin, G.; Coscarelli, A.; Giordano, A.; Ungar, A. The Effects of Pain and Analgesic Medications on Blood Pressure. Curr. Hypertens. Rep. 2022, 24, 385–394. [Google Scholar] [CrossRef]
- Saloni, R.; Sharma, K.; Gupta, A.K. Classification of high blood pressure persons vs. normal blood pressure persons using voice analysis. IJ Image Graph. Signal Process. 2014, 1, 47–52. [Google Scholar]
- Wandner, L.D.; Scipio, C.D.; Hirsh, A.T.; Torres, C.A.; Robinson, M.E. The Perception of Pain in Others: How Gender, Race, and Age Influence Pain Expectations. J. Pain 2012, 13, 220–227. [Google Scholar] [CrossRef]
- Unruh, A.M. Gender variations in clinical pain experience. Pain 1996, 65, 123–167. [Google Scholar] [CrossRef]
- Horgas, A.L.; Elliott, A.F. Pain assessment and management in persons with dementia. Nurs. Clin. N. Am. 2004, 39, 593–606. [Google Scholar] [CrossRef]
- Lautenbacher, S.; Kunz, M.; Strate, P.; Nielsen, J.; Arendt-Nielsen, L. Age effects on pain thresholds, temporal summation and spatial summation of heat and pressure pain. Pain 2005, 115, 410–418. [Google Scholar] [CrossRef]
- Rittger, H.; Rieber, J.; Breithardt, O.; Dücker, M.; Schmidt, M.; Abbara, S.; Sinha, A.; Jakob, A.; Nölker, G.; Brachmann, J. Influence of age on pain perception in acute myocardial ischemia: A possible cause for delayed treatment in elderly patients. Int. J. Cardiol. 2011, 149, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.E.; Dannecker, E.A.; George, S.; Otis, J.; Atchison, J.W.; Fillingim, R.B. Sex Differences in the Associations among Psychological Factors and Pain Report: A Novel Psychophysical Study of Patients with Chronic Low Back Pain. J. Pain 2005, 6, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Werner, P.; Al-Hamadi, A.; Niese, R.; Walter, S.; Gruss, S.; Traue, H.C. Automatic pain recognition from video and biomedical signals. In Proceedings of the 2014 22nd International Conference on Pattern Recognition, Stockholm, Sweden, 24–28 August 2014. [Google Scholar]
- Van Iersel, T.; Timmerman, D.; Mullie, A. Introduction of a pain scale for palliative care patients with cognitive impairment. Int. J. Palliat. Nurs. 2006, 12, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Waters, S.J.; Riordan, P.A.; Keefe, F.J.; Lefebvre, J.C. Pain Behavior in Rheumatoid Arthritis Patients: Identification of Pain Behavior Subgroups. J. Pain Symptom Manag. 2008, 36, 69–78. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Subjects | Modality Type | Speech Parameterization Method | AI/ML Type | Model Validation Method | Pain Characteristics | Metric Score |
|---|---|---|---|---|---|---|---|
| Oshrat et al., 2016 [54] | Patients with spinal cord and/or brain injuries 27 cases (20 male, 7 female) 400 sound files | Audio | OpenSMILE toolkit RASTA-PLP MFCC logMelFreqBand lspFreq | CFS SMO on SVM | Cross-validation and five folds | Not significant (pain levels ≤ 2) Significant (pain levels ≥ 2.5) | CCI ratio 73.75% OpenSMILE 77.25% OpenSMILE+ new features Kappa 39.81% First Group 46.97% Second Group |
| Tsai et al., 2016 [57] | On-boarding emergency patients 117 cases (205 sound files) | Audio–video Physiological (HR, SBP, DBP) vital sign data Other physiologically relevant results (analgesic prescription and patient disposition) | LLD | 2-Class SVM 3-Class SVM Linear regression model (supervised) | Leave one patient out Cross-validation | Binary and tertiary pain severity classification | Accuracy 72.3% Binary Classification 51.6% Ternary Classification |
| Tsai et al., 2017 [14] | On-boarding emergency patients 63 cases (126 sound files) | Audio–video Physiological (HR, SBP, DBP) vital sign data Other physiologically relevant results | LLD | LSTMs with stacked bottlenecks | Leave one patient out Cross-validation | Binary and tertiary pain severity classification | Accuracy 72.3% Binary Classification 54.2% Tertiary Classification |
| Li et al., 2018 [7] | On-boarding emergency patients 141 cases 335 sound files (201 male, 134 female) | Audio–video | LLD (MFCC) | MMD-CVAE (unsupervised) linear-kernel SVM | Leave one speaker out Cross-validation | Binary and tertiary pain severity classification | UAR 70.7% Binary Classification 47.4% Tertiary Classification |
| Tsai et al., 2019 [2] | On-boarding emergency patients 184 cases (323 sound files) | Audio–video Physiological (HR, SBP, DBP) vital sign data other physiologically relevant results | OpenSMILE toolkit LLD | EEMN | Leave one patient out Cross-validation | Binary and tertiary pain severity classification | UAR 70.1% Multimodal Binary 52.1% Multimodal Tertiary |
| Mohan et al., 2022 [50] | Healthy adults 60 cases (360 sound files) | Audio | LLD (MFCC) | CNN | N/A | Pain Detection | TP 89% to 100% 97.91% Overall Accuracy |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borna, S.; Haider, C.R.; Maita, K.C.; Torres, R.A.; Avila, F.R.; Garcia, J.P.; De Sario Velasquez, G.D.; McLeod, C.J.; Bruce, C.J.; Carter, R.E.; et al. A Review of Voice-Based Pain Detection in Adults Using Artificial Intelligence. Bioengineering 2023, 10, 500. https://doi.org/10.3390/bioengineering10040500
Borna S, Haider CR, Maita KC, Torres RA, Avila FR, Garcia JP, De Sario Velasquez GD, McLeod CJ, Bruce CJ, Carter RE, et al. A Review of Voice-Based Pain Detection in Adults Using Artificial Intelligence. Bioengineering. 2023; 10(4):500. https://doi.org/10.3390/bioengineering10040500
Chicago/Turabian StyleBorna, Sahar, Clifton R. Haider, Karla C. Maita, Ricardo A. Torres, Francisco R. Avila, John P. Garcia, Gioacchino D. De Sario Velasquez, Christopher J. McLeod, Charles J. Bruce, Rickey E. Carter, and et al. 2023. "A Review of Voice-Based Pain Detection in Adults Using Artificial Intelligence" Bioengineering 10, no. 4: 500. https://doi.org/10.3390/bioengineering10040500