
Density Spectral Array Enables Precise Sedation Control for Supermicrosurgical Lymphaticovenous Anastomosis: A Retrospective Observational Cohort Study

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
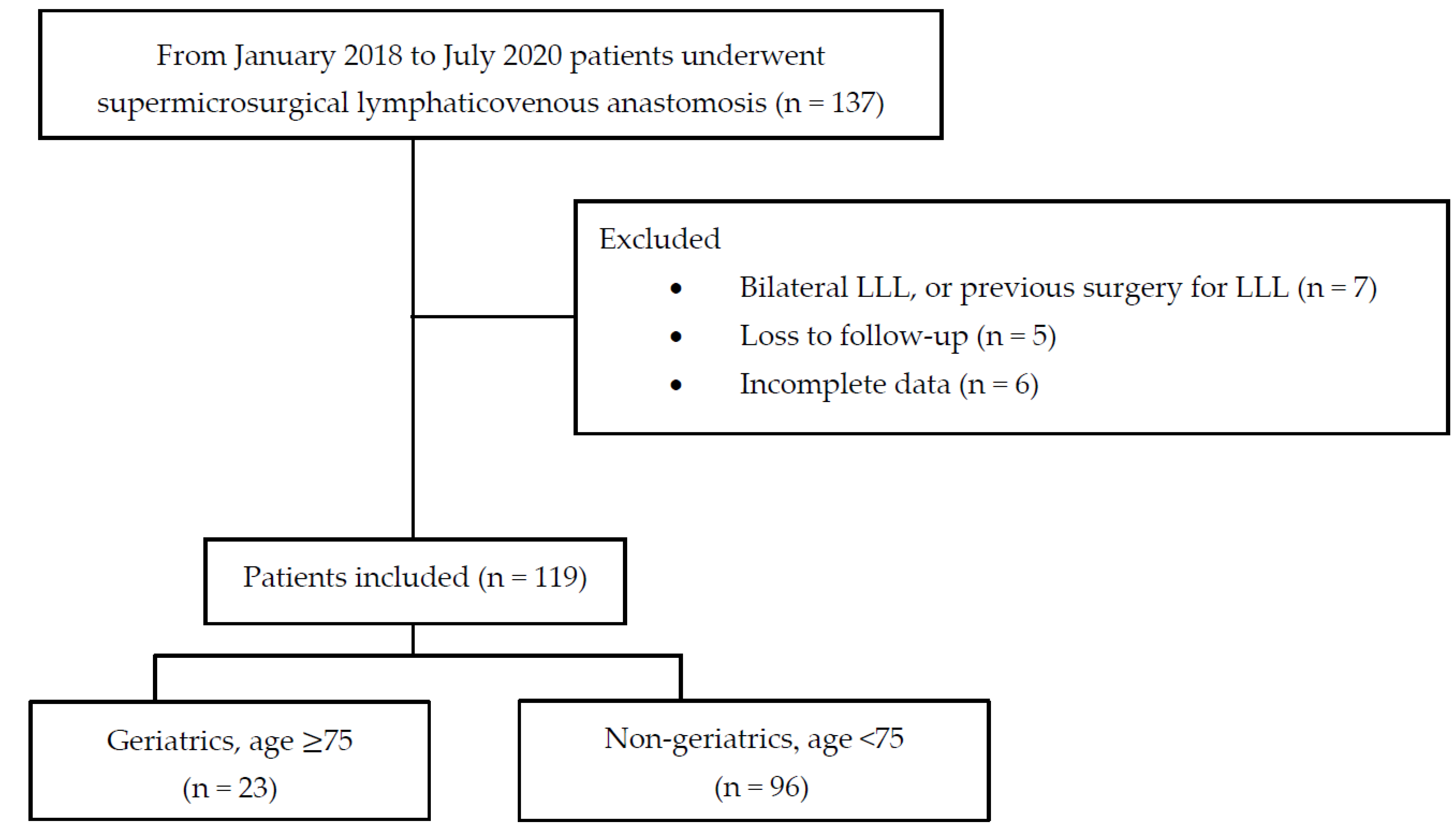
2.1. Patients
2.2. Evaluation of Lymphedema
2.3. Intraoperative and Postoperative Management
2.4. MR Volumetry for Lower Extremities
2.5. Anesthetic Management
2.6. Primary and Secondary Outcomes
2.7. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Intraoperative Findings
3.3. Surgical Outcomes
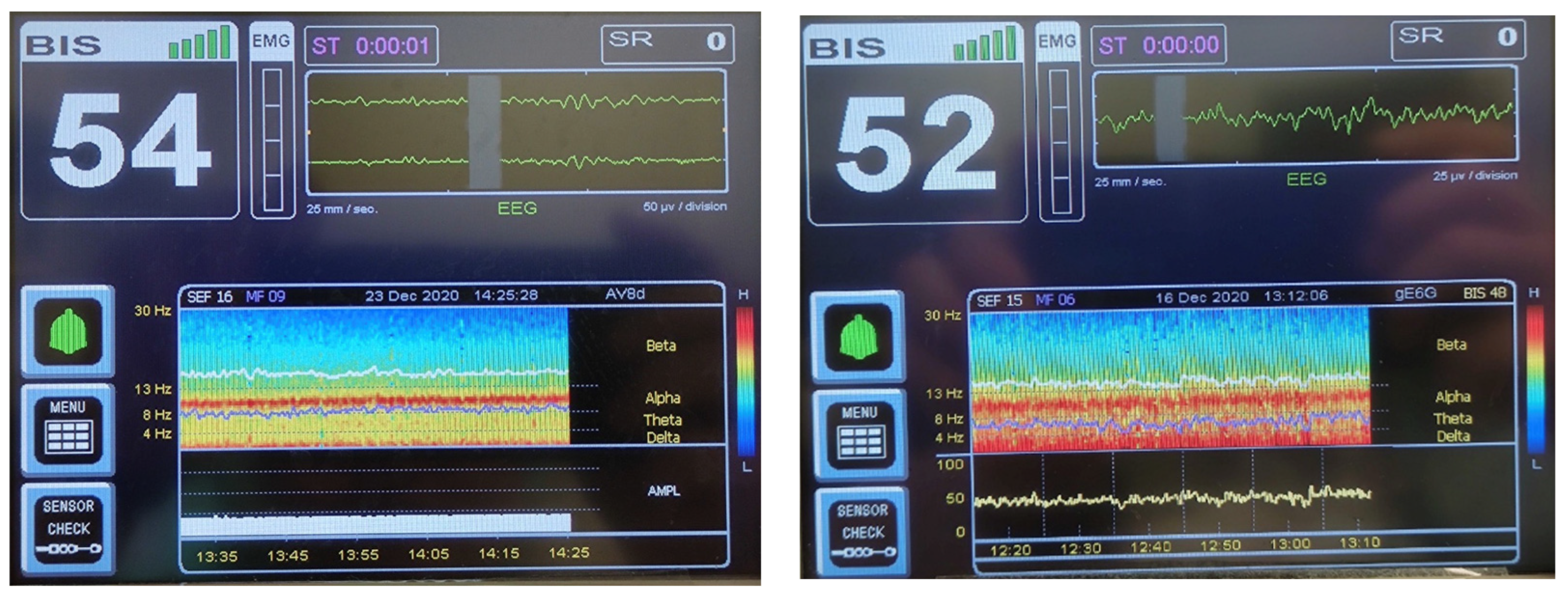
3.4. BIS-Guided Non-Intubated Anesthesia
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Ageing and health. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 1 October 2022).
- Orimo, H. Reviewing the definition of elderly. Nihon Ronen Igakkai Zasshi 2006, 43, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, Y.; Hamatani, Y.; Esato, M.; Chun, Y.H.; Tsuji, H.; Wada, H.; Hasegawa, K.; Abe, M.; Lip, G.Y.H.; Akao, M. Clinical characteristics and outcomes in extreme elderly (age >/= 85 years) Japanese patients with atrial fibrillation: The Fushimi AF registry. Chest 2016, 149, 401–412. [Google Scholar] [CrossRef] [PubMed]
- Becker, D.; Ryemon, S.; Gross, J.; Levy, B.; Grossbard, M.; Ennis, R. Cancer trends among the extreme elderly in the era of cancer screening. J. Geriatr. Oncol. 2014, 5, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Pigott, A.; Obermair, A.; Janda, M.; Vagenas, D.; Ward, L.C.; Reul-Hirche, H.; Hayes, S.C. Incidence and risk factors for lower limb lymphedema associated with endometrial cancer: Results from a prospective, longitudinal cohort study. Gynecol. Oncol. 2020, 158, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Deura, I.; Shimada, M.; Hirashita, K.; Sugimura, M.; Sato, S.; Sato, S.; Oishi, T.; Itamochi, H.; Harada, T.; Kigawa, J. Incidence and risk factors for lower limb lymphedema after gynecologic cancer surgery with initiation of periodic complex decongestive physiotherapy. Int. J. Clin. Oncol. 2015, 20, 556–560. [Google Scholar] [CrossRef]
- Kuroda, K.; Yamamoto, Y.; Yanagisawa, M.; Kawata, A.; Akiba, N.; Suzuki, K.; Naritaka, K. Risk factors and a prediction model for lower limb lymphedema following lymphadenectomy in gynecologic cancer: A hospital-based retrospective cohort study. BMC Womens Health 2017, 17, 50. [Google Scholar] [CrossRef]
- Bona, A.F.; Ferreira, K.R.; Carvalho, R.B.M.; Thuler, L.C.S.; Bergmann, A. Incidence, prevalence, and factors associated with lymphedema after treatment for cervical cancer: A systematic review. Int. J. Gynecol. Cancer 2020, 30, 1697–1704. [Google Scholar] [CrossRef]
- Hayes, S.C.; Janda, M.; Ward, L.C.; Reul-Hirche, H.; Steele, M.L.; Carter, J.; Quinn, M.; Cornish, B.; Obermair, A. Lymphedema following gynecological cancer: Results from a prospective, longitudinal cohort study on prevalence, incidence and risk factors. Gynecol. Oncol. 2017, 146, 623–629. [Google Scholar] [CrossRef]
- Huang, J.; Yu, N.; Wang, X.; Long, X. Incidence of lower limb lymphedema after vulvar cancer: A systematic review and meta-analysis. Medicine 2017, 96, e8722. [Google Scholar] [CrossRef]
- Balci, F.L.; DeGore, L.; Soran, A. Breast cancer–related lymphedema in elderly patients. Top Geriatr. Rehabil. 2012, 28, 243–253. [Google Scholar] [CrossRef]
- Yang, J.C.; Wu, S.C.; Lin, W.C.; Chiang, M.H.; Chiang, P.L.; Hsieh, C.H. Supermicrosurgical lymphaticovenous anastomosis as alternative treatment option for moderate-to-severe lower limb lymphedema. J. Am. Coll. Surg. 2020, 230, 216–227. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.C.; Wu, S.C.; Chiang, M.H.; Lin, W.C.; Hsieh, C.H. Intraoperative identification and definition of “functional” lymphatic collecting vessels for supermicrosurgical lymphatico-venous anastomosis in treating lymphedema patients. J. Surg. Oncol. 2018, 117, 994–1000. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.C.; Yen, Y.H.; Wu, S.C.; Lin, W.C.; Chiang, M.H.; Hsieh, C.H. Supermicrosurgical lymphaticovenous anastomosis as an alternative treatment option for patients with lymphorrhea. Plast. Reconstr. Surg. 2019, 144, 1214–1224. [Google Scholar] [CrossRef] [PubMed]
- Koshima, I.; Nanba, Y.; Tsutsui, T.; Takahashi, Y.; Itoh, S. Long-term follow-up after lymphaticovenular anastomosis for lymphedema in the leg. J. Reconstr. Microsurg. 2003, 19, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Koshima, I.; Nanba, Y.; Tsutsui, T.; Takahashi, Y.; Itoh, S.; Fujitsu, M. Minimal invasive lymphaticovenular anastomosis under local anesthesia for leg lymphedema: Is it effective for stage III and IV? Ann. Plast. Surg. 2004, 53, 261–266. [Google Scholar] [CrossRef]
- Yamamoto, T.; Yamamoto, N.; Yoshimatsu, H.; Narushima, M.; Koshima, I. Factors associated with lymphosclerosis: An analysis on 962 lymphatic vessels. Plast. Reconstr. Surg. 2017, 140, 734–741. [Google Scholar] [CrossRef]
- Cha, H.G.; Oh, T.M.; Cho, M.J.; Pak, C.S.J.; Suh, H.P.; Jeon, J.Y.; Hong, J.P. Changing the paradigm: Lymphovenous anastomosis in advanced stage lower extremity lymphedema. Plast. Reconstr. Surg. 2021, 147, 199–207. [Google Scholar] [CrossRef]
- Hara, H.; Mihara, M. Lymphaticovenous anastomosis for advanced-stage lower limb lymphedema. Microsurgery 2021, 41, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Fogarty, B.J.; Khan, K.; Ashall, G.; Leonard, A.G. Complications of long operations: A prospective study of morbidity associated with prolonged operative time (>6 h). Br. J. Plast. Surg. 1999, 52, 33–36. [Google Scholar] [CrossRef]
- Sieber, F.E. Postoperative delirium in the elderly surgical patient. Anesthesiol. Clin. 2009, 27, 451–464. [Google Scholar] [CrossRef]
- Raats, J.W.; van Eijsden, W.A.; Crolla, R.M.; Steyerberg, E.W.; van der Laan, L. Risk factors and outcomes for postoperative delirium after major surgery in elderly patients. PLoS ONE 2015, 10, e0136071. [Google Scholar] [CrossRef] [PubMed]
- Daiello, L.A.; Racine, A.M.; Yun Gou, R.; Marcantonio, E.R.; Xie, Z.; Kunze, L.J.; Vlassakov, K.V.; Inouye, S.K.; Jones, R.N.; Alsop, D.; et al. Postoperative delirium and postoperative cognitive dysfunction: Overlap and divergence. Anesthesiology 2019, 131, 477–491. [Google Scholar] [CrossRef] [PubMed]
- Schenning, K.J.; Deiner, S.G. Postoperative delirium in the geriatric patient. Anesthesiol. Clin. 2015, 33, 505–516. [Google Scholar] [CrossRef]
- Chiang, M.H.; Wu, S.C.; Hsu, S.W.; Chin, J.C. Bispectral Index and non-bispectral Index anesthetic protocols on postoperative recovery outcomes. Minerva Anestesiol. 2018, 84, 216–228. [Google Scholar] [CrossRef] [PubMed]
- Bocskai, T.; Kovács, M.; Szakács, Z.; Gede, N.; Hegyi, P.; Varga, G.; Pap, I.; Tóth, I.; Révész, P.; Szanyi, I.; et al. Is the bispectral index monitoring protective against postoperative cognitive decline? A systematic review with meta-analysis. PLoS ONE 2020, 15, e0229018. [Google Scholar] [CrossRef] [PubMed]
- Nunes, R.R.; Chaves, I.M.; de Alencar, J.C.; Franco, S.B.; de Oliveira, Y.G.; de Menezes, D.G. Bispectral index and other processed parameters of electroencephalogram: An update. Rev. Bras. Anestesiol. 2012, 62, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Dahaba, A.A.; Bornemann, H.; Hopfgartner, E.; Ohran, M.; Kocher, K.; Liebmann, M.; Wilfinger, G.; Metzler, H. Effect of sugammadex or neostigmine neuromuscular block reversal on bispectral index monitoring of propofol/remifentanil anaesthesia. Br. J. Anaesth. 2012, 108, 602–606. [Google Scholar] [CrossRef]
- Bouillon, T.W.; Bruhn, J.; Radulescu, L.; Andresen, C.; Shafer, T.J.; Cohane, C.; Shafer, S.L. Pharmacodynamic interaction between propofol and remifentanil regarding hypnosis, tolerance of laryngoscopy, bispectral index, and electroencephalographic approximate entropy. Anesthesiology 2004, 100, 1353–1372. [Google Scholar] [CrossRef]
- Guignard, B.; Menigaux, C.; Dupont, X.; Fletcher, D.; Chauvin, M. The effect of remifentanil on the bispectral index change and hemodynamic responses after orotracheal intubation. Anesth. Analg. 2000, 90, 161–167. [Google Scholar] [CrossRef]
- Schnider, T.W.; Minto, C.F.; Gambus, P.L.; Andresen, C.; Goodale, D.B.; Shafer, S.L.; Youngs, E.J. The influence of method of administration and covariates on the pharmacokinetics of propofol in adult volunteers. Anesthesiology 1998, 88, 1170–1182. [Google Scholar] [CrossRef]
- Scott, J.C.; Ponganis, K.V.; Stanski, D.R. EEG quantitation of narcotic effect: The comparative pharmacodynamics of fentanyl and alfentanil. Anesthesiology 1985, 62, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Schnider, T.W.; Minto, C.F.; Shafer, S.L.; Gambus, P.L.; Andresen, C.; Goodale, D.B.; Youngs, E.J. The influence of age on propofol pharmacodynamics. Anesthesiology 1999, 90, 1502–1516. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, R.; Beech, F.; Brown, A.; Dhesi, J.; Foo, I.; Goodall, J.; Harrop-Griffiths, W.; Jameson, J.; Love, N.; Pappenheim, K.; et al. Peri-operative care of the elderly 2014: Association of Anaesthetists of Great Britain and Ireland. Anaesthesia 2014, 69 (Suppl. S1), 81–98. [Google Scholar] [CrossRef] [PubMed]
- Checketts, M.R.; Alladi, R.; Ferguson, K.; Gemmell, L.; Handy, J.M.; Klein, A.A.; Love, N.J.; Misra, U.; Morris, C.; Nathanson, M.H.; et al. Recommendations for standards of monitoring during anaesthesia and recovery 2015: Association of Anaesthetists of Great Britain and Ireland. Anaesthesia 2016, 71, 85–93. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [PubMed]
- Executive Committee of the International Society of Lymphology. The diagnosis and treatment of peripheral lymphedema: 2020 Consensus Document of the International Society of Lymphology. Lymphology 2020, 53, 3–19. [Google Scholar]
- MacKenzie, K.K.; Britt-Spells, A.M.; Sands, L.P.; Leung, J.M. Processed electroencephalogram monitoring and postoperative delirium. Anesthesiology 2018, 129, 417–427. [Google Scholar] [CrossRef]
- Mihara, M.; Hara, H.; Hayashi, Y.; Narushima, M.; Yamamoto, T.; Todokoro, T.; Iida, T.; Sawamoto, N.; Araki, J.; Kikuchi, K.; et al. Pathological steps of cancer-related lymphedema: Histological changes in the collecting lymphatic vessels after lymphadenectomy. PLoS ONE 2012, 7, e41126. [Google Scholar] [CrossRef]
- Kortelainen, J.; Koskinen, M.; Mustola, S.; Seppänen, T. Effects of remifentanil on the spectrum and quantitative parameters of electroencephalogram in propofol anesthesia. Anesthesiology 2009, 111, 574–583. [Google Scholar] [CrossRef]
- Li, X.; Gichin, C.; Xiang, S.; Zhou, L.; Chang, L. Non-intubated general anesthesia based on Bi-spectral index monitoring: Case reports of 2 patients undergoing endo-bronchial ultrasound guided trans-bronchial needle aspiration. Medicine 2020, 99, e22458. [Google Scholar] [CrossRef]
- Gonzalez-Rivas, D.; Bonome, C.; Fieira, E.; Aymerich, H.; Fernandez, R.; Delgado, M.; Mendez, L.; de la Torre, M. Non-intubated video-assisted thoracoscopic lung resections: The future of thoracic surgery? Eur. J. Cardiothorac. Surg. 2016, 49, 721–731. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.G.; Jing, R.; Mo, Y.J.; Lin, F.; Du, X.K.; Ge, W.Y.; Dai, H.J.; Hu, Z.K.; Zhang, S.S.; Pan, L.H. Non-intubated anesthesia in patients undergoing video-assisted thoracoscopic surgery: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0224737. [Google Scholar] [CrossRef] [PubMed]
- Wen, Y.; Liang, H.; Qiu, G.; Liu, Z.; Liu, J.; Ying, W.; Liang, W.; He, J. Non-intubated spontaneous ventilation in video-assisted thoracoscopic surgery: A meta-analysis. Eur. J. Cardiothorac. Surg. 2020, 57, 428–437. [Google Scholar] [CrossRef] [PubMed]
- Kiss, G.; Castillo, M. Nonintubated anesthesia in thoracic surgery: General issues. Ann. Transl. Med. 2015, 3, 110. [Google Scholar] [CrossRef]
- Zhu, T.; Pang, Q.; McCluskey, S.A.; Luo, C. Effect of propofol on hepatic blood flow and oxygen balance in rabbits. Can. J. Anaesth. 2008, 55, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Shafer, S.L. The pharmacology of anesthetic drugs in elderly patients. Anesthesiol. Clin. N. Am. 2000, 18, 1–29. [Google Scholar] [CrossRef]
- Short, T.G.; Plummer, J.L.; Chui, P.T. Hypnotic and anaesthetic interactions between midazolam, propofol and alfentanil. Br. J. Anaesth. 1992, 69, 162–167. [Google Scholar] [CrossRef]
- Luo, C.; Zou, W. Cerebral monitoring of anaesthesia on reducing cognitive dysfunction and postoperative delirium: A systematic review. J. Int. Med. Res. 2018, 46, 4100–4110. [Google Scholar] [CrossRef]
- Hesse, S.; Kreuzer, M.; Hight, D.; Gaskell, A.; Devari, P.; Singh, D.; Taylor, N.B.; Whalin, M.K.; Lee, S.; Sleigh, J.W.; et al. Association of electroencephalogram trajectories during emergence from anaesthesia with delirium in the postanaesthesia care unit: An early sign of postoperative complications. Br. J. Anaesth. 2019, 122, 622–634. [Google Scholar] [CrossRef]
- Klimesch, W. EEG-alpha rhythms and memory processes. Int. J. Psychophysiol. 1997, 26, 319–340. [Google Scholar] [CrossRef]
- Purdon, P.L.; Pavone, K.J.; Akeju, O.; Smith, A.C.; Sampson, A.L.; Lee, J.; Zhou, D.W.; Solt, K.; Brown, E.N. The Ageing Brain: Age-dependent changes in the electroencephalogram during propofol and sevoflurane general anaesthesia. Br. J. Anaesth. 2015, 115 (Suppl. 1), i46–i57. [Google Scholar] [CrossRef] [PubMed]
- Hight, D.F.; Gaskell, A.L.; Kreuzer, M.; Voss, L.J.; García, P.S.; Sleigh, J.W. Transient electroencephalographic alpha power loss during maintenance of general anaesthesia. Br. J. Anaesth. 2019, 122, 635–642. [Google Scholar] [CrossRef] [PubMed]
- Pawar, N.; Chang, B.; Burst, O.L. Burst Suppression during General Anesthesia and postoperative outcomes: Mini review. Front. Syst. Neurosci. 2021, 15, 767489. [Google Scholar] [CrossRef] [PubMed]
- García, P.S.; Kreuzer, M.; Hight, D.; Sleigh, J.W. Effects of noxious stimulation on the electroencephalogram during general anaesthesia: A narrative review and approach to analgesic titration. Br. J. Anaesth. 2021, 126, 445–457. [Google Scholar] [CrossRef]
- Kim, D.; Ahn, J.H.; Heo, G.; Jeong, J.S. Comparison of bispectral Index and Patient State Index values according to recovery from moderate neuromuscular block under steady-state total intravenous anesthesia. Sci. Rep. 2021, 11, 5908. [Google Scholar] [CrossRef]
- Bruhn, J.; Bouillon, T.W.; Shafer, S.L. Electromyographic activity falsely elevates the bispectral index. Anesthesiology 2000, 92, 1485–1487. [Google Scholar] [CrossRef]
- Savoia, G.; Scibelli, G. From balanced to precision anesthesia: A complex road map. Minerva Anestesiol. 2018, 84, 534–537. [Google Scholar] [CrossRef]
- Meijer, F.; Honing, M.; Roor, T.; Toet, S.; Calis, P.; Olofsen, E.; Martini, C.; van Velzen, M.; Aarts, L.; Niesters, M.; et al. Reduced postoperative pain using nociception Level-guided fentanyl dosing during sevoflurane anaesthesia: A randomised controlled trial. Br. J. Anaesth. 2020, 125, 1070–1078. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables (Unit) | Geriatrics (Age ≥ 75, n = 23) | Non-Geriatrics (Age < 75, n = 96) | p-Value |
|---|---|---|---|
| Female/male | 21/2 | 93/3 | 0.247 |
| Age (year) | 79.4 ± 2.7 | 59.2 ± 9.4 | <0.001 |
| Etiology of LLL, n (%) | 0.173 | ||
| Gynecologic cancer * | 18 (78.3%) | 68 (70.8%) | |
| Non-gynecologic cancer ** | 5 (21.7%) | 28 (29.2%) | |
| ISL stage (0–1/2–3) | 2/21 | 4/92 | 0.328 |
| BMI (kg/m2) | 27.5 ± 5.6 | 26.5 ± 5.0 | 0.392 |
| Diabetes mellitus, yes/no | 2/21 | 19/77 | 0.360 |
| Hypertension, yes/no | 15/8 | 37/59 | 0.021 |
| Affected lower limb (left/right) | 13/10 | 55/38 | 0.947 |
| Chemotherapy, yes/no | 4/19 | 42/54 | 0.020 |
| Radiotherapy, yes/no | 11/12 | 42/54 | 0.724 |
| Duration of lymphedema (year) | 9.6 (3.4–13.7) | 4.2 (1.3–10.2) | 0.06 |
| Cellulitis episode (per year) | 2 (1–3) | 1 (0–2) | 0.027 |
| Volume gained in the lymphedematous limb @ (mL) | 2325.0 (1709.0–3921.7) | 2123.5 (1548.5–2923.5) | 0.286 |
| Variables (Unit) | Geriatrics (Age ≥ 75, n = 23) | Non-Geriatrics (Age < 75, n = 96) | p-Value |
|---|---|---|---|
| Intraoperative | |||
| Incisions (n) | 4 (3–4) | 4 (3–5) | 0.380 |
| Lymphatic vessels found (n) | 5 (4–6) | 5 (4.5–7) | 0.123 |
| Size of lymphatic vessels (mm) | 0.80 (0.5–1.0) | 0.60 (0.45–0.80) | <0.001 |
| Total number of recipient’s veins (n) | 85 | 433 | |
| Recipient veins per patient (n) | 4 (3–5.5) | 4 (3–5) | 0.887 |
| Size of recipient veins per patient (mm) | 0.80 (0.7–1.0) | 0.80 (0.6–1.0) | 0.837 |
| Number of LVA performed per patient (n) | 7 (5.5–8.5) | 8 (5–10) | 0.314 |
| NECST classification, n (%) | <0.001 | ||
| Normal | 62.40% | 384.51% | |
| Ectasis | 53.34% | 113.15% | |
| Constriction | 31.20% | 226.30% | |
| Sclerosis | 9.6% | 30.4% | |
| Postoperative | |||
| Mean follow-up, post-LVA (month) | 10.6 ± 5.8) | 10.6 ± 6.0 | 0.988 |
| Post-LVA volume reduction * (mL) | 513 (178–1080) | 684 (101.5–1505.5) | 0.614 |
| Post-LVA percentage of volume Reduction ** (%) | 19.7 (8.0–60.2) | 34.1 (6.9–62.1) | 0.681 |
| Variables (Unit) | Geriatrics (Age ≥ 75, n = 23) | Non-Geriatrics (Age < 75, n = 96) | p-Value |
|---|---|---|---|
| Operation time (min) | 463.0 (389.0–504.0) | 451.5 (385.0–511.0) | 0.593 |
| Respiratory rate (/min) | 11 (9–12.5) | 11 (10–13) | 0.987 |
| SpO2 (%) | 99 (98–100) | 99 (98–100) | 0.953 |
| Urine output (ml/kg/h) | 1.59 (0.84–2.70) | 2.58 (1.78–3.79) | 0.012 |
| Bispectral index (BIS value) | 55 (49–58) | 55 (50–60) | 0.773 |
| Propofol | |||
| Total consumption (mg/kg/h) | 4.05 (3.73–4.77) | 5.01 (4.34–5.92) | 0.001 |
| Maintenance Ce by Schnider model (μg/mL) | 2.0 (1.5–2.2) | 2.0 (1.8–2.5) | 0.240 |
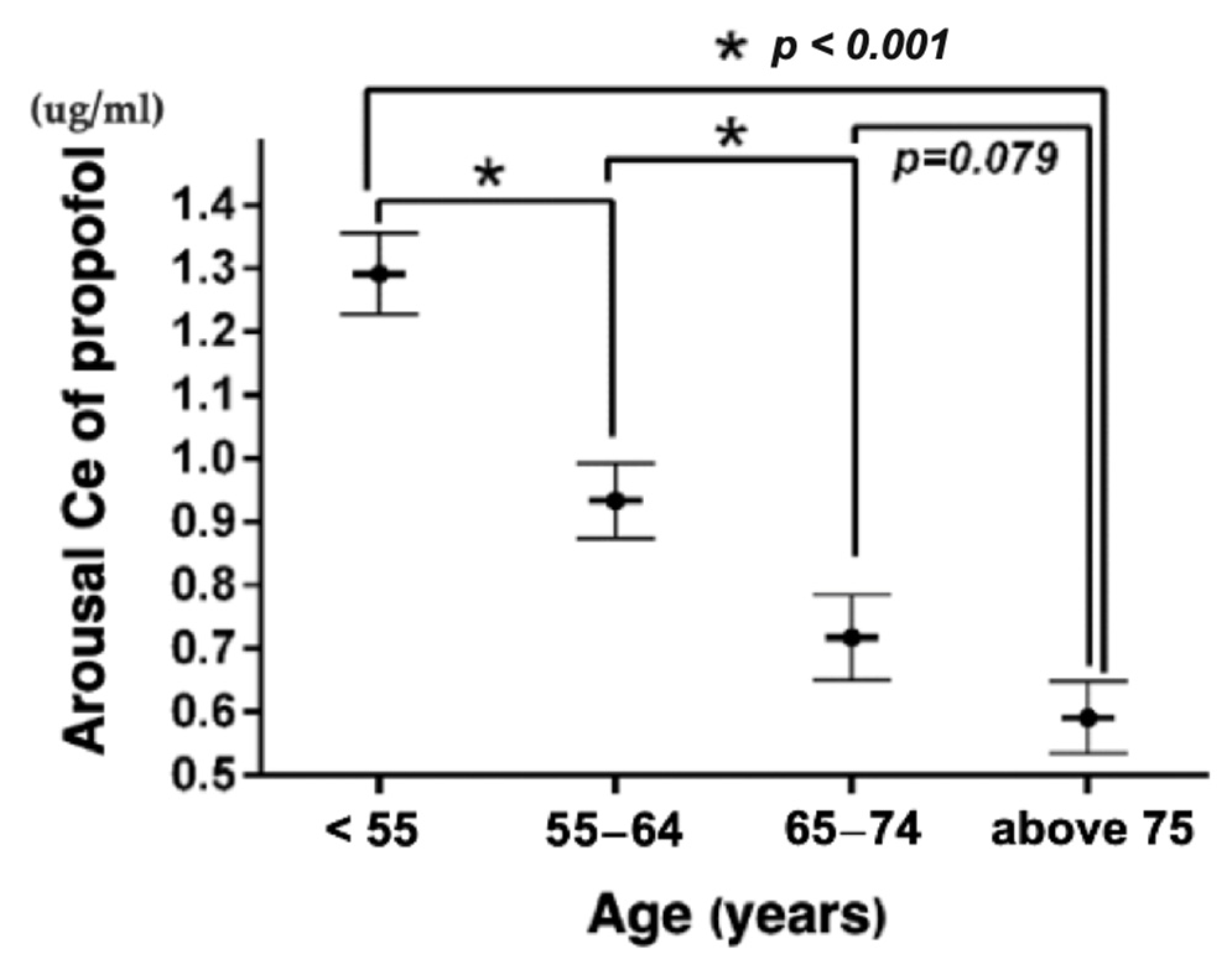
| Arousal Ce (μg/mL) | ≥75 years, 0.6 (0.5–0.7) | 0.9 (0.8–1.2) | <0.001 |
| ≤54 years, 1.3 (1.2–1.4) | <0.001 | ||
| 55–64 years, 0.9 (0.8–1.0) | <0.001 | ||
| 65–74 years, 0.7 (0.6–0.8) | 0.079 | ||
| Alfentanil | |||
| Total consumption (μg/kg/h) | 4.67 (2.53–5.82) | 6.68 (3.85–8.77) | 0.047 |
| Maintenance Ce by Scott model (ng/mL) | 18 (15–30) | 25 (20–30) | 0.114 |
| Arousal Ce (ng/mL) | 15 (10–30) | 25 (20–30) | 0.026 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, E.-B.; Lin, Y.-H.; Yang, J.C.-S.; Lai, C.-W.; Chin, J.-C.; Wu, S.-C. Density Spectral Array Enables Precise Sedation Control for Supermicrosurgical Lymphaticovenous Anastomosis: A Retrospective Observational Cohort Study. Bioengineering 2023, 10, 494. https://doi.org/10.3390/bioengineering10040494
Wu E-B, Lin Y-H, Yang JC-S, Lai C-W, Chin J-C, Wu S-C. Density Spectral Array Enables Precise Sedation Control for Supermicrosurgical Lymphaticovenous Anastomosis: A Retrospective Observational Cohort Study. Bioengineering. 2023; 10(4):494. https://doi.org/10.3390/bioengineering10040494
Chicago/Turabian StyleWu, En-Bo, Yu-Hsuan Lin, Johnson Chia-Shen Yang, Chiung-Wen Lai, Jo-Chi Chin, and Shao-Chun Wu. 2023. "Density Spectral Array Enables Precise Sedation Control for Supermicrosurgical Lymphaticovenous Anastomosis: A Retrospective Observational Cohort Study" Bioengineering 10, no. 4: 494. https://doi.org/10.3390/bioengineering10040494