1. Introduction
Patients with terminal heart failure (HF) often require heart transplantation or mechanical circulatory support (MCS). Left ventricular assist devices (LVAD) support the unloading of the left ventricle (LV), increase cardiac output, and improve end-organ perfusion. They are implanted as bridges to transplant and increasingly as destination therapy. Over the past years, centrifugal-flow pumps have replaced axial-flow pumps. New devices have not only become smaller but safer [
1]. Nowadays, the most widely implanted LVAD is the HeartMate3 (HM3, Abbott, Abbott Park, IL, USA). Despite steady development, LVAD implantation is still considered a high-risk procedure [
2]. In addition to death, stroke, and bleeding, common LVAD-associated adverse events include cardiac arrhythmia, driveline and blood infections, respiratory failure, and right HF. Although rare, external compression of the outflow graft can cause relevant graft obstruction requiring surgical revision or stent implantation [
3].
There are various approaches to increase the safety of LVAD implantations. Particularly, minimally invasive implantation techniques, defined as LVAD surgery without sternotomy, have gained importance [
2]. LVADs might be implanted via upper hemisternotomy and left anterolateral thoracotomy. In the case of isolated LVAD implantation, off-pump implantation might be considered [
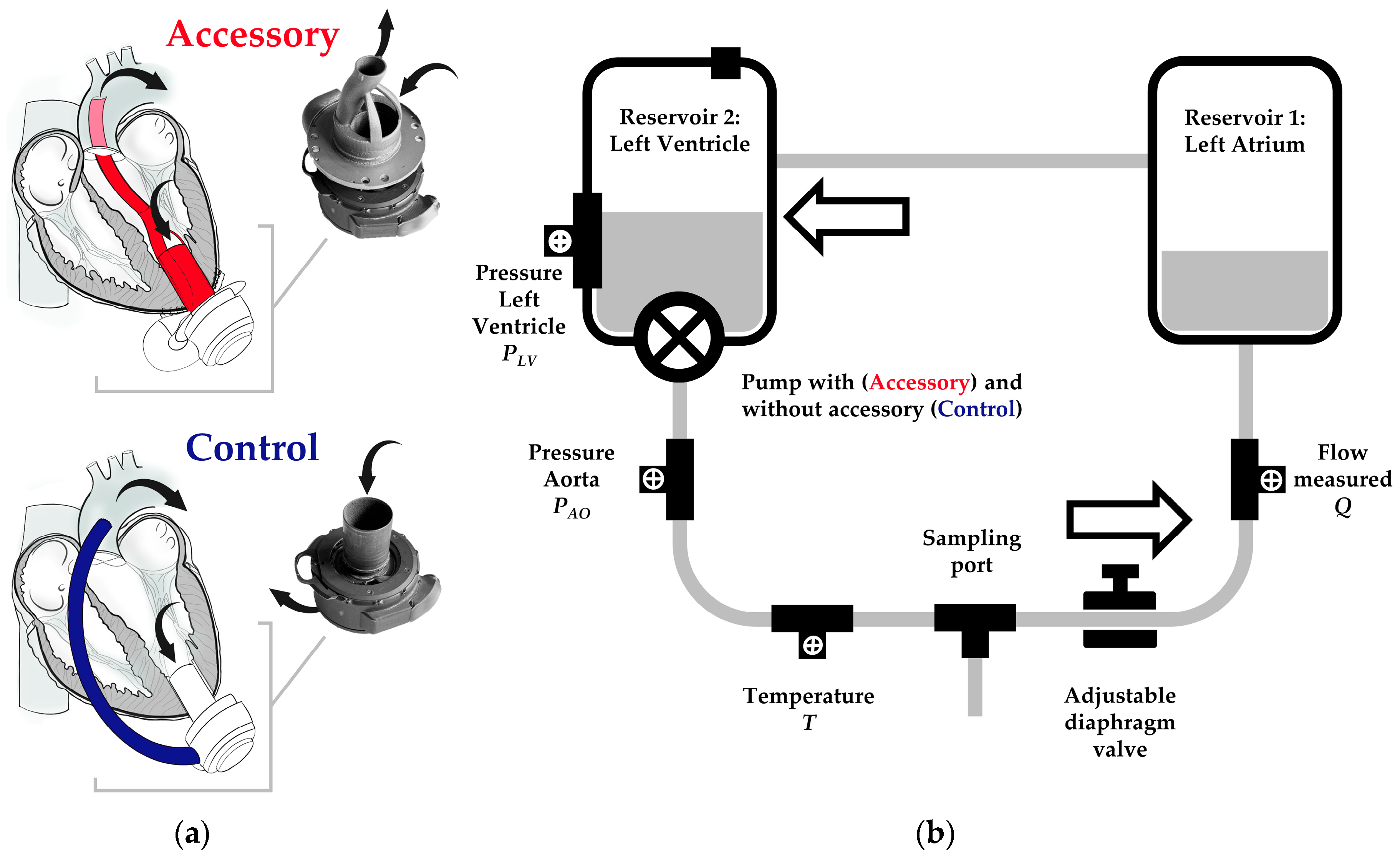
4]. With the aim of both minimizing surgical access and off-pump implantation, we are developing an LVAD accessory. The accessory combines LVAD inflow and outflow and can be attached to the actual device. The outflow graft is positioned through the LV across the aortic valve. Thus, transapical access solely is required for LVAD implantation. Recently, we have demonstrated the successful off-pump implantation of a first prototype via left thoracotomy in five pigs [
5]. The accessory tested in vivo revealed several rheological limitations. Among others, it had redirections with rather small radii favoring flow turbulences. Furthermore, it was characterized by varying inflow and outflow diameters. The alterations of the cross-sectional area resulted in flow acceleration in more narrow sections and flow deceleration in wider ones. Supported by computational fluid dynamics, we have improved the design of the LVAD accessory continuously. The new prototype is characterized by a flow-optimized design and is made of titanium. The prototype is 3D printed and can be adapted individually to the LV dimensions of the in vivo model. Prospectively, it might be designed individually for the patient undergoing LVAD implantation. In addition to computational fluid dynamics and ahead of in vivo testing, we aimed to assess the performance of the new LVAD accessory with respect to flow, pressure head, and pump power in vitro.
Mock circulatory loops (MCL) are frequently used to assess the performance of MCS devices in vitro. They consist of hydraulic and mechanical components representing defined cardiovascular structures such as the heart and aorta. A broad variety of physiological and pathological conditions (e.g., HF) can be simulated by specific parameters, including systemic resistance and vascular compliance [
6]. Although in vitro testing in MCLs is characterized by a high level of standardization and reproducibility, their evidence is limited by the simplification of complex anatomical structures and physiological mechanisms.
In this study, we compared the performance of a continuous-flow HM3 with and without the LVAD accessory in vitro in an MCL using a water/glycerol solution as a blood substitute. Primarily, we aimed to compare both groups in terms of flow, pressure head, and pump power to optimize the accessory’s design further. Secondarily, we aimed to determine the accuracy and reliability of HM3 flow estimation derived from fixed speed, power, and patient’s hematocrit (HCT) as indicators for fluid viscosity [
7]. Since the exact algorithm has not been publicly reported by the manufacturer, we aimed to compare measured and estimated flow with and without LVAD accessory in an MCL using a water/glycerol solution instead of human blood.
4. Discussion
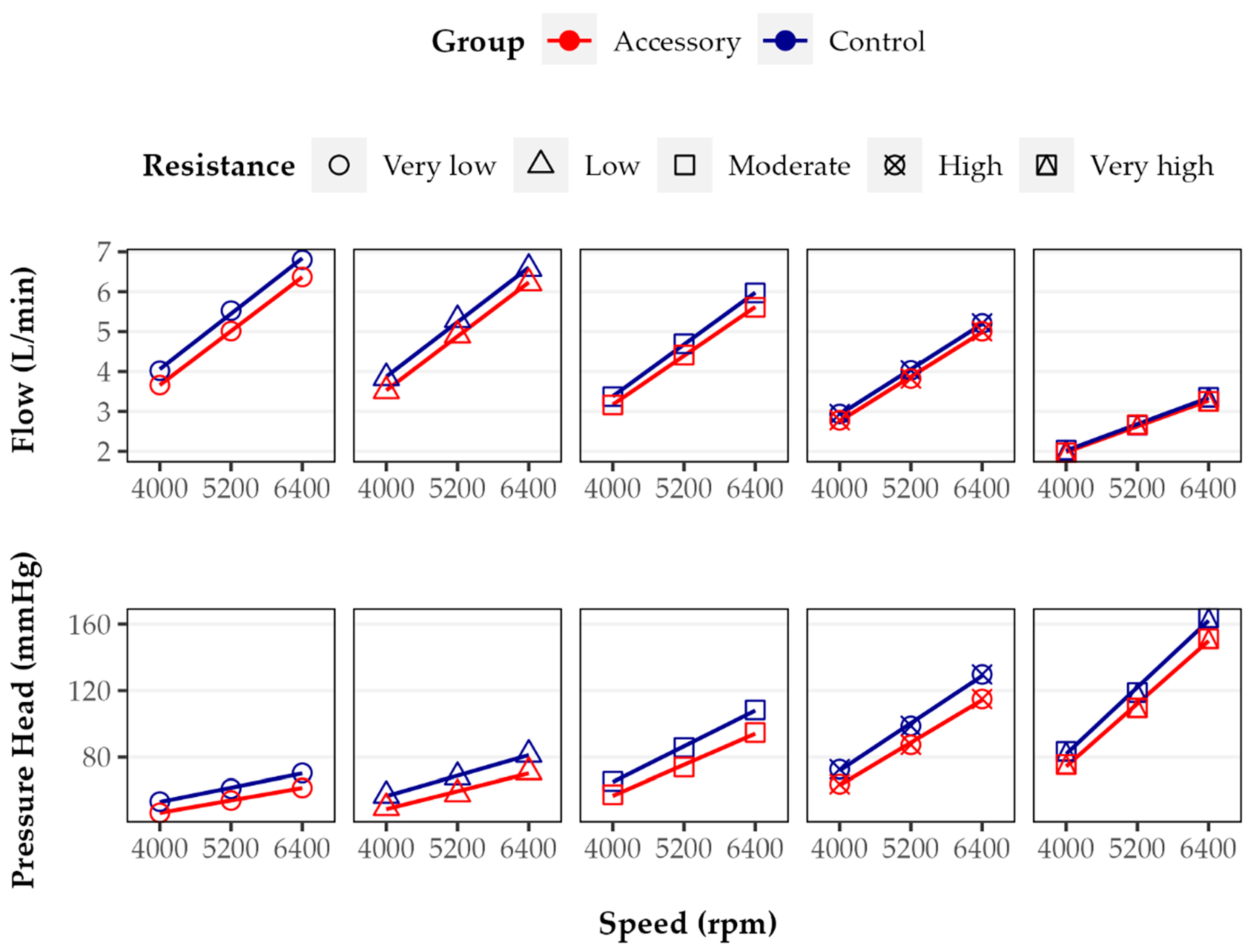
In general, LVAD flow is dependent on rotational speed and inversely dependent on pressure head or differential pressure between the pump inlet and outlet, in clinical use determined by left ventricular and aortic pressure [
6]. This study showed that operating HM3 with LVAD accessory reduced flow and pressure head up to 9.3% and 15.0%, respectively.
These findings lead to the question of potential causes, including the accessory’s design. Among others, we identified three main limitations of the current accessory design. First, the accessory reveals two almost rectangular redirections with small radii just behind its inlet. In the case of design optimization, the redirections should be replaced, and the radii, if possible, be increased. Second, in the middle section of the accessory (not shown in detail in
Figure 1), the main flow channel is divided into two parallel subchannels. Although the cross-sectional area remains constant, the channel surface area increases, favoring friction loss. Third, in the middle section of the outflow channel, the cross-sectional shape changes from round to oval, which presumably generates turbulences at channel separation and confluence, contributing to flow reduction. This is because consideration should be given to foregoing flow channel separation and changing the cross-sectional shape. The proposed design optimizations may result in a partial loss of the compact and, thus, space-saving design. To achieve an optimal balance between pump performance, characterized by flow and pressure head, and design constraints restricting the size of the implanted device (in particular, due to the limited space between apex and rib cage), the findings from computational fluid dynamics, further MCL tests, and ultimately animal testing must be considered together. A design that has been optimized solely based on in vitro tests does not necessarily correspond to the best design for implantation in vivo.
For in vivo testing, it is additionally important to consider different outflow lengths and graft materials in the Accessory and Control groups. While the length of the accessory’s transventrciular outflow graft depends on the distance between the LV apex and mid-ascending aorta, the length of extracardiac outflow grafts is determined by the anterior shape of the heart, which makes conventional outflow grafts significantly longer (according to our own but not yet published data). For this in vitro study, we decided to apply outflow grafts of equal lengths in both groups. Overall, we hypothesize that the influence of graft length is less relevant than the influence of graft geometry and changes in the cross-sectional area. With respect to the graft material, we apply different materials for MCL and animal testing. In the case of animal testing, we use stent grafts made of well-proven polyester and nitinol materials. These materials have unique mechanical properties but are only limited and suitable for MCL experiments, in particular, due to leakage. This is because we prefer to use PVC tubing with a suitable diameter as an outflow graft in the case of MCL testing. We assume that the influence of different materials is rather small in the case of large-diameter grafts (greater than 8 mm in diameter). Prospectively, we intend to investigate both the effect of different graft lengths as well as the effect of different materials.
Beyond the implications for the accessory’s design, including the outflow graft, it has to be noted that the application of an LVAD accessory, which can be seen as an add-on to the actual LVAD, requires operating the LVAD at a higher rotational speed in order to achieve the same flow and pressure head as the application without an LVAD accessory. Although the differences appear rather small, it cannot be negated that higher pump speeds might contribute to adverse events, for example, increased degradation of hemostatic blood proteins such as von Willebrand factor (vWF). To our knowledge, there has been no study assessing the relationship between HM3 pump speed and vWF degradation in an MCL. However, Bartoli and colleagues investigated the centrifugal-flow EVAHEART pump (EVAHEART, Bellaire, TX) in vitro and found significantly fewer vWF fragments at lower pump speeds as a result of less shear stress [
9]. On the other hand, studies on axial-flow HeartMate II (Abbott, Abbott Park, IL, USA), the pump generation before centrifugal-flow HM3, show that reduced pump speed does not significantly decrease vWF degradation [
10]. In the absence of data for HM3, however, we hypothesize that blood trauma increases when the use of an LVAD accessory requires higher pump speeds. To determine the exact relationship between HM3 pump speed and vWF degradation, further investigations are necessary.
Each LVAD pump has its unique pressure head–flow relationship, also referred to as pump or HQ curve. Since for HM3, the HQ curves with and without LVAD accessory are curvilinear and parallel, the same change in flow results in almost the same change in pressure head. From a clinical perspective, the accessory seems to have no relevant impact on the pump’s sensitivity to afterload as well as higher blood pressure [
11]. Compared to the reference HQ curves for HM3 reported in intervals of 1000 rpm by the manufacturer [
12], there are slight differences to the HQ curves obtained for HM3 without the accessory in this study. Although all curves are curvilinear, the negative slopes of the reference curves are smaller. Therefore, the same increase in pressure head leads to a higher increase in flow [
13]. This might be explained by differences in the experimental setup of the MCL including pre- and afterload.
The pump’s power consumption is the product of current and voltage applied to the motor. In the case of HM3, it ranges from 3 to 7 W [
11]. During our in vitro testing, the lowest pump power was found at the lowest resistance level and pump speed without the accessory. In both groups, the power at least doubled while increasing the pump speed from 4000 to 6400 rpm but slightly decreased with higher resistance. The relative difference found with and without the accessory was rather small, ranging from 0.0 to 4.0%. Taking into consideration that a fully charged set of batteries powers the system for 10 to 17 h, this duration would be reduced by about 25 to 40 min.
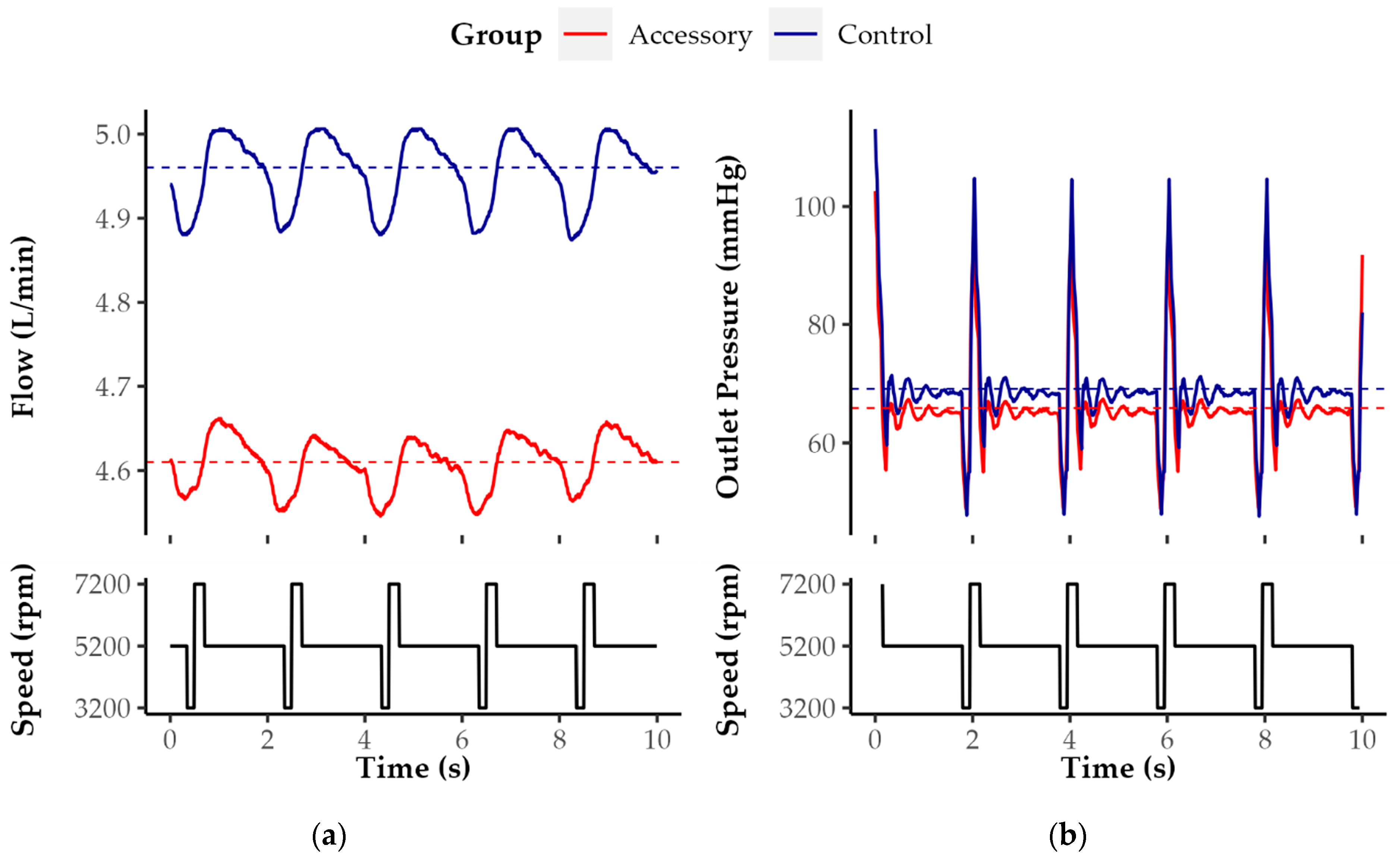
In clinical use, the PI quantifies the flow variation across the cardiac cycle. It is calculated from maximum and minimum flow as well as mean flow (PI = [Maximum − Minimum]/Mean Flow). In the case of HM3, it ranges between 1 and 4 [
11]. Our results indicate that in both groups the PI decreases with increasing pump speed. The PI decreases most likely due to the increase in mean flow.
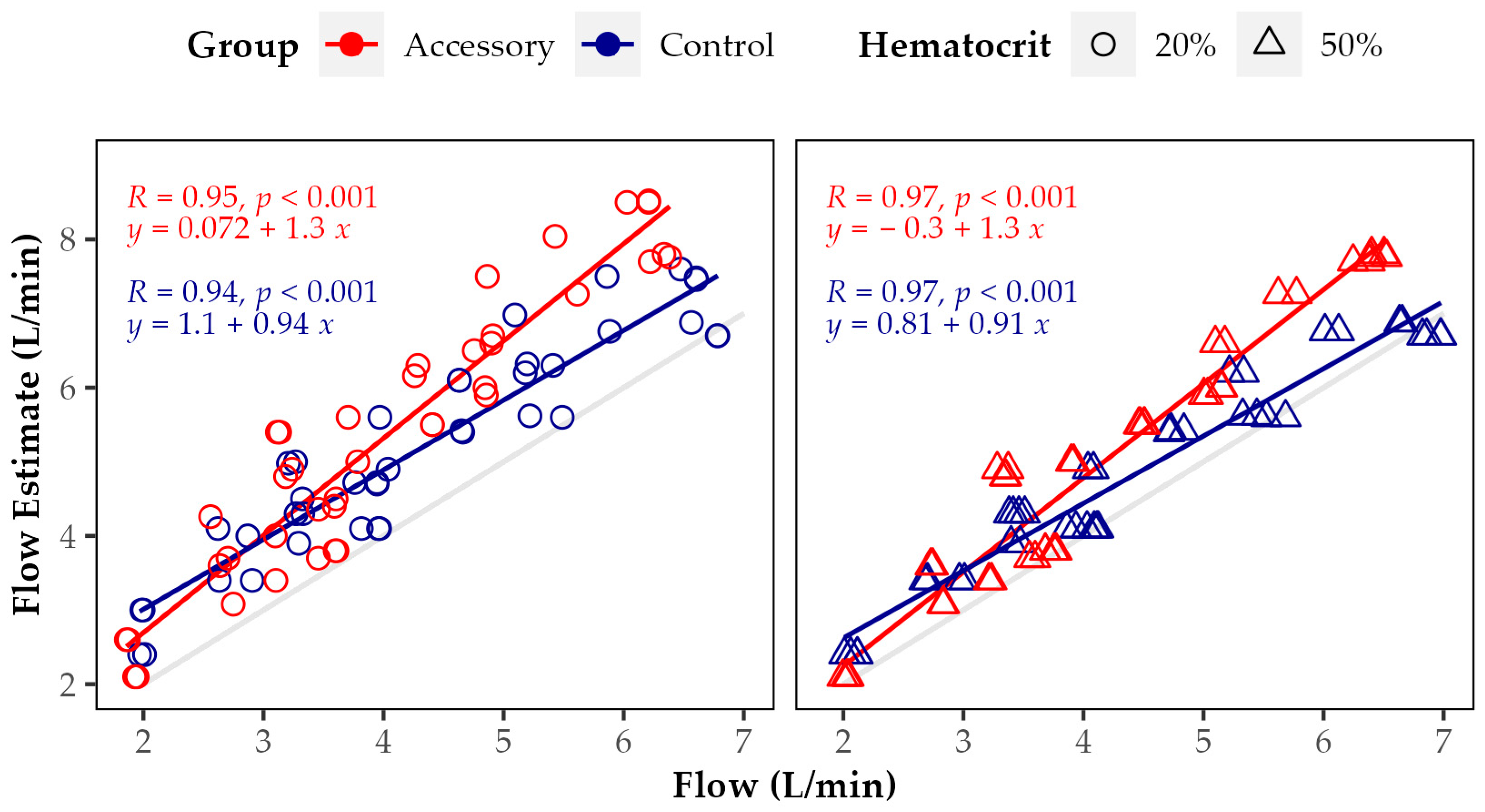
Referring to the accuracy of HM3 flow estimation with and without the accessory, our data show that there is a strong and highly significant correlation between measured and estimated flow. However, overall, the flow estimate is significantly higher than the measured flow, in particular, when applying an HCT value of 20%. The relative overestimation increased with higher resistance, higher pump speed, and with the LVAD accessory. The greatest relative difference between measured and estimated flow was found at 6400 rpm and very high resistance with LVAD accessory and at low HCT. Since the HM3 flow estimation algorithm does not account for the use of an accessory, which according to our results, reduces flow and pressure head, this might explain, in part, the observed increased flow overestimation in the Accessory group. Overall, the reliability of HM3 flow estimation in an MCL without appropriate correction is limited. To our knowledge, so far, the exact algorithm applied for HM3 flow estimation has not been reported. Nevertheless, according to the manufacturer, it is derived from fixed speed, power, and the patient’s HCT or preset viscosity. Furthermore, the flow estimate is reduced by increased blood pressure [
7]. As in our MCL, the first in vitro studies evaluating the algorithm’s accuracy were performed with a water/glycerol solution. For flows greater than 3 L/min, the accuracy was about 10%, which is comparable to the results of our study at a very low resistance level throughout all tested pump speeds without the accessory [
14]. Analogous to Hasin and colleagues for HeartMate II, Castagna and colleagues found only a poor correlation between HM3 flow estimate and the cardiac output measured by thermodilution (R = 0.46,
p < 0.0001). The authors proposed to include LVAD power, systolic blood pressure, hemoglobin, and weight in the algorithm applied for flow estimation [
15].
Addressing the limitations of this study, the MCL used to determine the impact of the LVAD accessory on flow and pressure head was simplified. For example, the remaining heart function and physiological pulsatility as well as vascular compliance were not considered. Furthermore, the MCL did not account for HF and specific hemodynamic conditions in particular. The diaphragm valve could be adjusted only gradually, which made precise adjustment difficult. Instead of whole blood, a water/glycerol solution was applied as fluid. Lastly, all experiments were conducted at room temperature (about 23 °C) instead of body temperature.

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





