

Virtual Reality and Augmented Reality in Plastic and Craniomaxillofacial Surgery: A Scoping Review
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Search
2.4. Selection Criteria
2.5. Data Collection Process
2.6. Data Items
3. Results
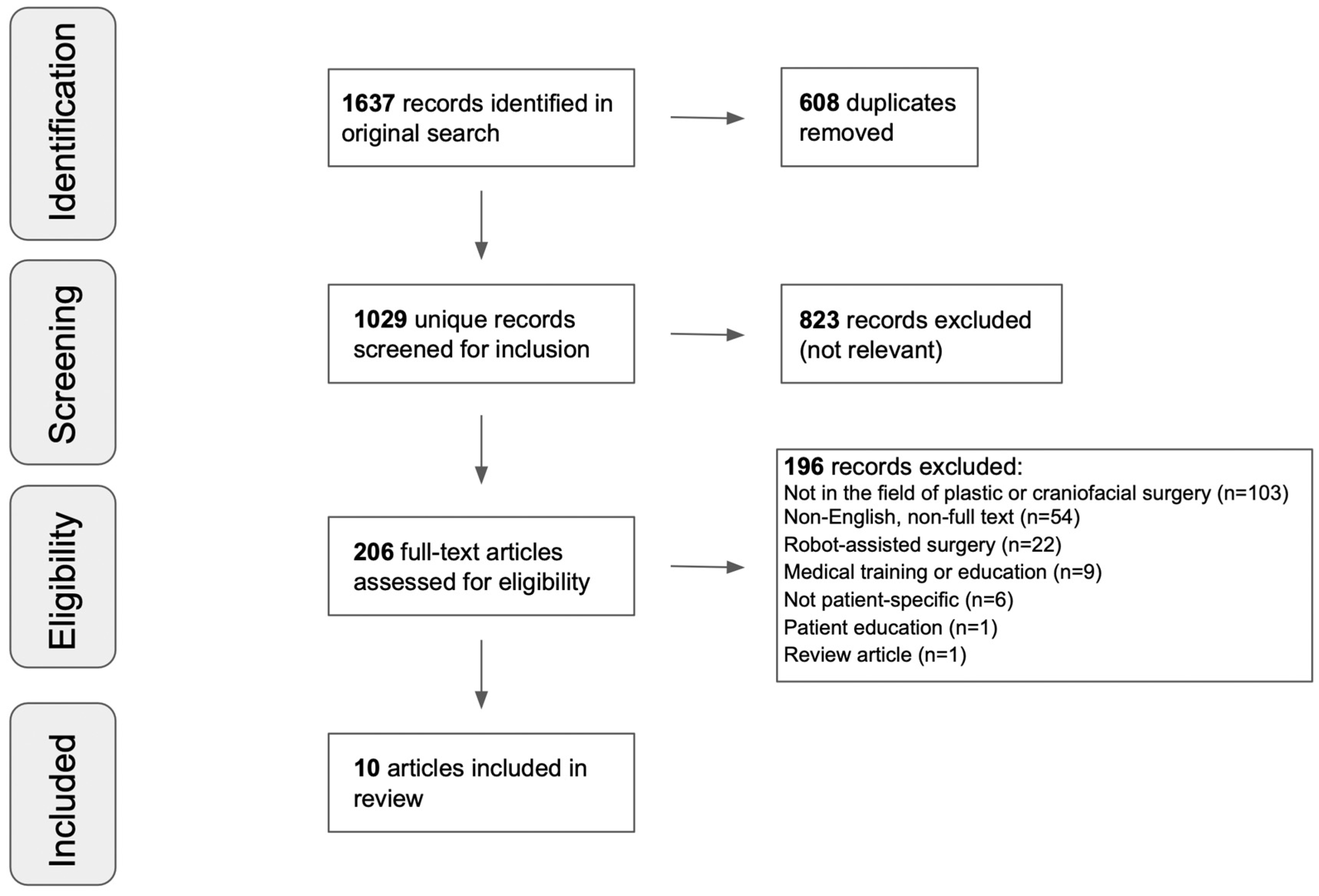
3.1. Search Results
3.2. Characteristics of Included Studies
3.3. Year of Publication
3.4. Type of Paper
3.5. Timing of Implementation
3.6. Clinical Context
3.7. Hardware
3.8. Software
4. Discussion
4.1. Three-Dimensional Imaging in Plastic and Craniomaxillofacial Surgery
4.2. Methodologies of the Included Studies
4.3. Preoperative and Intraoperative Use in Plastic and Craniomaxillofacial Surgery
4.4. Broader Utility of VR and AR in Surgery
4.5. Cost and Time Savings
4.6. Limitations
4.6.1. Data Collection
4.6.2. Limitations of AR and VR in Plastic and Craniomaxillofacial Surgery
4.6.3. Limitations of the Included Studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Caudell, T.P.; Mizell, D.W. Augmented reality: An application of heads-up display technology to manual manufacturing processes. In Proceedings of the Twenty-Fifth Hawaii International Conference on System Sciences, Kauai, HI, USA, 7–10 January 1992; Volume 2, pp. 659–669. [Google Scholar] [CrossRef]
- Eckert, M.; Volmerg, J.S.; Friedrich, C.M. Augmented Reality in Medicine: Systematic and Bibliographic Review. JMIR MHealth UHealth 2019, 7, e10967. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, I.E. Head-Mounted Three Dimensional Display. In Proceedings of the AFIPS ‘68 Fall Joint Computer Conference, San Francisco, CA, USA, 9–11 December 1968; Volume 33 Pt 1, pp. 757–764. [Google Scholar] [CrossRef]
- Sutherland, J.; Belec, J.; Sheikh, A.; Chepelev, L.; Althobaity, W.; Chow, B.J.W.; Mitsouras, D.; Christensen, A.; Rybicki, F.J.; La Russa, D.J. Applying Modern Virtual and Augmented Reality Technologies to Medical Images and Models. J. Digit. Imaging 2019, 32, 38–53. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Kim, H.; Kim, Y.O. Virtual Reality and Augmented Reality in Plastic Surgery: A Review. Arch. Plast. Surg. 2017, 44, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Somma, L.; Iacoangeli, M.; Nasi, D.; Balercia, P.; Lupi, E.; Girotto, R.; Polonara, G.; Scerrati, M. Combined supra-transorbital keyhole approach for treatment of delayed intraorbital encephalocele: A minimally invasive approach for an unusual complication of decompressive craniectomy. Surg. Neurol. Int. 2016, 7, S12–S16. [Google Scholar] [CrossRef]
- Sayadi, L.R.; Naides, A.; Eng, M.; Fijany, A.; Chopan, M.; Sayadi, J.J.; Shaterian, A.; Banyard, D.A.; Evans, G.R.D.; Vyas, R.; et al. The New Frontier: A Review of Augmented Reality and Virtual Reality in Plastic Surgery. Aesthet. Surg. J. 2019, 39, 1007–1016. [Google Scholar] [CrossRef]
- Lee, G.K.; Moshrefi, S.; Fuertes, V.; Veeravagu, L.; Nazerali, R.; Lin, S.J. What Is Your Reality? Virtual, Augmented, and Mixed Reality in Plastic Surgery Training, Education, and Practice. Plast. Reconstr. Surg. 2021, 147, 505–511. [Google Scholar] [CrossRef]
- Burdea, G.C.; Coiffet, P. Virtual Reality Technology; Wiley: Hoboken, NJ, USA, 2003. [Google Scholar]
- Foxlin, E.; Harrington, M.; Pfeifer, G. Constellation: A Wide-Range Wireless Motion-tracking System for Augmented Reality and Virtual Set Applications. In Proceedings of the 25th Annual Conference on Computer Graphics and Interactive Techniques, SIGGRAPH 1998, Orlando, FL, USA, 19–24 July 1998; pp. 371–378. [Google Scholar]
- Valve: SteamVR Tracking. Available online: https://partner.steamgames.com/vrtracking (accessed on 14 November 2022).
- Amini, S.; Kersten-Oertel, M. Augmented reality mastectomy surgical planning prototype using the HoloLens template for healthcare technology letters. Healthc. Technol. Lett. 2019, 6, 261–265. [Google Scholar] [CrossRef]
- Coelho, G.; Rabelo, N.N.; Vieira, E.; Mendes, K.; Zagatto, G.; de Oliveira, R.S.; Raposo-Amaral, C.E.; Yoshida, M.; de Souza, M.R.; Fagundes, C.F.; et al. Augmented reality and physical hybrid model simulation for preoperative planning of metopic craniosynostosis surgery. Neurosurg. Focus 2020, 48, E19. [Google Scholar] [CrossRef]
- García-Mato, D.; Moreta-Martínez, R.; García-Sevilla, M.; Ochandiano, S.; García-Leal, R.; Pérez-Mañanes, R.; Calvo-Haro, J.A.; Salmerón, J.I.; Pascau, J. Augmented reality visualization for craniosynostosis surgery. Comput. Methods Biomech. Biomed. Eng. Imaging Vis. 2021, 9, 392–399. [Google Scholar] [CrossRef]
- Pratt, P.; Ives, M.; Lawton, G.; Simmons, J.; Radev, N.; Spyropoulou, L.; Amiras, D. Through the HoloLensTM looking glass: Augmented reality for extremity reconstruction surgery using 3D vascular models with perforating vessels. Eur. Radiol. Exp. 2018, 2, 2. [Google Scholar] [CrossRef]
- Wesselius, T.S.; Meulstee, J.W.; Luijten, G.; Xi, T.; Maal, T.J.J.; Ulrich, D.J.O. Holographic Augmented Reality for DIEP Flap Harvest. Plast. Reconstr. Surg. 2020, 147, 25E–29E. [Google Scholar] [CrossRef] [PubMed]
- Bergeron, L.; Bonapace-Potvin, M.; Bergeron, F. In-house 3D Model Printing for Acute Cranio-maxillo-facial Trauma Surgery: Process, Time, and Costs. Plast. Reconstr. Surg.—Glob. Open. 2021, 9, e3804. [Google Scholar] [CrossRef] [PubMed]
- Cates, C.U.; Lönn, L.; Gallagher, A.G. Prospective, randomised andblinded comparison of proficiency-based progression full-physicsvirtual reality simulator training versus invasive vascular experi-ence for learning carotid artery angiography by very experiencedoperators. BMJ Simul. Technol. Enhanc. Learn 2016, 2, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.; Qandeel, M.; Ramakrishna, R.; Yang, C.W. Virtual simulation inenhancing procedural training for fluoroscopy-guided lumbar punc-ture: A Pilot Study. Acad. Radiol. 2018, 25, 235–239. [Google Scholar] [CrossRef]
- Bianchi, S.; Bernardi, S.; Perilli, E.; Cipollone, C.; Di Biasi, J.; Macchiarelli, G. Evaluation of Effectiveness of Digital Technologies During Anatomy Learning in Nursing School. Appl. Sci. 2020, 10, 2357. [Google Scholar] [CrossRef]
- Bekelis, K.; Calnan, D.; Simmons, N.; MacKenzie, T.A.; Kakoulides, G. Effect of an immersive preoperative virtual reality experience on patient reported outcomes: A randomized controlled trial. Ann. Surg. 2017, 265, 1068–1073. [Google Scholar] [CrossRef]
- Noben, L.; Goossens, S.; Truijens, S.E.M.; Van Berckel, M.M.G.; Perquin, C.W.; Slooter, G.D.; Van Rooijen, S.J. A virtual reality video to improve information provision and reduce anxiety before cesarean delivery: Randomized controlled trial. JMIR Ment. Health. 2019, 6, e15872. [Google Scholar] [CrossRef]
- Mahajan, U.V.; Sunshine, K.S.; Herring, E.Z.; Labak, C.M.; Wright, J.M.; Smith, G. Virtual reality in presurgical patient education: A scoping review and recommended trial design guidelines. Am. J. Surg. 2021, 222, 704–705. [Google Scholar] [CrossRef]
- Pensieri, C.; Pennacchini, M. Virtual Reality in Medicine. In Handbook on 3D3C Platforms; Springer: Berlin, Germany, 2016; pp. 353–401. [Google Scholar] [CrossRef]
- IDC Spending Guide Forecasts Strong Growth for Augmented and Virtual Reality. Available online: https://www.idc.com/getdoc.jsp?containerId=prUS49916122 (accessed on 22 December 2022).
- Giacalone, G.; Yamamoto, T.; Belva, F.; Hayashi, A.; Dori, Y.; Zviman, M.M.; Gysen, M.; Nam, H.H.; Jolley, M.A.; Kato, M. The application of virtual reality for preoperative planning of lymphovenous anastomosis in a patient with a complex lymphatic malformation. J. Clin. Med. 2019, 8, 371. [Google Scholar] [CrossRef]
- Cho, K.H.; Papay, F.A.; Yanof, J.; West, K.; Gharb, B.B.; Rampazzo, A.; Gastman, B.; Schwarz, G.S. Mixed Reality and 3D Printed Models for Planning and Execution of Face Transplantation. Ann. Surg. 2021, 274, E1238–E1246. [Google Scholar] [CrossRef]
- Mespreuve, M.; Waked, K.; Collard, B.; De Ranter, J.; Vanneste, F.; Hendrickx, B. The Usefulness of Magnetic Resonance Angiography to Analyze the Variable Arterial Facial Anatomy in an Effort to Reduce Filler-Associated Blindness: Anatomical Study and Visualization Through an Augmented Reality Application. Aesthetic Surg. J. Open Forum 2021, 3, ojab018. [Google Scholar] [CrossRef]
- Waked, K.; Mespreuve, M.; De Ranter, J.; Collard, B.; Hahn, S.; Hendrickx, B. Visualizing the Individual Arterial Anatomy of the Face Through Augmented Reality—A Useful and Accurate Tool During Dermal Filler Injections. Aesthetic Surg. J. Open Forum 2022, 4, ojac012. [Google Scholar] [CrossRef]
- Yaremenko, A.I.; Lysenko, A.V.; Ivanova, E.A.; Galibin, O.V. Augmented reality technology for auricular reconstruction in the treatment of microtia. Cell. Ther. Transplant. 2020, 9, 78–82. [Google Scholar] [CrossRef]
- Rybicki, F.J.; Grant, G.T. 3D Printing in Medicine; Springer International Publishing: NY, NY, USA, 2017. [Google Scholar]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
- Farronato, G.; Galbiati, G.; Esposito, L.; Mortellaro, C.; Zanoni, F.; Maspero, C. Three-dimensional virtual treatmentplanning: Presurgical evaluation. J. Craniofac. Surg. 2018, 29, e433–e437. [Google Scholar] [CrossRef]
- Steinbacher, D.M. Three-dimensional analysis and surgical planning in craniomaxillofacial surgery. J. Oral. Maxillofac. Surg. 2015, 73, S40–S56. [Google Scholar] [CrossRef] [PubMed]
- Seruya, M.; Borsuk, D.E.; Khalifian, S.; Carson, B.S.; Dalesio, N.M.; Dorafshar, A.H. Computer-aided design and manufacturing in craniosynostosis surgery. J. Craniofac. Surg. 2013, 24, 1100–1105. [Google Scholar] [CrossRef]
- Glover, J.C. 3D bioprinting applications for in vitro mode-ling of cellular interactions and tissues. Cell Transpl. 2016, 5, 8–11. [Google Scholar]
- Wake, N.; Rosenkrantz, A.B.; Huang, R.; Park, K.U.; Wysock, J.S.; Taneja, S.S.; Huang, W.C.; Sodickson, D.K.; Chandarana, H. Patient-specific 3D printed and augmented reality kidney and prostate cancer models: Impact on patient education. 3D Print. Med. 2019, 5, 4. [Google Scholar] [CrossRef] [PubMed]
- Tepper, O.M.; Rudy, H.L.; Lefkowitz, A.; Weimer, K.A.; Marks, S.M.; Stern, C.S.; Garfein, E.S. Mixed reality with hololens: Wherevirtual reality meets augmented reality in the operating room. Plast. Reconstr. Surg. 2017, 140, 1066–1070. [Google Scholar] [CrossRef]
- Cho, K.H.; Yanof, J.; Schwarz, G.S.; West, K.; Gharb, B.B.; Papay, F.A. Holographic surgical planning andtelementoring for craniofacial surgery. Plast. Reconstr. Surg.—Glob Open 2019, 7, 43–44. [Google Scholar] [CrossRef]
- Nuri, T.; Mitsuno, D.; Otsuki, Y.; Ueda, K. Augmented reality technology for the positioning of the auricle in the treatment of microtia. Plast. Reconstr. Surg.—Glob Open 2020, 8, e2626. [Google Scholar] [CrossRef] [PubMed]
- Mischkowski, R.A.; Zinser, M.J.; Kübler, A.C.; Krug, B.; Seifert, U.; Zöller, J.E. Application of an augmented reality tool for maxillary positioning in orthognathic surgery—A feasibility study. J. Cranio-Maxillofac. Surg. 2006, 34, 478–483. [Google Scholar] [CrossRef] [PubMed]
- Iseki, H.; Masutani, Y.; Iwahara, M.; Tanikawa, T.; Muragaki, Y.; Taira, T.; Dohi, T.; Takakura, K. Volumegraph (overlaid three-dimensional image-guided navigation). Clinical application of augmented reality in neurosurgery. Stereotact. Funct. Neurosurg. 1997, 68, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Marescaux, J.; Rubino, F.; Arenas, M.; Mutter, D.; Soler, L. Augmented-Reality–Assisted Laparoscopic Adrenalectomy. JAMA 2004, 292, 2211–2215. [Google Scholar] [CrossRef]
- Wong, K.; Yee, H.M.; Xavier, B.A.; Grillone, G.A. Applications of Augmented Reality in Otolaryngology: A Systematic Review. Otolaryngol.–Head Neck Surg. 2018, 159, 956–967. [Google Scholar] [CrossRef]
- Yang, D.L.; Xu, Q.W.; Che, X.M.; Wu, J.S.; Sun, B. Clinical evaluation and follow-up outcome of presurgical plan by Dextroscope: A prospective controlled study in patients with skull base tumors. Surg. Neurol. 2009, 72, 682–689. [Google Scholar] [CrossRef]
- Mazur, T.; Mansour, T.R.; Mugge, L.; Medhkour, A. Virtual Reality-Based Simulators for Cranial Tumor Surgery: A Systematic Review. World Neurosurg. 2018, 110, 414–422. [Google Scholar] [CrossRef]
- Wang, H.; Wang, F.; Leong, A.P.Y.; Xu, L.; Chen, X.; Wang, Q. Precision insertion of percutaneous sacroiliac screws using a novel augmented reality-based navigation system: A pilot study. Int. Orthop. 2016, 40, 1941–1947. [Google Scholar] [CrossRef]
- Wu, X.; Liu, R.; Yu, J.; Xu, S.; Yang, C.; Yang, S.; Shao, Z.; Ye, Z. Mixed Reality Technology Launches in Orthopedic Surgery for Comprehensive Preoperative Management of Complicated Cervical Fractures. Surg. Innov. 2018, 25, 421–422. [Google Scholar] [CrossRef]
- Verhey, J.T.; Haglin, J.M.; Verhey, E.M.; Hartigan, D.E. Virtual, augmented, and mixed reality applications in orthopedic surgery. Int. J. Med. Robot. Comput. Assist. Surg. 2020, 16, e2067. [Google Scholar] [CrossRef] [PubMed]
- Jin, C.; Dai, L.; Wang, T. The application of virtual reality in the training of laparoscopic surgery: A systematic review and meta-analysis. Int. J. Surg. 2021, 87, 105859. [Google Scholar] [CrossRef]
- Villanueva, C.; Xiong, J.; Rajput, S. Simulation-based surgical education in cardiothoracic training. ANZ J. Surg. 2020, 90, 978–983. [Google Scholar] [CrossRef] [PubMed]
- Cao, C.; Cerfolio, R.J. Virtual or Augmented Reality to Enhance Surgical Education and Surgical Planning. Thorac. Surg. Clin. 2019, 29, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Panel, P.; Neveu, M.E.; Villain, C.; Debras, F.; Fernandez, H.; Debras, E. Hysteroscopic resection on virtual reality simulator: What do we measure? J. Gynecol. Obstet. Hum. Reprod. 2018, 47, 247–252. [Google Scholar] [CrossRef]
- Barsom, E.Z.; Graafland, M.; Schijven, M.P. Systematic review on the effectiveness of augmented reality applications in medical training. Surg. Endosc. 2016, 30, 4174–4183. [Google Scholar] [CrossRef]
- Zhang, J.; Lu, V.; Khanduja, V. The impact of extended reality on surgery: A scoping review. Int. Orthop. 2023, 47, 1–11. [Google Scholar] [CrossRef]
- Klasson, S.; Svensson, H.; Malm, K.; Wassélius, J.; Velander, P. Preoperative CT angiography versus Doppler ultrasound mapping of abdominal perforator in DIEP breast reconstructions: A randomized prospective study. J. Plast. Reconstr. Aesthet. Surg. 2015, 68, 782–786. [Google Scholar] [CrossRef]
- Shaw, R.J.; Batstone, M.D.; Blackburn, T.K.; Brown, J.S. Preoperative Doppler assessment of perforator anatomy in the anterolat-eral thigh flap. Br. J. Oral. Maxillofac. Surg. 2010, 48, 419–422. [Google Scholar] [CrossRef] [PubMed]
- Stekelenburg, C.M.; Sonneveld, P.M.; Bouman, M.B.; van der Wal, M.B.; Knol, D.L.; de Vet, H.C.; van Zuijlen, P.P. The hand held Doppler device for the detection of perforators in reconstructive surgery: What you hear is not always what you get. Burns 2014, 40, 1702–1706. [Google Scholar] [CrossRef]
- Blondeel, P.N.; Beyens, G.; Verhaeghe, R.; Van Landuyt, K.; Tonnard, P.; Monstrey, S.J.; Matton, G. Doppler flow-metry in the planning of perforator flaps. Br. J. Plast. Surg. 1998, 51, 202–209. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | Year | Institution | Publication Type | Surgical Stage | Procedure | Device | Software | Aim | Conclusion |
|---|---|---|---|---|---|---|---|---|---|
| Waked | 2022 | Department of Plastic and Reconstructive Surgery, University Hospital Brussel, Brussels, Belgium | Workflow description | Intraoperative | Facial artery mapping | Smartphone | Not reported | Test application and determine the accuracy of an AR app for visualizing patient-specific facial arterial anatomy | AR tool accurately visualized patient facial arterial anatomy and can contribute to safer dermal injections |
| Cho | 2021 | Department of Plastic Surgery, Cleveland Clinic | Workflow description | Preoperative | Facial vascularized composite allotransplantation | HoloLens | Unity platform and Visual Studio | Describe an AR workflow for use in facial transplantation | AR proved to be a time and cost saver, with the potential for pre- and intraoperative use |
| Garcia-Mato | 2021 | Departamento de Bioingenieria E Ingenieria Aerospacial, Universidad Carlos III De Madrid | Workflow description | Intraoperative | Metopic Craniosynostosis | Smartphone | Custom AR application based on the Unity platform (version 2019.3) | Develop AR preoperative planning method for craniosynostosis repair | AR workflow was successful both in practice and in real cases for assisting craniosynostosis repair |
| Mespreuve | 2021 | Department of Plastic and Reconstructive Surgery, University Hospital Brussel | Workflow description | Intraoperative | Dermal filler injection | Smartphone | Not reported | Examine the viability of pairing magnetic resonance angiography (MRA) with AR to visualize facial anatomy and avoid filler injection injuries | MRA and AR dual workflow was largely successful in identifying facial vasculature, and the proof of concept was successful |
| Coelho | 2020 | Santa Marcelina Hospital | Workflow description | Preoperative | Metopic Craniosynostosis | Smartphone | Custom AR application built using Unity framework and ARCore | Develop AR preoperative planning method for craniosynostosis repair | Their AR workflow can be used to visualize patient-specific anatomy |
| Wesselius | 2020 | Department of Oral and Maxillofacial Surgery, Radboud University Medical Center | Workflow description | Intraoperative | Deep inferior epigastric perforator (DIEP) flap | HoloLens | In-house developed HoloLens application (using Unity framework) | Describe an AR workflow designed to visualize vessels for a DIEP flap | Their AR workflow can be used to visualize patient-specific anatomy |
| Yaremenko | 2020 | Department of Maxillofacial Surgery, Pavlov University | Case report and workflow description | Intraoperative | Auricular reconstruction | Epson Moverio BT-300 | Not reported | Examine the use of AR for microtia correction | AR was useful in visualizing anatomy and conducting a microtia correction |
| Amini | 2019 | Department of Computer Science and Software Engineering, Concordia University | Workflow description | Preoperative | Single Mastectomy | HoloLens | Custom AR application built using Unity version 2018.1.0 and the Vuforia SDK Engine. | Present an augmented reality application, which enables surgeons to see the shape of the implants, as 3D holograms on the patient’s body. | AR can be used to model 3D objects in real time with some subject education |
| Giacalone | 2019 | Department of Lymphatic Surgery, Sint-Maarten Hospital | Workflow description and Case report | Preoperative | Lymphovenous Anastomosis | Medicalholodeck | Custom VR application using Medicalholodeck platform and software | Describe a VR workflow designed to preoperatively plan a lymphatic malformation repair | VR workflow was successful in visualizing complex anatomy in streamlining the operation |
| Pratt | 2018 | Department of Surgery and Cancer, Imperial College London | Case series and workflow description | Intraoperative | Deep inferior epigastric perforator (DIEP) flap | HoloLens | Custom AR application based on the Unity platform (version 2017.1) | Describe an AR workflow designed to visualize vessels for a DIEP flap and demonstrate accuracy in patients | AR workflow was demonstrated to be accurate in viewing patient anatomy and assisting in DIEP procedures |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaplan, N.; Marques, M.; Scharf, I.; Yang, K.; Alkureishi, L.; Purnell, C.; Patel, P.; Zhao, L. Virtual Reality and Augmented Reality in Plastic and Craniomaxillofacial Surgery: A Scoping Review. Bioengineering 2023, 10, 480. https://doi.org/10.3390/bioengineering10040480
Kaplan N, Marques M, Scharf I, Yang K, Alkureishi L, Purnell C, Patel P, Zhao L. Virtual Reality and Augmented Reality in Plastic and Craniomaxillofacial Surgery: A Scoping Review. Bioengineering. 2023; 10(4):480. https://doi.org/10.3390/bioengineering10040480
Chicago/Turabian StyleKaplan, Nicolas, Mitchell Marques, Isabel Scharf, Kevin Yang, Lee Alkureishi, Chad Purnell, Pravin Patel, and Linping Zhao. 2023. "Virtual Reality and Augmented Reality in Plastic and Craniomaxillofacial Surgery: A Scoping Review" Bioengineering 10, no. 4: 480. https://doi.org/10.3390/bioengineering10040480