

Pallidal Recordings in Chronically Implanted Dystonic Patients: Mitigation of Tremor-Related Artifacts
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects, Surgery, and Clinical Evaluation
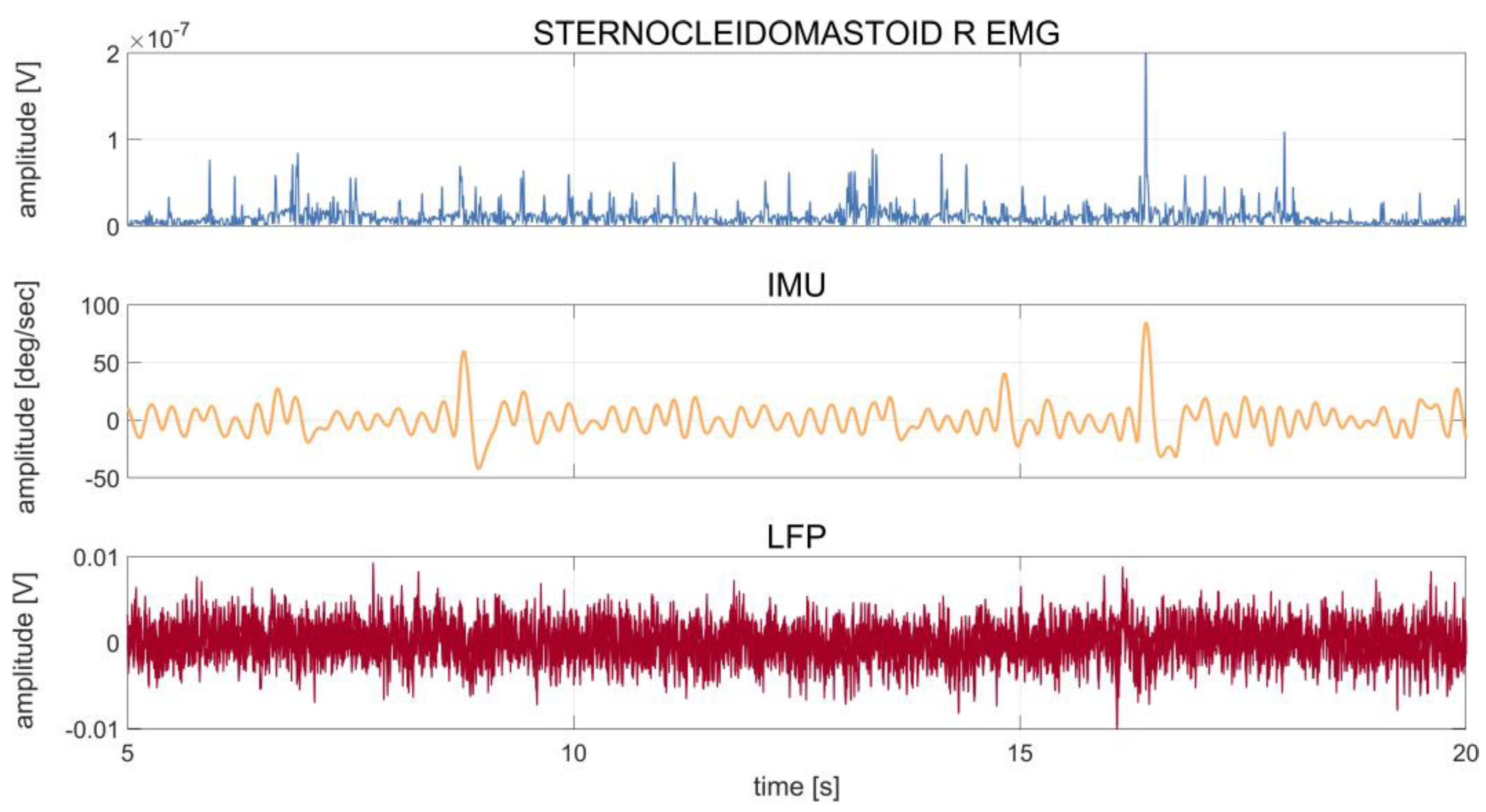
2.2. Experimental Setup and Recordings
2.3. Data Analysis
2.3.1. Data Preprocessing
2.3.2. Spectral Analyses
2.3.3. Assessment of Tremor-Artifacts in LFP Recording and Comparison of IMU vs. EMG Regression Analysis
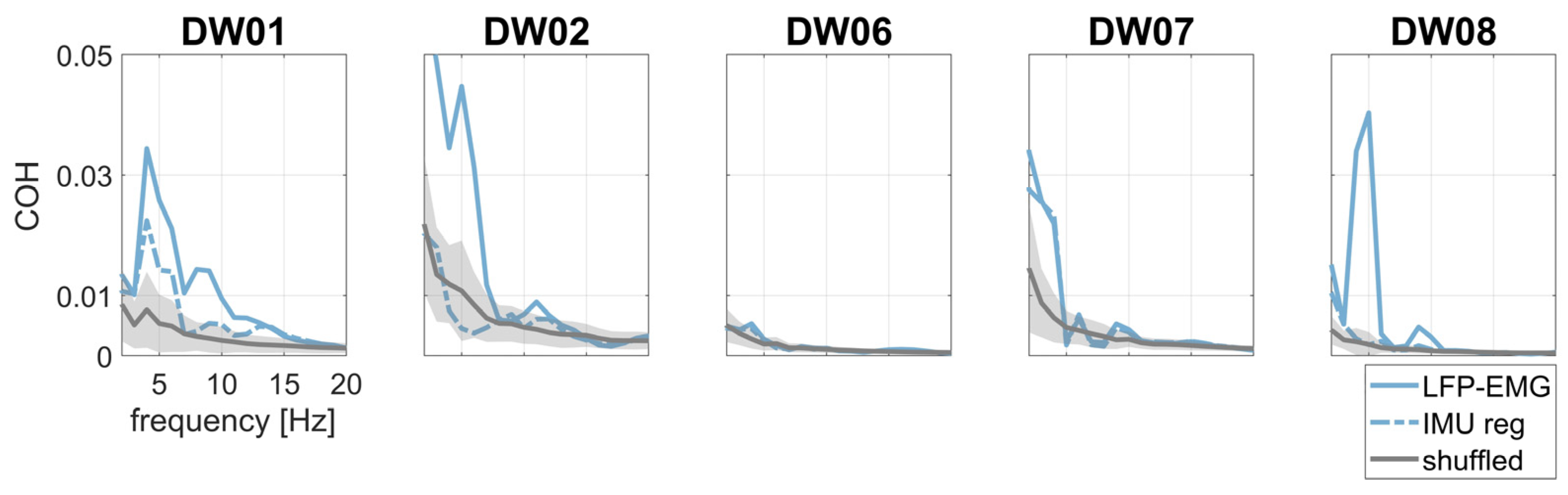
2.3.4. Evaluation of Pallido-Muscular Coherence with IMU-Regression
2.3.5. Statistical Analysis
3. Results
3.1. Clinical and Demographic Data
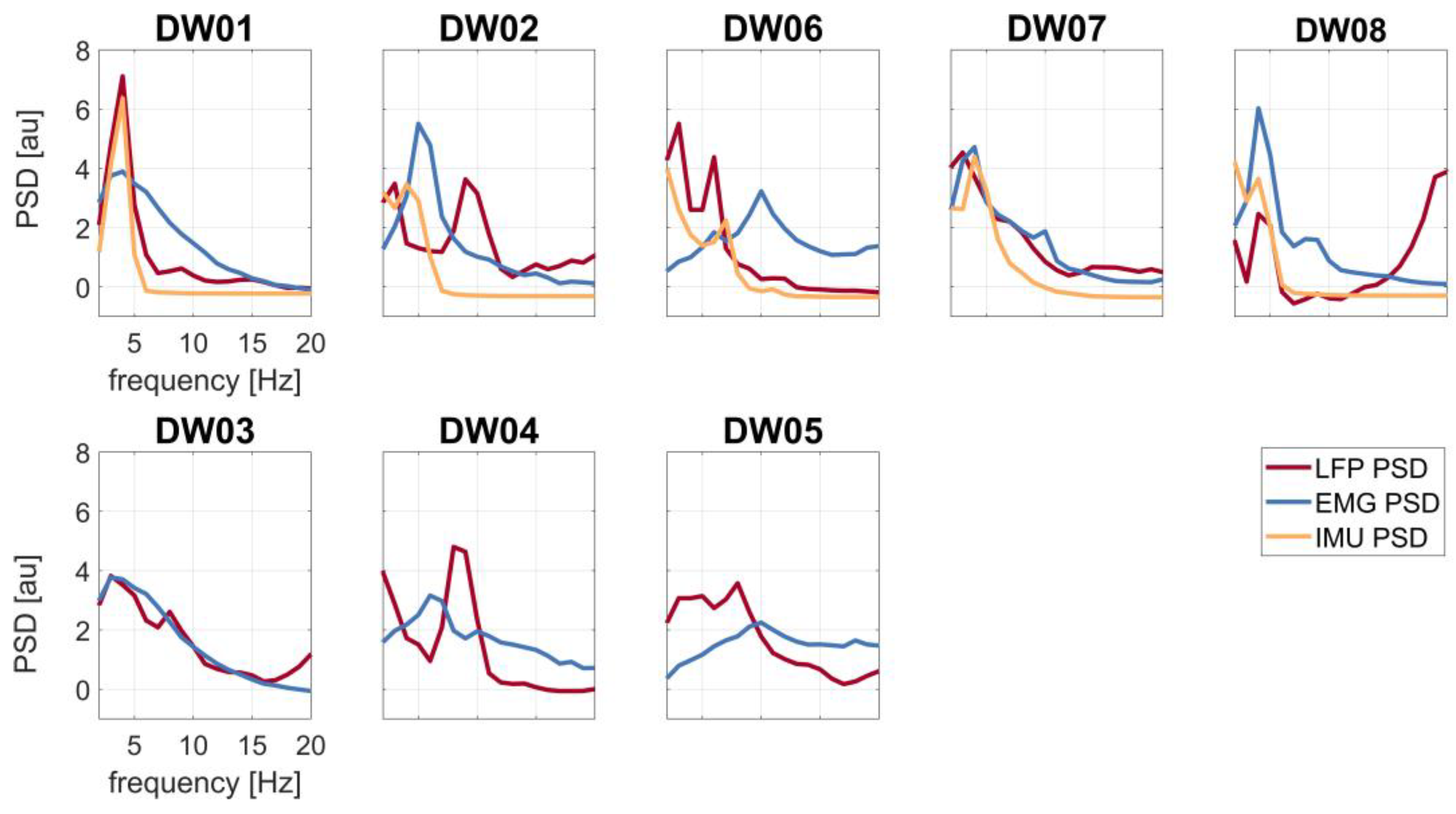
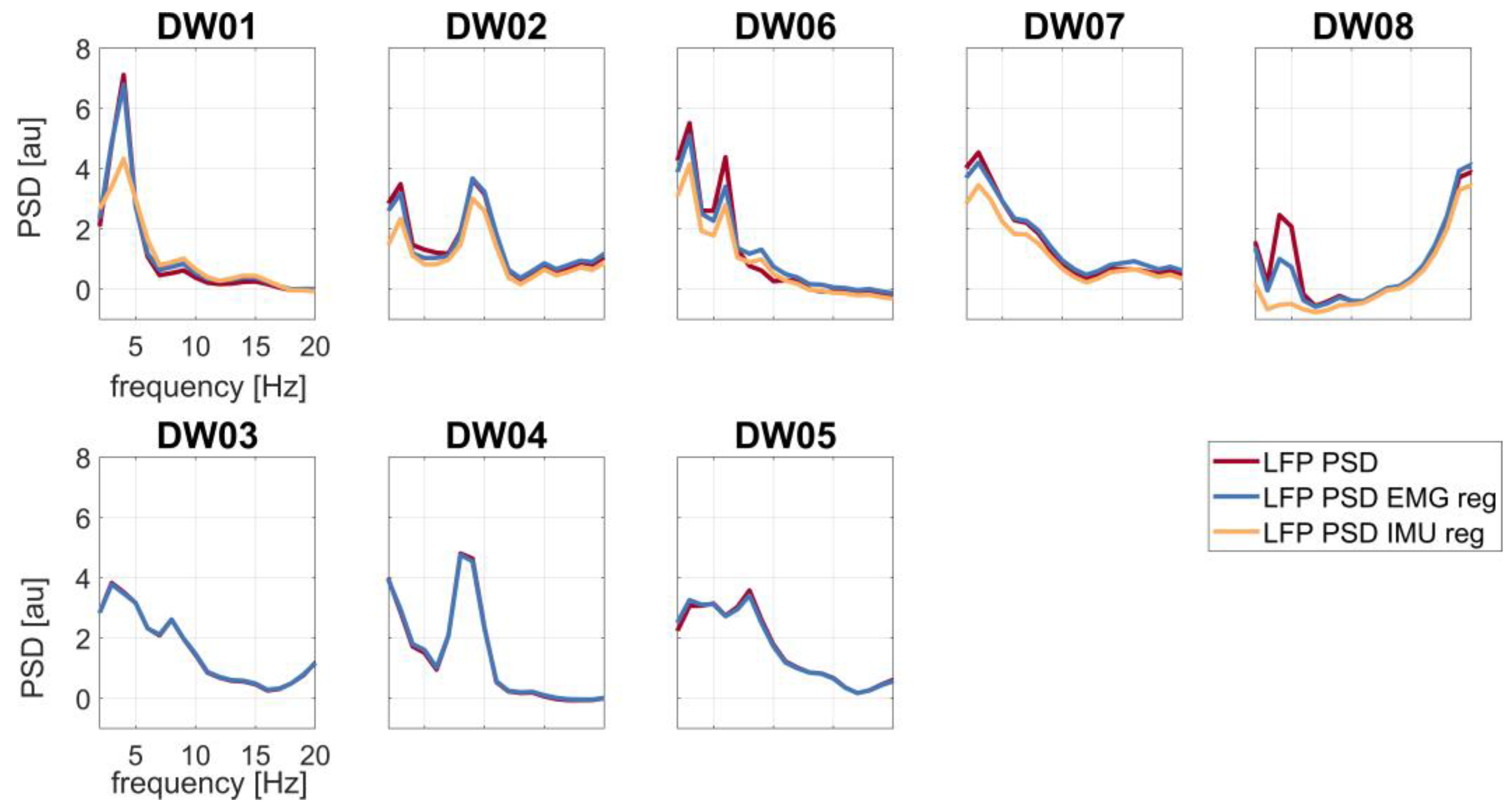
3.2. Tremor Contamination of LFP Recordings and Comparison of IMU vs. EMG Regression Analysis
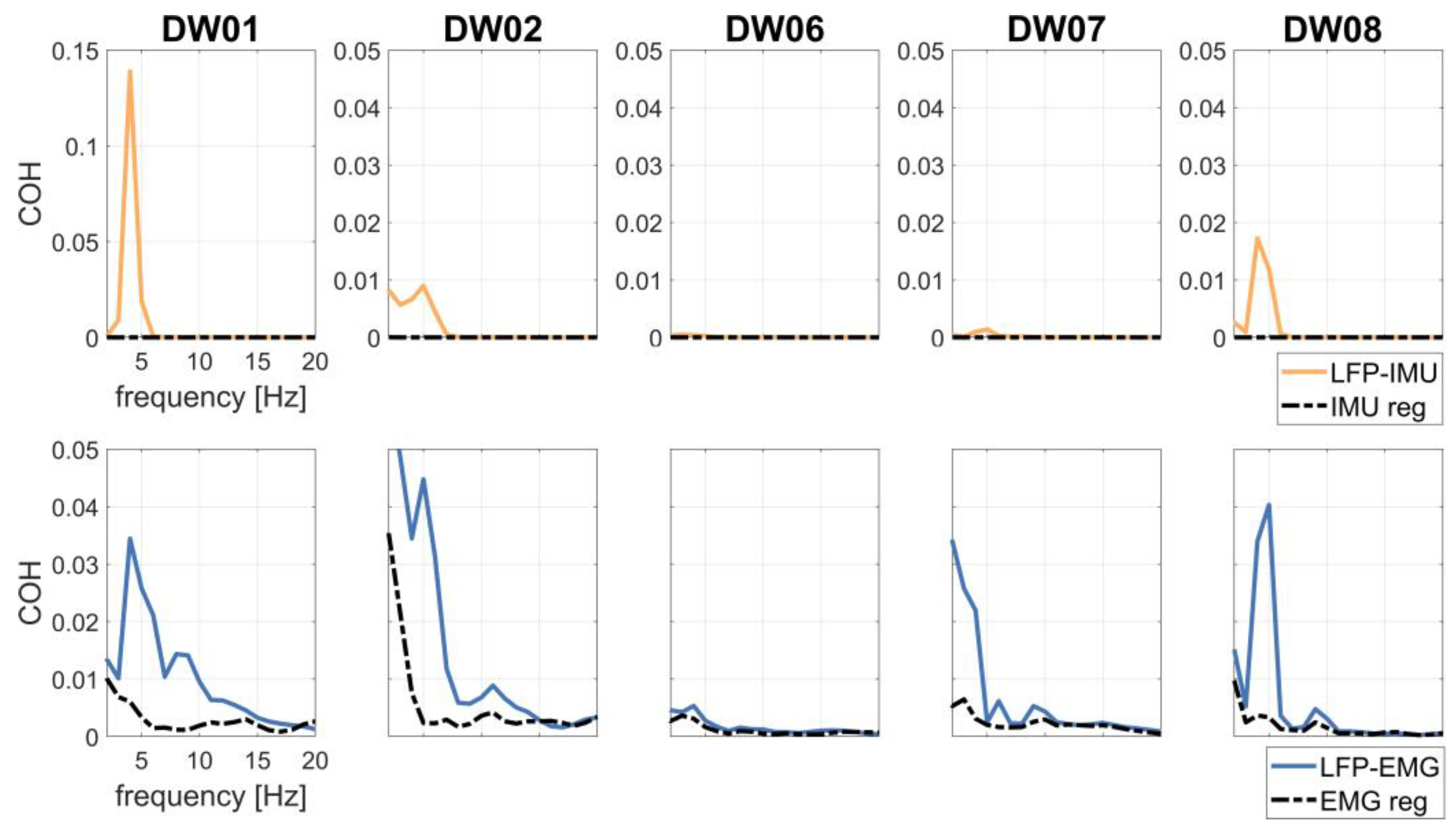
3.3. Pallido-Muscular Coherence after Cleaning
3.4. Sensory Trick and Voluntary Rhythmic Movement
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Albanese, A.; Bhatia, K.; Bressman, S.B.; DeLong, M.R.; Fahn, S.; Fung, V.S.C.; Hallett, M.; Jankovic, J.; Jinnah, H.A.; Klein, C.; et al. Phenomenology and Classification of Dystonia: A Consensus Update: Dystonia: Phenomenology and Classification. Mov. Disord. 2013, 28, 863–873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandey, S.; Sarma, N. Tremor in dystonia. Park. Relat. Disord. 2016, 29, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, A.G.; Beylergil, S.B.; Scorr, L.; Kilic-Berkmen, G.; Freeman, A.; Klein, C.; Junker, J.; Loens, S.; Brüggemann, N.; Münchau, A.; et al. Dystonia and Tremor. Neurology 2021, 96, e563–e574. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, K.P.; Bain, P.; Bajaj, N.; Elble, R.J.; Hallett, M.; Louis, E.D.; Raethjen, J.; Stamelou, M.; Testa, C.M.; Deuschl, G.; et al. Consensus Statement on the classification of tremors. from the task force on tremor of the International Parkinson and Movement Disorder Society: IPMDS Task Force on Tremor Consensus Statement. Mov. Disord. 2018, 33, 75–87. [Google Scholar] [CrossRef]
- Defazio, G.; Conte, A.; Gigante, A.F.; Fabbrini, G.; Berardelli, A. Is tremor in dystonia a phenotypic feature of dystonia? Neurology 2015, 84, 1053. [Google Scholar] [CrossRef]
- Panyakaew, P.; Cho, H.J.; Lee, S.W.; Wu, T.; Hallett, M. The Pathophysiology of Dystonic Tremors and Comparison With Essential Tremor. J. Neurosci. Off. J. Soc. Neurosci. 2020, 40, 9317–9326. [Google Scholar] [CrossRef]
- Hallett, M. Neurophysiology of dystonia: The role of inhibition. Neurobiol. Dis. 2011, 42, 177–184. [Google Scholar] [CrossRef] [Green Version]
- Atkinson-Clement, C.; Pinto, S.; Eusebio, A.; Coulon, O. Diffusion tensor imaging in Parkinson’s disease: Review and meta-analysis. Neuroimage Clin. 2017, 16, 98–110. [Google Scholar] [CrossRef]
- Quartarone, A.; Ruge, D. How Many Types of Dystonia? Pathophysiological Considerations. Front. Neurol. 2018, 9, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Münchau, A.; Schrag, A.; Chuang, C.; MacKinnon, C.D.; Bhatia, K.P.; Quinn, N.P.; Rothwell, J.C. Arm tremor in cervical dystonia differs from essential tremor and can be classified by onset age and spread of symptoms. Brain J. Neurol. 2001, 124, 1765–1776. [Google Scholar] [CrossRef] [Green Version]
- Tinazzi, M.; Fasano, A.; Di Matteo, A.; Conte, A.; Bove, F.; Bovi, T.; Peretti, A.; Defazio, G.; Fiorio, M.; Berardelli, A. Temporal discrimination in patients with dystonia and tremor and patients with essential tremor. Neurology 2013, 80, 76. [Google Scholar] [CrossRef]
- Conte, A.; Ferrazzano, G.; Belvisi, D.; Manzo, N.; Battista, E.; Voti, P.L.; Nardella, A.; Fabbrini, G.; Berardelli, A. Somatosensory temporal discrimination in Parkinson’s disease, dystonia and essential tremor: Pathophysiological and clinical implications. Clin. Neurophysiol. 2018, 129, 1849–1853. [Google Scholar] [CrossRef] [PubMed]
- Cerasa, A.; Nisticò, R.; Salsone, M.; Bono, F.; Salvino, D.; Morelli, M.; Arabia, G.; Quattrone, A. Neuroanatomical correlates of dystonic tremor: A cross-sectional study. Park. Relat. Disord. 2014, 20, 314–317. [Google Scholar] [CrossRef]
- Kirke, D.N.; Battistella, G.; Kumar, V.; Rubien-Thomas, E.; Choy, M.; Rumbach, A.; Simonyan, K. Neural correlates of dystonic tremor: A multimodal study of voice tremor in spasmodic dysphonia. Brain Imaging Behav. 2017, 11, 166–175. [Google Scholar] [CrossRef] [Green Version]
- Madelein van der Stouwe, A.M.; Nieuwhof, F.; Helmich, R.C. Tremor pathophysiology: Lessons from neuroimaging. Curr. Opin. Neurol. 2020, 33, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Tsuboi, T.; Wong, J.K.; Eisinger, R.S.; Okromelidze, L.; Burns, M.R.; Ramirez-Zamora, A.; Almeida, L.; Wagle Shukla, A.; Foote, K.D.; Okun, M.S.; et al. Comparative connectivity correlates of dystonic and essential tremor deep brain stimulation. Brain 2021, 144, 1774–1786. [Google Scholar] [CrossRef] [PubMed]
- Nieuwhof, F.; Panyakaew, P.; van de Warrenburg, B.P.; Gallea, C.; Helmich, R.C. The patchy tremor landscape: Recent advances in pathophysiology. Curr. Opin. Neurol. 2018, 31, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Panyakaew, P.; Jinnah, H.A.; Shaikh, A.G. Clinical features, pathophysiology, treatment, and controversies of tremor in dystonia. J. Neurol. Sci. 2022, 435, 120199. [Google Scholar] [CrossRef]
- DeSimone, J.C.; Archer, D.B.; Vaillancourt, D.E.; Wagle Shukla, A. Network-level connectivity is a critical feature distinguishing dystonic tremor and essential tremor. Brain 2019, 142, 1644–1659. [Google Scholar] [CrossRef] [Green Version]
- van den Berg, K.R.E.; Helmich, R.C. The Role of the Cerebellum in Tremor–Evidence from Neuroimaging. Tremor Hyperkinetic Mov. 2021, 11, 49. [Google Scholar] [CrossRef]
- Ma, H.; Chen, H.; Fang, J.; Gao, L.; Ma, L.; Wu, T.; Hou, Y.; Zhang, J.; Feng, T. Resting-state functional connectivity of dentate nucleus is associated with tremor in Parkinson’s disease. J. Neurol. 2015, 262, 2247–2256. [Google Scholar] [CrossRef]
- Battaglia, S.; Thayer, J.F. Functional interplay between central and autonomic nervous systems in human fear conditioning. Trends Neurosci. 2022, 45, 504–506. [Google Scholar] [CrossRef]
- Ippolito, G.; Bertaccini, R.; Tarasi, L.; Di Gregorio, F.; Trajkovic, J.; Battaglia, S.; Romei, V. The Role of Alpha Oscillations among the Main Neuropsychiatric Disorders in the Adult and Developing Human Brain: Evidence from the Last 10 Years of Research. Biomedicines 2022, 10, 3189. [Google Scholar] [CrossRef] [PubMed]
- Alongi, P.; Iaccarino, L.; Perani, D. PET Neuroimaging: Insights on Dystonia and Tourette Syndrome and Potential Applications. Front. Neurol. 2014, 5, 183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poston, K.L.; Eidelberg, D. Functional brain networks and abnormal connectivity in the movement disorders. NeuroImage 2012, 62, 2261–2270. [Google Scholar] [CrossRef] [Green Version]
- Lehéricy, S.; Tijssen, M.A.J.; Vidailhet, M.; Kaji, R.; Meunier, S. The anatomical basis of dystonia: Current view using neuroimaging. Mov. Disord. 2013, 28, 944–957. [Google Scholar] [CrossRef] [PubMed]
- Carbon, M.; Argyelan, M.; Eidelberg, D. Functional imaging in hereditary dystonia. Eur. J. Neurol. 2010, 17, 58–64. [Google Scholar] [CrossRef] [Green Version]
- Merola, A.; Dwivedi, A.K.; Shaikh, A.G.; Tareen, T.K.; Da Prat, G.A.; Kauffman, M.A.; Hampf, J.; Mahajan, A.; Marsili, L.; Jankovic, J.; et al. Head tremor at disease onset: An ataxic phenotype of cervical dystonia. J. Neurol. 2019, 266, 1844–1851. [Google Scholar] [CrossRef]
- Prudente, C.N.; Stilla, R.; Singh, S.; Buetefisch, C.; Evatt, M.; Factor, S.A.; Freeman, A.; Hu, X.P.; Hess, E.J.; Sathian, K.; et al. A Functional Magnetic Resonance Imaging Study of Head Movements in Cervical Dystonia. Front. Neurol. 2016, 7, 201. [Google Scholar] [CrossRef] [Green Version]
- Filip, P.; Gallea, C.; Lehéricy, S.; Bertasi, E.; Popa, T.; Mareček, R.; Lungu, O.V.; Kašpárek, T.; Vaníček, J.; Bareš, M. Disruption in cerebellar and basal ganglia networks during a visuospatial task in cervical dystonia. Mov. Disord. 2017, 32, 757–768. [Google Scholar] [CrossRef]
- Tsuboi, T.; Jabarkheel, Z.; Foote, K.D.; Okun, M.S.; Wagle Shukla, A. Importance of the initial response to GPi deep brain stimulation in dystonia: A nine year quality of life study. Park. Relat. Disord. 2019, 64, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Sedov, A.; Usova, S.; Semenova, U.; Gamaleya, A.; Tomskiy, A.; Beylergil, S.B.; Jinnah, H.A.; Shaikh, A.G. Pallidal Activity in Cervical Dystonia with and Without Head Tremor. Cerebellum Lond. Engl. 2020, 19, 409–418. [Google Scholar] [CrossRef]
- Kiss, Z.H.T.; Doig-Beyaert, K.; Eliasziw, M.; Tsui, J.; Haffenden, A.; Suchowersky, O. The Canadian multicentre study of deep brain stimulation for cervical dystonia. Brain 2007, 130, 2879–2886. [Google Scholar] [CrossRef]
- Volkmann, J.; Wolters, A.; Kupsch, A.; Müller, J.; Kühn, A.A.; Schneider, G.-H.; Poewe, W.; Hering, S.; Eisner, W.; Müller, J.-U.; et al. Pallidal deep brain stimulation in patients with primary generalised or segmental dystonia: 5-year follow-up of a randomised trial. Lancet Neurol. 2012, 11, 1029–1038. [Google Scholar] [CrossRef]
- Isaias, I.U.; Alterman, R.L.; Tagliati, M. Deep Brain Stimulation for Primary Generalized Dystonia: Long-term Outcomes. Arch. Neurol. 2009, 66, 465–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaelin-Lang, A.; You, H.; Burgunder, J.-M.; Lönnfors-Weitze, T.; Loher, T.J.; Taub, E.; Isaias, I.U.; Krauss, J.K.; Michael Schüpbach, W.M. Bilateral pallidal stimulation improves cervical dystonia for more than a decade. Park. Relat. Disord. 2020, 81, 78–81. [Google Scholar] [CrossRef]
- Tisch, S. Deep brain stimulation in dystonia: Factors contributing to variability in outcome in short and long term follow-up. Curr. Opin. Neurol. 2022, 35, 510–517. [Google Scholar] [CrossRef]
- Isaias, I.U.; Volkmann, J.; Kupsch, A.; Burgunder, J.-M.; Ostrem, J.L.; Alterman, R.L.; Mehdorn, H.M.; Sch?necker, T.; Krauss, J.K.; Starr, P.; et al. Factors predicting protracted improvement after pallidal DBS for primary dystonia: The role of age and disease duration. J. Neurol. 2011, 258, 1469–1476. [Google Scholar] [CrossRef] [PubMed]
- Reich, M.M.; Horn, A.; Lange, F.; Roothans, J.; Paschen, S.; Runge, J.; Wodarg, F.; Pozzi, N.G.; Witt, K.; Nickl, R.C.; et al. Probabilistic mapping of the antidystonic effect of pallidal neurostimulation: A multicentre imaging study. Brain 2019, 142, 1386–1398. [Google Scholar] [CrossRef] [Green Version]
- Vissani, M.; Isaias, I.U.; Mazzoni, A. Deep brain stimulation: A review of the open neural engineering challenges. J. Neural Eng. 2020, 17, 051002. [Google Scholar] [CrossRef] [PubMed]
- Pozzi, N.G.; Isaias, I.U. Adaptive deep brain stimulation: Retuning Parkinson’s disease. Handb. Clin. Neurol. 2022, 184, 273–284. [Google Scholar]
- Neumann, W.; Horn, A.; Ewert, S.; Huebl, J.; Brücke, C.; Slentz, C.; Schneider, G.; Kühn, A.A. A localized pallidal physiomarker in cervical dystonia. Ann. Neurol. 2017, 82, 912–924. [Google Scholar] [CrossRef] [PubMed]
- Piña-Fuentes, D.; van Dijk, J.M.C.; Drost, G.; van Zijl, J.C.; van Laar, T.; Tijssen, M.A.J.; Beudel, M. Direct comparison of oscillatory activity in the motor system of Parkinson’s disease and dystonia: A review of the literature and meta-analysis. Clin. Neurophysiol. 2019, 130, 917–924. [Google Scholar] [CrossRef] [PubMed]
- Zhu, G.-Y.; Zhang, R.-L.; Chen, Y.-C.; Liu, Y.-Y.; Liu, D.-F.; Wang, S.-Y.; Jiang, Y.; Zhang, J.-G. Characteristics of globus pallidus internus local field potentials in generalized dystonia patients with TWNK mutation. Clin. Neurophysiol. 2020, 131, 1453–1461. [Google Scholar] [CrossRef]
- Piña-Fuentes, D.; Beudel, M.; Van Zijl, J.C.; Van Egmond, M.E.; Oterdoom, D.L.M.; Van Dijk, J.M.C.; Tijssen, M.A.J. Low-frequency oscillation suppression in dystonia: Implications for adaptive deep brain stimulation. Park. Relat. Disord. 2020, 79, 105–109. [Google Scholar] [CrossRef]
- Thenaisie, Y.; Palmisano, C.; Canessa, A.; Keulen, B.J.; Capetian, P.; Jiménez, M.C.; Bally, J.F.; Manferlotti, E.; Beccaria, L.; Zutt, R.; et al. Towards adaptive deep brain stimulation: Clinical and technical notes on a novel commercial device for chronic brain sensing. J. Neural Eng. 2021, 18, 042002. [Google Scholar] [CrossRef] [PubMed]
- Sirica, D.; Hewitt, A.L.; Tarolli, C.G.; Weber, M.T.; Zimmerman, C.; Santiago, A.; Wensel, A.; Mink, J.W.; Lizárraga, K.J. Neurophysiological biomarkers to optimize deep brain stimulation in movement disorders. Neurodegener. Dis. Manag. 2021, 11, 315–328. [Google Scholar] [CrossRef] [PubMed]
- Hess, C.W.; Pullman, S.L. Tremor: Clinical Phenomenology and Assessment Techniques. Tremor Hyperkinetic Mov. 2012, 2, 02. [Google Scholar] [CrossRef]
- Lalli, S.; Albanese, A. Dystonic Tremor. In Mechanisms and Emerging Therapies in Tremor Disorders; Grimaldi, G., Manto, M., Eds.; Springer: New York, NY, USA, 2013; pp. 203–218. ISBN 978-1-4614-4026-0. [Google Scholar]
- Volkmann, J.; Mueller, J.; Deuschl, G.; Kühn, A.A.; Krauss, J.K.; Poewe, W.; Timmermann, L.; Falk, D.; Kupsch, A.; Kivi, A.; et al. Pallidal neurostimulation in patients with medication-refractory cervical dystonia: A randomised, sham-controlled trial. Lancet Neurol 2014, 13, 875–884. [Google Scholar] [CrossRef] [PubMed]
- Jost, W.H.; Hefter, H.; Stenner, A.; Reichel, G. Rating scales for cervical dystonia: A critical evaluation of tools for outcome assessment of botulinum toxin therapy. J. Neural Transm. Vienna Austria 1996 2013, 120, 487–496. [Google Scholar] [CrossRef] [Green Version]
- Boyce, M.J.; Canning, C.G.; Mahant, N.; Morris, J.; Latimer, J.; Fung, V.S.C. The Toronto Western Spasmodic Torticollis Rating Scale: Reliability in neurologists and physiotherapists. Park. Relat. Disord. 2012, 18, 635–637. [Google Scholar] [CrossRef] [PubMed]
- Masuhr, F.; Wissel, J.; Müller, J.; Scholz, U.; Poewe, W. Quantification of sensory trick impact on tremor amplitude and frequency in 60 patients with head tremor. Mov. Disord. 2001, 15, 960–964. [Google Scholar] [CrossRef]
- Deuschl, G.; Heinen, F.; Kleedorfer, B.; Wagner, M.; Lücking, C.H.; Poewe, W. Clinical and polymyographic investigation of spasmodic torticollis. J. Neurol. 1992, 239, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Canessa, A.; Palmisano, C.; Isaias, I.U.; Mazzoni, A. Gait-related frequency modulation of beta oscillatory activity in the subthalamic nucleus of parkinsonian patients. Brain Stimul. 2020, 13, 1743–1752. [Google Scholar] [CrossRef] [PubMed]
- Canessa, A.; Pozzi, N.G.; Arnulfo, G.; Brumberg, J.; Reich, M.M.; Pezzoli, G.; Ghilardi, M.F.; Matthies, C.; Steigerwald, F.; Volkmann, J.; et al. Striatal Dopaminergic Innervation Regulates Subthalamic Beta-Oscillations and Cortical-Subcortical Coupling during Movements: Preliminary Evidence in Subjects with Parkinson’s Disease. Front. Hum. Neurosci. 2016, 10, 611. [Google Scholar] [CrossRef] [Green Version]
- Arnulfo, G.; Pozzi, N.G.; Palmisano, C.; Leporini, A.; Canessa, A.; Brumberg, J.; Pezzoli, G.; Matthies, C.; Volkmann, J.; Isaias, I.U. Phase matters: A role for the subthalamic network during gait. PLoS ONE 2018, 13, e0198691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumann, W.-J.; Memarian Sorkhabi, M.; Benjaber, M.; Feldmann, L.K.; Saryyeva, A.; Krauss, J.K.; Contarino, M.F.; Sieger, T.; Jech, R.; Tinkhauser, G.; et al. The sensitivity of ECG contamination to surgical implantation site in brain computer interfaces. Brain Stimul. 2021, 14, 1301–1306. [Google Scholar] [CrossRef] [PubMed]
- Donoghue, T.; Haller, M.; Peterson, E.J.; Varma, P.; Sebastian, P.; Gao, R.; Noto, T.; Lara, A.H.; Wallis, J.D.; Knight, R.T.; et al. Parameterizing Neural Power Spectra into Periodic and Aperiodic Components. Nat. Neurosci. 2020, 23, 1655–1665. [Google Scholar] [CrossRef]
- Barow, E.; Neumann, W.J.; Brücke, C.; Huebl, J.; Horn, A.; Brown, P.; Krauss, J.K.; Schneider, G.H.; Kühn, A.A. Deep brain stimulation suppresses pallidal low frequency activity in patients with phasic dystonic movements. Brain 2014, 137, 3012–3024. [Google Scholar] [CrossRef] [Green Version]
- Sharott, A.; Grosse, P.; Kühn, A.A.; Salih, F.; Engel, A.K.; Kupsch, A.; Schneider, G.H.; Krauss, J.K.; Brown, P. Is the synchronization between pallidal and muscle activity in primary dystonia due to peripheral afferance or a motor drive? Brain 2008, 131, 473–484. [Google Scholar] [CrossRef] [Green Version]
- Haufe, S.; Isaias, I.; Pellegrini, F.; Palmisano, C. Gait event prediction from surface electromyography in parkinsonian patients. medRxiv 2023. [Google Scholar] [CrossRef]
- Schnitzler, A.; Gross, J. Normal and pathological oscillatory communication in the brain. Nat. Rev. Neurosci. 2005, 6, 285–296. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, A.G.; Jinnah, H.A.; Tripp, R.M.; Optican, L.M.; Ramat, S.; Lenz, F.A.; Zee, D.S. Irregularity distinguishes limb tremor in cervical dystonia from essential tremor. J. Neurol. Neurosurg. Psychiatry 2008, 79, 187–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.C.; Kühn, A.A.; Hoffmann, K.T.; Kupsch, A.; Schneider, G.H.; Trottenberg, T.; Krauss, J.K.; Wöhrle, J.C.; Bardinet, E.; Yelnik, J.; et al. Oscillatory pallidal local field potential activity correlates with involuntary EMG in dystonia. Neurology 2006, 66, 418–420. [Google Scholar] [CrossRef]
- Averna, A.; Arlotti, M.; Rosa, M.; Chabardès, S.; Seigneuret, E.; Priori, A.; Moro, E.; Meoni, S. Pallidal and Cortical Oscillations in Freely Moving Patients With Dystonia. Neuromodulation Technol. Neural Interface 2022, S1094715922000162. [Google Scholar] [CrossRef] [PubMed]
- Schramm, A.; Reiners, K.; Naumann, M. Complex mechanisms of sensory tricks in cervical dystonia. Mov. Disord. 2004, 19, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Steeves, T.D.; Day, L.; Dykeman, J.; Jette, N.; Pringsheim, T. The prevalence of primary dystonia: A systematic review and meta-analysis. Mov. Disord. Off. J. Mov. Disord. Soc. 2012, 27, 1789–1796. [Google Scholar] [CrossRef]
- Ortiz, R.M.; Scheperjans, F.; Pekkonen, E. Deep brain stimulation for dystonia in Finland during 2007–2016. BMC Neurol. 2019, 19, 137. [Google Scholar] [CrossRef] [Green Version]
- Scheller, U.; Lofredi, R.; Wijk, B.C.M.; Saryyeva, A.; Krauss, J.K.; Schneider, G.; Kroneberg, D.; Krause, P.; Neumann, W.; Kühn, A.A. Pallidal low-frequency activity in dystonia after cessation of long-term deep brain stimulation. Mov. Disord. 2019, 34, 1734–1739. [Google Scholar] [CrossRef]
- Popov, T.; Tröndle, M.; Baranczuk, Z.; Pfeiffer, C.; Haufe, S.; Langer, N. Test–retest reliability of resting-state EEG in young and older adults. Psychophysiology 2023, e14268. [Google Scholar] [CrossRef]
- Pellegrini, F.; Delorme, A.; Nikulin, V.; Haufe, S. Identifying best practices for detecting inter-regional functional connectivity from EEG. bioRxiv 2022. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | DW01 (T+) | DW02 (T+) | DW06 (T+) | DW07 * (T+) | DW08 (T+) | DW03 * (T−) | DW04 * (T−) | DW05 (T−) | |
|---|---|---|---|---|---|---|---|---|---|
| Sex | F | F | F | F | F | M | M | F | |
| Age | 52 | 44 | 57 | 50 | 33 | 74 | 62 | 65 | |
| Age at onset, years | 38 | 36 | 42 | Childhood | Childhood | 42 | Childhood | Childhood | |
| Age at surgery | 50 | 43 | 56 | 48 ** | 31 | 72 ** | 62 ** | 63 | |
| Disease | CD | CD | CD | MFD | DM | CD | DM | DM | |
| TWSTRS pre-DBS, score | 18 | 19 | 13 | NA | 22 | 22 | NA | 18 | |
| TWSTRS post-DBS, score | Stim-off | 16 | 18 | 8 | 17 | 19 | 16 | 21 | 18 |
| TWSTRS post-DBS, score | Stim-on | 15 | 14 | 6 | 8 | NA | 5 | 13 | 6 |
| Patient | LFP θ-α Power | LFP θ-α Power EMG Reg (Δ) | LFP θ-α Power IMU Reg (Δ) | LFP-EMG θ-α COH | LFP-EMG θ-α COH—IMU Reg (Δ) |
|---|---|---|---|---|---|
| DW01 | 17.84 | 17.93 (−0.09) | 15.01 (2.83) | 0.015 | 0.008 (0.007) |
| DW02 | 8.16 | 7.03 (1.13) | 4.50 (3.66) | 0.020 | 0.007 (0.013) |
| DW06 | 14.34 | 12.85 (1.49) | 9.78 (4.56) | 0.002 | 0.002 (0) |
| DW07 | 14.56 | 13.70 (0.86) | 10.59 (3.97) | 0.007 | 0.007 (0) |
| DW08 | 6.07 | 2.66 (3.41) | −2.21 (8.28) | 0.010 | 0.002 (0.008) |
| DW03 | 16.32 | 16.22 (0.10) | NA | NA | NA |
| DW04 | 11.06 | 10.88 (0.18) | NA | NA | NA |
| DW05 | 7.33 | 8.00 (0.67) | NA | NA | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Del Vecchio Del Vecchio, J.; Hanafi, I.; Pozzi, N.G.; Capetian, P.; Isaias, I.U.; Haufe, S.; Palmisano, C. Pallidal Recordings in Chronically Implanted Dystonic Patients: Mitigation of Tremor-Related Artifacts. Bioengineering 2023, 10, 476. https://doi.org/10.3390/bioengineering10040476
Del Vecchio Del Vecchio J, Hanafi I, Pozzi NG, Capetian P, Isaias IU, Haufe S, Palmisano C. Pallidal Recordings in Chronically Implanted Dystonic Patients: Mitigation of Tremor-Related Artifacts. Bioengineering. 2023; 10(4):476. https://doi.org/10.3390/bioengineering10040476
Chicago/Turabian StyleDel Vecchio Del Vecchio, Jasmin, Ibrahem Hanafi, Nicoló Gabriele Pozzi, Philipp Capetian, Ioannis U. Isaias, Stefan Haufe, and Chiara Palmisano. 2023. "Pallidal Recordings in Chronically Implanted Dystonic Patients: Mitigation of Tremor-Related Artifacts" Bioengineering 10, no. 4: 476. https://doi.org/10.3390/bioengineering10040476