
A Comparative Study on Predication of Appropriate Mechanical Ventilation Mode through Machine Learning Approach
 , , , , ,
, , , , ,
Abstract
:1. Introduction
1.1. Ventilation Modes: Origin to Today
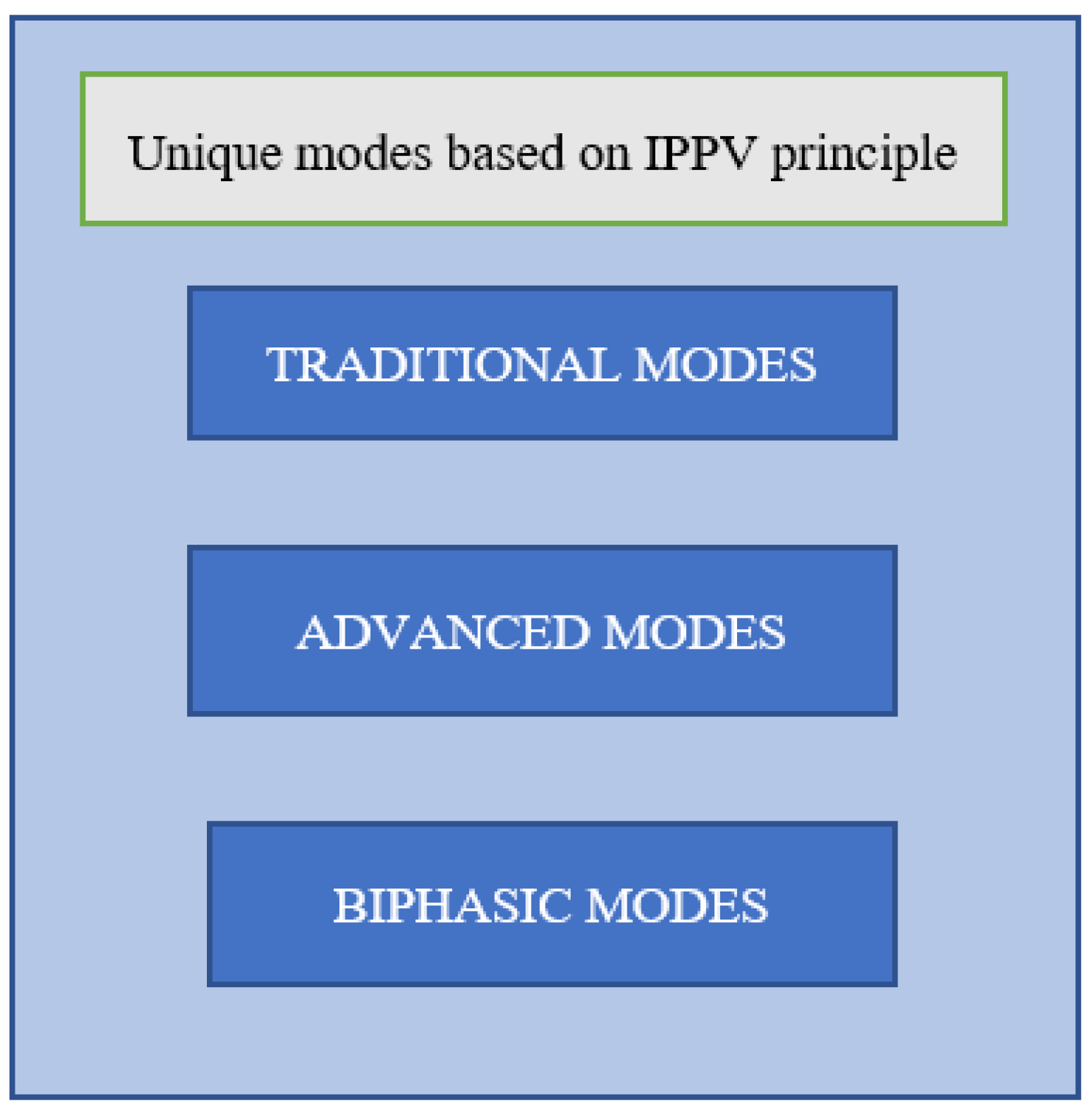
1.2. Unique Modes of Mechanical Ventilation
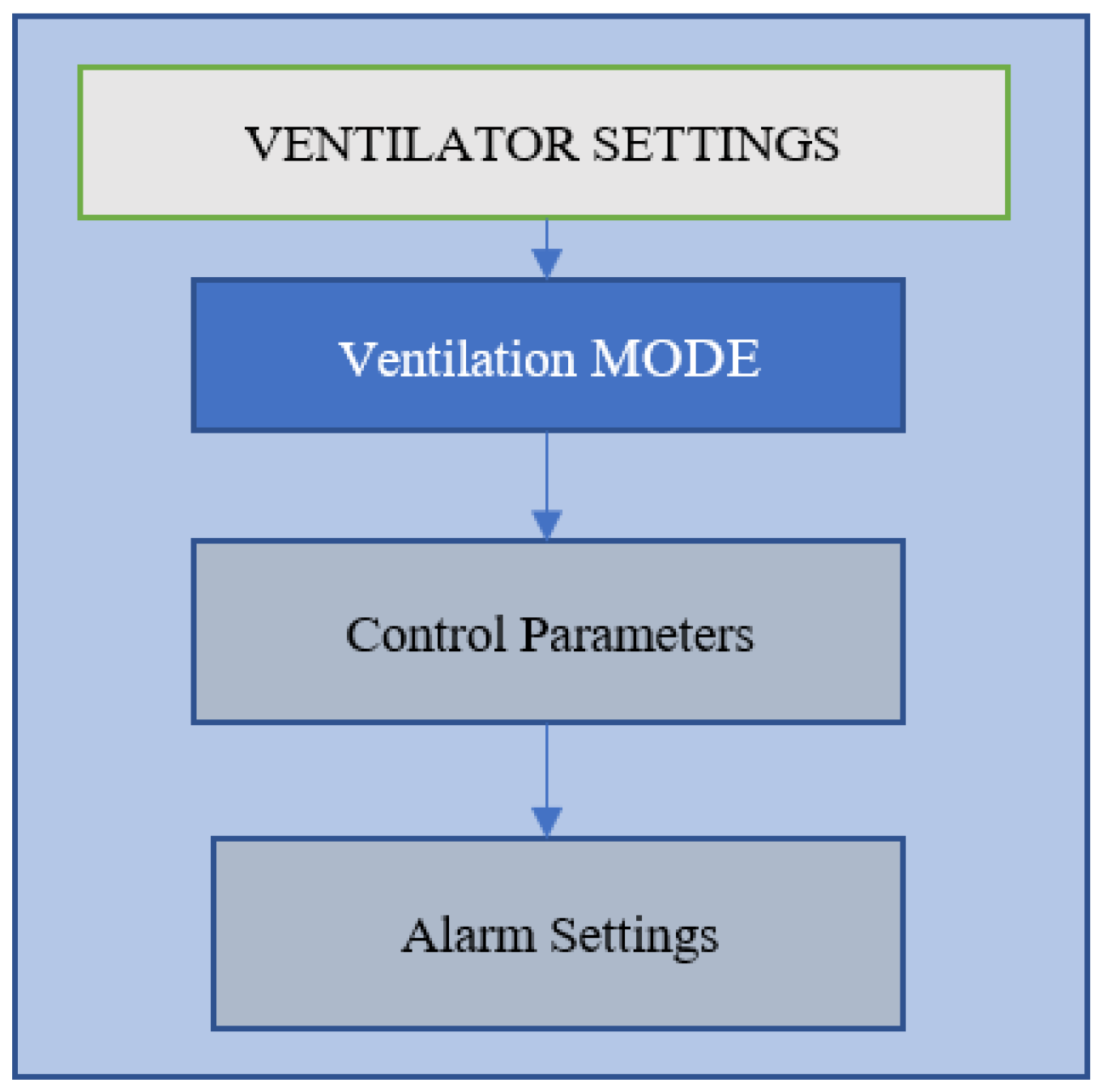
1.3. Ventilation Mode: Control Parameters
2. Material and Methods
2.1. Data Collection
2.2. Data Preprocessing
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chakkarapani, A.A.; Adappa, R.; Mohammad Ali, S.K.; Gupta, S.; Soni, N.B.; Chicoine, L.; Hummler, H.D. Current concepts in assisted mechanical ventilation in the neonate—Part 2: Understanding various modes of mechanical ventilation and recommendations for individualized disease-based approach in neonates. Int. J. Pediatr. Adolesc. Med. 2020, 7, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Sternbach, G.L.; Fromm, R.E., Jr.; Varon, J. Mechanical ventilation: Past and present. J. Emerg. Med. 1998, 16, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Garnero, A.J.; Abbona, H.; Gordo-Vidal, F.; Hermosa-Gelbard, C.; Grupo de Insuficiencia Respiratoria Aguda de SEMICYUC. Pressure versus volume controlled modes in invasive mechanical ventilation. Med. Intensiv. 2013, 37, 292–298. [Google Scholar] [CrossRef]
- Chatburn, R.L.; Primiano, F.P., Jr. A new system for understanding modes of mechanical ventilation. Respir. Care 2001, 46, 604–621. [Google Scholar]
- Lei, Y. Ventilation Modes ABC. 2019. Available online: https://college.hamilton-medical.com/auth/RepositoryEntry/ (accessed on 3 July 2022).
- Rose, L. Clinical application of ventilator modes: Ventilatory strategies for lung protection. Aust. Crit. Care 2010, 23, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Pham, T.; Brochard, L.J.; Slutsky, A.S. Mechanical Ventilation: State of the Art. Mayo Clin. Proc. 2017, 92, 1382–1400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talavera-Llames, R.; Pérez-Chacón, R.; Troncoso, A.; Martínez-Álvarez, F. MV-kWNN: A novel multivariate and multi-output weighted nearest neighbours algorithm for big data time series forecasting. Neurocomputing 2019, 353, 56–73. [Google Scholar] [CrossRef]
- Talavera-Llames, R.; Pérez-Chacón, R.; Troncoso, A.; Martínez-Álvarez, F. Big data time series forecasting based on nearest neighbours distributed computing with Spark. Knowl. Based Syst. 2018, 161, 12–25. [Google Scholar] [CrossRef]
- Meyfroidt, G.; Güiza, F.; Ramon, J.; Bruynooghe, M. Machine learning techniques to examine large patient databases. Best Pract. Res. Clin. Anaesthesiol. 2009, 23, 127–143. [Google Scholar] [CrossRef] [Green Version]
- Peine, A.; Hallawa, A.; Bickenbach, J.; Hallawa, A.; Bickenbach, J.; Dartmann, G.; Fazlic, L.B.; Schmeink, A.; Ascheid, G.; Thiemermann, C.; et al. Development and validation of a reinforcement learning algorithm to dynamically optimize mechanical ventilation in critical care. NPJ Digit. Med. 2021, 4, 32. [Google Scholar] [CrossRef]
- Walls, R.; Hockberger, R.; Gausche-Hill, M. Rosen’s Emergency Medicine; Elsevier Health Sciences: Mumbai, India, 2018. [Google Scholar]
- Archambault, P.M.; St-Onge, M. Invasive and Noninvasive Ventilation in the Emergency Department. Emerg. Med. Clin. N. Am. 2012, 30, 421–449. [Google Scholar] [CrossRef] [PubMed]
- The National Heart, Lung, and Blood Institute PETAL Clinical Trials Network. Early Neuromuscular Blockade in the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2019, 380, 1997–2008. [Google Scholar] [CrossRef] [PubMed]
- Wright, B.J. Lung-protective Ventilation Strategies and Adjunctive Treatments for the Emergency Medicine Patient with Acute Respiratory Failure. Emerg. Med. Clin. N. Am. 2014, 32, 871–887. [Google Scholar] [CrossRef] [PubMed]
- Weingart, S.D. Managing Initial Mechanical Ventilation in the Emergency Department. Ann. Emerg. Med. 2016, 68, 614–617. [Google Scholar] [CrossRef] [PubMed]
- Fan, E.; Del Sorbo, L.; Goligher, E.C.; Hodgson, C.L.; Munshi, L.; Walkey, A.J.; Adhikari NK, J.; Amato MB, P.; Branson, R.; Brower, R.G.; et al. An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2017, 195, 1253–1263. [Google Scholar] [CrossRef] [PubMed]
- Curley, G.F.; Laffey, J.G.; Zhang, H.; Slutsky, A.S. Biotrauma and Ventilator-Induced Lung Injury. Chest 2016, 150, 1109–1117. [Google Scholar] [CrossRef] [PubMed]
- Weiss, C.H.; McSparron, J.I.; Chatterjee, R.S.; Herman, D.; Fan, E.; Wilson, K.C.; Thomson, C.C. Summary for Clinicians: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome Clinical Practice Guideline. Ann. Am. Thorac. Soc. 2017, 14, 1235–1238. [Google Scholar] [CrossRef]
- Papazian, L.; Aubron, C.; Brochard, L.; Chiche, J.D.; Combes, A.; Dreyfuss, D.; Forel, J.M.; Guérin, C.; Jaber, S.; Mekontso-Dessap, A.; et al. Formal guidelines: Management of acute respiratory distress syndrome. Ann. Intensive Care 2019, 9, 69. [Google Scholar] [CrossRef] [Green Version]
- Goligher, E.C.; Ferguson, N.D.; Brochard, L.J. Clinical challenges in mechanical ventilation. Lancet 2016, 387, 1856–1866. [Google Scholar] [CrossRef]
- Loo, N.; Chiew, Y.; Tan, C.; Arunachalam, G.; Ralib, A.; Mat-Nor, M.B. A machine learning model for real-time asynchronous breathing monitoring. IFAC-PapersOnLine 2018, 51, 378–383. [Google Scholar] [CrossRef]
- Zhang, L.; Mao, K.; Duan, K.; Fang, S.; Lu, Y.; Gong, Q.; Lu, F.; Jiang, Y.; Jiang, L.; Fang, W.; et al. Detection of patient-ventilator asynchrony from mechanical ventilation waveforms using a two-layer long short-term memory neural network. Comput. Biol. Med. 2020, 120, 103721. [Google Scholar] [CrossRef] [PubMed]
- Gholami, B.; Phan, T.S.; Haddad, W.M.; Cason, A.; Mullis, J.; Price, L.; Bailey, J.M. Replicating human expertise of mechanical ventilation waveform analysis in detecting patient-ventilator cycling asynchrony using machine learning. Comput. Biol. Med. 2018, 97, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Parreco, J.; Hidalgo, A.; Parks, J.J.; Kozol, R.; Rattan, R. Using artificial intelligence to predict prolonged mechanical ventilation and tracheostomy placement. J. Surg. Res. 2018, 228, 179–187. [Google Scholar] [CrossRef]
- Yuan, K.C.; Tsai, L.W.; Lee, K.H.; Cheng, Y.W.; Hsu, S.C.; Lo, Y.S.; Chen, R.J. The development an artificial intelligence algorithm for early sepsis diagnosis in the intensive care unit. Int. J. Med. Inform. 2020, 141, 104176. [Google Scholar] [CrossRef] [PubMed]
- Hezarjaribi, N.; Dutta, R.; Xing, T.; Murdoch, G.K.; Mazrouee, S.; Mortazavi, B.J.; Ghasemzadeh, H. Monitoring Lung Mechanics during Mechanical Ventilation using Machine Learning Algorithms. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2018, 2018, 1160–1163. [Google Scholar] [CrossRef]
- Chen, T.; Xu, J.; Ying, H.; Chen, X.; Feng, R.; Fang, X.; Gao, H.; Wu, J. Prediction of Extubation Failure for Intensive Care Unit Patients Using Light Gradient Boosting Machine. IEEE Access 2019, 7, 150960–150968. [Google Scholar] [CrossRef]
- Fabregat, A.; Magret, M.; Ferré, J.A.; Vernet, A.; Guasch, N.; Rodríguez, A.; Gómez, J.; Bodí, M. A Machine Learning decision-making tool for extubation in Intensive Care Unit patients. Comput. Methods Programs Biomed. 2021, 200, 105869. [Google Scholar] [CrossRef] [PubMed]
- Shuzan, M.N.I.; Chowdhury, M.H.; Chowdhury, M.E.H.; Murugappan, M.; Bhuiyan, E.H.; Ayari, M.A.; Khandakar, A. Machine Learning-Based Respiration Rate and Blood Oxygen Saturation Estimation Using Photoplethysmogram Signals. Bioengineering 2023, 10, 167. [Google Scholar] [CrossRef]
- Poli, J.A.; Howard, C.; Garcia, A.J., III; Remboski, D.; Littlewood, P.B.; Kress, J.P.; Kasthuri, N.; Comai, A.; Soni, K.; Kennedy, P.; et al. Performance Characteristics of a Novel 3D-Printed Bubble Intermittent Mandatory Ventilator (B-IMV) for Adult Pulmonary Support. Bioengineering 2022, 9, 151. [Google Scholar] [CrossRef]
- Sauki, M.; Sa’adah, N.; Damanhuri, N.S.; Othman, N.A.; Meng, B.C.C.; Chiew, Y.S.; Nor, M.B.M. Assessing the Asynchrony Event Based on the Ventilation Mode for Mechanically Ventilated Patients in ICU. Bioengineering 2021, 8, 222. [Google Scholar] [CrossRef]
- Venkata, O.; Sarma, S.; Koenig, A.; Pidaparti, R.M. Mechanical Ventilator Parameter Estimation for Lung Health through Machine Learning. Bioengineering 2021, 8, 60. [Google Scholar] [CrossRef] [PubMed]
- Murias, G.; Montanya, J.; Chacón, E.; Estruga, A.; Subirà, C.; Fernández, R.; Sales, B.; de Haro, C.; Lopez-Aguilar, J.; Lucangelo, U.; et al. Automatic detection of ventilatory modes during invasive mechanical ventilation. Crit. Care 2016, 20, 258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rittayamai, N.; Katsios, C.M.; Beloncle, F.; Friedrich, J.O.; Mancebo, J.; Brochard, L. Pressure-Controlled vs Volume-Controlled Ventilation in Acute Respiratory Failure: A Physiology-Based Narrative and Systematic Review. Chest 2015, 148, 340–355. [Google Scholar] [CrossRef] [PubMed]
- Rehm, G.B.; Kuhn, B.T.; Nguyen, J.; Anderson, N.R.; Chuah, C.N.; Adams, J.Y. Improving Mechanical Ventilator Clinical Decision Support Systems with a Machine Learning Classifier for Determining Ventilator Mode. Stud. Health Technol. Inform. 2019, 264, 318–322. [Google Scholar] [CrossRef]
- Müller, A.; Karathanasopoulos, N.; Roth, C.C.; Mohr, D. Machine Learning Classifiers for Surface Crack Detection in Fracture Experiments. Int. J. Mech. Sci. 2021, 209, 106698. [Google Scholar] [CrossRef]
- Qi, C.; Tang, X. Slope stability prediction using integrated metaheuristic and machine learning approaches: A comparative study. Comput. Ind. Eng. 2018, 118, 112–122. [Google Scholar] [CrossRef]
- Han, Q.; Gui, C.; Xu, J.; Lacidogna, G. A generalized method to predict the compressive strength of high-performance concrete by improved random forest algorithm. Constr. Build. Mater. 2019, 226, 734–742. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Traditional Modes | Advanced Modes | Biphasic Modes |
|---|---|---|
| Continuous mandatory ventilation (CMV) Synchronized intermittent mandatory ventilation (SIMV) Support mode | Proportional assist ventilation (PAV) Proportional pressure support (PPS) Adaptive support ventilation (ASV) Automatic controller of oxygen Neutrally adjusted ventilatory assist IntelliVent SmartCare | Continuous positive airway pressure (CPAP) DuoPAP mode Airway pressure release ventilation (APRV) |
| Controls for Ventilation | Controls for Adequate Oxygenation | Controls for Patient–Ventilator Synchronization |
|---|---|---|
| Inspiratory Tidal Volume [VTi (ml)] | Fraction of inspired oxygenation FiO2 (%) | Trigger sensitivity |
| Mandatory breaths per minute [ f (rpm)] | Positive end expiratory pressure | Patient trigger (pressure or flow) |
| Inspiratory time (s) I:E ratio (inspiratory to expiratory time ratio) Pressure control (cm H2O) Pressure support (cm H2O) | [PEEP (cm H2O)] | Flow cycle |
| N | Minimum | Maximum | Mean | Std. Deviation | Variance | Skewness | Kurtosis | ||
|---|---|---|---|---|---|---|---|---|---|
| Statistic | Statistic | Statistic | Statistic | Statistic | Statistic | Statistic | Std.Error | Statistic | Std.Error |
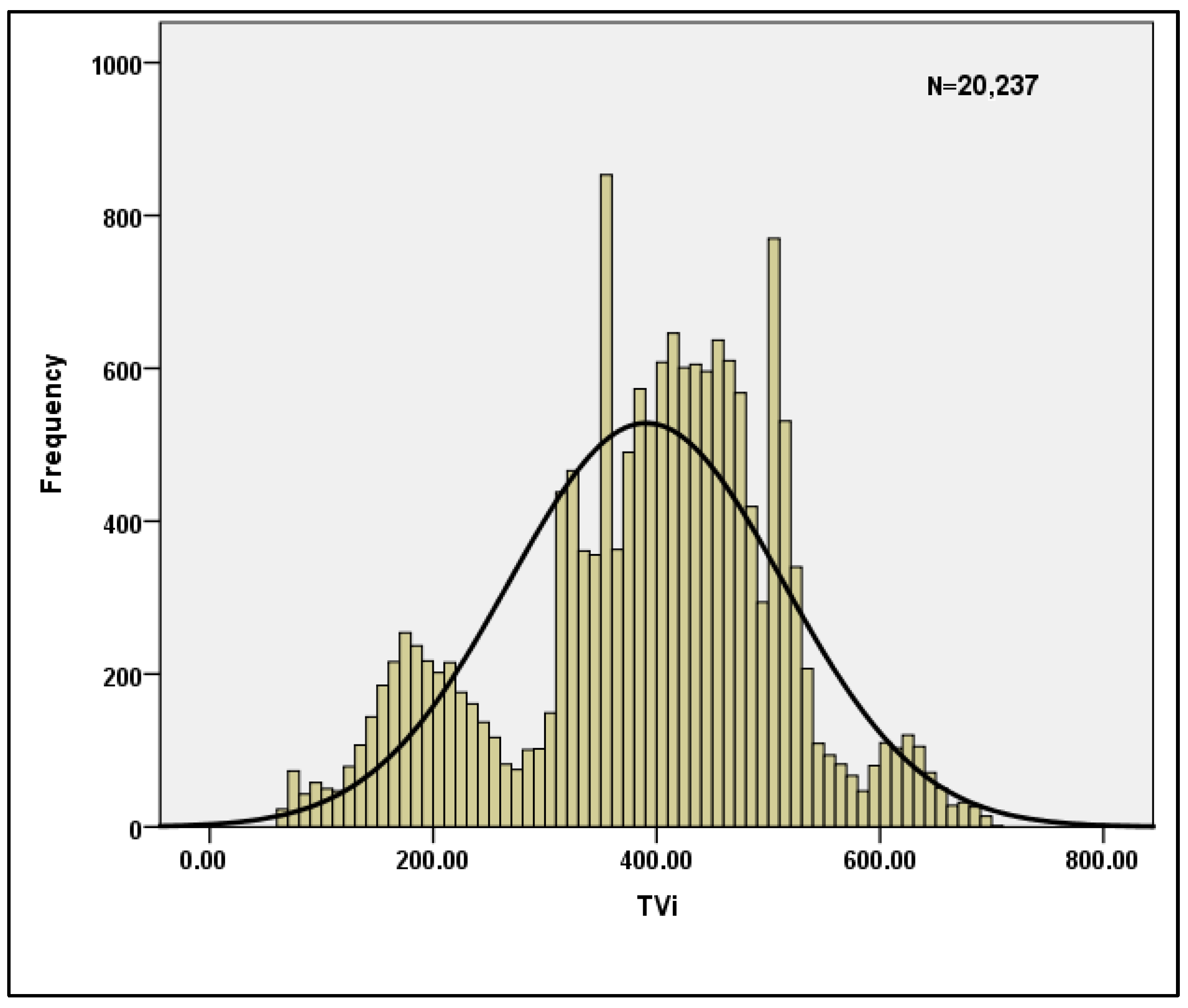
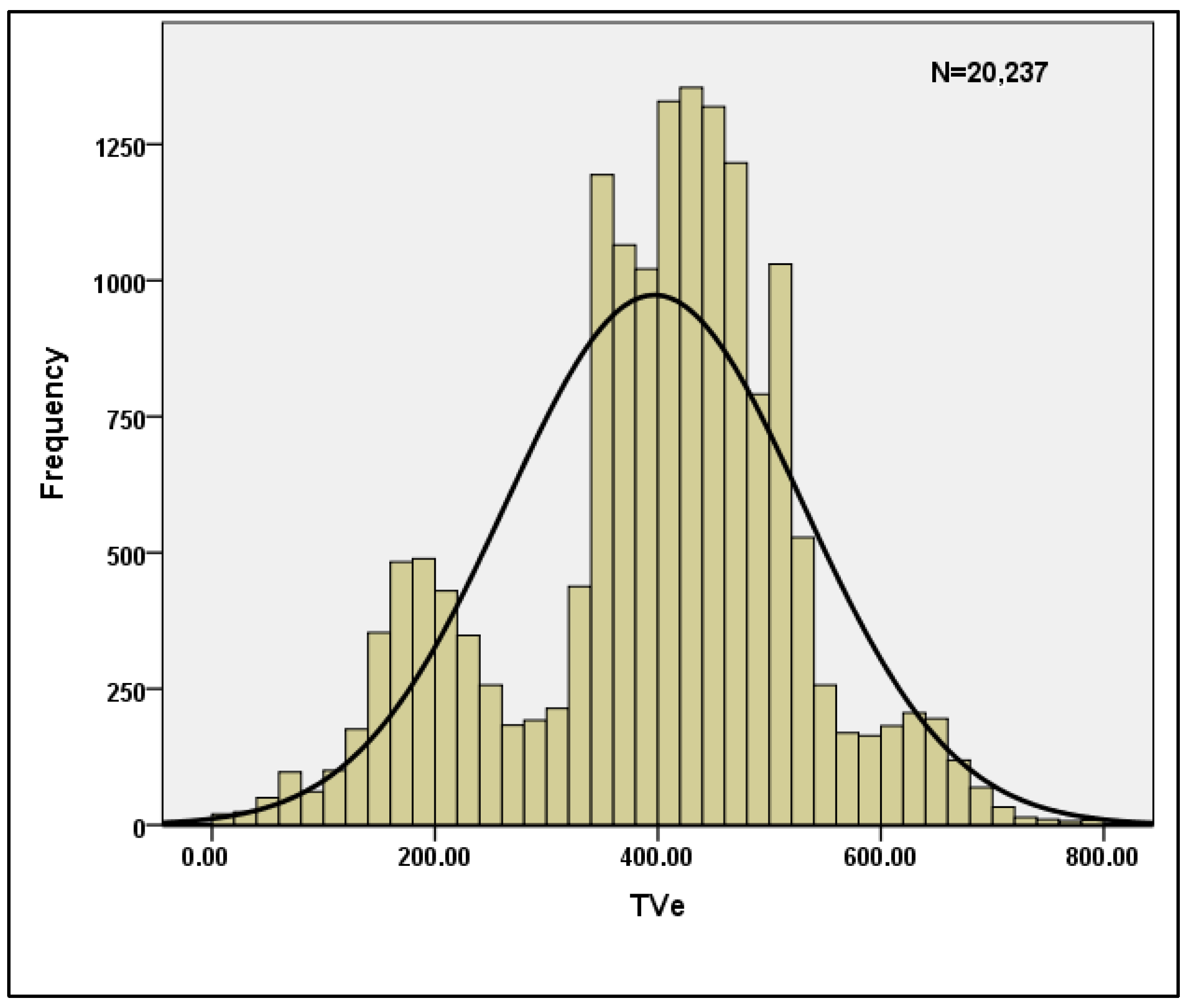
| 20,237 | 61.00 | 700.00 | 390.6240 | 122.65019 | 15,043.069 | 0.421 | 0.019 | 0.104 | 0.038 |
| 20,237 | 1.00 | 1170.00 | 396.7983 | 133.21416 | 17,746.013 | 0.164 | 0.019 | 0.873 | 0.038 |
| 20,237 | 0.23 | 14.51 | 7.4352 | 3.05062 | 9.306 | 0.666 | 0.019 | 1.067 | 0.038 |
| 20,237 | 0.15 | 36.80 | 11.5536 | 7.29206 | 53.174 | 0.805 | 0.019 | 0.736 | 0.038 |
| 20,237 | 0.28 | 14.51 | 7.4459 | 3.05173 | 9.313 | 0.664 | 0.019 | 1.081 | 0.038 |
| Reliability Statistics | Hotelling’s T-Squared Test | ||||||
|---|---|---|---|---|---|---|---|
| Cronbach’s Alpha | Cronbach’s Alpha Based on Standardized Items | N of Items | Hotelling’s T-Squared | F | df1 | df2 | Sig |
| 0.787 | 0.89 | 5 | 168,373.607 | 42,085.629 | 4 | 20,237 | 0 |
| TVi | TVe | PEEPprev | Pmin | PEEP | |
|---|---|---|---|---|---|
| TVi | 1 | 0.174 ** | 0.095 ** | 0.272 ** | 0.014 |
| TVe | 0.174 ** | 1 | 0.287 ** | 0.039 | 0.403 ** |
| PEEPprev | 0.095 ** | 0.287 ** | 1 | 0.502 ** | 0.035 |
| Pmin | 0.272 ** | 0.039 | 0.502 ** | 1 | 0.082 ** |
| PEEP | 0.014 | 0.403 ** | 0.035 | 0.082 ** | 1 |
| ML Algorithm | Parameters | Definition | Value |
|---|---|---|---|
| Random-Forest | criterion | Quality measurement of a split. | Gini |
| n_estimators | The number of trees in the forest | 0–100 | |
| Logistic Regression | tol | Tolerance for stopping criteria. | 10−4 |
| C_inverse | Inverse of regularization strength. | 1.0 | |
| max_iter | Max iterations taken for solvers to converge. | 100 | |
| Support Vector Machine | penalty | Specifies the norm used in penalization. | l2 1000 |
| max_iter | Max number of iterations to be run. | ||
| C | Regularization parameter. | ||
| Guassian Naive Bayes | var_smoothing | Portion of largest variance including | 0.1 10−9 |
| all features added to variances for | |||
| stability calculation. | |||
| K Nearest Neighbors | n_neighbors | Number of neighbors to be used. Weight function to be used. Algorithm used to compute the nearest neighbors. | 5 uniform auto |
| weights | |||
| algorithm | |||
| Decision-Tree | criterion | Quality measurement of a split. Strategy used to choose the split at each node. | Gini best |
| splitter |
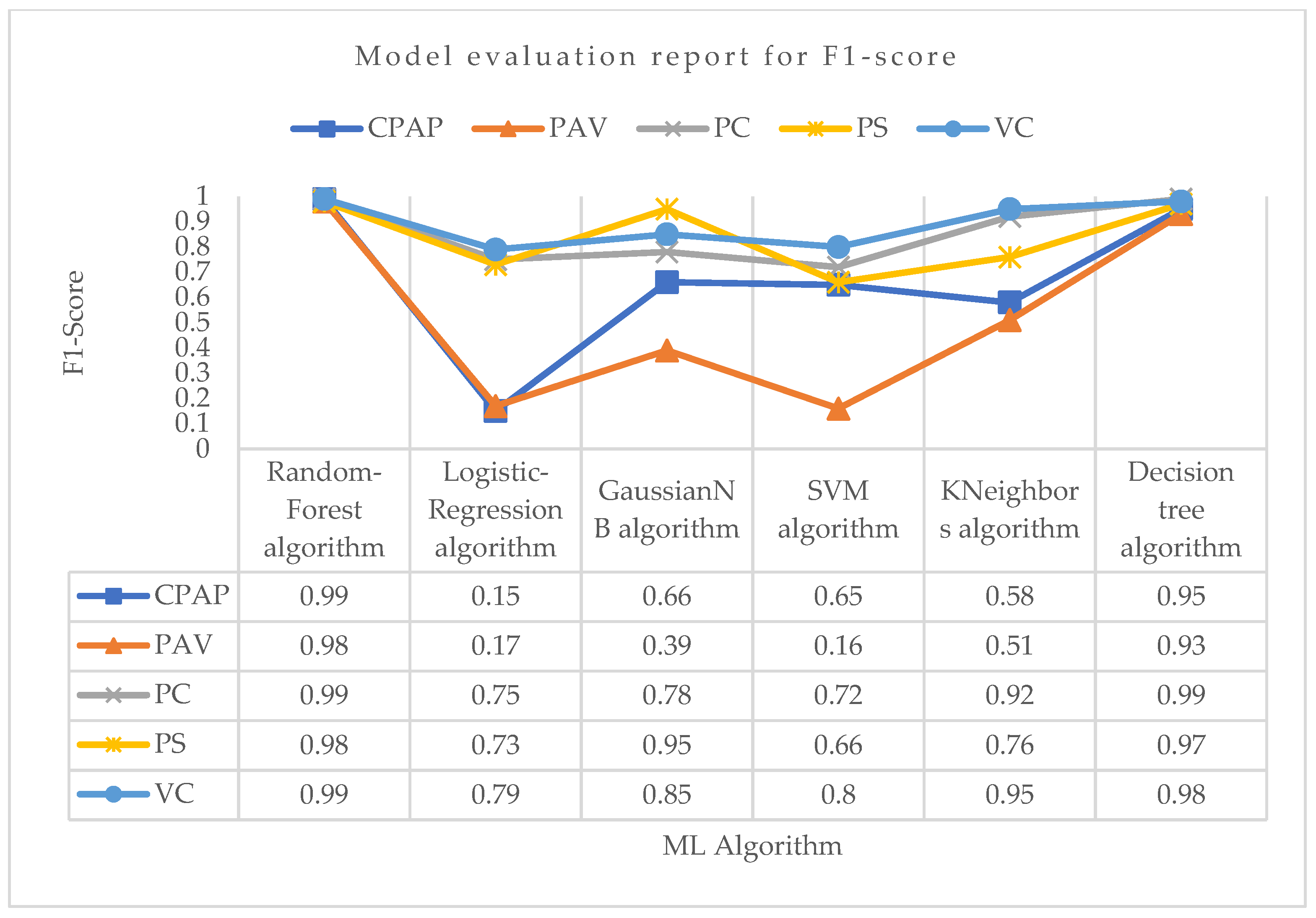
| Modes | Precision | Recall | F1-Score | ||
|---|---|---|---|---|---|
| Training | Testing | Overall | |||
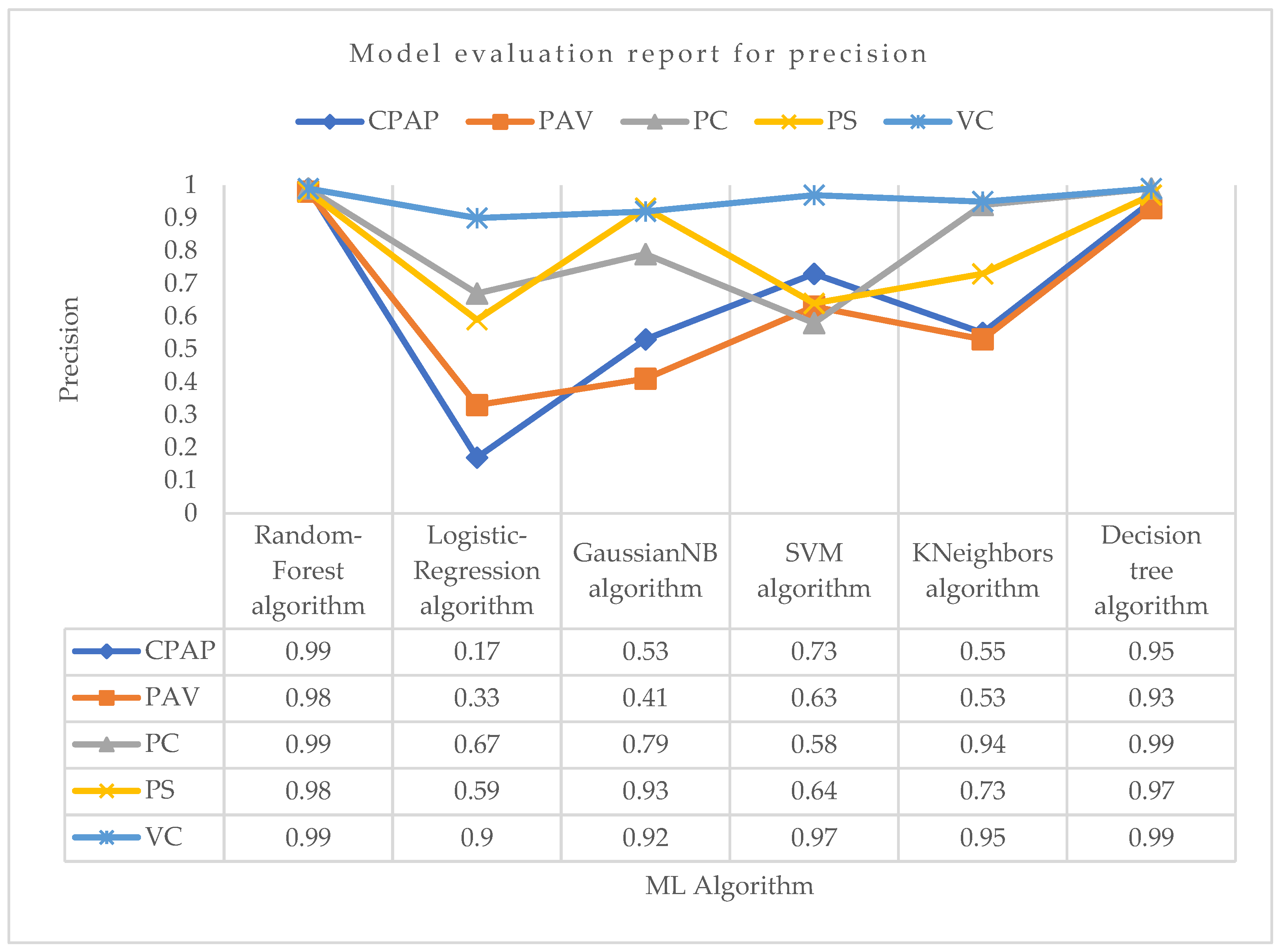
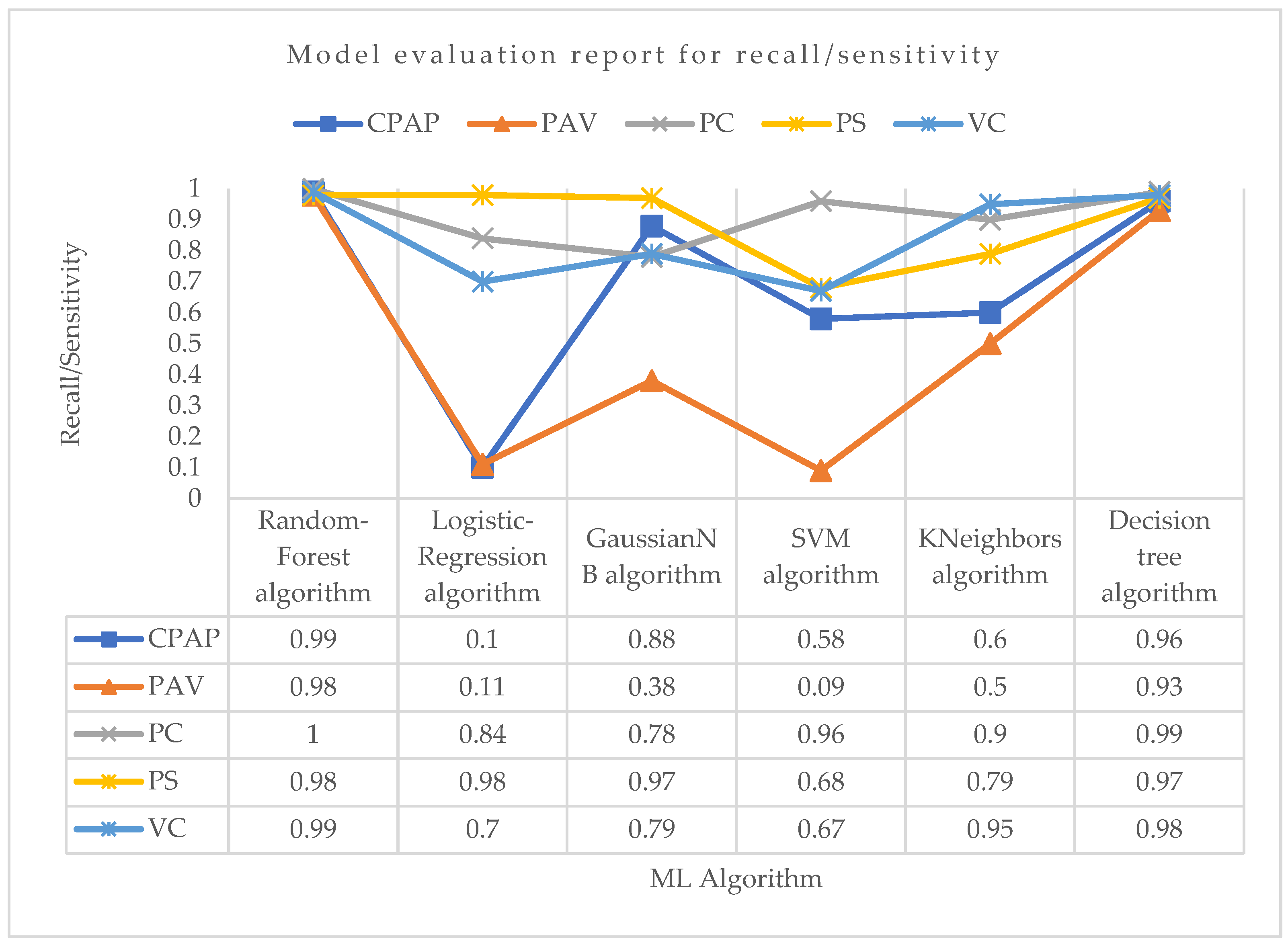
| CPAP | 0.99 | 0.99 | 0.98 | 0.99 | 0.99 |
| PAV | 0.98 | 0.97 | 0.99 | 0.98 | 0.98 |
| PC | 0.99 | 0.99 | 1.0 | 1.0 | 0.99 |
| PS | 0.98 | 0.97 | 0.99 | 0.98 | 0.98 |
| VC | 0.99 | 0.99 | 0.98 | 0.99 | 0.99 |
| Modes | Precision | Recall | F1-Score | ||
|---|---|---|---|---|---|
| Training | Testing | Overall | |||
| CPAP | 0.17 | 0.09 | 0.11 | 0.10 | 0.15 |
| PAV | 0.33 | 0.11 | 0.10 | 0.11 | 0.17 |
| PC | 0.67 | 0.82 | 0.85 | 0.84 | 0.75 |
| PS | 0.59 | 0.99 | 0.98 | 0.98 | 0.73 |
| VC | 0.90 | 0.71 | 0.69 | 0.70 | 0.79 |
| Modes | Precision | Recall | F1-Score | ||
|---|---|---|---|---|---|
| Training | Testing | Overall | |||
| CPAP | 0.53 | 0.87 | 0.88 | 0.88 | 0.66 |
| PAV | 0.41 | 0.36 | 0.39 | 0.38 | 0.39 |
| PC | 0.79 | 0.77 | 0.79 | 0.78 | 0.78 |
| PS | 0.93 | 0.96 | 0.99 | 0.97 | 0.95 |
| VC | 0.92 | 0.78 | 0.79 | 0.79 | 0.85 |
| Modes | Precision | Recall | F1-Score | ||
|---|---|---|---|---|---|
| Training | Testing | Overall | |||
| CPAP | 0.73 | 0.59 | 0.57 | 0.58 | 0.65 |
| PAV | 0.63 | 0.08 | 0.09 | 0.09 | 0.16 |
| PC | 0.58 | 0.95 | 0.97 | 0.96 | 0.72 |
| PS | 0.64 | 0.67 | 0.69 | 0.68 | 0.66 |
| VC | 0.97 | 0.66 | 0.68 | 0.67 | 0.80 |
| Modes | Precision | Recall | F1-Score | ||
|---|---|---|---|---|---|
| Training | Testing | Overall | |||
| CPAP | 0.55 | 0.61 | 0.59 | 0.60 | 0.58 |
| PAV | 0.53 | 0.51 | 0.49 | 0.50 | 0.51 |
| PC | 0.94 | 0.92 | 0.89 | 0.90 | 0.92 |
| PS | 0.73 | 0.78 | 0.80 | 0.79 | 0.76 |
| VC | 0.95 | 0.96 | 0.95 | 0.95 | 0.95 |
| Modes | Precision | Recall | F1-Score | ||
|---|---|---|---|---|---|
| Training | Testing | Overall | |||
| CPAP | 0.95 | 0.94 | 0.96 | 0.96 | 0.95 |
| PAV | 0.93 | 0.91 | 0.94 | 0.93 | 0.93 |
| PC | 0.99 | 0.98 | 0.99 | 0.99 | 0.99 |
| PS | 0.97 | 0.96 | 0.98 | 0.97 | 0.97 |
| VC | 0.99 | 0.99 | 0.98 | 0.98 | 0.98 |
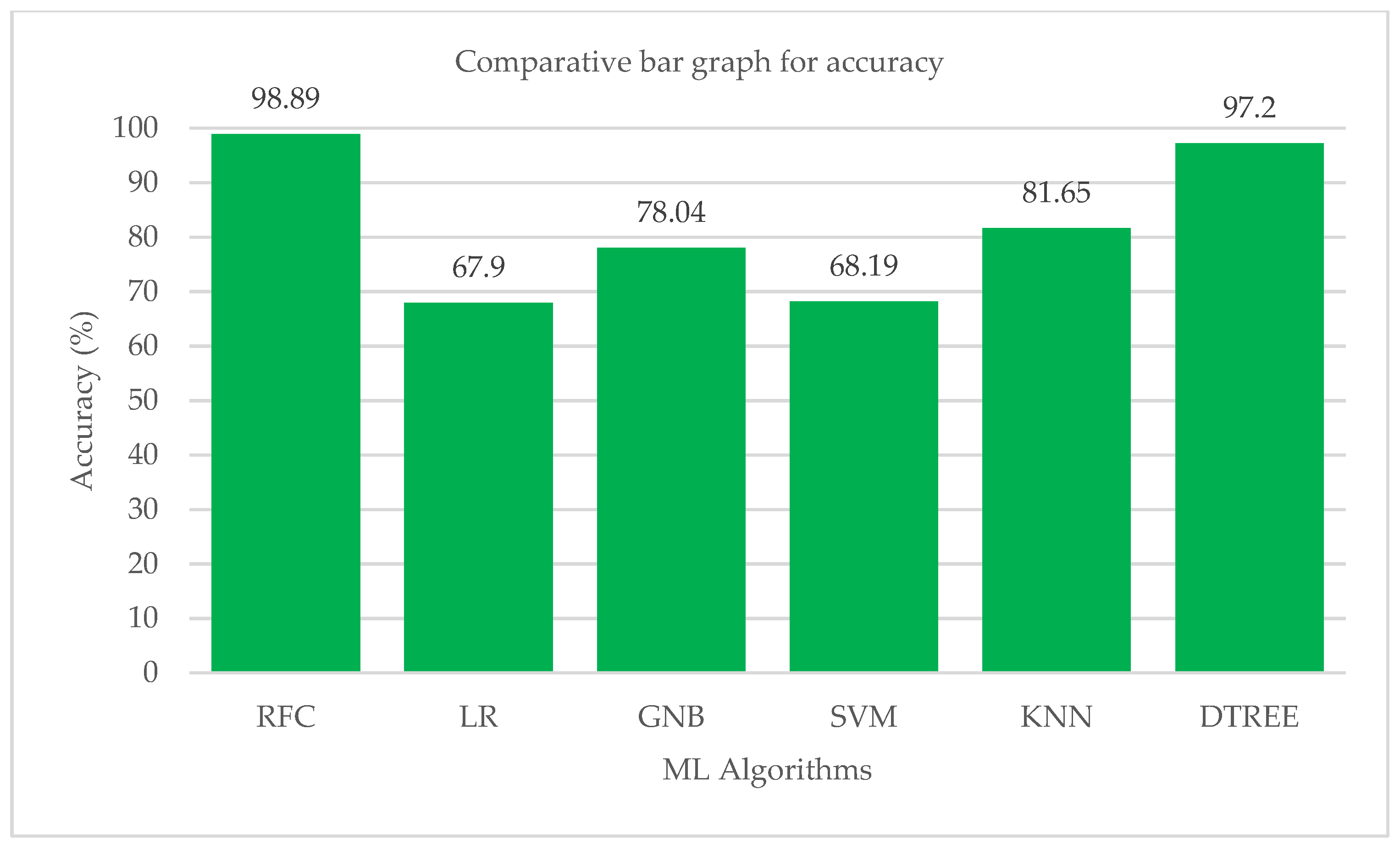
| ML Algorithm | Accuracy |
|---|---|
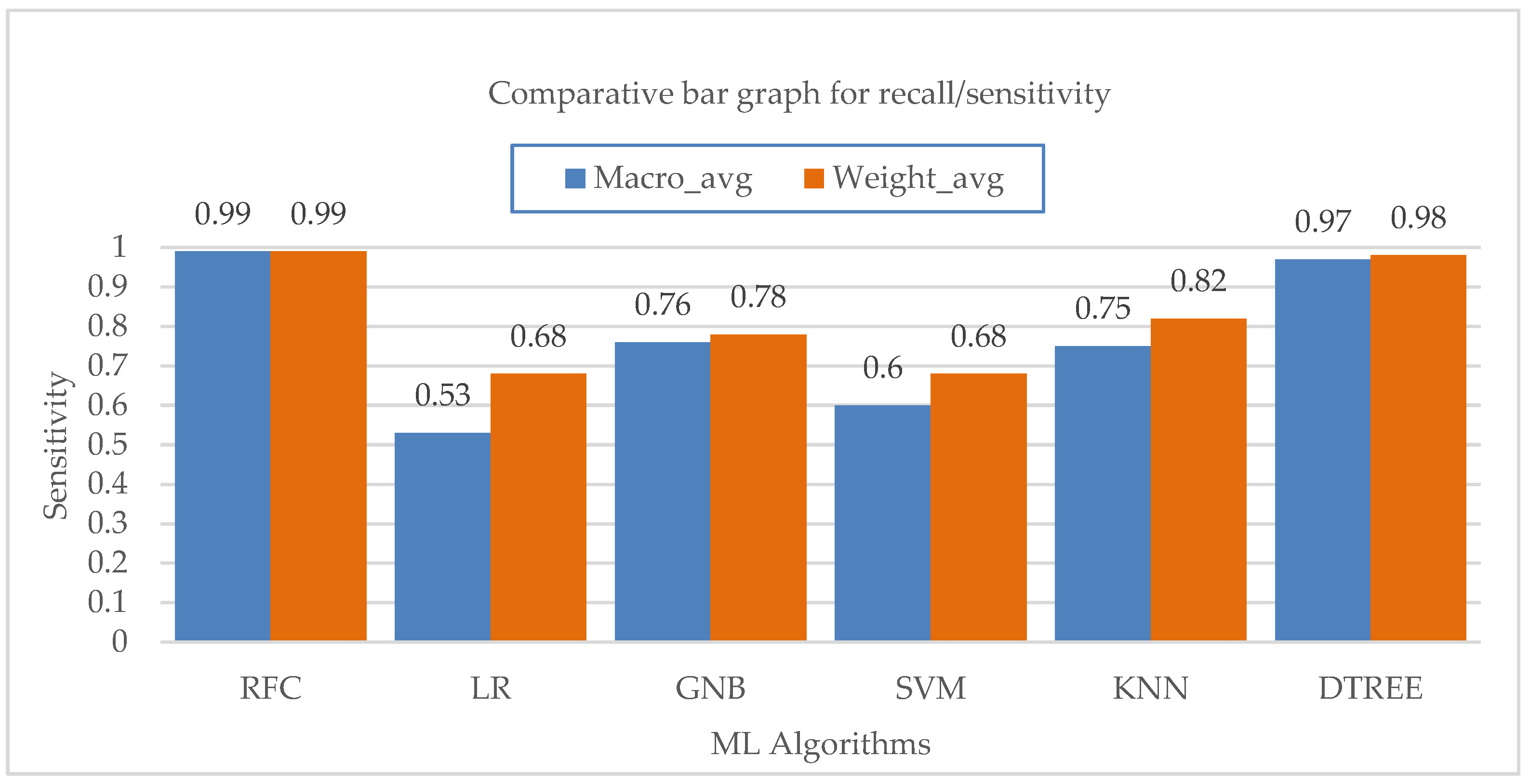
| Random-Forest | 0.9889 |
| Logistic regression | 0.6790 |
| GaussianNB | 0.7804 |
| Support vector machine | 0.6819 |
| KNeighbors | 0.8165 |
| Decision-Tree | 0.9716 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giri, J.; Al-Lohedan, H.A.; Mohammad, F.; Soleiman, A.A.; Chadge, R.; Mahatme, C.; Sunheriya, N.; Giri, P.; Mutyarapwar, D.; Dhapke, S. A Comparative Study on Predication of Appropriate Mechanical Ventilation Mode through Machine Learning Approach. Bioengineering 2023, 10, 418. https://doi.org/10.3390/bioengineering10040418
Giri J, Al-Lohedan HA, Mohammad F, Soleiman AA, Chadge R, Mahatme C, Sunheriya N, Giri P, Mutyarapwar D, Dhapke S. A Comparative Study on Predication of Appropriate Mechanical Ventilation Mode through Machine Learning Approach. Bioengineering. 2023; 10(4):418. https://doi.org/10.3390/bioengineering10040418
Chicago/Turabian StyleGiri, Jayant, Hamad A. Al-Lohedan, Faruq Mohammad, Ahmed A. Soleiman, Rajkumar Chadge, Chetan Mahatme, Neeraj Sunheriya, Pallavi Giri, Dhananjay Mutyarapwar, and Shreya Dhapke. 2023. "A Comparative Study on Predication of Appropriate Mechanical Ventilation Mode through Machine Learning Approach" Bioengineering 10, no. 4: 418. https://doi.org/10.3390/bioengineering10040418