

The Significant Potential of Simonkolleite Powder for Deep Wound Healing under a Moist Environment: In Vivo Histological Evaluation Using a Rat Model

Abstract
:1. Introduction
2. Materials and Method
2.1. Synthesis of Simonkolleite Powder Using a Solution Process
2.2. Powder Characterizations
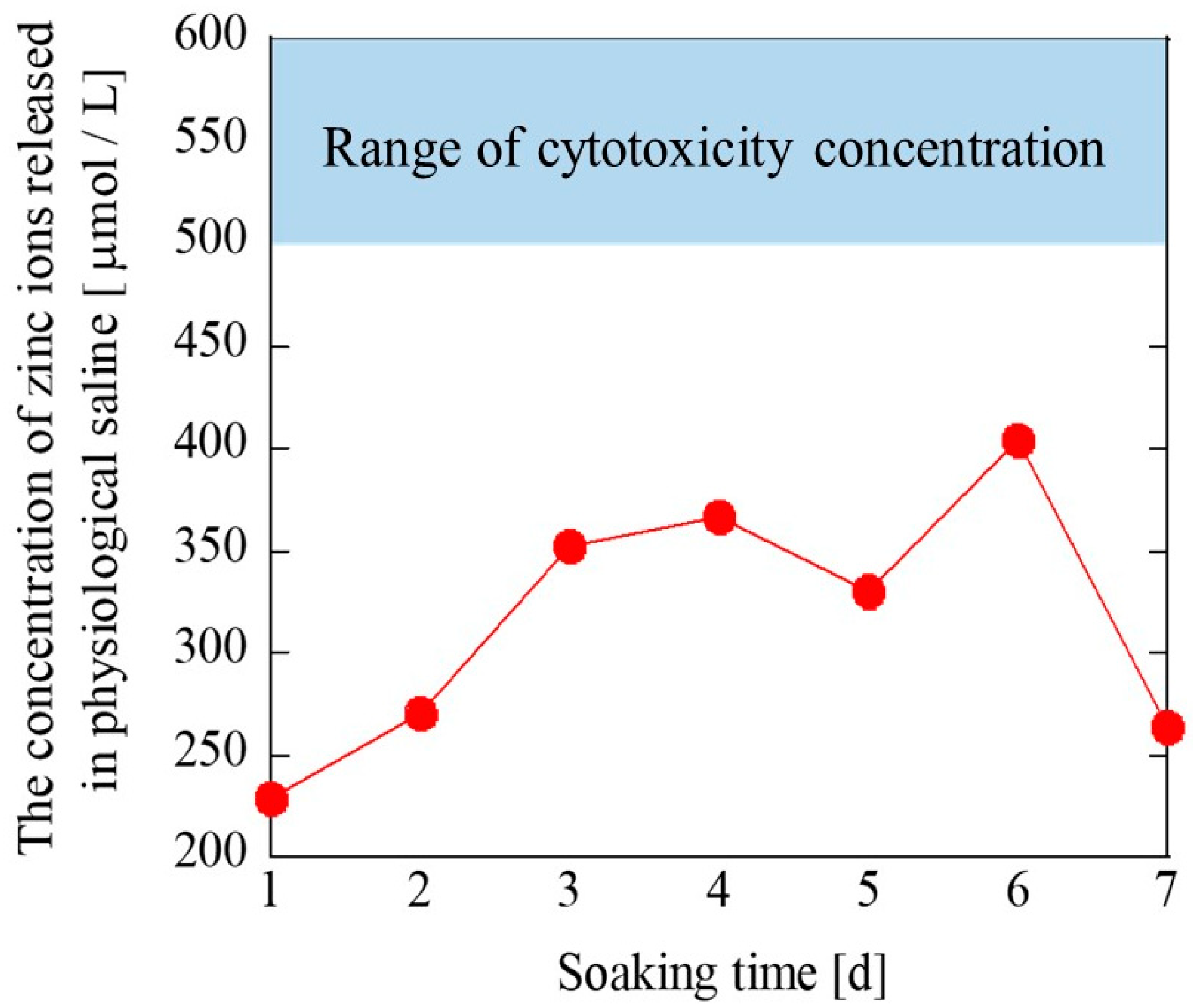
2.3. Zn2+ Ions Releasing Test and pH Value
2.4. In Vivo Evaluation of Simonkolleite
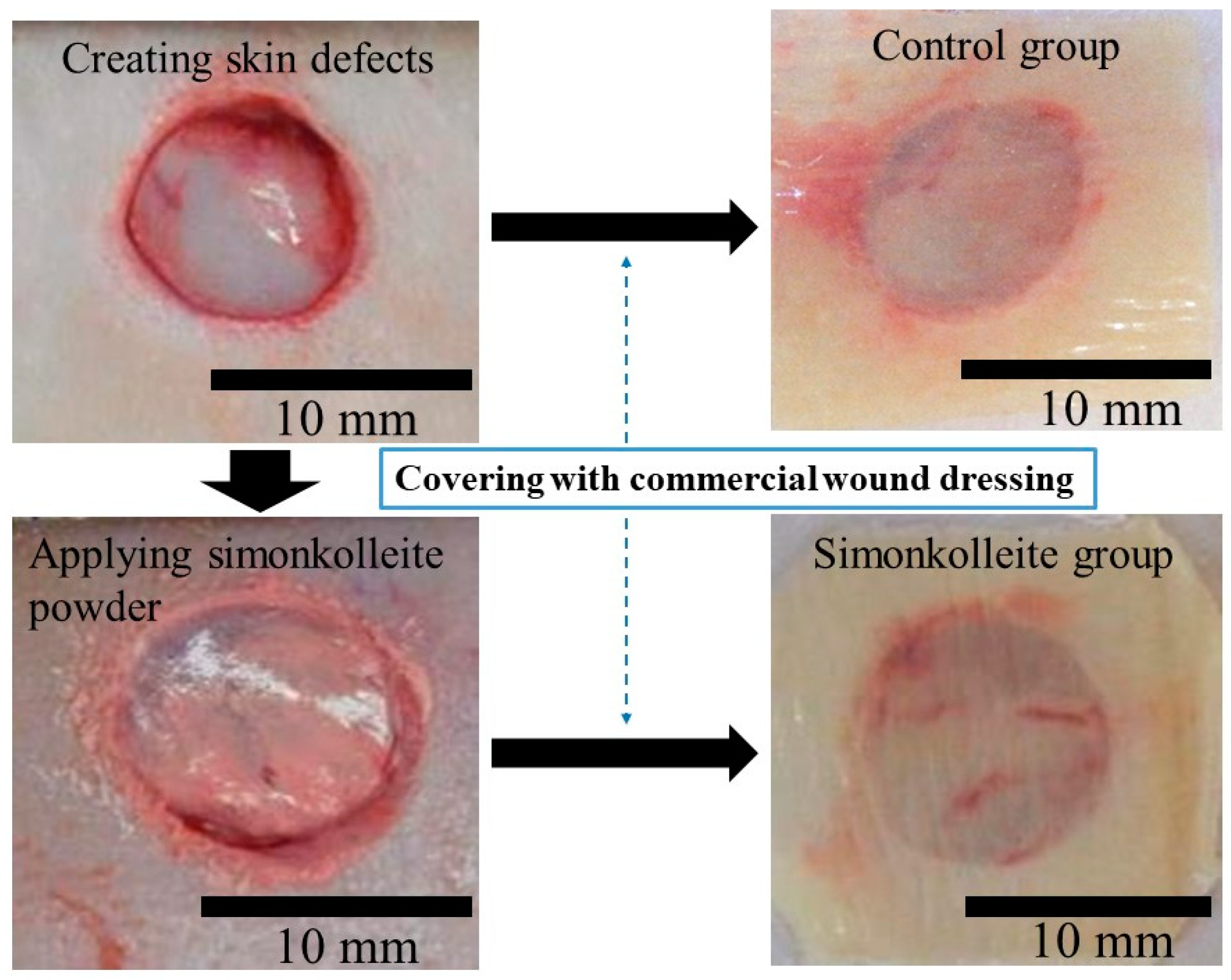
2.4.1. Animal Experiment
Preparation for Animal Surgery
Animal Models
2.4.2. Morphometric Analysis
2.4.3. Histological Evaluation
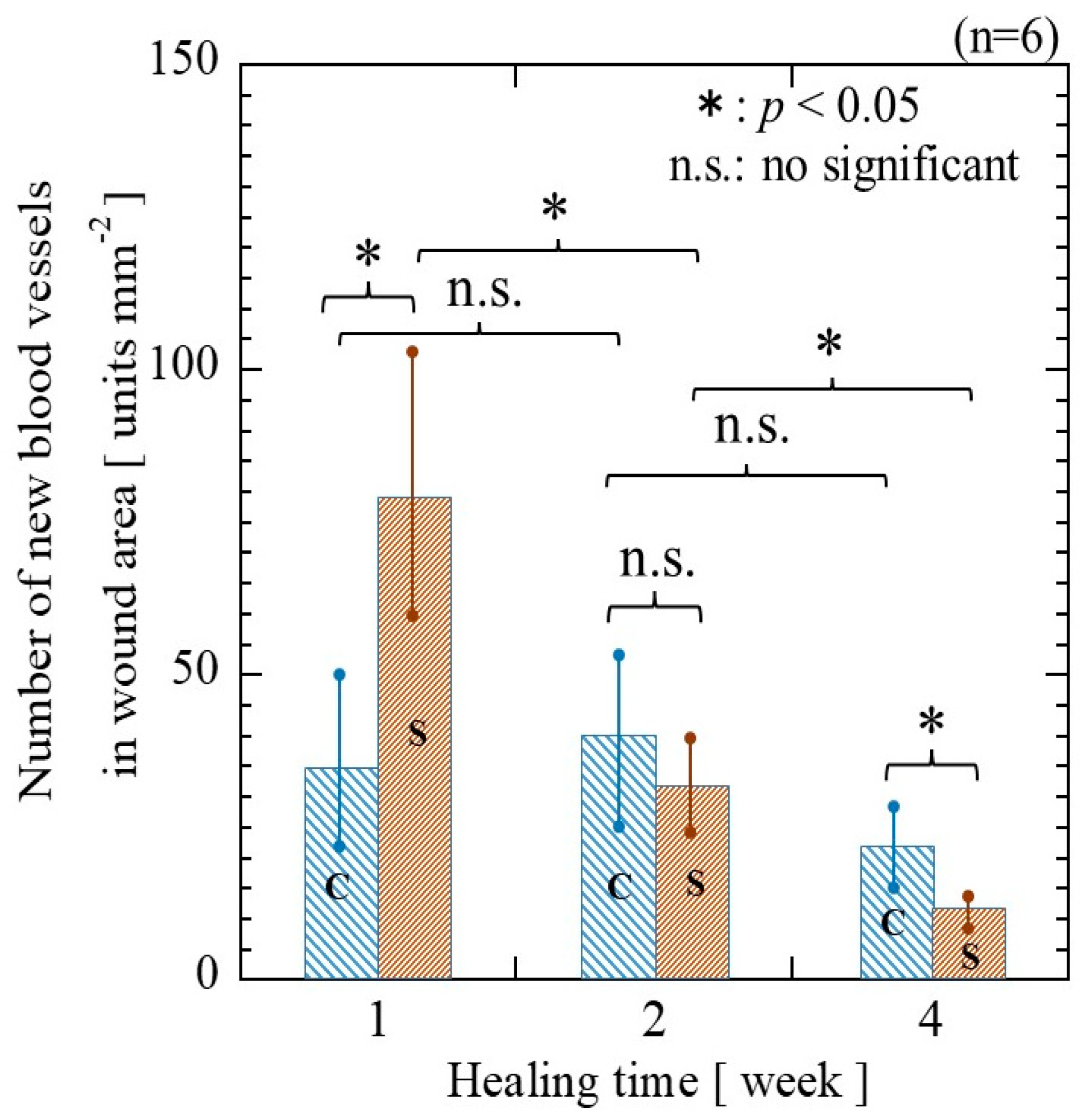
2.4.4. Blood Vessels Counting
2.5. Statistical Analyses
3. Results
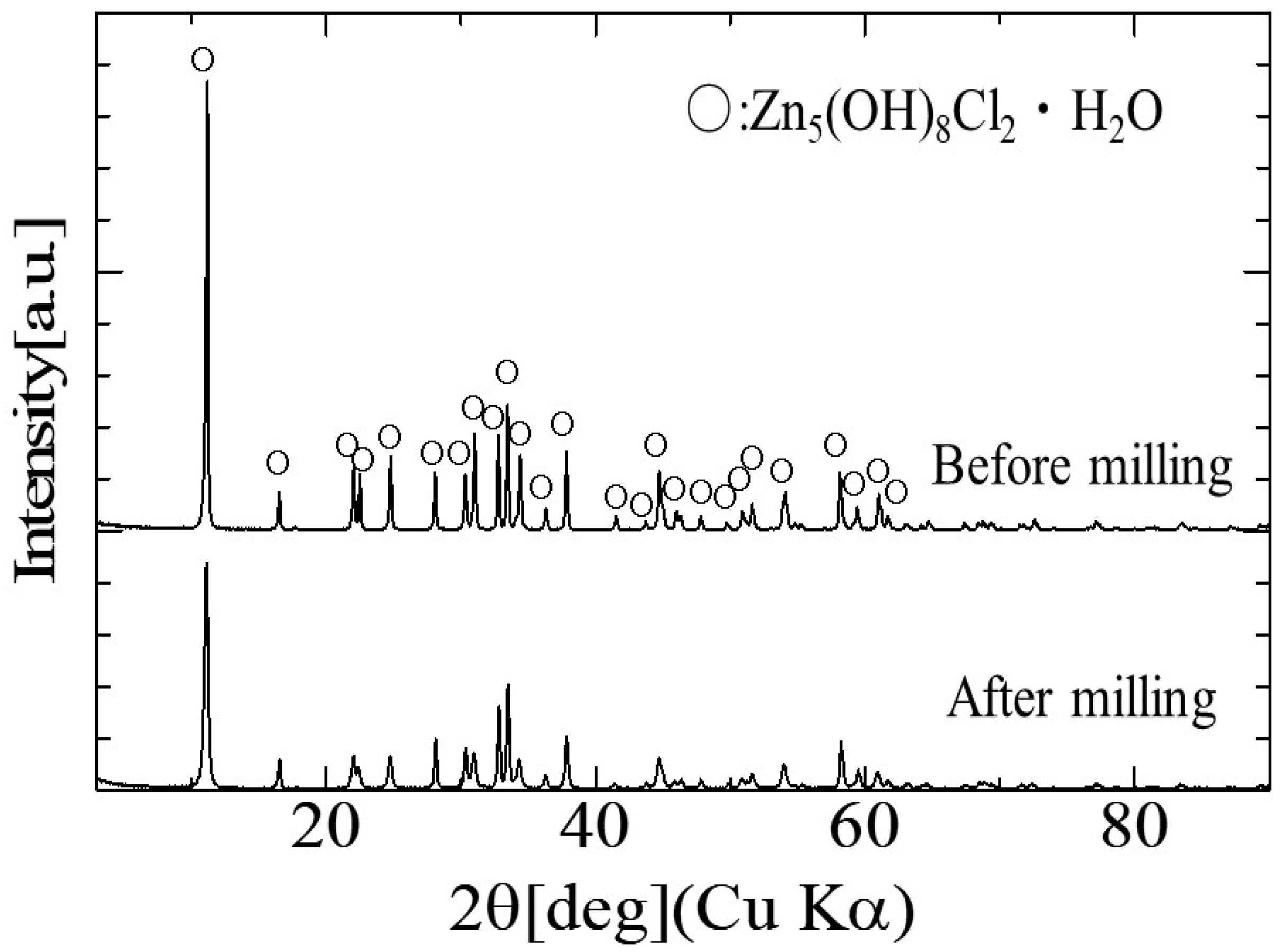
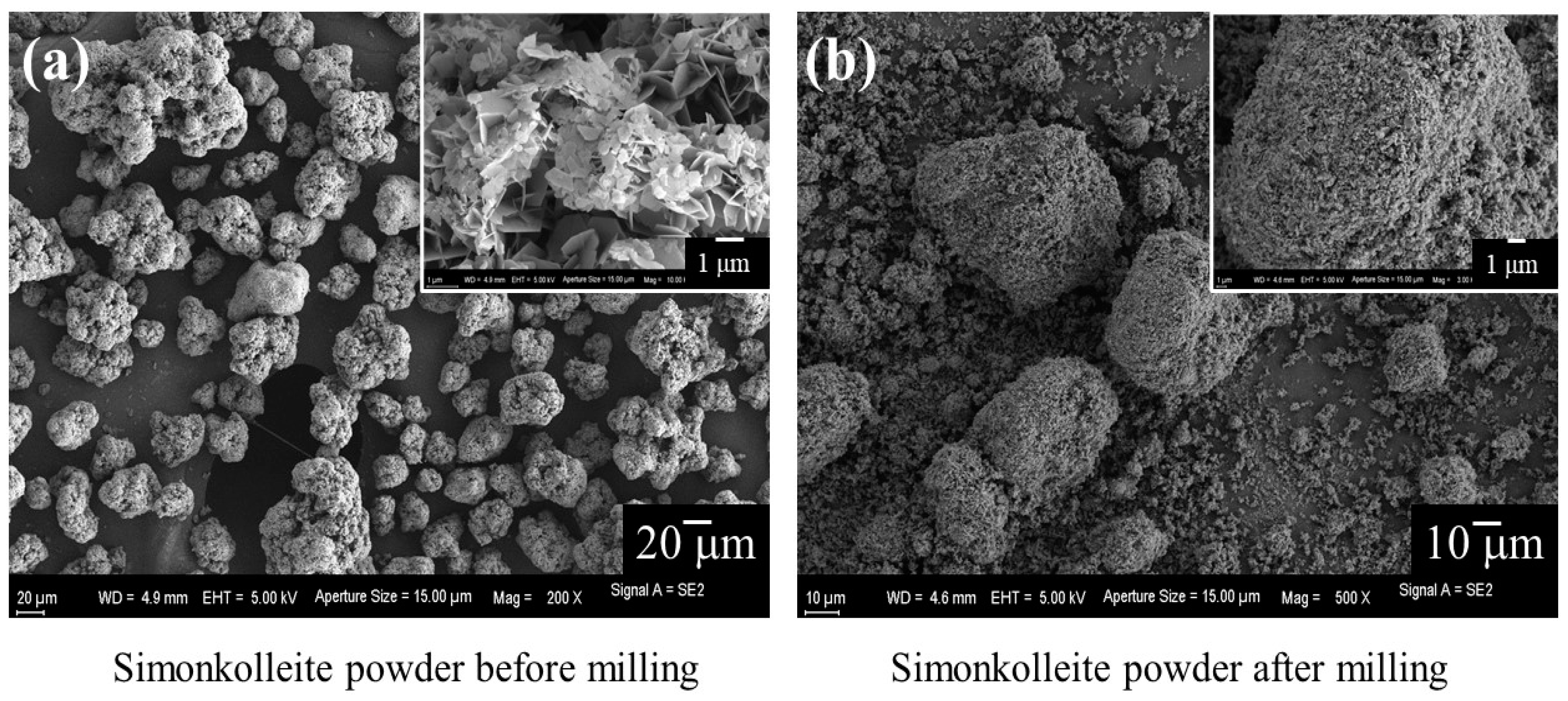
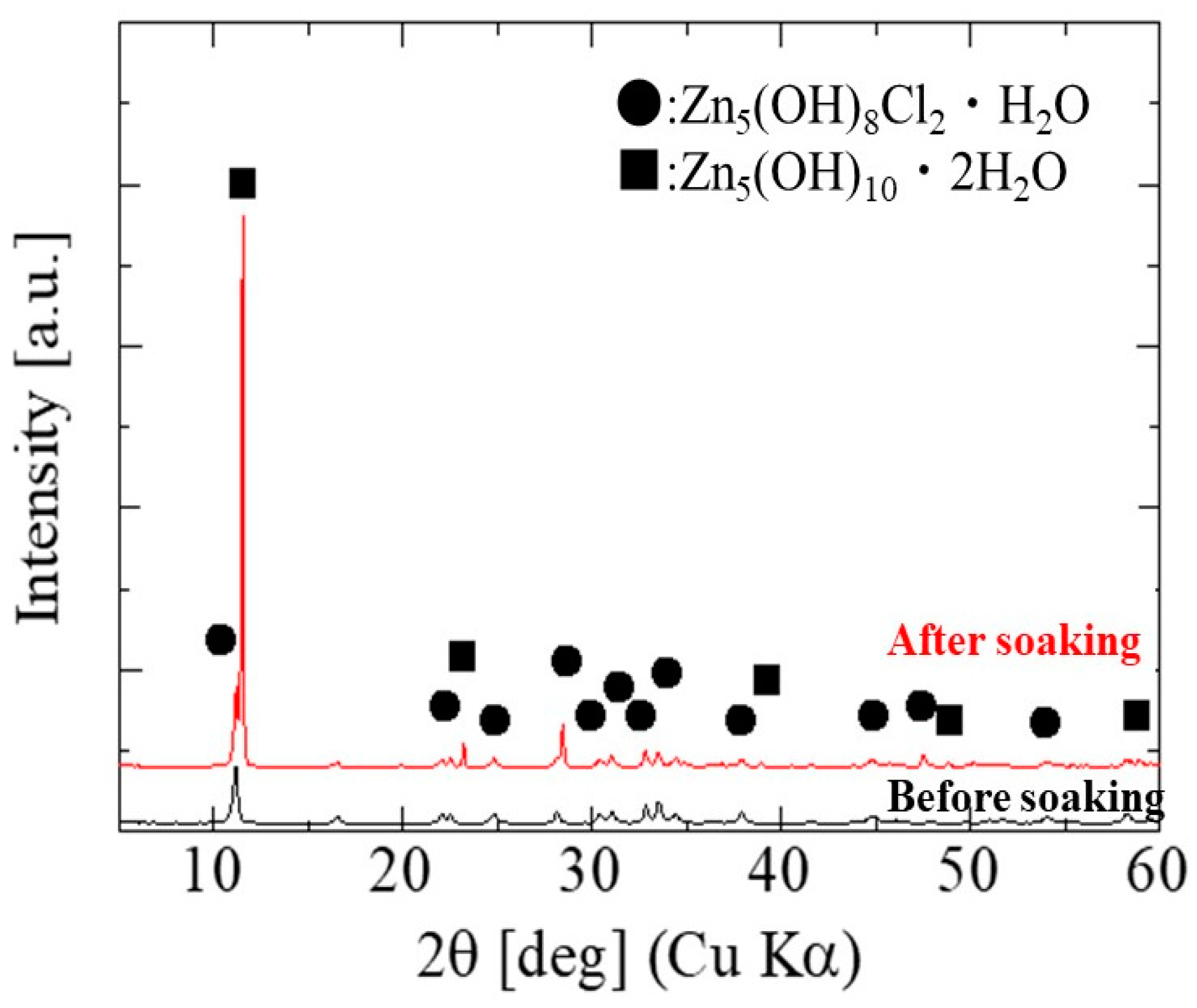
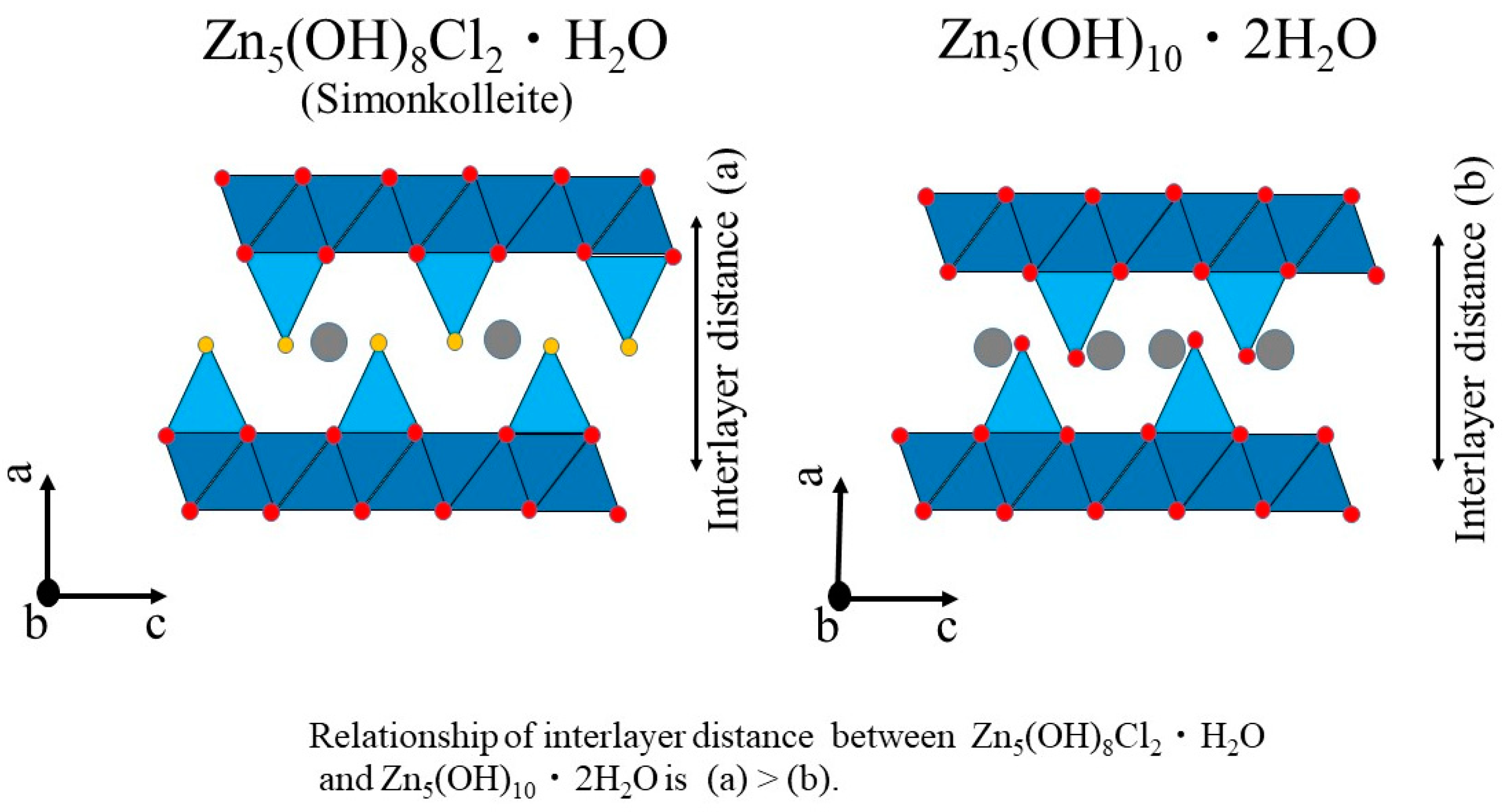
3.1. Characterization of Simonkolleite
3.2. The Wound Healing Effect of Simonkolleite
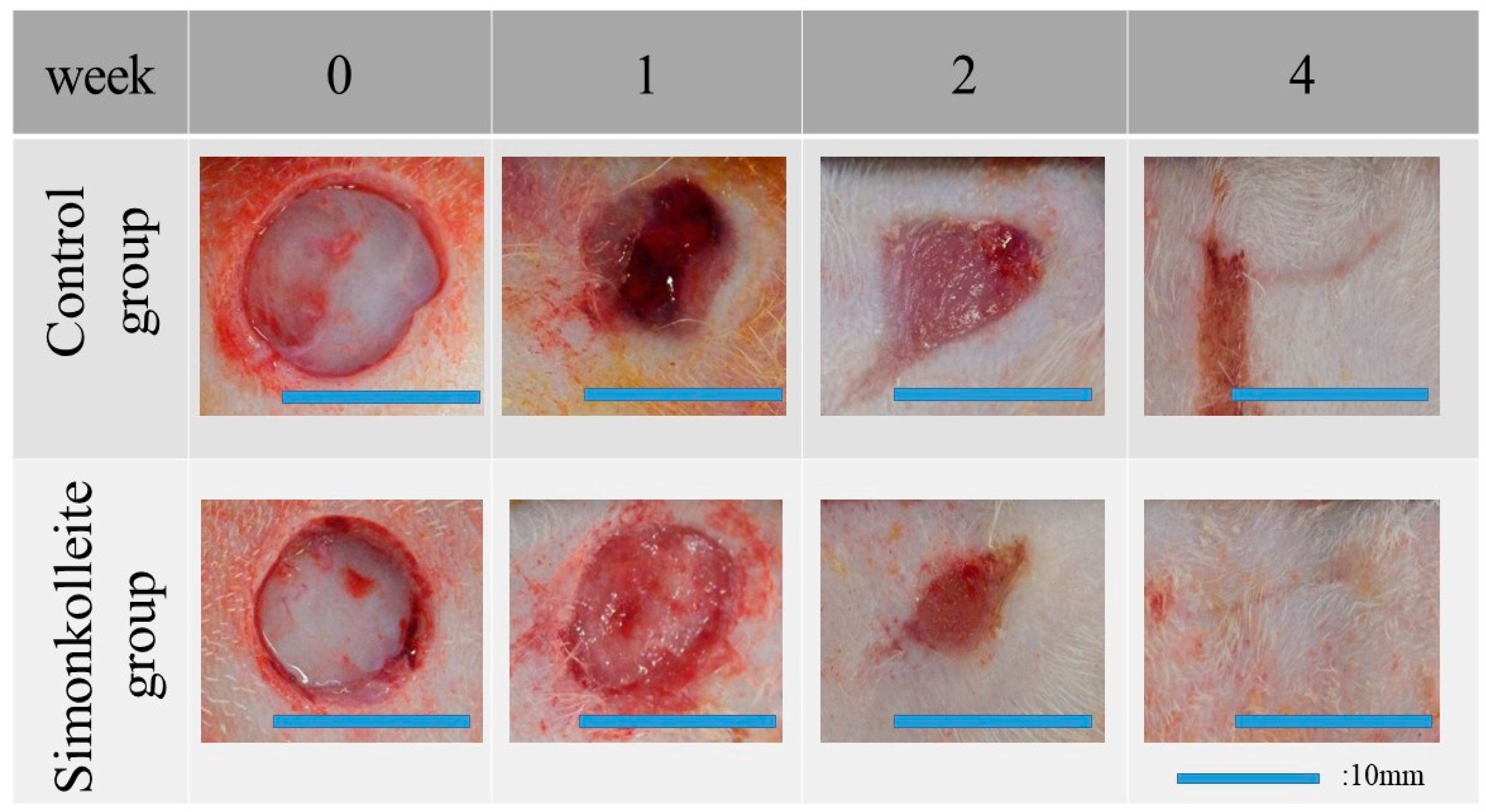
3.2.1. Macroscopic Changes in the Residual Wound Area
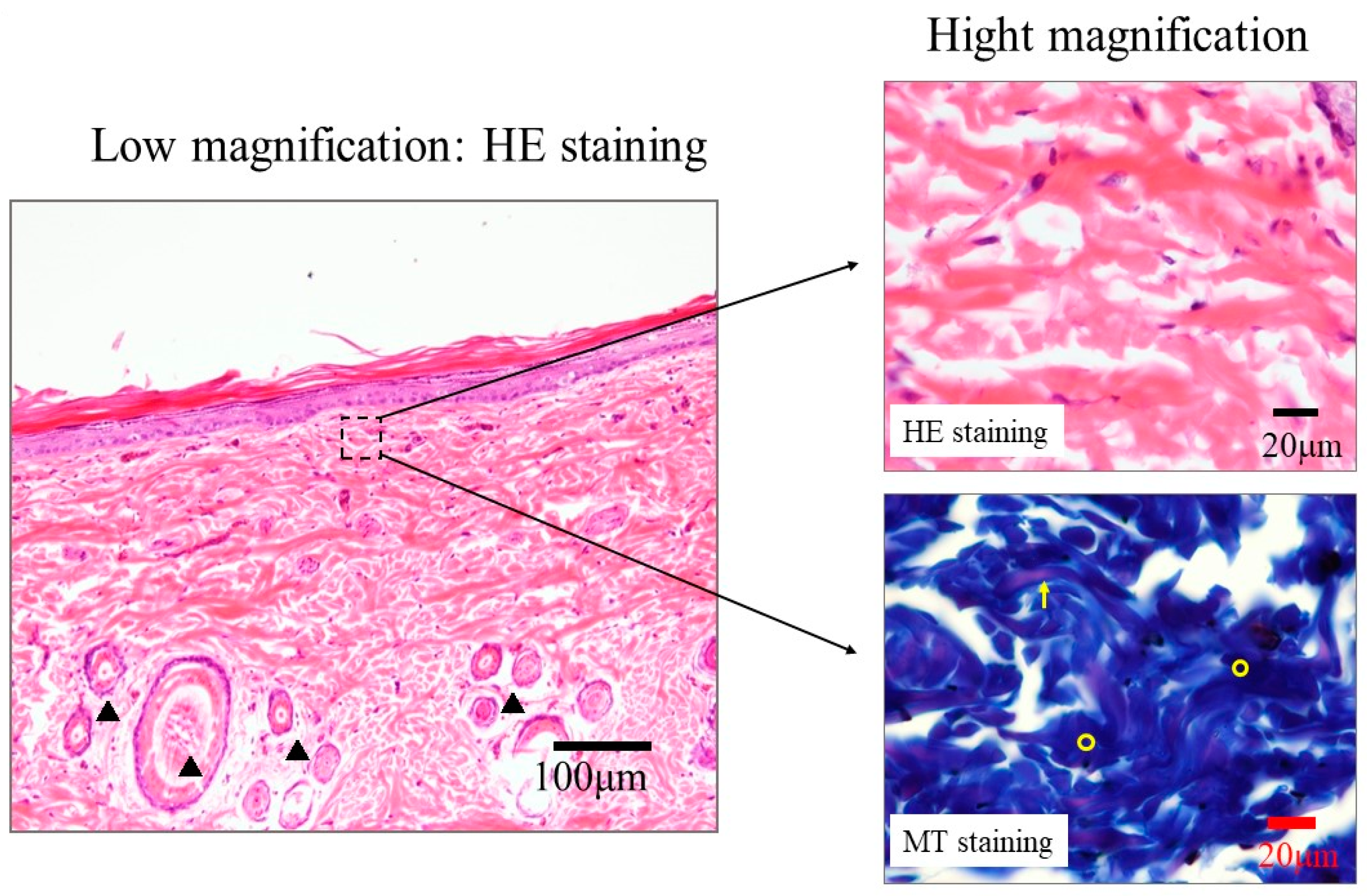
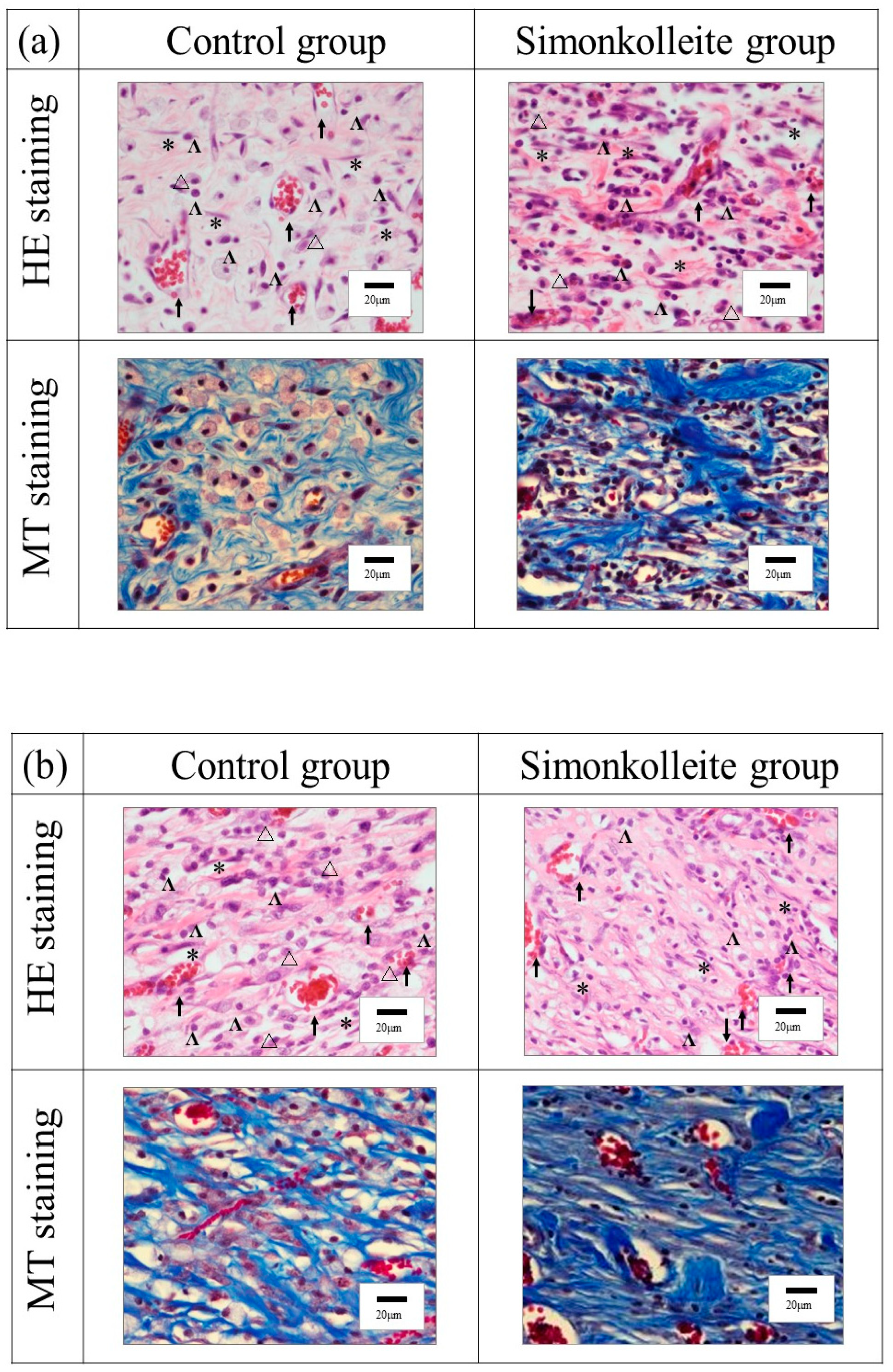
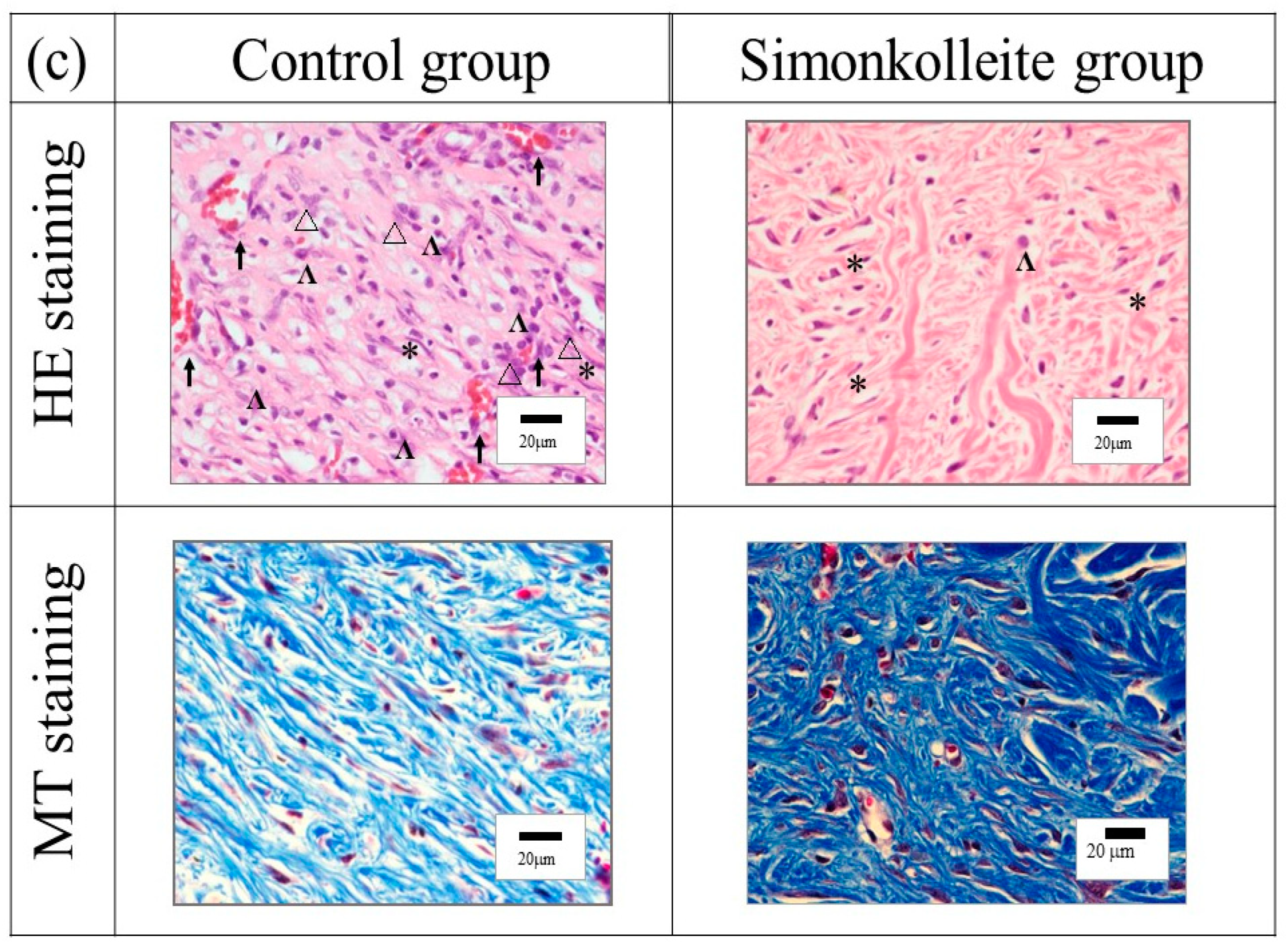
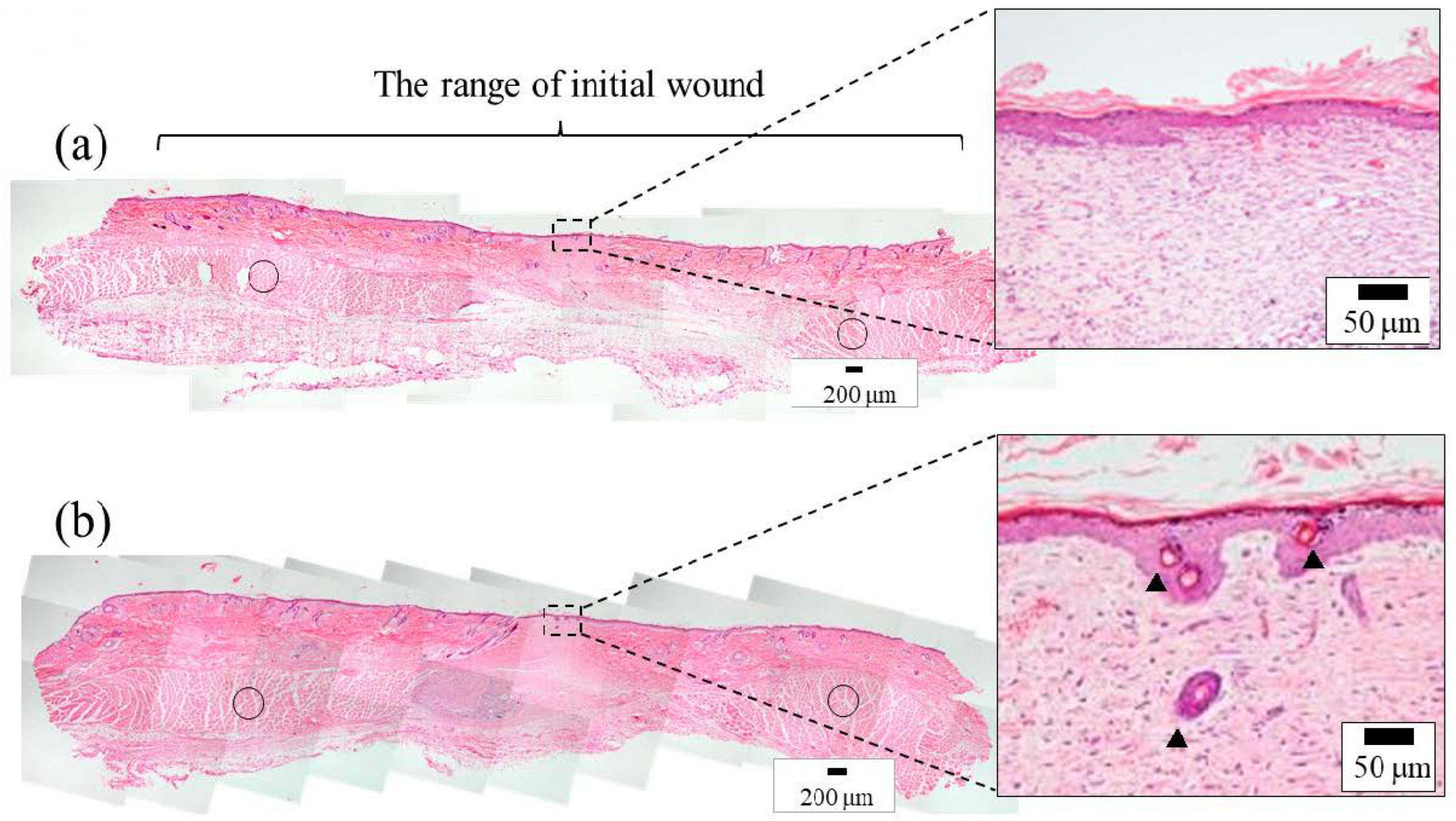
3.2.2. Histological Evaluation
4. Discussion
Zn5(OH)8Cl2·H2O + 8NaCl + NH3 + HCl + (n−1)H2O
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ikeda, Y. Challenges in tissue engineering. J. R. Soc. Interface 2006, 3, 589–601. [Google Scholar] [CrossRef]
- Zhao, S.; Li, L.; Wang, H.; Zhang, Y.; Cheng, X.; Zhou, N.; Rahaman, M.N.; Liu, Z.; Huang, W.; Zhang, C. Wound dressings com-posed of copper-doped borate bioactive glass microfibers stimulate angiogenesis and heal full-thickness skin defects in a ro-dent model. Biomaterials 2015, 53, 379–391. [Google Scholar] [CrossRef]
- Greaves, N.S.; Ashcroft, K.J.; Baguneid, M.; Bayat, A. Current understanding of molecular and cellular mechanisms in fibro-plasia and angiogenesis during acute wound healing. J. Dermatol. Sci. 2013, 72, 206–217. [Google Scholar] [CrossRef]
- Bauer, S.M.; Bauer, R.J.; Velazquez, O.C. Angiogenesis, Vasculogenesis, and Induction of Healing in Chronic Wounds. Vasc. Endovasc. Surg. 2005, 39, 293–306. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Brown, R.F.; Jung, S.B.; Day, D.E. Angiogenic effects of borate glass microfibers in a rodent model. J. Biomed. Mater. Res. A 2014, 102, 4491–4499. [Google Scholar] [CrossRef] [PubMed]
- Lokhande, G.; Carrow, J.K.; Thakur, T.; Xavier, J.R.; Parani, M.; Bayless, K.J.; Gaharwar, A.K. Nanoengineered injectable hy-drogels for wound healing application. Acta Biomater. 2018, 70, 35–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamoun, E.A.; Kenawy, E.-R.S.; Chen, X. A review on polymeric hydrogel membranes for wound dressing applications: PVA-based hydrogel dressings. J. Adv. Res. 2017, 8, 217–233. [Google Scholar] [CrossRef]
- Akita, S.; Akino, K.; Imaizumi, T.; Tanaka, K.; Anraku, K.; Yano, H.; Hirano, A. A polyurethane dressing is beneficial for split-thickness skin-graft donor wound healing. Burns 2006, 32, 447–451. [Google Scholar] [CrossRef]
- Zhang, Y.; Jiang, M.; Zhang, Y.; Cao, Q.; Wang, X.; Han, Y.; Sun, G.; Li, Y.; Zhou, J. Novel lignin–chitosan–PVA composite hydro-gel for wound dressing. Mater. Sci. Eng. C 2019, 104, 110002. [Google Scholar] [CrossRef]
- Razzak, M.T.; Darwis, D.; Zainuddin, H. Sukirno Irradiation of polyvinyl alcohol and polyvinyl pyrrolidone blended hydrogel for wound dressing. Radiat. Phys. Chem. 2001, 62, 107–113. [Google Scholar] [CrossRef]
- Jin, S.G.; Yousaf, A.M.; Kim, K.S.; Kim, D.W.; Kim, J.K.; Yong, C.S.; Youn, Y.S.; Kim, J.O.; Choi, H.-G. Influence of hydrophilic polymers on functional properties and wound healing efficacy of hydrocolloid based wound dressings. Int. J. Pharm. 2016, 501, 160–166. [Google Scholar] [CrossRef]
- Moura, D.; Souza, M.; Liverani, L.; Rella, G.; Luz, G.; Mano, J.; Boccaccini, A. Development of a bioactive glass-polymer composite for wound healing applications. Mater. Sci. Eng. C 2017, 76, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Cheng, F.; Liu, J.; Smått, J.-H.; Gepperth, D.; Lastusaari, M.; Xu, C.; Hupa, L. Biocomposites of copper-containing mes-oporous bioactive glass and nanofibrillated cellulose: Biocompatibility and angiogenic promotion in chronic wound healing application. Acta Biomater. 2016, 46, 286–298. [Google Scholar] [CrossRef] [PubMed]
- Hench, L.L. Genetic design of bioactive glass. J. Eur. Ceram. Soc. 2009, 29, 1257–1265. [Google Scholar] [CrossRef]
- Yu, H.; Peng, J.; Xu, Y.; Chang, J.; Li, H. Bioglass Activated Skin Tissue Engineering Constructs for Wound Healing. ACS Appl. Mater. Interfaces 2016, 8, 703–715. [Google Scholar] [CrossRef] [PubMed]
- Fan, C.; Xu, Q.; Hao, R.; Wang, C.; Que, Y.; Chen, Y.; Yang, C.; Chang, J. Multi-functional wound dressings based on silicate bio-active materials. Biomaterials 2022, 287, 121652. [Google Scholar] [CrossRef]
- Sasaki, Y.; Sathi, G.A.; Yamamoto, O. Wound healing effect of bioactive ion released from Mg-smectite. Mater. Sci. Eng. C 2017, 77, 52–57. [Google Scholar] [CrossRef]
- Sasaki, Y.; Sathi, G.A.; Yamamoto, O. In vivo evaluation of wound healing property of zinc smectite using a rat model. J. Ceram. Soc. Jpn. 2016, 124, 1199–1204. [Google Scholar] [CrossRef] [Green Version]
- Maier, J.A.M.; Bernardini, D.; Rayssiguier, Y.; Mazur, A. High concentrations of magnesium modulate vascular endothelial cell behaviour in vitro. Biochim. Biophys. Acta 2004, 1689, 6–12. [Google Scholar]
- Worf, F.I.; Trapani, V. Cell (patho)physiology of magnesium. Clin. Sci. 2008, 114, 27–35. [Google Scholar]
- Stechmiller, J.K.; Faan, A.C. Understanding the Role of Nutrition and Wound Healing. Nutr. Clin. Pract. 2010, 25, 61–68. [Google Scholar] [CrossRef]
- Senni, K.; Foucault-Bertaud, A.; Godeau, G. Magnesium and connective tissue. Magnes. Res. 2003, 16, 70–74. [Google Scholar] [PubMed]
- Li, H.; Chang, J. Bioactive silicate materials stimulate angiogenesis in fibroblast and endothelial cell co-culture system through paracrine effect. Acta Biomater. 2013, 9, 6981–6991. [Google Scholar] [CrossRef] [PubMed]
- Lantenois, S.; Champallier, R.; Bény, J.-M.; Muller, F. Hydrothermal synthesis and characterization of dioctahedral smectites: A montmorillonites series. Appl. Clay Sci. 2008, 38, 165–178. [Google Scholar] [CrossRef] [Green Version]
- Ishii, R.; Teshima, N.; Ebina, T.; Mizukami, F. Increasing particle size of a synthetic smectite for polymer nanocomposites using a supercritical hydrothermal treatment. J. Colloid Interface Sci. 2010, 348, 313–321. [Google Scholar] [CrossRef]
- Saghiri, M.A.; Asatourian, A.; Orangi, J.; Sorenson, C.M.; Sheibeni, N. Functional role of inorganic trace elements in angiogene-sis—Part II: Cr, Si, Zn, Cu, and S. Crit. Rev. Oncol. Hematol. 2015, 96, 143–155. [Google Scholar] [CrossRef]
- Inoue, K.; O’Bryant, Z.; Xiong, Z.-G. Zinc-Permeable Ion Channels: Effects on Intracellular Zinc Dynamics and Potential Phys-iological/Pathophysiological Significance. Curr. Med. Chem. 2015, 22, 1248–1257. [Google Scholar] [CrossRef] [Green Version]
- Lansdown, A.B.G.; Mirastschijski, U.; Stubbs, N.; Scanlon, E.; Ågren, M.S. Zinc in wound healing: Theoretical, experimental, and clinical aspects. Wound Repair Regen. 2007, 15, 2–16. [Google Scholar] [CrossRef]
- Yabluchanski, A.; Ma, Y.; Iyer, R.P.; Hall, M.E.; Lindsey, M.L. Matrix Metalloproteinase-9: Many Shades of Function in Cardi-ovascular Disease. Physiology 2013, 28, 391–403. [Google Scholar] [CrossRef] [Green Version]
- Anzellotti, A.I.; Farrell, N.P. Zincmetalloproteins as medicinal targets. Chem. Soc. Rev. 2008, 37, 1629–1651. [Google Scholar] [CrossRef]
- Evans, D.G.; Slade, R.C.T. Structural Aspects of Layered Double Hydroxides, (Structure and Bonding); Springer: Berlin, Germany, 2006; Volume 119, pp. 1–87. [Google Scholar]
- Stählin, W.; Oswald, H.R. The crystal structure of zinc hydroxide nitrate, Zn5(OH)8(NO3)2·2H2O. Acta Cryst. 1970, B26, 860–863. [Google Scholar] [CrossRef]
- Gordeeva, A.; Hsu, Y.-J.; Jenei, I.Z.; Brant Carvalho, P.H.B.; Simak, S.I.; Andersson, O.; Häussermann, U. Layered Zinc Hy-droxide Dihydrate, Zn5(OH)10·2H2O, from Hydrothermal Conversion of ε-Zn(OH)2 at Gigapascal Pressures and its Transfor-mation to Nanocrystalline ZnO. ACS Omega 2020, 5, 17617–17627. [Google Scholar] [CrossRef]
- Hawthorne, F.C.; Sokolova, E. Simonkolleite, Zn5(OH)8Cl2(H2O), A decorated interrupted-sheet Structure of the form [Mφ2]4. Can. Mineral. 2002, 40, 939–946. [Google Scholar] [CrossRef]
- Sharpe, J.R.; Harris, K.L.; Jubin, K.; Bainbridge, N.R.; Jordan, N.R. The effect of pH in modulating skin cell behaviour. Br. J. Dermatol. 2009, 161, 671–673. [Google Scholar] [CrossRef] [PubMed]
- Dąbrowska, A.; Spano, F.; Derler, S.; Adlhart, C.; Spencer, N.D.; Rossi, R. The relationship between skin function, barrier properties, and body-dependent factors. Skin. Res. Technol. 2018, 24, 165–174. [Google Scholar] [CrossRef] [Green Version]
- Schultz, G.S.; Sibbald, R.G.; Falanga, V.; Ayello, E.A.; Dowsett, C.; Harding, K.; Romanelli, M.; Stacey, M.C.S.; Teot, L.; Vanscheidt, W. Wound bed preparation: A systematic approach to wound management. Wound Repair Regen. 2003, 11, S1–S28. [Google Scholar] [CrossRef] [PubMed]
- Amadeu, T.P.; Coulomb, B.; Desmouliere, A.; Costa, A.M.A. Cutaneous Wound Healing: Myofibroblastic Differentiation and in Vitro Models. Int. J. Low. Extrem. Wounds 2003, 2, 60–68. [Google Scholar] [CrossRef]
- Prasad, A.S. Zinc: An antioxidant and anti-inflammatory agent: Role of zinc in degenerative disorders of aging. J. Trace Elem. Med. Biol. 2014, 28, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Jiang, D.; Ou, Y.; Hu, Z.; Jiang, J.; Lei, X. An anti-inflammatory role of A20 zinc finger protein during trauma combined with endotoxin challenge. J. Surg. Res. 2013, 185, 717–725. [Google Scholar] [CrossRef]
- Wey, A.; Cunningham, C.; Hreha, J.; Breitbart, E.; Cottrell, J.; Ippolito, J.; Clark, D.; Lin, H.N.; Benevenia, J.; Patrick O’Connor, J.; et al. Local ZnCl2 accelerates fracture healing. J. Orthop. Res. 2014, 32, 834–841. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Week | 0 | 1 | 2 | 4 |
|---|---|---|---|---|
| Control group | 100 | 61 ± 11.5 | 20 ± 11.3 | 1.5 ± 0.5 |
| Simonkolleite group | 100 | 52 ± 9.5 | 12 ± 8.2 | 0.5 ± 0.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamamoto, O.; Nagashima, M.; Nakata, Y.; Udagawa, E. The Significant Potential of Simonkolleite Powder for Deep Wound Healing under a Moist Environment: In Vivo Histological Evaluation Using a Rat Model. Bioengineering 2023, 10, 375. https://doi.org/10.3390/bioengineering10030375
Yamamoto O, Nagashima M, Nakata Y, Udagawa E. The Significant Potential of Simonkolleite Powder for Deep Wound Healing under a Moist Environment: In Vivo Histological Evaluation Using a Rat Model. Bioengineering. 2023; 10(3):375. https://doi.org/10.3390/bioengineering10030375
Chicago/Turabian StyleYamamoto, Osamu, Miki Nagashima, Yoshimi Nakata, and Etsuro Udagawa. 2023. "The Significant Potential of Simonkolleite Powder for Deep Wound Healing under a Moist Environment: In Vivo Histological Evaluation Using a Rat Model" Bioengineering 10, no. 3: 375. https://doi.org/10.3390/bioengineering10030375