
Clinicopathological Features of Invasive Breast Cancer: A Five-Year Retrospective Study in Southern and South-Western Ethiopia

 , , ,
, , ,
Abstract
:1. Background
2. Materials and Methods
2.1. Data Collection
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Classification Criteria
2.5. Data Analysis
3. Results
3.1. Demographic Characteristics
3.2. Clinicopathological Features
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sudhakar, A. History of Cancer, Ancient and Modern Treatment Methods. J. Cancer Sci. Ther. 2009, 1, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Ginsburg, O.; Bray, F.; Coleman, M.P.; Vanderpuye, V.; Eniu, A.; Kotha, S.R.; Sarker, M.; Huong, T.T.; Allemani, C.; Dvaladze, A.; et al. The global burden of women’s cancers: A grand challenge in global health. Lancet 2017, 389, 847–860. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Arnold, M.; Morgan, E.; Rumgay, H.; Mafra, A.; Singh, D.; Laversanne, M.; Vignat, J.; Gralow, J.R.; Cardoso, F.; Siesling, S.; et al. Current and future burden of breast cancer: Global statistics for 2020 and 2040. Breast 2022, 66, 15–23. [Google Scholar] [CrossRef]
- Palma, G.; Frasci, G.; Chirico, A.; Esposito, E.; Siani, C.; Saturnino, C.; Arra, C.; Ciliberto, G.; Giordano, A.; D’aiuto, M. Triple negative breast cancer: Looking for the missing link between biology and treatments. Oncotarget 2015, 6, 26560–26574. [Google Scholar] [CrossRef] [PubMed]
- Azubuike, S.O.; Muirhead, C.; Hayes, L.; McNally, R. Rising global burden of breast cancer: The case of sub-Saharan Africa (with emphasis on Nigeria) and implications for regional development: A review. World J. Surg. Oncol. 2018, 16, 63. [Google Scholar] [CrossRef]
- Jedy-Agba, E.; McCormack, V.; Adebamowo, C.; Dos-Santos-Silva, I. Stage at diagnosis of breast cancer in sub-Saharan Africa: A systematic review and meta-analysis. Lancet Glob. Health 2016, 4, e923–e935. [Google Scholar] [CrossRef]
- Brewster, A.M.; Chavez-MacGregor, M.; Brown, P. Epidemiology, biology, and treatment of triple-negative breast cancer in women of African ancestry. Lancet Oncol. 2014, 15, e625–e634. [Google Scholar] [CrossRef]
- Duffy, M.J.; O’Donovan, N.; McDermott, E.; Crown, J. Validated biomarkers: The key to precision treatment in patients with breast cancer. Breast 2016, 29, 192–201. [Google Scholar] [CrossRef]
- Howell, A.; Anderson, A.S.; Clarke, R.B.; Duffy, S.W.; Evans, D.G.; Garcia-Closas, M.; Gescher, A.J.; Key, T.J.; Saxton, J.M.; Harvie, M.N. Risk determination and prevention of breast cancer. Breast Cancer Res. 2014, 16, 446. [Google Scholar] [CrossRef] [PubMed]
- Gemta, E.A.; Bekele, A.; Mekonen, W.; Seifu, D.; Bekurtsion, Y.; Kantelhardt, E.J. Patterns of Breast Cancer Among Ethiopian Patients: Presentations and Histopathological Features. J. Cancer Sci. Ther. 2019, 11, 38–42. [Google Scholar] [CrossRef]
- Hailu, H.E.; Mondul, A.M.; Rozek, L.S.; Geleta, T. Descriptive Epidemiology of breast and gynecological cancers among patients attending Saint Paul’s Hospital Millennium Medical College, Ethiopia. PLoS ONE 2020, 15, e0230625. [Google Scholar] [CrossRef]
- Elston, C.W.; Ellis, I.O. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: Experience from a large study with long-term follow-up. Histopathology 1991, 19, 403–410. [Google Scholar] [CrossRef]
- Edge, S.; Byrd, D.; Compton, C.; Fritz, A.; Greene, F.; Trotti, A. AJCC Cancer Staging Manual, 7th ed.; Springer: New York, NY, USA, 2009. [Google Scholar]
- Kantelhardt, E.; Zerche, P.; Mathewos, A.; Trocchi, P.; Addissie, A.; Aynalem, A.; Wondemagegnehu, T.; Ersumo, T.; Reeler, A.; Yonas, B.; et al. Breast cancer survival in Ethiopia: A cohort study of 1070 women. Int. J. Cancer 2013, 135, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Ersumo, T. Breast cancer in an Ethiopian population, Addis Ababa. East Cent. Afr. J. Surg. 2006, 11, 81–86. [Google Scholar]
- Balekouzou, A.; Yin, P.; Pamatika, C.M.; Bishwajit, G.; Nambei, S.W.; Djeintote, M.; Ouansaba, B.E.; Shu, C.; Yin, M.; Fu, Z.; et al. Epidemiology of breast cancer: Retrospective study in the Central African Republic. BMC Public Health 2016, 16, 1230. [Google Scholar] [CrossRef]
- Rambau, P.F.; Chalya, P.L.; Manyama, M.M.; Jackson, K.J. Pathological features of Breast Cancer seen in Northwestern Tanzania: A nine years retrospective study. BMC Res. Notes 2011, 4, 214. [Google Scholar] [CrossRef]
- Fitzpatrick, M.B.; Rendi, M.H.; Kiviat, N.B.; Toure, P.; Dem, A.; Sow, P.S.; Hawes, S.E.; Feng, Q.; Allison, K.H. Pathology of Senegalese breast cancers. Pan Afr. Med. J. 2019, 34, 67. [Google Scholar] [CrossRef]
- Abdel-Razeq, H.; Iweir, S.; Abdel-Razeq, R.; Rahman, F.A.; Almasri, H.; Bater, R.; Taqash, A.; Abdelkhaleq, H. Differences in clinicopathological characteristics, treatment, and survival outcomes between older and younger breast cancer patients. Sci. Rep. 2021, 11, 14340. [Google Scholar] [CrossRef]
- Akakpo, P.K.; Imbeah, E.G.; Edusei, L.; Naporo, S.; Ulzen-Appiah, K.; Clegg-Lamptey, J.N.; Dedey, F.; Nsaful, J.; Affram, N.; Wiafe, B.; et al. Clinicopathologic characteristics of early-onset breast cancer: A comparative analysis of cases from across Ghana. BMC Womens Health 2023, 23, 5. [Google Scholar] [CrossRef]
- Abdulrahman, G.O.; Rahman, G.A. Epidemiology of Breast Cancer in Europe and Africa. J. Cancer Epidemiol. 2012, 2012, 915610. [Google Scholar] [CrossRef]
- Hadi, N.I.; Jamal, Q. Comparison of clinicopathological characteristics of lymph node positive and lymph node negative breast cancer. Pak. J. Med Sci. 1969, 32, 863–868. [Google Scholar] [CrossRef]
- DeGennaro, V., Jr.; Jiwani, F.; Patberg, E.; Gibbs, M.; Libby, R.; Gabriel, D.; Heldermon, C.D.; Daily, K.; Bernard, J., Jr. Epidemiological, clinical, and histopathological features of breast cancer in Haiti. J. Glob. Oncol. 2018, 4, 1–9. [Google Scholar] [CrossRef]
- Takalkar, U.V.; Asegaonkar, S.B.; Kulkarni, U.; Kodlikeri, P.R.; Kulkarni, U.; Saraf, M.; Advani, S. Clinicopathological Profile of Breast Cancer Patients at a Tertiary Care Hospital in Marathwada Region of Westen India. Asian Pac. J. Cancer Prev. 2016, 17, 2195–2198. [Google Scholar] [CrossRef]
- Legesse, B.; Gedif, T. Knowledge on breast cancer and its prevention among women household heads in Northern Ethiopia. Open J. Prev. Med. 2014, 2014, 32–40. [Google Scholar] [CrossRef]
- Black, E.; Richmond, R. Improving early detection of breast cancer in sub-Saharan Africa: Why mammography may not be the way forward. Glob. Health 2019, 15, 3. [Google Scholar] [CrossRef] [PubMed]
- Titloye, N.; Foster, A.; Omoniyi-Esan, G.; Komolafe, A.; Daramola, A.; Adeoye, O.; Adisa, A.; Manoharan, A.; Pathak, D.; D’Cruz, M.; et al. Histological Features and Tissue Microarray Taxonomy of Nigerian Breast Cancer Reveal Predominance of the High-Grade Triple-Negative Phenotype. Pathobiology 2016, 83, 24–32. [Google Scholar] [CrossRef]
- Maffuz-Aziz, A.; Labastida-Almendaro, S.; Espejo-Fonseca, A.; Rodriguez-Cuevas, S. Clinical and pathological features of breast cancer in a population of Mexico. Cirugía Cir. Engl. Ed. 2017, 85, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Toma, A.; O’Neil, D.; Joffe, M.; Ayeni, O.; Nel, C.; Berg, E.v.d.; Nayler, S.; Cubasch, H.; Phakathi, B.; Buccimazza, I.; et al. Quality of histopathological reporting in breast cancer: Re-sults from four South African breast units. JCO Glob. Oncol. 2021, 7, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Malanda, D.M.M.; Boumba, A.L.M.; Malonga, G.A.; Mouamba, F.G.; Mambouene, F.D.; Moukassa, D.; Peko, J.F. Breast Cancer in Women: Epidemiological, Histological, Immunohistochemical and Molecular Sub-Types in the Republic of Congo. Int. J. Health Sci. Res. 2021, 11, 103–116. [Google Scholar] [CrossRef]
- Adeniji, A.A.; Dawodu, O.O.; Habeebu, M.Y.; Oyekan, A.O.; Bashir, M.A.; Martin, M.G.; Keshinro, S.O.; Fagbenro, G.T. Distribution of Breast Cancer Subtypes Among Nigerian Women and Correlation to the Risk Factors and Clinicopathological Characteristics. World J. Oncol. 2020, 11, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Ezike, K.N.; Raphael, S.; Okonkwo, D.I.; Okwudire-Ijeh, I.A. Pattern of molecular phenotypes of breast carcinomas using immunohistochemistry in a district hospital in Nigeria. Niger. J. Med. 2021, 34, 362–367. [Google Scholar]
- Zilenaite, D.; Rasmusson, A.; Augulis, R.; Besusparis, J.; Laurinaviciene, A.; Plancoulaine, B.; Ostapenko, V.; Laurinavicius, A. Independent Prognostic Value of Intratumoral Heterogeneity and Immune Response Features by Automated Digital Immunohistochemistry Analysis in Early Hormone Receptor-Positive Breast Carcinoma. Front. Oncol. 2020, 10, 950. [Google Scholar] [CrossRef]
- Uyisenga, J.P.; Butera, Y.; Debit, A.; Josse, C.; Ainhoa, C.C.; Karinganire, E.; Cyuzuzo, A.P.; Umurungi, N.; Kalinijabo, Y.; Uwimana, S.; et al. Prevalence of Histological Characteristics of Breast Cancer in Rwanda in Relation to Age and Tumor Stages. Horm. Cancer 2020, 11, 240–249. [Google Scholar] [CrossRef]
- Amend, K.; Hicks, D.; Ambrosone, C.B. Breast Cancer in African-American Women: Differences in Tumor Biology from European-American Women. Cancer Res. 2006, 66, 8327–8330. [Google Scholar] [CrossRef] [PubMed]
- Adani-Ifè, A.; Amégbor, K.; Doh, K.; Darré, T. Breast cancer in togolese women: Immunohistochemistry subtypes. BMC Women’s Health 2020, 20, 261. [Google Scholar] [CrossRef]
- Orang, E.; Marzony, E.T.; Afsharfard, A. Predictive role of tumor size in breast cancer with axillary lymph node involvement-can size of primary tumor be used to omit an unnecessary axillary lymph node dissection? Asian Pac. J. Cancer Prev. 2013, 14, 717–722. [Google Scholar] [CrossRef]
- American Cancer Society. Breast Cancer Facts & Figures 2019–2020; American Cancer Society: Atlanta, GA, USA, 2019; pp. 1–44. [Google Scholar]
- Pathak, R.; Jha, A.; Neupane, P.; Chalise, S.; Basnyat, A. Histopathological evaluation of carcinoma of breast. J. Pathol. Nepal 2016, 6, 922–927. [Google Scholar] [CrossRef]
- Oluogun, W.A.; Adedokun, K.A.; Oyenike, M.A.; Adeyeba, O.A. Histological classification, grading, staging, and prognostic indexing of female breast cancer in an African population: A 10-year retrospective study. Int. J. Health Sci. 2019, 13, 3–9. [Google Scholar]
- Mensah, A.C.; Yarney, J.; Nokoe, S.K.; Opoku, S.; Clegg-Lamptey, J.N. Survival Outcomes of Breast Cancer in Ghana: An Analysis of Clinicopathological Features. Oalib 2016, 3, e2145. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Stages | Tumor Size (T) | Regional Lymph Nodes (N) | Distant Metastases (M) |
|---|---|---|---|
| 0 | Tis | N0 | M0 |
| IA | T1 * | N0 | M0 |
| IB | T0 | N1mi | M0 |
| T1 * | N1mi | M0 | |
| IIA | T0 | N1 ** | M0 |
| T * | N1 ** | M0 | |
| T2 | N0 | M0 | |
| IIB | T2 | N1 | M0 |
| T3 | N0 | M0 | |
| IIIA | T0 | N2 | M0 |
| T1 * | N2 | M0 | |
| T2 | N2 | M0 | |
| T3 | N1 | M0 | |
| T3 | N2 | M0 | |
| IIIB | T4 | N0 | M0 |
| T4 | N1 | M0 | |
| T4 | N2 | M0 | |
| IIIC | Any T | N3 | M0 |
| IV | Any T | Any N | M1 |
| Variables | n (%) | ||
|---|---|---|---|
| Age group | 15–29 | 45 (15.3%) | |
| 30–44 | 136 (46.3) | ||
| 45–59 | 77 (26.2) | ||
| 60–74 | 28 (9.5) | ||
| ≥75 | 8 (2.7) | ||
| Total | 294 (100.0) | ||
| Mean ± Sd (Minimum, Maximum) 42.27 ± 13.57 (17,100) | |||
| Sex | Female | 284 (96.6) | |
| Male | 10 (3.4) | ||
| Total | 294 (100.0) | ||
| Patient residence | Hawassa | 113 (38.4) | |
| Jimma | 181 (61.6) | ||
| Total | 294 (100.0) | ||
| Variables | n (%) | |
|---|---|---|
| Stage | I | 5 (1.9) |
| II | 87 (33.2) | |
| III | 170 (64.9) | |
| Total | 262 (100.0) | |
| Tumor Size | pT1 | 8 (3.1) |
| pT2 | 71 (27.8) | |
| pT3 | 105 (41.2) | |
| pT4 | 71 (27.8) | |
| Total | 255 (100.0) | |
| Grade | I | 29 (21.8) |
| II | 66 (49.6) | |
| III | 38 (28.6) | |
| Total | 133 (100.0) | |
| Lymph node involvement | Positive | 173 (60.5) |
| Negative | 113 (39.5) | |
| Total | 286 (100.0) | |
| Positive lymph nodes at surgery | 1–3 | 70 (43.2) |
| 4–10 | 79 (48.8) | |
| >10 | 13 (8.0) | |
| Total | 162 (100.0) | |
| Type of surgery | Mastectomy | 245 (84.5) |
| Lumpectomy | 2 (0.7) | |
| Incisional biopsy | 43 (14.8) | |
| Total | 290 (100.0) |
| Variables | n (%) | Lymph Node Involvement | χ2 | p-Value | |
|---|---|---|---|---|---|
| Yes | No | ||||
| Tumor Size, n (%) | |||||
| ≤2 cm | 8 (3.1) | 3 (1.9) | 5 (5.4) | 8.55 | 0.033 |
| >2 cm and ≤5 cm | 70 (27.6) | 37 (23.0) | 33 (35.5) | ||
| >5 cm | 105 (41.3) | 75 (46.6) | 25 (26.9) | ||
| Any size extension to the chest wall or skin | 71 (28.0) | 46 (28.6) | 25 (26.9) | ||
| Total | 254 (100.0) | 161 (100.0) | 93 (100.0) | ||
| Type of surgery, n (%) | |||||
| Mastectomy | 242 (85.5) | 165 (95.9) | 77 (69.4) | 39.69 | < 0.001 |
| Lumpectomy | 2 (0.7) | 1 (0.6) | 1 (0.9) | ||
| Incisional biopsy | 39 (13.8) | 6 (3.5) | 33 (29.7) | ||
| Total | 283 (100.0) | 172 (100.0) | 111 (100.0) | ||
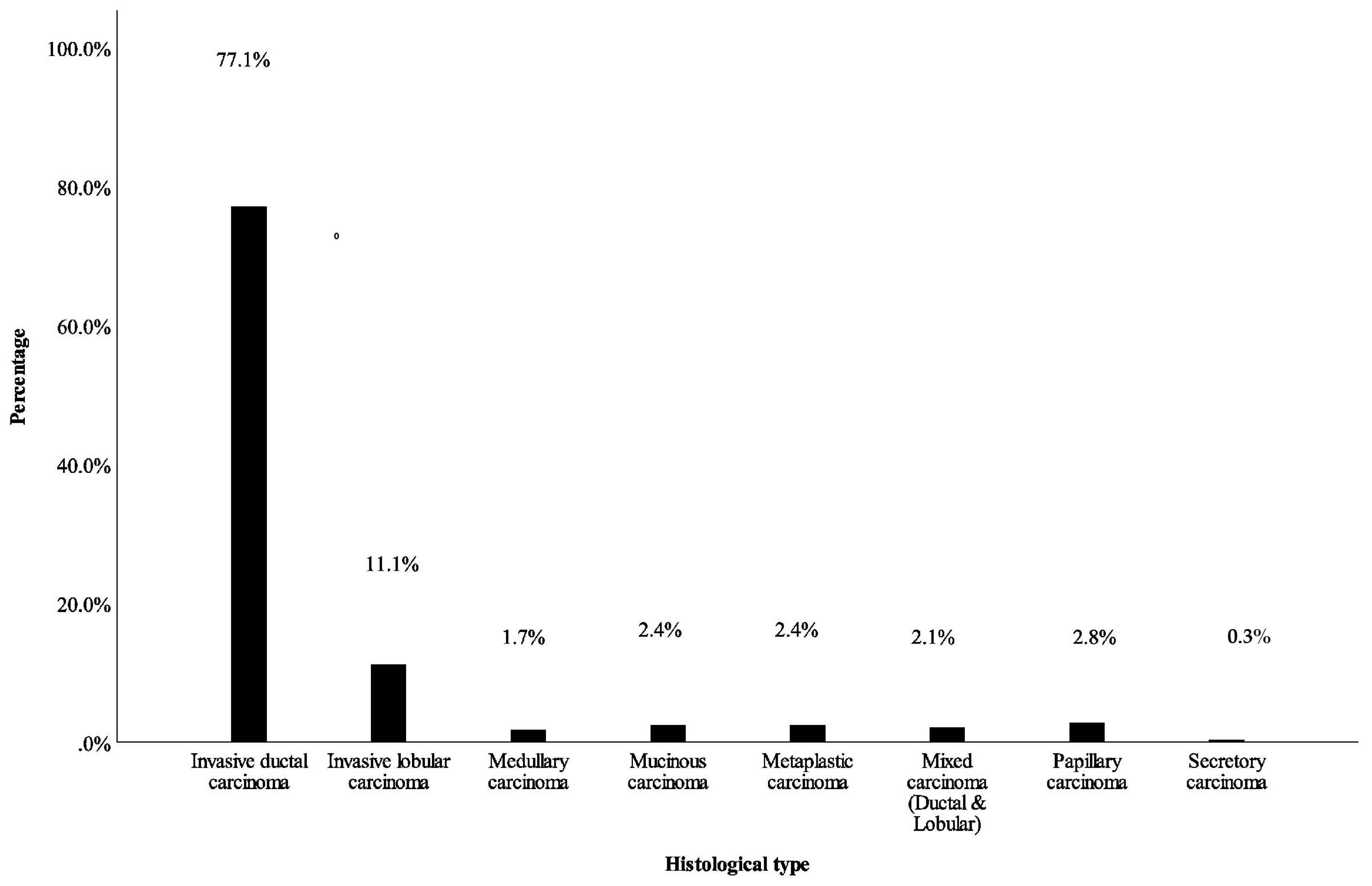
| Histologic type, n (%) | |||||
| Invasive ductal carcinoma | 218 (77.3) | 135 (78.9) | 83 (74.8) | ||
| Invasive lobular carcinoma | 32 (11.3) | 19 (11.1) | 13 (11.7) | 7.4 | 0.37 |
| Mixed carcinoma | 6 (2.1) | 4 (2.3) | 2 (1.8) | ||
| Papillary carcinoma | 7 (2.5) | 2 (1.2) | 5 (4.5) | ||
| Mucinous carcinoma | 6 (2.1) | 2 (1.2) | 4 (3.6) | ||
| Metaplastic carcinoma | 7 (2.5) | 5 (2.9) | 2 (1.8) | ||
| Medullary carcinoma | 5 (1.8) | 4 (2.3) | 1 (0.9) | ||
| Secretory carcinoma | 1 (0.4) | 0 (0.0) | 1 (0.9) | ||
| Total | 282 (100.0) | 171 (100.0) | 111 (100.0) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belachew, E.B.; Desta, A.F.; Deneke, D.B.; Fenta, B.D.; Alem, A.T.; Abafogi, A.K.; Lukas, F.Y.; Bezabih, M.; Sewasew, D.T.; Kantelhardt, E.J.; et al. Clinicopathological Features of Invasive Breast Cancer: A Five-Year Retrospective Study in Southern and South-Western Ethiopia. Medicines 2023, 10, 30. https://doi.org/10.3390/medicines10050030
Belachew EB, Desta AF, Deneke DB, Fenta BD, Alem AT, Abafogi AK, Lukas FY, Bezabih M, Sewasew DT, Kantelhardt EJ, et al. Clinicopathological Features of Invasive Breast Cancer: A Five-Year Retrospective Study in Southern and South-Western Ethiopia. Medicines. 2023; 10(5):30. https://doi.org/10.3390/medicines10050030
Chicago/Turabian StyleBelachew, Esmael Besufikad, Adey Feleke Desta, Dinksira Bekele Deneke, Bizunesh Dires Fenta, Alemwosen Teklehaymanot Alem, Abdo Kedir Abafogi, Fekade Yerakly Lukas, Mesele Bezabih, Dareskedar Tsehay Sewasew, Eva J. Kantelhardt, and et al. 2023. "Clinicopathological Features of Invasive Breast Cancer: A Five-Year Retrospective Study in Southern and South-Western Ethiopia" Medicines 10, no. 5: 30. https://doi.org/10.3390/medicines10050030