

Distinct Phenotypes of Non-Citizen Kidney Transplant Recipients in the United States by Machine Learning Consensus Clustering

 , , ,
, , ,  ,
,  ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Data Collection
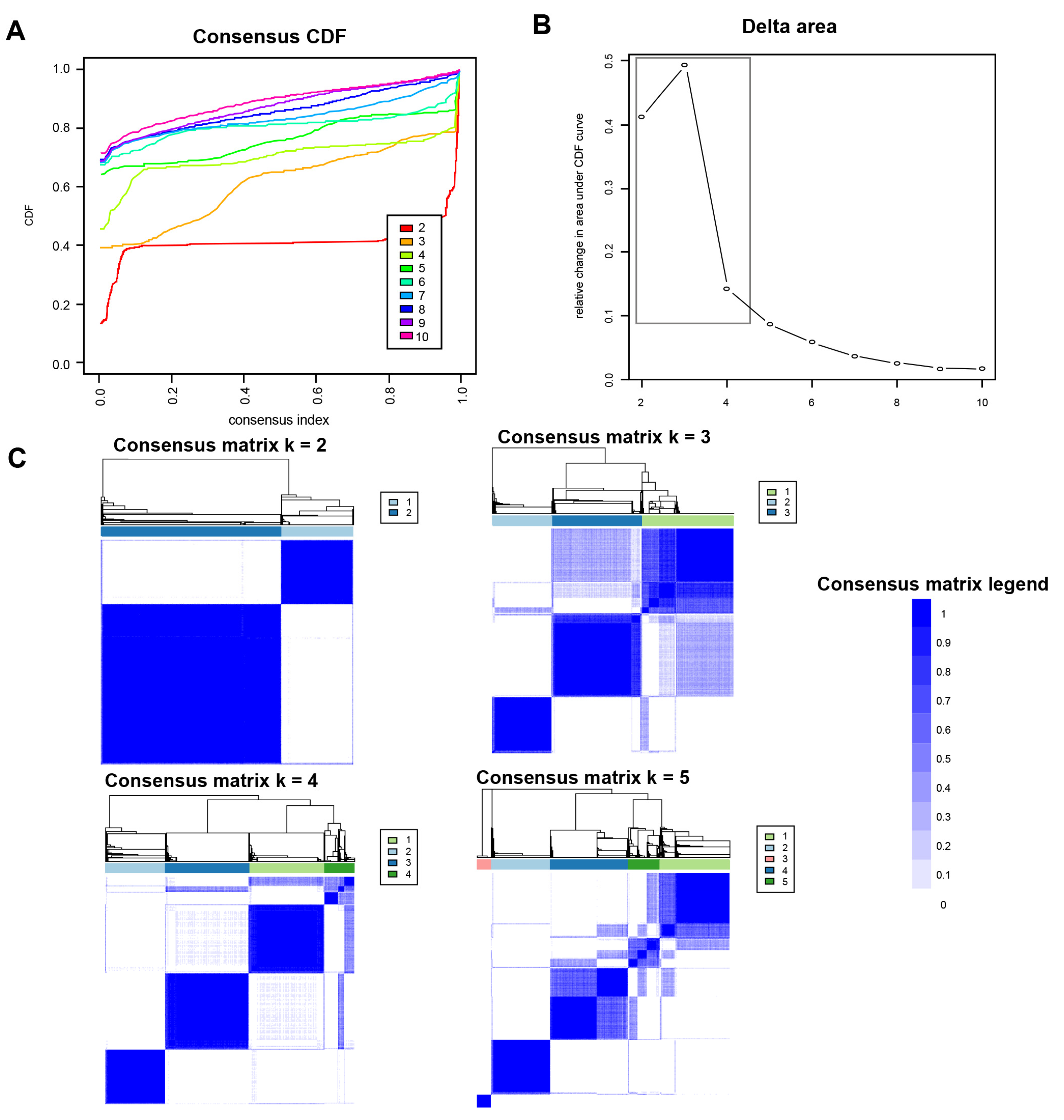
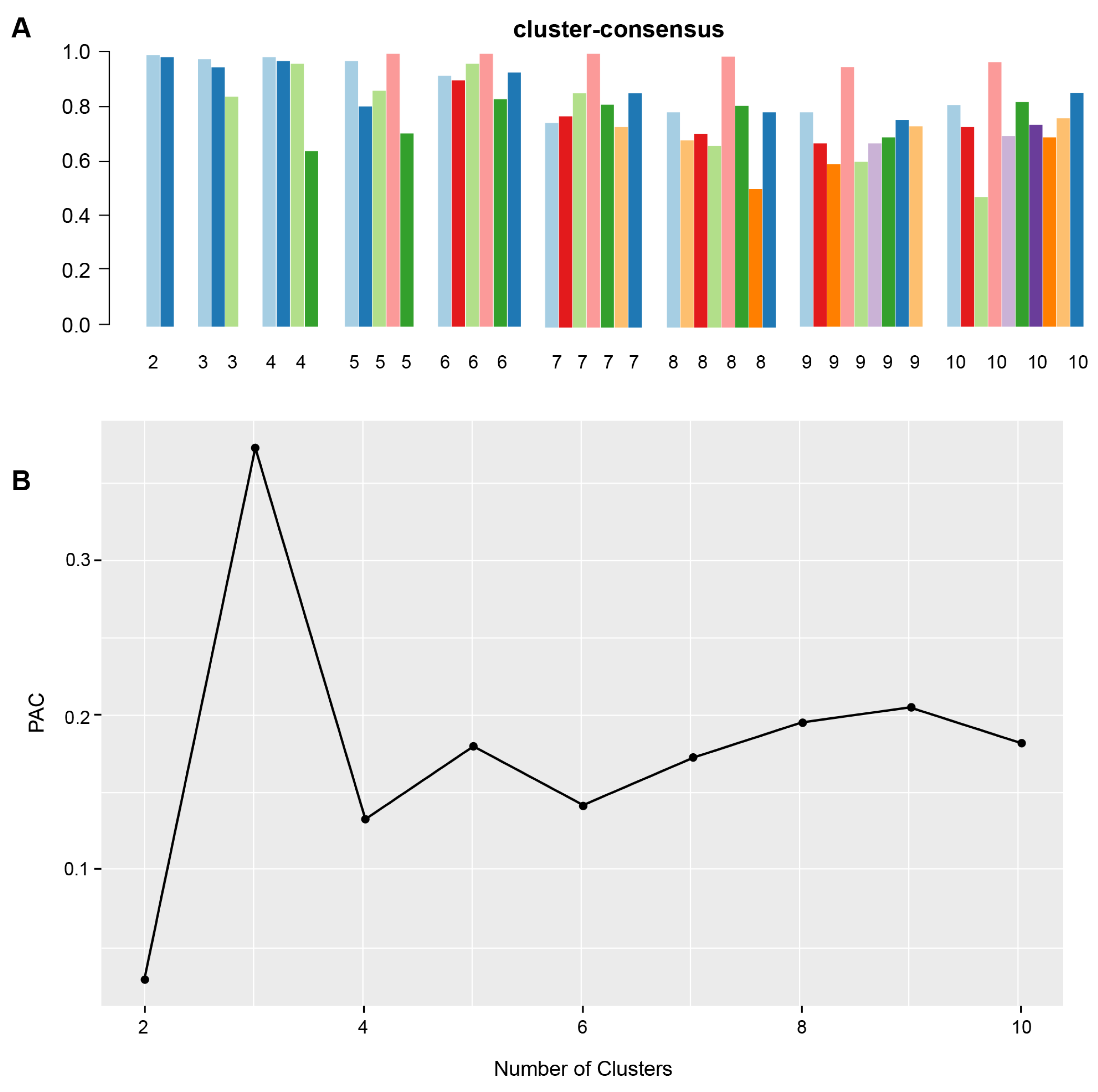
2.3. Clustering Analysis
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics of Each Non-U.S. Citizen Kidney Transplant Cluster
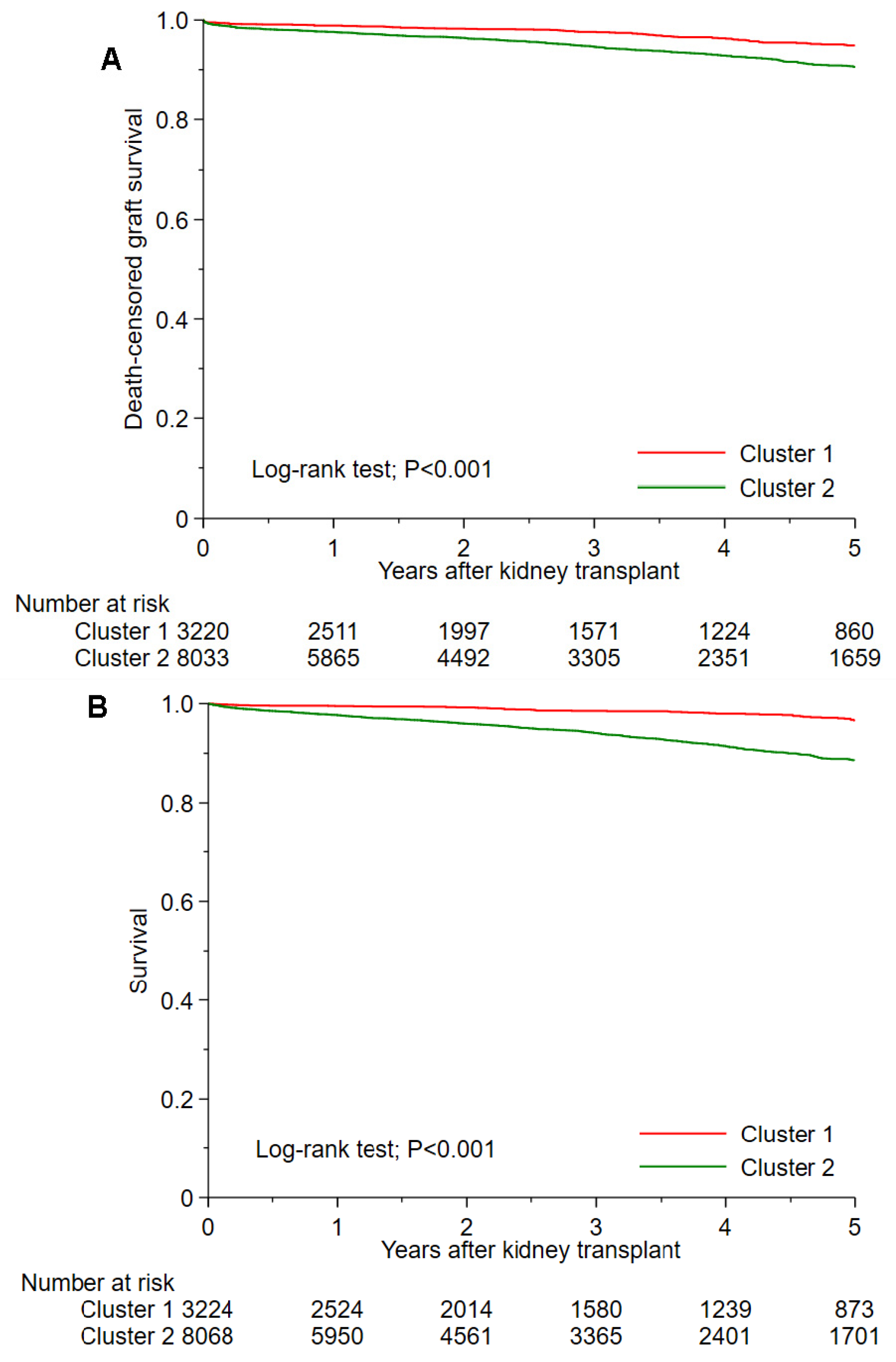
3.2. Post-Transplant Outcomes of Each Non-U.S. Citizen Kidney Transplant Cluster
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- OPTN Policy 17.1.C: Report of Activities Related to The Transplantation of Non-US Citizens/Non-US Residents. Available online: https://optn.transplant.hrsa.gov/media/eavh5bf3/optn_policies.pdf (accessed on 16 October 2021).
- Delmonico, F.L.; Gunderson, S.; Iyer, K.R.; Danovitch, G.M.; Pruett, T.L.; Reyes, J.D.; Ascher, N.L. Deceased Donor Organ Transplantation Performed in the United States for Noncitizens and Nonresidents. Transplantation 2018, 102, 1124–1131. [Google Scholar] [CrossRef] [PubMed]
- Glazier, A.K.; Danovitch, G.M.; Delmonico, F.L. Organ transplantation for nonresidents of the United States: A policy for transparency. Am. J. Transplant. 2014, 14, 1740–1743. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.I.; Hercz, D.; Barba, L.M.; Wilhalme, H.; Lum, E.L.; Huang, E.; Reddy, U.; Salas, L.; Vangala, S.; Norris, K.C. Association of Citizenship Status With Kidney Transplantation in Medicaid Patients. Am. J. Kidney Dis. 2018, 71, 182–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danovitch, G.M.; Cohen, D.J.; Weir, M.R.; Stock, P.G.; Bennett, W.M.; Christensen, L.L.; Sung, R.S. Current status of kidney and pancreas transplantation in the United States, 1994-2003. Am. J. Transplant. 2005, 5, 904–915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McEnhill, M.E.; Brennan, J.L.; Winnicki, E.; Lee, M.M.; Tavakol, M.; Posselt, A.M.; Stock, P.G.; Portale, A.A. Effect of Immigration Status on Outcomes in Pediatric Kidney Transplant Recipients. Am. J. Transplant. 2016, 16, 1827–1833. [Google Scholar] [CrossRef]
- Goldfarb-Rumyantzev, A.S.; Koford, J.K.; Baird, B.C.; Chelamcharla, M.; Habib, A.N.; Wang, B.J.; Lin, S.J.; Shihab, F.; Isaacs, R.B. Role of socioeconomic status in kidney transplant outcome. Clin. J. Am. Soc. Nephrol. 2006, 1, 313–322. [Google Scholar] [CrossRef] [Green Version]
- Schold, J.D.; Meier-Kriesche, H.U.; Duncan, R.P.; Reed, A.I. Deceased donor kidney and liver transplantation to nonresident aliens in the United States. Transplantation 2007, 84, 1548–1556. [Google Scholar] [CrossRef]
- Gupta, C. Immigrants and organ sharing: A one-way street. Virtual Mentor 2008, 10, 229–234. [Google Scholar] [CrossRef]
- Yu, E.; Wightman, A. Pediatric kidney transplant in undocumented immigrants: An American perspectives. Pediatr. Transplant. 2021, 25, e13788. [Google Scholar] [CrossRef]
- Kampaktsis, P.N.; Tzani, A.; Doulamis, I.P.; Moustakidis, S.; Drosou, A.; Diakos, N.; Drakos, S.G.; Briasoulis, A. State-of-the-art machine learning algorithms for the prediction of outcomes after contemporary heart transplantation: Results from the UNOS database. Clin. Transplant. 2021. [Google Scholar] [CrossRef]
- Killian, M.O.; Payrovnaziri, S.N.; Gupta, D.; Desai, D.; He, Z. Machine learning-based prediction of health outcomes in pediatric organ transplantation recipients. JAMIA Open 2021, 4, ooab008. [Google Scholar] [CrossRef] [PubMed]
- Ershoff, B.D.; Lee, C.K.; Wray, C.L.; Agopian, V.G.; Urban, G.; Baldi, P.; Cannesson, M. Training and Validation of Deep Neural Networks for the Prediction of 90-Day Post-Liver Transplant Mortality Using UNOS Registry Data. Transplant. Proc. 2020, 52, 246–258. [Google Scholar] [CrossRef] [PubMed]
- Wadhwani, S.I.; Hsu, E.K.; Shaffer, M.L.; Anand, R.; Ng, V.L.; Bucuvalas, J.C. Predicting ideal outcome after pediatric liver transplantation: An exploratory study using machine learning analyses to leverage Studies of Pediatric Liver Transplantation Data. Pediatr. Transplant. 2019, 23, e13554. [Google Scholar] [CrossRef] [PubMed]
- Schwantes, I.R.; Axelrod, D.A. Technology-Enabled Care and Artificial Intelligence in Kidney Transplantation. Curr. Transplant. Rep 2021, 1–6. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Vaitla, P.; Jadlowiec, C.C.; Leeaphorn, N.; Mao, S.A.; Mao, M.A.; Pattharanitima, P.; Bruminhent, J.; Khoury, N.J.; Garovic, V.D.; et al. Use of Machine Learning Consensus Clustering to Identify Distinct Subtypes of Black Kidney Transplant Recipients and Associated Outcomes. JAMA Surg. 2022, 157, e221286. [Google Scholar] [CrossRef]
- Wilkerson, M.D.; Hayes, D.N. ConsensusClusterPlus: A class discovery tool with confidence assessments and item tracking. Bioinformatics 2010, 26, 1572–1573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacEachern, S.J.; Forkert, N.D. Machine learning for precision medicine. Genome 2021, 64, 416–425. [Google Scholar] [CrossRef]
- Alyousef, A.A.; Nihtyanova, S.; Denton, C.; Bosoni, P.; Bellazzi, R.; Tucker, A. Nearest Consensus Clustering Classification to Identify Subclasses and Predict Disease. J. Healthc. Inform. Res. 2018, 2, 402–422. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Z.; Waikar, S.S.; Schmidt, I.M.; Landis, J.R.; Hsu, C.Y.; Shafi, T.; Feldman, H.I.; Anderson, A.H.; Wilson, F.P.; Chen, J.; et al. Subtyping CKD Patients by Consensus Clustering: The Chronic Renal Insufficiency Cohort (CRIC) Study. J. Am. Soc. Nephrol. 2021, 32, 639–653. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Kattah, A.G.; Mao, M.A.; Keddis, M.T.; Pattharanitima, P.; Vallabhajosyula, S.; Nissaisorakarn, V.; Erickson, S.B.; Dillon, J.J.; Garovic, V.D.; et al. Distinct Phenotypes of Hospitalized Patients with Hyperkalemia by Machine Learning Consensus Clustering and Associated Mortality Risks. Qjm 2021. [Google Scholar] [CrossRef]
- Van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate imputation by chained equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef] [Green Version]
- Monti, S.; Tamayo, P.; Mesirov, J.; Golub, T. Consensus clustering: A resampling-based method for class discovery and visualization of gene expression microarray data. Mach. Learn. 2003, 52, 91–118. [Google Scholar] [CrossRef]
- Șenbabaoğlu, Y.; Michailidis, G.; Li, J.Z. Critical limitations of consensus clustering in class discovery. Sci. Rep. 2014, 4, 6207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenberg, R.; Ballesteros-Gallego, F.; Allard, J.; Fortin, M.C. Organ Transplantation for Foreign Nationals in Canada: A Survey of Transplant Professionals. Can. J. Kidney Health Dis. 2019, 6, 2054358119859530. [Google Scholar] [CrossRef] [Green Version]
- Van Biesen, W.; Vanholder, R.; Vanderhaegen, B.; Lameire, N.; Wanner, C.; Wiecek, A.; Sever, M.S.; Feehally, J.; Kazancioglu, R.; Rondeau, E.; et al. Renal replacement therapy for refugees with end-stage kidney disease: An international survey of the nephrological community. Kidney Int. Suppl. 2016, 6, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, A.M.; Simmerling, M.; Frader, J.E. Why nondocumented residents should have access to kidney transplantation: Arguments for lifting the federal ban on reimbursement. Transplantation 2007, 83, 17–20. [Google Scholar] [CrossRef]
- Diaz, V.A., Jr. Cultural factors in preventive care: Latinos. Prim. Care 2002, 29, 503–517, viii. [Google Scholar] [CrossRef]
- Passel, J.S.; Cohn, D. Mexicans decline to less than half the US unauthorized immigrant population for the first time. Pew Res. Cent. 2019. [Google Scholar]
- Rodriguez, R.; Cervantes, L.; Raghavan, R. Estimating the prevalence of undocumented immigrants with end-stage renal disease in the United States. Clin. Nephrol. 2020, 93, 108–112. [Google Scholar] [CrossRef]
- Jannat-Khah, D.P.; Unterbrink, M.; McNairy, M.; Pierre, S.; Fitzgerald, D.W.; Pape, J.; Evans, A. Treating loss-to-follow-up as a missing data problem: A case study using a longitudinal cohort of HIV-infected patients in Haiti. BMC Public Health 2018, 18, 1269. [Google Scholar] [CrossRef] [Green Version]
- Knol, M.J.; Janssen, K.J.; Donders, A.R.; Egberts, A.C.; Heerdink, E.R.; Grobbee, D.E.; Moons, K.G.; Geerlings, M.I. Unpredictable bias when using the missing indicator method or complete case analysis for missing confounder values: An empirical example. J. Clin. Epidemiol. 2010, 63, 728–736. [Google Scholar] [CrossRef]
- White, I.R.; Carlin, J.B. Bias and efficiency of multiple imputation compared with complete-case analysis for missing covariate values. Stat. Med. 2010, 29, 2920–2931. [Google Scholar] [CrossRef] [PubMed]
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2011, 30, 377–399. [Google Scholar] [CrossRef] [PubMed]
- Hedden, S.L.; Woolson, R.F.; Carter, R.E.; Palesch, Y.; Upadhyaya, H.P.; Malcolm, R.J. The impact of loss to follow-up on hypothesis tests of the treatment effect for several statistical methods in substance abuse clinical trials. J. Subst. Abuse Treat. 2009, 37, 54–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donders, A.R.T.; Van Der Heijden, G.J.; Stijnen, T.; Moons, K.G. A gentle introduction to imputation of missing values. J. Clin. Epidemiol. 2006, 59, 1087–1091. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | Cluster 1 | Cluster 2 | p-Value | |
|---|---|---|---|---|
| (n = 11,300) | (n = 3226) | (n = 8074) | ||
| Recipient Age (year) | 48.4 ± 13.6 | 42.8 ± 14.0 | 50.6 ± 12.8 | <0.001 |
| Recipient male sex | 7058 (62.5) | 2144 (66.5) | 4914 (60.9) | <0.001 |
| Recipient race | ||||
| White | 1117 (9.9) | 569 (17.6) | 548 (6.8) | <0.001 |
| Black | 1101 (9.7) | 198 (6.1) | 903 (11.2) | <0.001 |
| Hispanic | 7023 (62.2) | 1958 (60.7) | 5065 (62.7) | 0.04 |
| Other | 2059 (18.2) | 501 (15.5) | 1558 (19.3) | <0.001 |
| ABO blood group | 0.01 | |||
| A | 3570 (31.6) | 983 (30.5) | 2587 (32.0) | |
| B | 498 (4.4) | 117 (3.6) | 381 (4.7) | |
| AB | 1594 (14.1) | 467 (14.5) | 1127 (14.0) | |
| O | 5638 (49.9) | 1659 (51.4) | 3979 (49.3) | |
| Body mass index (kg/m2) | 26.3 ± 4.8 | 26.1 ± 4.9 | 26.4 ± 4.7 | <0.001 |
| Kidney retransplant | 618 (5.5) | 130 (4.0) | 488 (6.0) | <0.001 |
| Dialysis duration | <0.001 | |||
| Preemptive | 1018 (9.0) | 690 (21.4) | 328 (4.1) | |
| <1 year | 1106 (9.8) | 692 (21.5) | 414 (5.1) | |
| 1–3 years | 6881 (60.9) | 805 (25.0) | 6076 (75.3) | |
| >3 years | 2295 (20.3) | 1039 (32.2) | 1256 (15.6) | |
| Cause of end-stage kidney disease | ||||
| Diabetes mellitus | 3087 (27.3) | 596 (18.5) | 2491 (30.9) | <0.001 |
| Hypertension | 2473 (21.9) | 961 (29.8) | 1512 (18.7) | <0.001 |
| Glomerular disease | 3042 (26.9) | 783 (24.3) | 2259 (28.0) | <0.001 |
| PKD | 612 (5.4) | 203 (6.3) | 409 (5.1) | 0.009 |
| Other | 2086 (18.5) | 683 (21.2) | 1403 (17.4) | <0.001 |
| Comorbidity | ||||
| Diabetes mellitus | 3588 (31.8) | 714 (22.1) | 2874 (35.6) | <0.001 |
| Malignancy | 326 (2.9) | 82 (2.5) | 244 (3.0) | 0.17 |
| Peripheral vascular disease | 788 (7.0) | 156 (4.8) | 632 (7.8) | <0.001 |
| PRA | 0 (0–23) | 0 (0–0) | 0 (0–34) | <0.001 |
| Positive HCV serostatus | 292 (2.6) | 46 (1.4) | 246 (3.0) | <0.001 |
| Positive HBs antigen | 261 (2.3) | 50 (1.5) | 211 (2.6) | 0.001 |
| Positive HIV serostatus | 62 (0.5) | 7 (0.2) | 55 (0.7) | 0.003 |
| Functional status | <0.001 | |||
| 10–30% | 19 (0.2) | 2 (0.1) | 17 (0.2) | |
| 40–70% | 4501 (39.8) | 943 (29.2) | 3558 (44.1) | |
| 80–100% | 6780 (60.0) | 2281 (70.7) | 4499 (55.7) | |
| Working income | 3193 (28.3) | 1407 (43.6) | 1786 (22.1) | <0.001 |
| Public insurance | 8052 (71.3) | 1557 (48.3) | 6495 (80.4) | <0.001 |
| U.S. residency status | <0.001 | |||
| Non-U.S. citizen/U.S. resident | 6217 (55.0) | 1807 (56.0) | 4410 (54.6) | |
| Non-U.S. citizen/non-U.S. resident, travel to U.S. for transplant | 296 (3) | 215 (7) | 81 (1) | |
| Non-U.S. citizen/non-U.S. resident, travel to U.S. for reason other than transplant | ||||
| Resident alien | 994 (9) | 344 (11) | 650 (8) | |
| Non-resident alien | ||||
| 3288 (29.1) | 696 (21.6) | 2592 (32.1) | ||
| 505 (4.5) | 164 (5.1) | 341 (4.2) | ||
| Undergraduate education or above | 3345 (29.6) | 1300 (40.3) | 2045 (25.3) | <0.001 |
| Serum albumin (g/dL) | 4.1 ± 0.6 | 4.0 ± 0.6 | 4.1 ± 0.6 | 0.01 |
| Kidney donor status | <0.001 | |||
| Non-ECD deceased | 7196 (63.7) | 470 (14.6) | 6726 (83.3) | |
| ECD deceased | 1307 (11.6) | 38 (1.2) | 1269 (15.7) | |
| Living | 2797 (24.8) | 2718 (84.3) | 79 (1.0) | |
| ABO incompatibility | 21 (0.2) | 21 (0.7) | 0 (0.0) | <0.001 |
| Donor age | 38.3 ± 15.6 | 37.8 ± 12.4 | 38.5 ± 16.7 | 0.01 |
| Donor male sex | 6377 (56.4) | 1425 (44.2) | 4952 (61.3) | <0.001 |
| Donor race | ||||
| White | 5629 (49.8) | 864 (26.8) | 4765 (59.0) | <0.001 |
| Black | 1117 (9.9) | 200 (6.2) | 917 (11.4) | <0.001 |
| Hispanic | 3623 (32.1) | 1742 (54.0) | 1881 (23.3) | <0.001 |
| Other | 931 (8.2) | 420 (13.0) | 511 (6.3) | <0.001 |
| History of hypertension in donor | 2358 (20.9) | 104 (3.2) | 2254 (27.9) | <0.001 |
| KDPI | <0.001 | |||
| Living donor | 2797 (24.8) | 2718 (84.3) | 79 (1.0) | |
| KDPI < 85 | 7708 (68.2) | 485 (15.0) | 7223 (89.5) | |
| KDPI ≥ 85 | 795 (7.0) | 23 (0.7) | 772 (9.6) | |
| HLA mismatch | ||||
| A | 1 (1–2) | 1 (0–1) | 2 (1–2) | <0.001 |
| B | 2 (1–2) | 1 (1–2) | 2 (1–2) | <0.001 |
| DR | 1 (1–2) | 1 (0–1) | 1 (1–2) | <0.001 |
| ABDR | 4 (3–5) | 3 (2–4) | 5 (4–5) | <0.001 |
| Cold ischemia time (hours) | 14.5 ± 11.0 | 3.6 ± 4.9 | 18.9 ± 9.7 | <0.001 |
| Kidney on pump | 3715 (32.9) | 62 (1.9) | 3653 (45.2) | <0.001 |
| Delay graft function | 2844 (25.2) | 152 (4.7) | 2692 (33.3) | <0.001 |
| Allocation type | <0.001 | |||
| Local | 8905 (78.8) | 3151 (97.7) | 5754 (71.3) | |
| Regional | 1049 (9.3) | 27 (0.8) | 1022 (12.7) | |
| National | 1344 (11.9) | 48 (1.5) | 1296 (16.1) | |
| Foreign | 2 (0.0) | 0 (0.0) | 2 (0.0) | |
| EBV status | ||||
| Low risk | 63 (0.6) | 25 (0.8) | 38 (0.5) | 0.05 |
| Moderate risk | 10,341 (91.5) | 2959 (91.7) | 7382 (91.4) | 0.61 |
| High risk | 896 (7.9) | 242 (7.5) | 654 (8.1) | 0.29 |
| CMV status | ||||
| D-/R- | 506 (4.5) | 199 (6.2) | 307 (3.8) | <0.001 |
| D-/R+ | 3264 (28.9) | 528 (16.4) | 2736 (33.9) | <0.001 |
| D+/R+ | 6819 (60.3) | 2201 (68.2) | 4618 (57.2) | <0.001 |
| D+/R- | 711 (6.3) | 298 (9.2) | 413 (5.1) | <0.001 |
| Induction immunosuppression | ||||
| Thymoglobulin | 6822 (60.4) | 1440 (44.6) | 5382 (66.7) | <0.001 |
| Alemtuzumab | 1438 (12.7) | 557 (17.3) | 881 (10.9) | <0.001 |
| Basiliximab | 2679 (23.7) | 1033 (32.0) | 1646 (20.4) | <0.001 |
| Other | 144 (1.3) | 53 (1.6) | 91 (1.1) | 0.03 |
| No induction | 819 (7.2) | 305 (9.5) | 514 (6.4) | <0.001 |
| Maintenance Immunosuppression | ||||
| Tacrolimus | 10,589 (93.7) | 3036 (94.1) | 7553 (93.5) | 0.27 |
| Cyclosporine | 159 (1.4) | 56 (1.7) | 103 (1.3) | 0.06 |
| Mycophenolate | 10,730 (95.0) | 3052 (94.6) | 7678 (95.1) | 0.28 |
| Azathioprine | 21 (0.2) | 3 (0.1) | 18 (0.2) | 0.15 |
| mTOR inhibitors | 51 (0.5) | 15 (0.5) | 36 (0.4) | 0.89 |
| Steroid | 7942 (70.3) | 2065 (64.0) | 5877 (72.8) | <0.001 |
| Cluster 1 | Cluster 2 | |
|---|---|---|
| One-year death-censored graft failure | 1.2% | 2.7% |
| HR for 1-year death-censored graft failure | 1 (ref) | 2.22 (1.59–3.19) |
| Five-year death-censored graft failure | 5.2% | 9.8% |
| HR for 5-year death-censored graft failure | 1 (ref) | 2.02 (1.63–2.52) |
| One-year death | 0.5% | 2.4% |
| HR for 1-year death | 1 (ref) | 4.68 (2.86–8.27) |
| Five-year death | 3.4% | 11.4% |
| HR for 5-year death | 1 (ref) | 3.92 (2.98–5.17) |
| One-year acute rejection | 4.7% | 4.9% |
| OR for 1-year acute rejection | 1 (ref) | 1.05 (0.87–1.27) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thongprayoon, C.; Vaitla, P.; Jadlowiec, C.C.; Leeaphorn, N.; Mao, S.A.; Mao, M.A.; Qureshi, F.; Kaewput, W.; Qureshi, F.; Tangpanithandee, S.; et al. Distinct Phenotypes of Non-Citizen Kidney Transplant Recipients in the United States by Machine Learning Consensus Clustering. Medicines 2023, 10, 25. https://doi.org/10.3390/medicines10040025
Thongprayoon C, Vaitla P, Jadlowiec CC, Leeaphorn N, Mao SA, Mao MA, Qureshi F, Kaewput W, Qureshi F, Tangpanithandee S, et al. Distinct Phenotypes of Non-Citizen Kidney Transplant Recipients in the United States by Machine Learning Consensus Clustering. Medicines. 2023; 10(4):25. https://doi.org/10.3390/medicines10040025
Chicago/Turabian StyleThongprayoon, Charat, Pradeep Vaitla, Caroline C. Jadlowiec, Napat Leeaphorn, Shennen A. Mao, Michael A. Mao, Fahad Qureshi, Wisit Kaewput, Fawad Qureshi, Supawit Tangpanithandee, and et al. 2023. "Distinct Phenotypes of Non-Citizen Kidney Transplant Recipients in the United States by Machine Learning Consensus Clustering" Medicines 10, no. 4: 25. https://doi.org/10.3390/medicines10040025