
Clinical Benefit of Autologous Platelet-Rich Plasma Infusion in Ovarian Function Rejuvenation: Evidence from a Before-After Prospective Pilot Study


Abstract
:1. Introduction
2. Materials and Methods
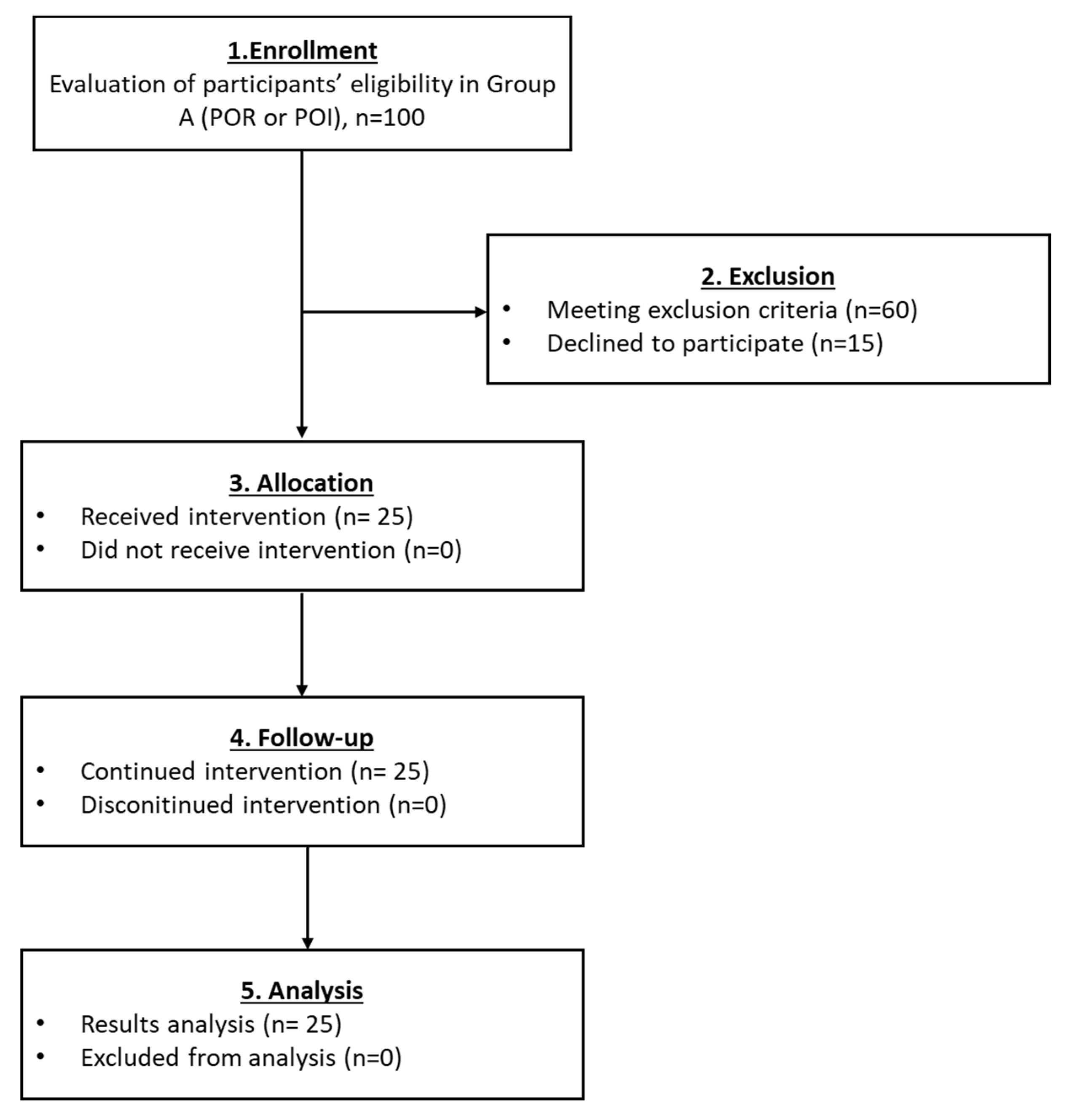
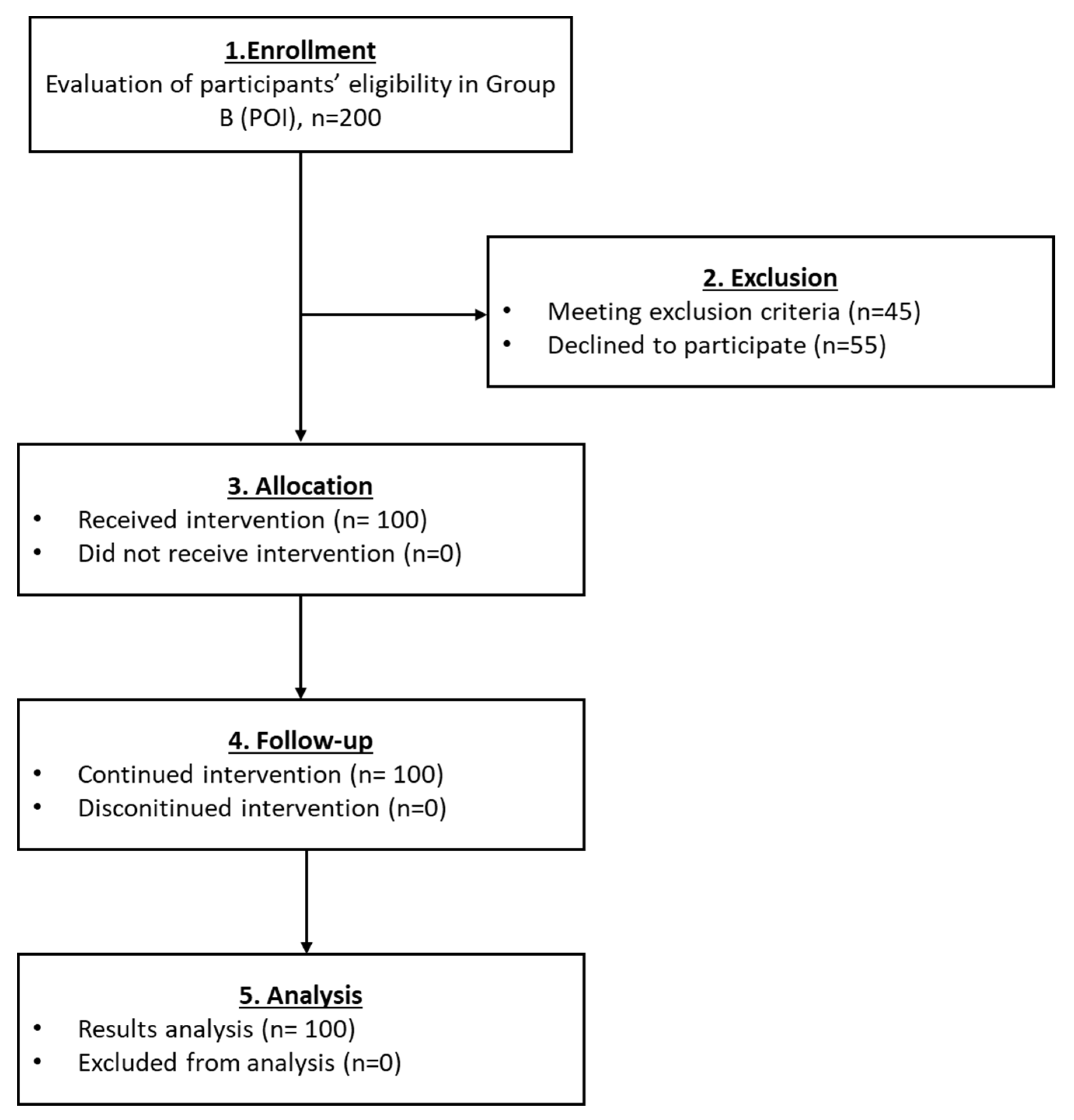
2.1. Study Design
2.2. Exclusion Criteria
2.3. Examination before the PRP Intraovarian Administration
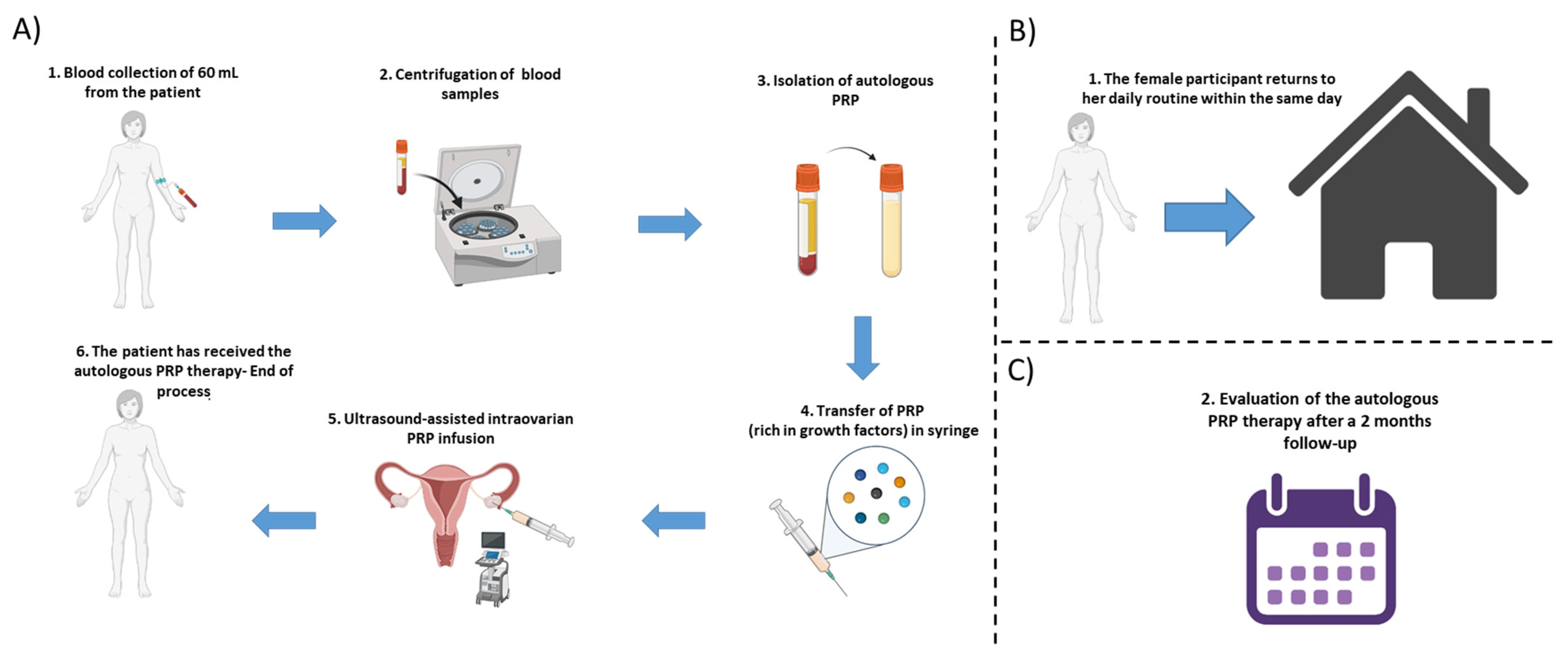
2.4. Preparation Protocol for PRP
2.5. PRP Intraovarian Infusion Methodology
2.6. Follow-Up Monitoring
2.7. Statistical Analysis
3. Results
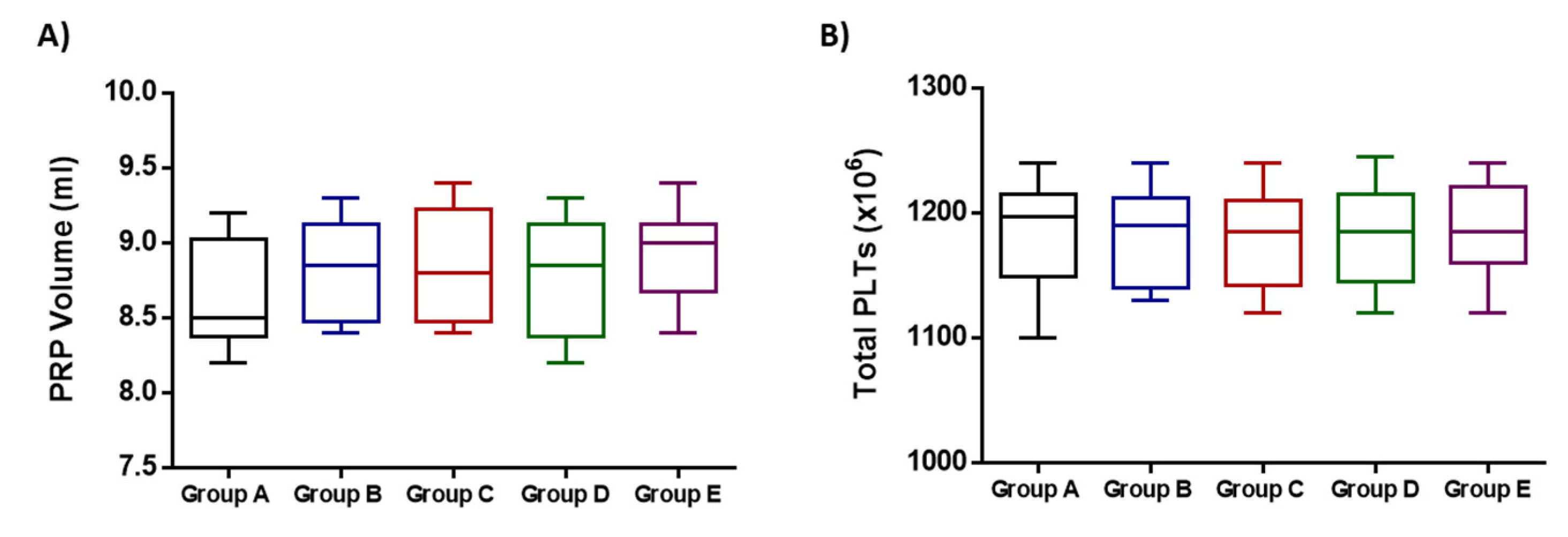
3.1. Assessment of the Intravorian Infusion of PRP
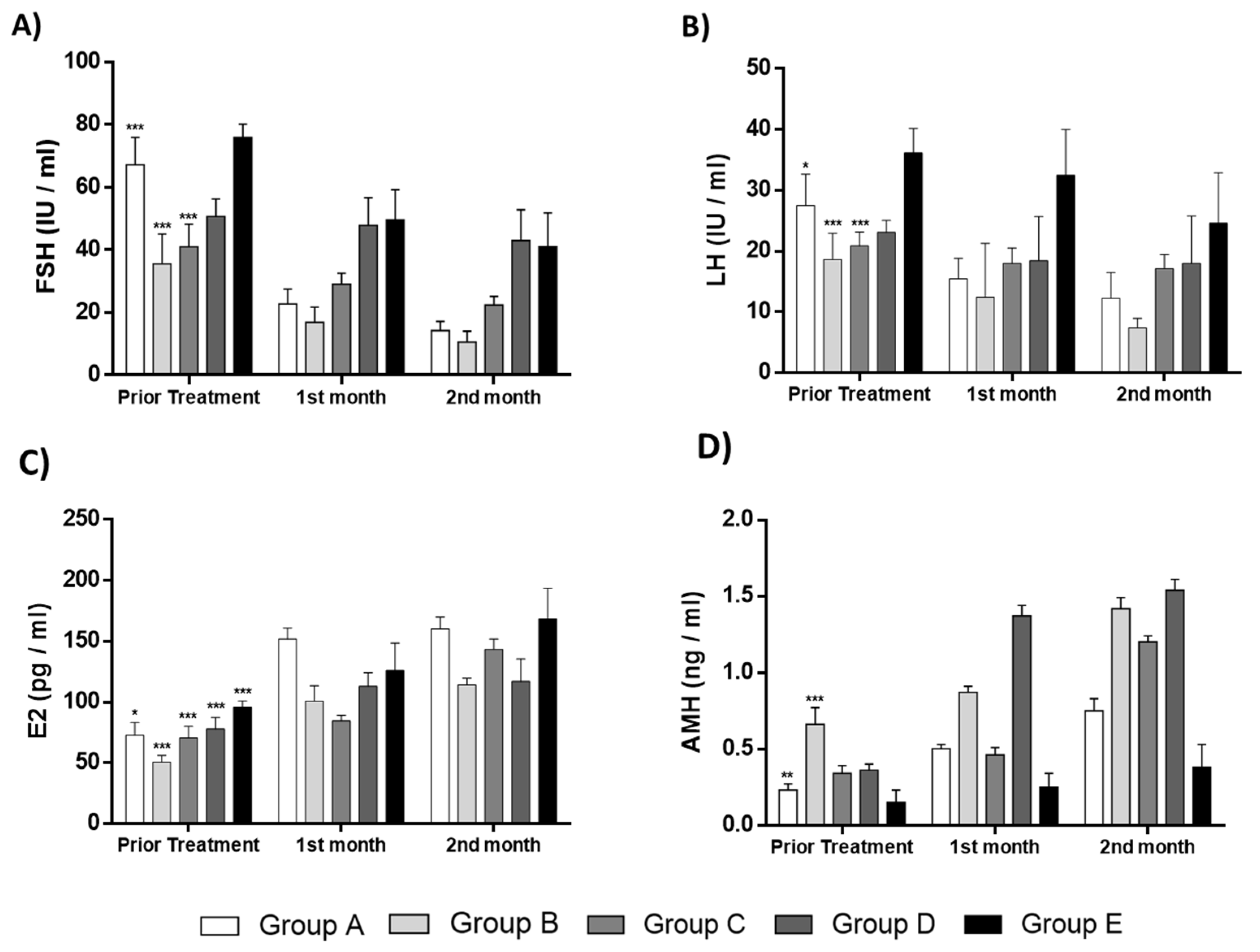
3.2. Evaluation of the Intraovarian PRP Infusion Outcome in All Participants
3.2.1. Results Regarding the Participants of Group A

3.2.2. Results Regarding the Participants of the Group B

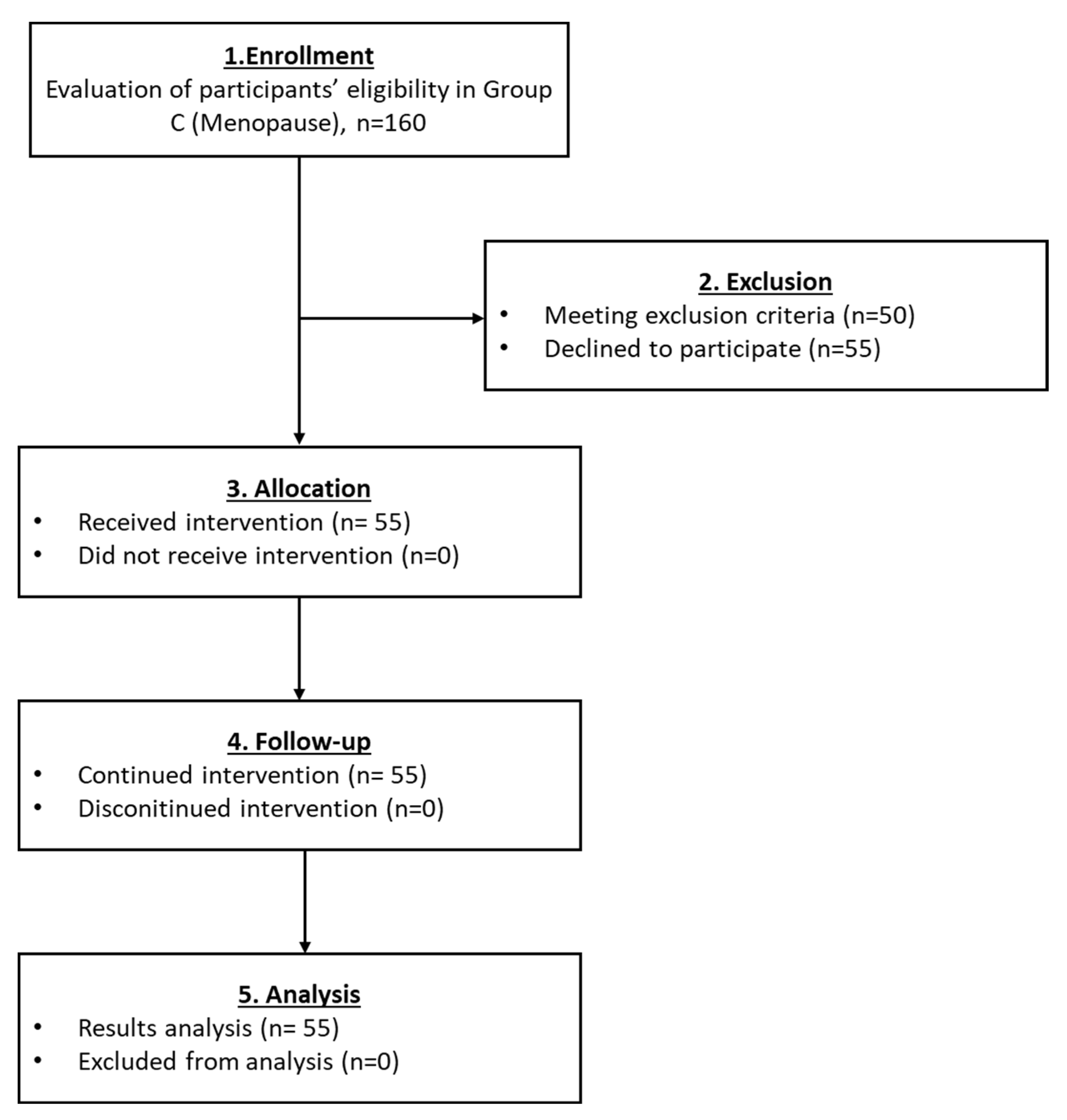
3.2.3. Results Regarding the Participants of Group C

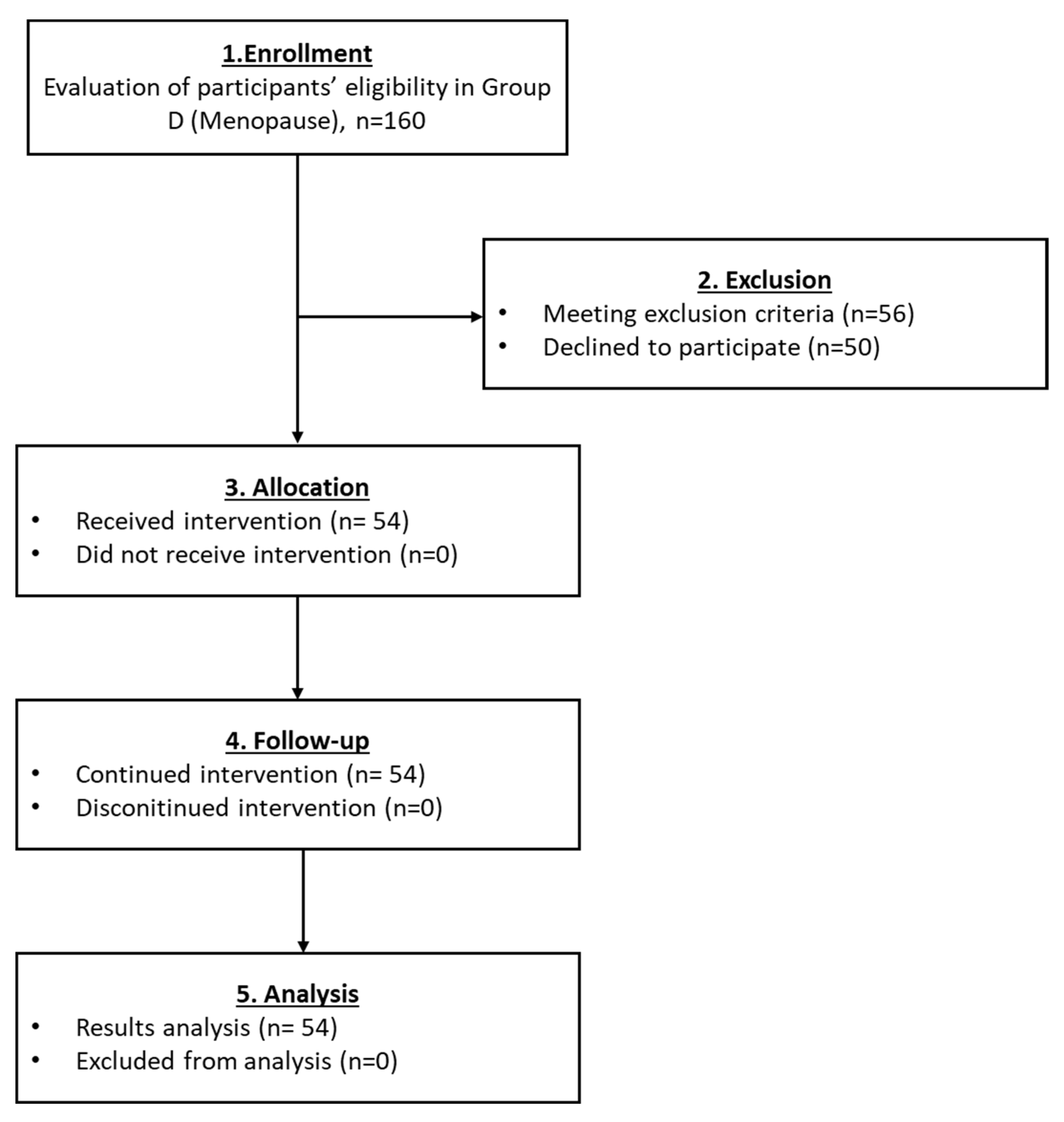
3.2.4. Results Regarding the Participants of Group D

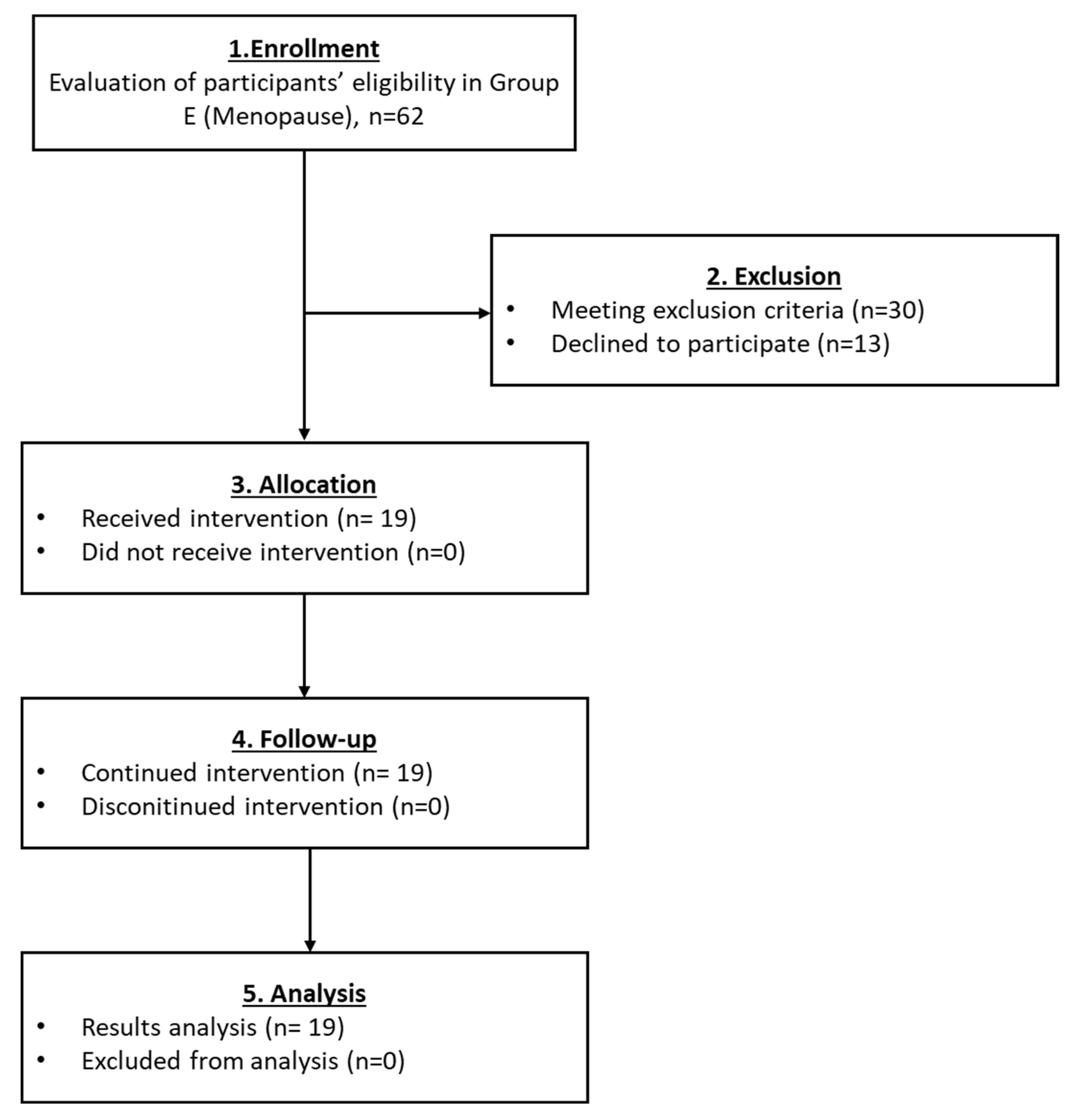
3.2.5. Results Regarding the Participants of Group E
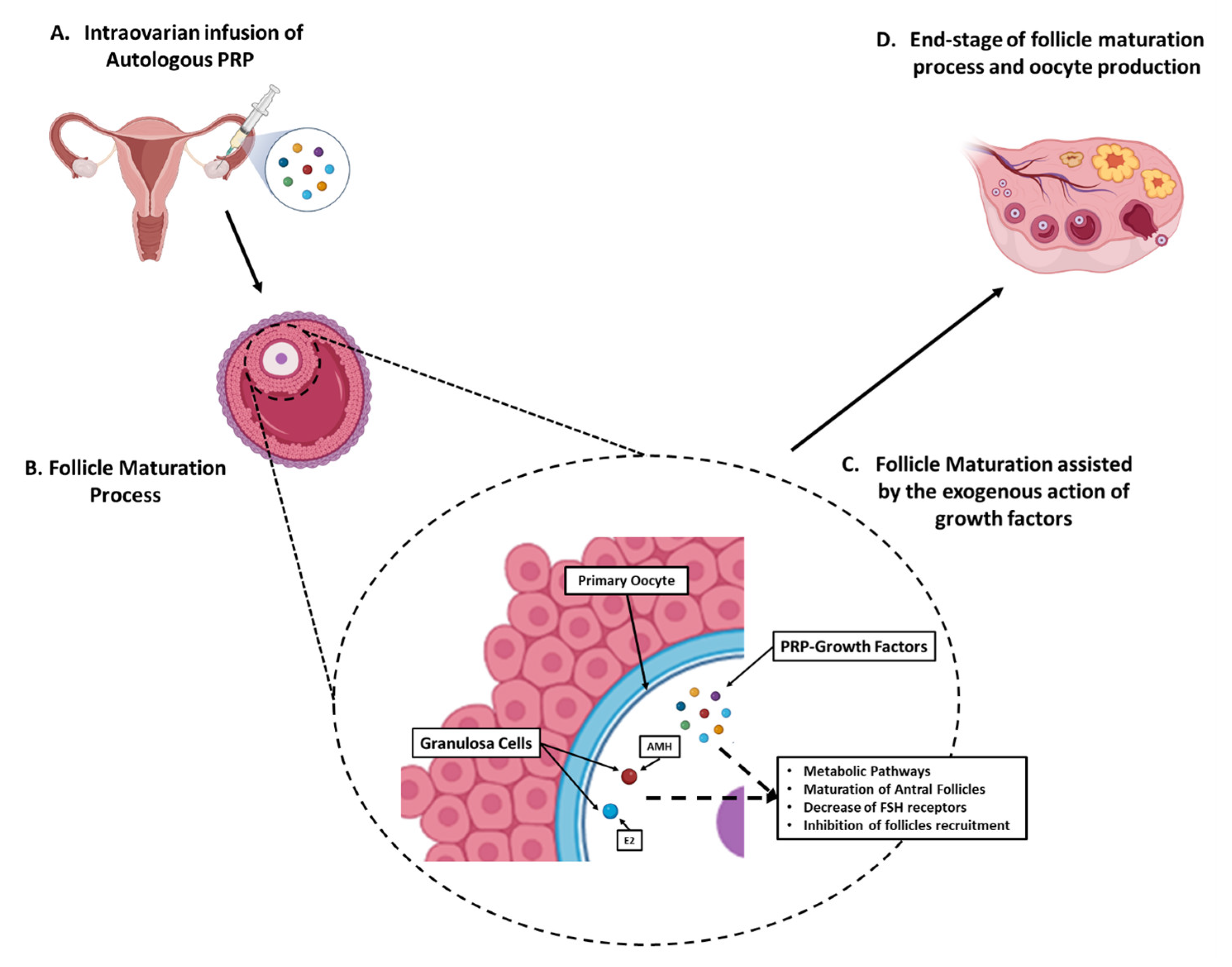
3.3. Proposed Model of Ovarian Rejuvenation Using the Autologous PRP
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rudnicka, E.; Kruszewska, J.; Klicka, K.; Kowalczyk, J.; Grymowicz, M.; Skórska, J.; Pięta, W.; Smolarczyk, R. Premature ovarian insufficiency—Aetiopathology, epidemiology, and diagnostic evaluation. Menopause Rev. 2018, 17, 105–108. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.H.; Milat, F.; Vincent, A. Premature ovarian insufficiency in general practice: Meeting the needs of women. Aust. Fam. Physician 2017, 46, 360–366. [Google Scholar] [PubMed]
- Golezar, S.; Ramezani Tehrani, F.; Khazaei, S.; Ebadi, A.; Keshavarz, Z. The global prevalence of primary ovarian insufficiency and early menopause: A meta-analysis. Climacteric 2019, 22, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Sauer, M.V. In vitro fertilization (IVF): A review of 3 decades of clinical innovation and technological advancement. Ther. Clin. Risk Manag. 2006, 2, 355–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Q.Y.; Chen, S.R.; Chen, J.M.; Shi, Q.Y.; Lin, S. Therapeutic options for premature ovarian insufficiency: An updated review. Reprod. Biol. Endocrinol. 2022, 20, 28. [Google Scholar] [CrossRef] [PubMed]
- Jeve, Y.B.; Bhandari, H.M. Effective treatment protocol for poor ovarian response: A systematic review and meta-analysis. J. Hum. Reprod. Sci. 2016, 9, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Muharam, R.; Sumapraja, K.; Pratama, G.; Azyati, M.; Prabowo, K.A. Impact of IVF on the Timing and Symptoms of Menopause. Int. J. Womens Health 2021, 13, 889–893. [Google Scholar] [CrossRef] [PubMed]
- Allahbadia, G.N. IVF in Developing Economies and Low Resource Countries: An Overview. J. Obstet. Gynaecol. India 2013, 63, 291–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fragoulakis, V.; Maniadakis, N. Estimating the long-term effects of in vitro fertilization in Greece: An analysis based on a lifetime-investment model. ClinicoEcon. Outcomes Res. 2013, 5, 247–255. [Google Scholar] [CrossRef] [Green Version]
- Sfakianoudis, K.; Simopoulou, M.; Rapani, A.; Grigoriadis, S.; Maziotis, E.; Giannelou, P.; Pantou, A.; Vaxevanoglou, T.; Fakiridou, M.; Koutsilieris, M.; et al. The Impact of the Economic Recession in Greece on Assisted Reproduction Demand: A Retrospective Longitudinal Study. Medicina 2019, 55, 654. [Google Scholar] [CrossRef] [Green Version]
- Women Are Having Their First Child at an Older Age. Available online: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/ddn-20200515-2 (accessed on 18 October 2022).
- Bala, R.; Singh, V.; Rajender, S.; Singh, K. Environment, Lifestyle and Female Infertility. Reprod. Sci. 2021, 28, 617–638. [Google Scholar] [CrossRef]
- Gleicher, N.; Kushnir, V.A.; Albertini, D.F.; Barad, D.H. Improvements in IVF in women of advanced age. J. Endocrinol. 2016, 230, F1–F6. [Google Scholar] [CrossRef] [Green Version]
- Petryk, N.; Petryk, M. Ovarian Rejuvenation Through Platelet-Rich Autologous Plasma (PRP)-a Chance to Have a Baby without Donor Eggs, Improving the Life Quality of Women Suffering from Early Menopause without Synthetic Hormonal Treatment. Reprod. Sci. 2020, 27, 1975–1982. [Google Scholar] [CrossRef]
- Matsuda, F.; Inoue, N.; Manabe, N.; Ohkura, S. Follicular growth and atresia in mammalian ovaries: Regulation by survival and death of granulosa cells. J. Reprod. Dev. 2012, 58, 44–50. [Google Scholar] [CrossRef] [Green Version]
- Persani, L.; Rossetti, R.; Cacciatore, C.; Fabre, S. Genetic defects of ovarian TGF-β-like factors and premature ovarian failure. J. Endocrinol. Investig. 2011, 34, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.Z.; Yang, W.; Li, Y.; He, Z. Progress in understanding human ovarian folliculogenesis and its implications in assisted reproduction. J. Assist. Reprod. Genet. 2013, 30, 213–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rimon-Dahari, N.; Yerushalmi-Heinemann, L.; Alyagor, L.; Dekel, N. Ovarian Folliculogenesis. Results Probl. Cell Differ. 2016, 58, 167–190. [Google Scholar] [PubMed]
- Fadini, R.; Coticchio, G.; Brambillasca, F.; Mignini Renzini, M.; Novara, P.V.; Brigante, C.; De Ponti, E.; Dal Canto, M. Clinical outcomes from mature oocytes derived from preovulatory and antral follicles: Reflections on follicle physiology and oocyte competence. J. Assist. Reprod. Genet. 2015, 32, 255–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vegetti, W.; Alagna, F. FSH and folliculogenesis: From physiology to ovarian stimulation. Reprod. Biomed. Online 2006, 12, 684–694. [Google Scholar] [CrossRef]
- Hussein, M.R. Apoptosis in the ovary: Molecular mechanisms. Hum. Reprod. Update 2005, 11, 162–177. [Google Scholar] [CrossRef] [Green Version]
- Erickson, G.F.; Shimasaki, S. The physiology of folliculogenesis: The role of novel growth factors. Fertil. Steril. 2001, 76, 943–949. [Google Scholar] [CrossRef]
- Trombly, D.J.; Woodruff, T.K.; Mayo, K.E. Roles for transforming growth factor beta superfamily proteins in early folliculogenesis. Semin. Reprod. Med. 2009, 27, 14–23. [Google Scholar] [CrossRef] [Green Version]
- Lang, S.; Loibl, M.; Herrmann, M. Platelet-Rich Plasma in Tissue Engineering: Hype and Hope. Eur. Surg. Res. 2018, 59, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi-Ataabadi, M.; Mostafavi-Pour, Z.; Vojdani, Z.; Sani, M.; Latifi, M.; Talaei-Khozani, T. Fabrication and characterization of platelet-rich plasma scaffolds for tissue engineering applications. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 71, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Mallis, P.; Papapanagiotou, A.; Katsimpoulas, M.; Kostakis, A.; Siasos, G.; Kassi, E.; Stavropoulos-Giokas, C.; Michalopoulos, E. Efficient differentiation of vascular smooth muscle cells from Wharton’s Jelly mesenchymal stromal cells using human platelet lysate: A potential cell source for small blood vessel engineering. World J. Stem Cells 2020, 12, 203–221. [Google Scholar] [CrossRef]
- Mazzucco, L.; Balbo, V.; Cattana, E.; Borzini, P. Platelet-rich plasma and platelet gel preparation using Plateltex. Vox Sang. 2008, 94, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Cavallo, C.; Roffi, A.; Grigolo, B.; Mariani, E.; Pratelli, L.; Merli, G.; Kon, E.; Marcacci, M.; Filardo, G. Platelet-Rich Plasma: The Choice of Activation Method Affects the Release of Bioactive Molecules. Biomed. Res. Int. 2016, 2016, 6591717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, F.; Kakudo, N.; Morimoto, N.; Taketani, S.; Hara, T.; Ogawa, T.; Kusumoto, K. Platelet-rich plasma enhances the proliferation of human adipose stem cells through multiple signaling pathways. Stem Cell Res. Ther. 2018, 9, 107. [Google Scholar] [CrossRef]
- Farghali, H.A.; AbdElKader, N.A.; Fathi, M.; Emam, I.A.; AbuBakr, H.O.; Alijuaydi, S.H.; Salem, N.Y.; Khattab, M.S.; Salama, A.; Ramadan, E.S.; et al. The efficiency of intrauterine infusion of platelet-rich plasma in the treatment of acute endometritis as assessed by endoscopic, Doppler, oxidative, immunohistochemical, and gene expression alterations in jennies. Theriogenology 2022, 181, 147–160. [Google Scholar] [CrossRef]
- Sfakianoudis, K.; Simopoulou, M.; Nitsos, N.; Lazaros, L.; Rapani, A.; Pantou, A.; Koutsilieris, M.; Nikas, Y.; Pantos, K. Successful Implantation and Live Birth Following Autologous Platelet-rich Plasma Treatment for a Patient with Recurrent Implantation Failure and Chronic Endometritis. In Vivo 2019, 33, 515–521. [Google Scholar] [CrossRef] [Green Version]
- Merhi, Z.; Seckin, S.; Mouanness, M. Intraovarian PRP Injection Improved Hot Flashes in a Woman with Very Low Ovarian Reserve. Reprod. Sci. 2022, 29, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Cakiroglu, Y.; Saltik, A.; Yuceturk, A.; Karaosmanoglu, O.; Kopuk, S.Y.; Scott, R.T.; Tiras, B.; Seli, E. Effects of intraovarian injection of autologous platelet rich plasma on ovarian reserve and IVF outcome parameters in women with primary ovarian insufficiency. Aging 2020, 12, 10211–10222. [Google Scholar] [CrossRef] [PubMed]
- Sills, E.S.; Rickers, N.S.; Li, X.; Palermo, G.D. First data on in vitro fertilization and blastocyst formation after intraovarian injection of calcium gluconate-activated autologous platelet rich plasma. Gynecol. Endocrinol. 2018, 34, 756–760. [Google Scholar] [CrossRef] [PubMed]
- Seckin, S.; Ramadan, H.; Mouanness, M.; Kohansieh, M.; Merhi, Z. Ovarian response to intraovarian platelet-rich plasma (PRP) administration: Hypotheses and potential mechanisms of action. J. Assist. Reprod. Genet. 2022, 39, 37–61. [Google Scholar] [CrossRef] [PubMed]
- Stenson, A.L.; Kapungu, C.T.; Geller, S.E.; Miller, S. Navigating the challenges of global reproductive health research. J. Womens Health (Larchmt). 2010, 19, 2101–2107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sfakianoudis, K.; Simopoulou, M.; Grigoriadis, S.; Pantou, A.; Tsioulou, P.; Maziotis, E.; Rapani, A.; Giannelou, P.; Nitsos, N.; Kokkali, G.; et al. Reactivating Ovarian Function through Autologous Platelet-Rich Plasma Intraovarian Infusion: Pilot Data on Premature Ovarian Insufficiency, Perimenopausal, Menopausal, and Poor Responder Women. J. Clin. Med. 2020, 10, 1809. [Google Scholar] [CrossRef]
- Available online: https://clinicaltrials.gov/ct2/results?cond=Premature+Ovarian+Failure%2C+menopause&term=platelet+rich+plasma&cntry=&state=&city=&dist= (accessed on 20 October 2022).
- Verma, R.; Kumar, S.; Garg, P.; Verma, Y.K. Platelet-rich plasma: A comparative and economical therapy for wound healing and tissue regeneration. Cell Tissue Bank. 2022, 12, 1–22. [Google Scholar] [CrossRef]
- Ferrari, A.R.; Cortrezzi, S.; Borges, E.J.; Braga, D.; Souza, M.D.C.B.; Antunes, R.A. Evaluation of the Effects of Platelet-Rich Plasma on Follicular and Endometrial Growth: A Literature Review. JBRA Assist. Reprod. 2021, 25, 601–607. [Google Scholar] [CrossRef]
- Ishizuka, B. Current Understanding of the Etiology, Symptomatology, and Treatment Options in Premature Ovarian Insufficiency (POI). Front. Endocrinol. 2021, 12, 626924. [Google Scholar] [CrossRef]
- Fraser, H.M. Regulation of the ovarian follicular vasculature. Reprod. Biol. Endocrinol. 2006, 4, 18. [Google Scholar] [CrossRef] [Green Version]
- McFee, R.M.; Rozell, T.G.; Cupp, A.S. The balance of proangiogenic and antiangiogenic VEGFA isoforms regulate follicle development. Cell Tissue Res. 2012, 349, 635–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikhael, S.; Punjala-Patel, A.; Gavrilova-Jordan, L. Hypothalamic-Pituitary-Ovarian Axis Disorders Impacting Female Fertility. Biomedicines 2019, 7, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mallis, P.; Michalopoulos, E.; Sarri, E.F.; Papadopoulou, E.; Theodoropoulou, V.; Katsimpoulas, M.; Stavropoulos-Giokas, C. Evaluation of the Regenerative Potential of Platelet-Lysate and Platelet-Poor Plasma Derived from the Cord Blood Units in Corneal Wound Healing Applications: An In Vitro Comparative Study on Corneal Epithelial Cells. Curr. Issues Mol. Biol. 2022, 44, 4415–4438. [Google Scholar] [CrossRef] [PubMed]
- Medenica, S.; Abazovic, D.; Ljubić, A.; Vukovic, J.; Begovic, A.; Cucinella, G.; Zaami, S.; Gullo, G. The Role of Cell and Gene Therapies in the Treatment of Infertility in Patients with Thyroid Autoimmunity. Int. J. Endocrinol. 2022, 2022, 4842316. [Google Scholar] [CrossRef]
- Cevher Akdulum, M.F.; Erdem, M.; Barut, G.; Demirdag, E.; İyidir, Ö.T.; Guler, I.; Erdem, A. The relationship between thyroid autoimmunity and poor response to ovarian stimulation in in vitro fertilization women with infertility. Endokrynol. Pol. 2022, 73, 699–705. [Google Scholar] [CrossRef]
- Collins, P. Risk factors for cardiovascular disease and hormone therapy in women. Heart 2006, 92 (Suppl. 3), iii24-8. [Google Scholar] [CrossRef]
- Delamater, L.; Santoro, N. Management of the Perimenopause. Clin. Obstet. Gynecol. 2018, 61, 419–432. [Google Scholar] [CrossRef]
- Coopman, K.; Medcalf, N. From Production to Patient: Challenges and Approaches for Delivering Cell Therapies; Harvard Stem Cell Institute: Cambridge, MA, USA, 2014. Available online: https://www.ncbi.nlm.nih.gov/books/NBK208660/figure/fromproductiontopatientchallengesan.T1/ (accessed on 12 October 2022).
- Fitzpatrick, J.; Bulsara, M.K.; McCrory, P.R.; Richardson, M.D.; Zheng, M.H. Analysis of Platelet-Rich Plasma Extraction: Variations in Platelet and Blood Components Between 4 Common Commercial Kits. Orthop. J. Sports Med. 2017, 5, 2325967116675272. [Google Scholar] [CrossRef] [Green Version]
- Dhurat, R.; Sukesh, M. Principles and Methods of Preparation of Platelet-Rich Plasma: A Review and Author’s Perspective. J. Cutan. Aesthet. Surg. 2014, 7, 189–197. [Google Scholar] [CrossRef]
- Zadehmodarres, S.; Salehpour, S.; Saharkhiz, N.; Nazari, L. Treatment of thin endometrium with autologous platelet-rich plasma: A pilot study. JBRA Assist. Reprod. 2017, 21, 54–56. [Google Scholar] [CrossRef]
- Coksuer, H.; Akdemir, Y.; Barut, M.U. Improved in vitro fertilization success and pregnancy outcome with autologous platelet-rich plasma treatment in unexplained infertility patients that had repeated implantation failure history. Gynecol. Endocrinol. 2019, 35, 815–818. [Google Scholar] [CrossRef] [PubMed]
- Tehraninejad, E.S.; Kashani, N.G.; Hosseini, A.; Tarafdari, A. Autologous platelet-rich plasma infusion does not improve pregnancy outcomes in frozen embryo transfer cycles in women with history of repeated implantation failure without thin endometrium. J. Obstet. Gynaecol. Res. 2021, 47, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Eftekhar, M.; Neghab, N.; Naghshineh, E.; Khani, P. Can autologous platelet rich plasma expand endometrial thickness and improve pregnancy rate during frozen-thawed embryo transfer cycle? A randomized clinical trial. Taiwan J. Obstet. Gynecol. 2018, 57, 810–813. [Google Scholar] [CrossRef] [PubMed]
- Russell, S.J.; Kwok, Y.S.S.; Nguyen, T.T.N.; Librach, C. Autologous platelet-rich plasma improves the endometrial thickness and live birth rate in patients with recurrent implantation failure and thin endometrium. J. Assist. Reprod. Genet. 2022, 39, 1305–1312. [Google Scholar] [CrossRef]
- Simionescu, G.; Doroftei, B.; Maftei, R.; Obreja, B.E.; Anton, E.; Grab, D.; Ilea, C.; Anton, C. The complex relationship between infertility and psychological distress (Review). Exp. Ther. Med. 2021, 21, 306. [Google Scholar] [CrossRef]
- Patel, M. The socioeconomic impact of infertility on women in developing countries. Facts Views Vis. Obgyn. 2016, 8, 59–61. [Google Scholar]
- Nelson, L.M. Clinical practice. Primary ovarian insufficiency. N. Engl. J. Med. 2009, 360, 606–614. [Google Scholar] [CrossRef]
- Mallis, P.; Michalopoulos, E.; Chatzistamatiou, T.; Giokas, C.S. Interplay between mesenchymal stromal cells and immune system: Clinical applications in immune-related diseases. Explor. Immunol. 2021, 1, 112–139. [Google Scholar] [CrossRef]
- Yoon, S.Y. Mesenchymal stem cells for restoration of ovarian function. Clin. Exp. Reprod. Med. 2019, 46, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Ulin, M.; Cetin, E.; Hobeika, E.; Chugh, R.M.; Park, H.S.; Esfandyari, S.; Al-Hendy, A. Human Mesenchymal Stem Cell Therapy and Other Novel Treatment Approaches for Premature Ovarian Insufficiency. Reprod. Sci. 2021, 28, 1688–1696. [Google Scholar] [CrossRef]
- Mashayekhi, M.; Mirzadeh, E.; Chekini, Z.; Ahmadi, F.; Eftekhari-Yazdi, P.; Vesali, S.; Madani, T.; Aghdami, N. Evaluation of safety, feasibility and efficacy of intra-ovarian transplantation of autologous adipose derived mesenchymal stromal cells in idiopathic premature ovarian failure patients: Non-randomized clinical trial, phase I, first in human. J. Ovarian Res. 2021, 14, 5. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Eligibility Criteria | Standard Examination before the PRP Intraovarian Infusion | Follow-Up Monitoring | Assessment of the Outcome after the PRP Infusion |
|---|---|---|---|---|
| A (n = 100) | Age: 22–38 years POR or POI | Determination of FSH, LH, AMH and E2 levels | Performed at 1st and 2nd month | Determination of FSH, LH, AMH and E2 levels Successful Pregnancy: Y/N After Natural Conceive Or IVF Cycle Or ICSI-ET Cycle |
| B (n = 200) | Age: 39–44 years POI Perimenopause | |||
| C (n = 160) | Age: 45–57 years Menopause | |||
| D (n = 160) | Age: 48–50 Menopause | |||
| E (n = 62) | Age: 51–56 Menopause |
| Participant’s Characteristics | Biochemical Parameters | Prior Treatment | Month 1 Follow-Up | Month 2 Follow-Up | p-Value | |
|---|---|---|---|---|---|---|
| n | 25 | FSH (IU/mL) | 67.15 ± 8.72 | 22.74 ± 4.75 | 14.17 ± 2.93 | 0.001 |
| Age | 29.8 ± 3.9 | LH (IU/mL) | 27.51 ± 5.13 | 15.42 ± 3.42 | 12.25 ± 4.21 | 0.046 |
| Number of Pregnancies | 6 | E2 (pg/mL) | 72.78 ± 10.42 | 152.05 ± 8.73 | 160.02 ± 9.85 | 0.035 |
| Number of Live Births | 6 | AMH (ng/mL) | 0.23 ± 0.04 | 0.50 ± 0.03 | 0.75 ± 0.08 | 0.012 |
| Participant’s Characteristics | Biochemical Parameters | Prior Treatment | Month 1 Follow-Up | Month 2 Follow-Up | p-Value | |
|---|---|---|---|---|---|---|
| n | 100 | FSH (IU/mL) | 35.52 ± 9.53 | 16.85 ± 4.86 | 10.58 ± 3.42 | <0.001 |
| Age | 42.1 ± 2.1 | LH (IU/mL) | 18.64 ± 4.31 | 12.42 ± 8.87 | 7.38 ± 1.58 | 0.001 |
| Number of Pregnancies | 28 | E2 (pg/mL) | 50.45 ± 5.62 | 100.68 ± 12.85 | 114.04 ± 5.63 | <0.001 |
| Number of Live Births | 28 | AMH (ng/mL) | 0.66 ± 0.11 | 0.87 ± 0.04 | 1.42 ± 0.07 | <0.001 |
| Participant’s Characteristics | Biochemical Parameters | Prior Treatment | Month 1 Follow-Up | Month 2 Follow-Up | p-Value | |
|---|---|---|---|---|---|---|
| n | 55 | FSH (IU/mL) | 40.85 ± 7.24 | 29.91 ± 3.55 | 22.35 ± 2.81 | <0.001 |
| Age | 45.8 ± 0.7 | LH (IU/mL) | 20.91 ± 2.25 | 18.02 ± 2.48 | 17.10 ± 2.36 | <0.001 |
| Number of Pregnancies | 7 | E2 (pg/mL) | 70.46 ± 9.73 | 84.55 ± 4.56 | 143.26 ± 8.75 | <0.001 |
| Number of Live Births | 7 | AMH (ng/mL) | 0.34 ± 0.05 | 0.46 ± 0.05 | 1.20 ± 0.04 | 0.656 |
| Participant’s Characteristics | Biochemical Parameters | Prior Treatment | Month 1 Follow-Up | Month 2 Follow-Up | p-Value | |
|---|---|---|---|---|---|---|
| n | 54 | FSH (IU/mL) | 50.59 ± 5.64 | 47.81 ± 8.85 | 42.95 ± 9.84 | 0.514 |
| Age | 48.3 ± 1.6 | LH (IU/mL) | 23.09 ± 1.98 | 18.43 ± 7.26 | 18.03 ± 7.75 | 0.869 |
| Number of Pregnancies | 2 | E2 (pg/mL) | 77.71 ± 9.90 | 113.12 ± 10.84 | 116.95 ± 18.45 | 0.003 |
| Number of Live Births | 2 | AMH (ng/mL) | 0.36 ± 0.04 | 1.37 ± 0.07 | 1.54 ± 0.07 | 0.618 |
| Participant’s Characteristics | Biochemical Parameters | Prior Treatment | Month 1 Follow-Up | Month 2 Follow-Up | p-Value | |
|---|---|---|---|---|---|---|
| n | 19 | FSH (IU/mL) | 75.91 ± 4.21 | 49.56 ± 9.68 | 41.07 ± 10.76 | 0.319 |
| Age | 51.61 ± 2.64 | LH (IU/mL) | 36.13 ± 4.04 | 32.47 ± 7.56 | 24.62 ± 8.29 | 0.773 |
| Number of Pregnancies | - | E2 (pg/mL) | 95.68 ± 5.32 | 126.11 ± 22.5 | 168.47. ± 25.09 | 0.002 |
| Number of Live Births | - | AMH (ng/mL) | 0.15± 0.08 | 0.25 ± 0.09 | 0.38 ± 0.15 | 0.860 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garavelas, A.; Mallis, P.; Michalopoulos, E.; Nikitos, E. Clinical Benefit of Autologous Platelet-Rich Plasma Infusion in Ovarian Function Rejuvenation: Evidence from a Before-After Prospective Pilot Study. Medicines 2023, 10, 19. https://doi.org/10.3390/medicines10030019
Garavelas A, Mallis P, Michalopoulos E, Nikitos E. Clinical Benefit of Autologous Platelet-Rich Plasma Infusion in Ovarian Function Rejuvenation: Evidence from a Before-After Prospective Pilot Study. Medicines. 2023; 10(3):19. https://doi.org/10.3390/medicines10030019
Chicago/Turabian StyleGaravelas, Athanasios, Panagiotis Mallis, Efstathios Michalopoulos, and Eros Nikitos. 2023. "Clinical Benefit of Autologous Platelet-Rich Plasma Infusion in Ovarian Function Rejuvenation: Evidence from a Before-After Prospective Pilot Study" Medicines 10, no. 3: 19. https://doi.org/10.3390/medicines10030019