
The Use of Zirconia for Implant-Supported Fixed Complete Dental Prostheses: A Narrative Review
 , , ,
, , , 
Abstract
:1. Introduction
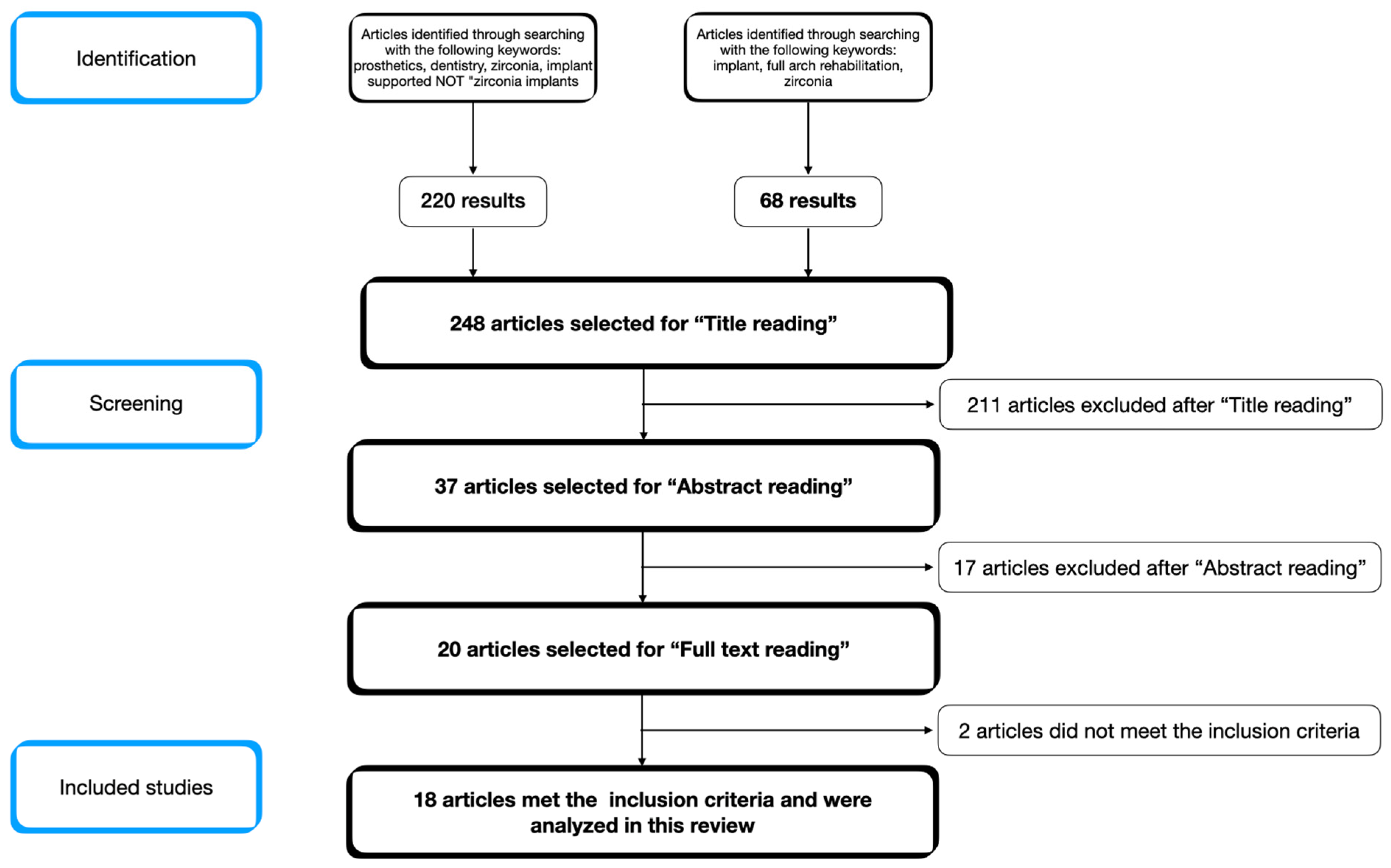
2. Materials and Methods
- -
- Human clinical studies (prospective studies, retrospective studies, randomized clinical trials, and case series);
- -
- Articles evaluating the clinical outcomes of zirconia-based implant-supported full-arch rehabilitations or comparing zirconia to other restorative materials;
- -
- Articles published in English.
- -
- Exclusion criteria:
- -
- Animal studies;
- -
- Case reports;
- -
- Articles published in languages other than English.
3. Results
4. Discussion
- -
- Monolithic form, where no additional ceramic is added and esthetics are provided by the zirconia itself and glazes applied by the technician;
- -
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barootchi, S.; Askar, H.; Ravidà, A.; Gargallo-Albiol, J.; Travan, S.; Wang, H.-L. Long-term Clinical Outcomes and Cost-Effectiveness of Full-Arch Implant-Supported Zirconia-Based and Metal-Acrylic Fixed Dental Prostheses: A Retrospective Analysis. Int. J. Oral Maxillofac. Implant. 2020, 35, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Douglass, C.W.; Shih, A.; Ostry, L. Will there be a need for complete dentures in the United States in 2020? J. Prosthet. Dent. 2002, 87, 5–8. [Google Scholar] [CrossRef]
- Carlsson, G.E. Facts and Fallacies: An Evidence Base for Complete Dentures. Dent. Update 2006, 33, 134–142. [Google Scholar] [CrossRef]
- Stellingsma, C.; Vissink, A.; Meijer, H.; Kuiper, C.; Raghoebar, G. Implantology and the severely Resorbed Edentulous Mandible. Crit. Rev. Oral Biol. Med. 2004, 15, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Hjalmarsson, L.; Gheisarifar, M.; Jemt, T. A systematic review of survival of single implants as presented in longitudinal studies with a follow-up of at least 10 years. Eur. J. Oral Implantol. 2016, 9 (Suppl. S1), S155–S162. [Google Scholar]
- Fueki, K.; Kimoto, K.; Ogawa, T.; Garrett, N.R. Effect of implant-supported or retained dentures on masticatory performance: A systematic review. J. Prosthet. Dent. 2007, 98, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, G.E.; Lindquist, L.W. Ten-year longitudinal study of masticatory function in edentulous patients treated with fixed complete dentures on osseointegrated implants. Int. J. Prosthodont. 1994, 7, 448–453. [Google Scholar]
- Zarb, G.A.; Schmitt, A. The edentulous predicament. I: A prospective study of the effectiveness of implant-supported fixed prostheses. J. Am. Dent. Assoc. 1996, 127, 59–65. [Google Scholar] [CrossRef]
- Ravidà, A.; Barootchi, S.; Tattan, M.; Saleh, M.H.A.; Gargallo-Albiol, J.; Wang, H. Clinical outcomes and cost effectiveness of computer-guided versus conventional implant-retained hybrid prostheses: A long-term retrospective analysis of treatment protocols. J. Periodontol. 2018, 89, 1015–1024. [Google Scholar] [CrossRef]
- Fischer, K.; Stenberg, T. Prospective 10-Year Cohort Study Based on a Randomized, Controlled Trial (RCT) on Implant-Supported Full-Arch Maxillary Prostheses. Part II: Prosthetic Outcomes and Maintenance. Clin. Implant. Dent. Relat. Res. 2013, 15, 498–508. [Google Scholar] [CrossRef]
- Ozkurt, Z.; Kazazoğlu, E. Clinical Success of Zirconia in Dental Applications. J. Prosthodont. 2010, 19, 64–68. [Google Scholar] [CrossRef]
- Limmer, B.; Sanders, A.E.; Reside, G.; Cooper, L.F. Complications and Patient-Centered Outcomes with an Implant-Supported Monolithic Zirconia Fixed Dental Prosthesis: 1 Year Results. J. Prosthodont. 2014, 23, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Morton, D.; Gallucci, G.; Lin, W.; Pjetursson, B.; Polido, W.; Roehling, S.; Sailer, I.; Aghaloo, T.; Albera, H.; Bohner, L.; et al. Group 2 ITI Consensus Report: Prosthodontics and implant dentistry. Clin. Oral Implant. Res. 2018, 29, 215–223. [Google Scholar] [CrossRef]
- Sadowsky, S.J. Has zirconia made a material difference in implant prosthodontics? A review. Dent. Mater. 2020, 36, 1–8. [Google Scholar] [CrossRef]
- Larsson, C.; Vult von Steyern, P.; Nilner, K. A prospective study of implant-supported full-arch yttria-stabilized tetragonal zirconia polycrystal mandibular fixed dental prostheses: Three-year results. Int. J. Prosthodont. 2010, 23, 364–369. [Google Scholar]
- Oliva, J.; Oliva, X.; Oliva, J.D. All-on-three delayed implant loading concept for the completely edentulous maxilla and mandible: A retrospective 5-year follow-up study. Int. J. Oral Maxillofac. Implant. 2012, 27, 1584–1592. [Google Scholar]
- Papaspyridakos, P.; Lal, K. Computer-assisted design/computer-assisted manufacturing zirconia implant fixed complete prostheses: Clinical results and technical complications up to 4 years of function. Clin. Oral Implant. Res. 2013, 24, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Pozzi, A.; Holst, S.; Fabbri, G.; Tallarico, M. Clinical Reliability of CAD/CAM Cross-Arch Zirconia Bridges on Immediately Loaded Implants Placed with Computer-Assisted/Template-Guided Surgery: A Retrospective Study with a Follow-Up between 3 and 5 Years. Clin. Implant. Dent. Relat. Res. 2015, 17, e86–e96. [Google Scholar] [CrossRef]
- Worni, A.; Kolgeci, L.; Rentsch-Kollàr, A.; Katsoulis, J.; Mericske-Stern, R. Zirconia-Based Screw-Retained Prostheses Supported by Implants: A Retrospective Study on Technical Complications and Failures. Clin. Implant. Dent. Relat. Res. 2015, 17, 1073–1081. [Google Scholar] [CrossRef]
- Venezia, P.; Torsello, F.; Cavalcanti, R.; D’Amato, S. Retrospective analysis of 26 complete-arch implant-supported monolithic zirconia prostheses with feldspathic porcelain veneering limited to the facial surface. J. Prosthet. Dent. 2015, 114, 506–512. [Google Scholar] [CrossRef]
- Tartaglia, G.M.; Maiorana, C.; Gallo, M.; Codari, M.; Sforza, C. Implant-Supported Immediately Loaded Full-Arch Rehabilitations. Implant. Dent. 2016, 25, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Rojas Vizcaya, F. Retrospective 2- to 7-Year Follow-Up Study of 20 Double Full-Arch Implant-Supported Monolithic Zirconia Fixed Prostheses: Measurements and Recommendations for Optimal Design. J. Prosthodont. 2018, 27, 501–508. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; Kang, K.; DeFuria, C.; Amin, S.; Kudara, Y.; Weber, H.-P. Digital workflow in full-arch implant rehabilitation with segmented minimally veneered monolithic zirconia fixed dental prostheses: 2-year clinical follow-up. J. Esthet. Restor. Dent. 2018, 30, 5–13. [Google Scholar] [CrossRef]
- Gonzalez, J.; Triplett, R. Complications and Clinical Considerations of the Implant-Retained Zirconia Complete-Arch Prosthesis with Various Opposing Dentitions. Int. J. Oral Maxillofac. Implant. 2017, 32, 864–869. [Google Scholar] [CrossRef]
- Box, V.H.; Sukotjo, C.; Knoernschild, K.L.; Campbell, S.D.; Afshari, F.S. Patient-Reported and Clinical Outcomes of Implant-Supported Fixed Complete Dental Prostheses: A Comparison of Metal-Acrylic, Milled Zirconia, and Retrievable Crown Prostheses. J. Oral Implantol. 2018, 44, 51–61. [Google Scholar] [CrossRef]
- Caramês, J.; Marques, D.; Barbosa, J.M.; Moreira, A.; Crispim, P.; Chen, A. Full-arch implant-supported rehabilitations: A prospective study comparing porcelain-veneered zirconia frameworks to monolithic zirconia. Clin. Oral Implant. Res. 2019, 30, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Diéguez-Pereira, M.; Chávarri-Prado, D.; Estrada-Martínez, A.; Pérez-Pevida, E.; Brizuela-Velasco, A. Monolithic and Minimally Veneered Zirconia Complications as Implant-Supported Restorative Material: A Retrospective Clinical Study up to 5 Years. Biomed. Res. Int. 2020, 2020, 8821068. [Google Scholar] [CrossRef]
- Pozzi, A.; Arcuri, L.; Fabbri, G.; Singer, G.; Londono, J. Long-term survival and success of zirconia screw-retained implant-supported prostheses for up to 12 years: A retrospective multicenter study. J. Prosthet. Dent. 2021, 129, 96–108. [Google Scholar] [CrossRef]
- Tirone, F.; Salzano, S.; Rolando, E.; Pozzatti, L.; Rodi, D. Framework Fracture of Zirconia Supported Full Arch Implant Rehabilitation: A Retrospective Evaluation of Cantilever Length and Distal Cross-Sectional Connection Area in 140 Patients Over an Up-To-7 Year Follow-Up Period. J. Prosthodont. 2022, 31, 121–129. [Google Scholar] [CrossRef]
- Richerson, D.W.; Lee, W.E. Modern Ceramic Engineering; CRC Press: Boca Raton, FL, USA, 2018. [Google Scholar] [CrossRef]
- Pjetursson, B.E.; Sailer, I.; Zwahlen, M.; Hämmerle, C.H.F. A systematic review of the survival and complication rates of all-ceramic and metal-ceramic reconstructions after an observation period of at least 3 years. Part I: Single crowns. Clin. Oral Implant. Res. 2007, 18, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Papaspyridakos, P.; Chochlidakis, K.; Kang, K.; Chen, Y.; Alghfeli, A.; Kudara, Y.; Weber, H. Digital Workflow for Implant Rehabilitation with Double Full-Arch Monolithic Zirconia Prostheses. J. Prosthodont. 2020, 29, 460–465. [Google Scholar] [CrossRef]
- Monaco, C.; Caldari, M.; Scotti, R. Clinical Evaluation of Zirconia-Based Restorations on Implants: A Retrospective Cohort Study from the AIOP Clinical Research Group. Int. J. Prosthodont. 2016, 28, 239–242. [Google Scholar] [CrossRef] [PubMed]
- Kolgeci, L.; Mericske, E.; Worni, A.; Walker, P.; Katsoulis, J.; Mericske-Stern, R. Technical Complications and Failures of Zirconia-Based Prostheses Supported by Implants Followed Up to 7 Years: A Case Series. Int. J. Prosthodont. 2014, 27, 544–552. [Google Scholar] [CrossRef] [PubMed]
- Spitznagel, F.A.; Balmer, M.; Wiedemeier, D.B.; Jung, R.E.; Gierthmuehlen, P.C. Clinical outcomes of all-ceramic single crowns and fixed dental prostheses supported by ceramic implants: A systematic review and meta-analyses. Clin. Oral Implant. Res. 2022, 33, 1–20. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference | Type of Study | Number of Patients | Number and Type of ISFCDPs | Experimental Groups/Type of Restorative Material Used | Follow-Up | Prosthetic Survival Rate | Prosthetic Success Rate | Prosthetic Complications |
|---|---|---|---|---|---|---|---|---|
| Larsson C. et al. (2010) [15] | Prospective Clinical Study | 10 patients | 10 mandibular arches | Yttria-stabilized tetragonal zirconia polycrystal (Y-TZP) ISFCDPs (Cercon technique) | 3 years | 100% | 66% | Superficial chipping (90%); marginal integrity was considered excellent in 70% of the cases and acceptable in 30%. No prosthesis was lost, fractured, or required laboratory repair. |
| Oliva J. et al. (2012) [16] | Retrospective Clinical Study | 17 patients | 24 arches | Full zirconia framework + ceramic on the buccal aspect | 5 years | 100% | 100% | Buccal ceramic chipping (4.1%) Screw loosening (4.1%) |
| Papaspyridakos P. and Lal K. (2013) [17] | Retrospective Clinical Study | 14 patients | 16 arches (10 in mandible, 6 in maxilla) | Porcelain fused to zirconia (PFZ) | 2–4 years | 100% | Not specified | Ceramic chipping (31.25%) |
| Pozzi et al. (2015) [18] | Retrospective Clinical Study | 22 patients | 26 arches (14 in mandible, 12 in maxilla) | Full Zirconia framework + ceramic veneering | >3 years (36 to 60 months) | 100% | 89% | Ceramic chipping (11%) |
| Limmer B. et al. (2014) [12] | Prospective Clinical Study | 17 patients | 17 mandibular arches | Monolithic zirconia fixed dental prosthesis (MZ-FDP) | 1 year | 88% | Not specified | Prosthetic complications (58.8%), including tooth chipping of the opposing removable denture, abutment loosening, fracture of the abutments, and debonding of the prosthetic components. One prosthesis was lost due to fracture and one due to implant failure (12%). |
| Worni A. et al. (2015) [19] | Retrospective Clinical Study | 90 patients | 156 screw-retained zirconia prosthesis (11 maxillary full-arches) | Full Zirconia framework + ceramic veneering | 2–7 years | 91% | Not specified | Extensive ceramic chipping in one maxillary arch (9%). No framework fracture was observed. |
| Venezia P. at al. (2015) [20] | Retrospective Clinical Study | 18 patients | 26 arches (17 in maxilla and 9 in mandible) | Full zirconia framework + ceramic on the buccal aspect | 10 to 36 months (mean = 20.9 months/1.6 years) | 100% | Not specified | Minor ceramic chipping (11.5%) |
| Tartaglia G.M. et al. (2016) [21] | Retrospective Clinical Study | 113 patients | 214 arches (105 maxillary, 109 mandibular) | Group 1: polymethyl methacrylate (PMMA framework) veneered with resin (166 prostheses on 96 patients) Group 2: Full Zirconia framework + ceramic veneering (48 prostheses on 32 patients) | 5 years | 88.9% | 60.5% | 37 out of 113 patients (32.7%) had prosthetic complications (reparable fractures, abutment-prosthesis screws loosening, ceramic chipping for zirconia prostheses); the prosthetic material did not influence the risk of developing complications. |
| Rojas Vizcaya F. et al. (2018) [22] | Retrospective Clinical Study | 10 patients | 20 arches | Monolithic full arch zirconia prostheses10 with partial cutback10 without cutback | 2–7 years | 100% implant and prosthetic | 100% | one prosthetic complication was reported for each group: gingival pink ceramic chipping in the non-cutback group and screw loosening in the cutback group. |
| Papaspyridakos P. et al. (2018) [23] | Prospective Clinical Study | 3 patients | 5 arches | Monolithic zirconia with mild facial porcelain veneering, not full arch but multiple FDPS | 2 years | Implant and prosthetic 100% | 100% | 1 porcelain chipping |
| Gonzales J. and Triplett R. (2017) [24] | Retrospective Clinical Study | 40 patients | 56 arches 44 zirconia and 12 hybrid prostheses (metal-acrylic) | Maxillary ZIRCAP and mandibular ZIRCAP (4 patients, 8 prostheses)Maxillary ZIRCAP and mandibular natural dentition (24 patients) Maxillary ZIRCAP and mandibular conventional hybrid prosthesis (metal-acrylic) (12 patients) | Mean of 2.75 years (33 months) | 100% (extrapolated) | 100% (extrapolated) | MZIRCAP vs. MZIRCAP 1 minor porcelain chipping and 1 debonded metal insert MZIRCAP vs. NATDENT 6/24 complications, 5 minor porcelain chippings and 1 debonded metal insert MZIRCAP vs. metal-acrylic no complications, but complications on metal acrylic: 16 tooth fractures among 12 prostheses. ZIRCAP 6 minor porcelain fractures and 2 debonded inserts, metal acrylic 16 tooth fractures. |
| Box V. et al. (2018) [25] | retrospective | 37 patients | 49 arches | 22 metal acrylic 14 retrievable crown 7 monolithic zirconia 6 porcelain veneered zirconia | Between 1 and 5.8 years (12 to 70 months) | Not specified | Not specified | 12/22 for metal acrylic, 10/14 for retrievable crown, 2/7 monolithic zirconia, 5/6 porcelain veneered zirconia Fractured teeth highest in retrievable crown (6/14) then metal-acrylic (4) then PVZ (3). The most common complications were: (1) MA: posterior tooth wear, highest in metal acrylic (10), then retrievable crown (3), then PVZ (2), then monolithic zirconia (1) (2) RC: chipping and fracturing of the restorations, debonding of crowns (4) (3) MZ: wear of opposing restorations, and (4) PVZ: chipping of opposing restorations. |
| Caramês J. et al. (2019) [26] | Prospective Clinical Study | 150 patients | 193 arches | 83 ceramic-veneered zirconia full arches (PVZ) 110 buccal-veneered (nonfunctional) monolithic zirconia full arches (MZ) | 608.80 ± 172.52 days for PVZ (1.66 ± 0.47 yrs) 552.63 ± 197.57 days for MZ (1.51 ± 0.5 days) | Over 99% for both groups. | Not specified | PVZ group: 10 MZ group: 10 Total complication rate: 11.3%. Most common: -loss of access chamber composite plug -screw loosening 85% of the complications occurred when the opposing arch consisted also of a full-arch implant-supported rehabilitation. |
| Barootchi S. et al. (2020) [1] | Retrospective Clinical Study | 56 patients | 74 full arches | 43 metal-acrylic 31 zirconia | Min 5 years (mean 8.7 ± 3.37) | AT 5 YEARS: Zirconia: 93.7 ± 5.5% Metal acrylic: 83.0 ± 11.1% AT 8 YEARS Zirconia: 88 ± 8.8% Metal acrylic: 67.6 ± 14.8% | Metal acrylic: 94 single tooth fracture/dislodgement in 22 prostheses. Zirconia: single tooth chipping fracture (36 times in 9 prostheses). Minor complications 67.6%, major complications 35.1%. Major complications: multiple teeth fracture requiring lab work (40 times in 17 metal-acrylic prostheses, 17 times in 4 zirconia fixed prostheses) More minor complications in metal-acrylic than zirconia (72.1% vs. 61.3% P = 0.329) mean of 3.4 vs. 1.7 minor complications PER CASE. Major complications more common in metal-acrylic prostheses than in zirconia ones (41.9% vs. 25.8%) No statistical significance after adjusting for the different follow-up times. | |
| Capparè P. et al. (2021) [27] | Retrospective Clinical Study | 50 patients | 50 arches (22 maxillary, 28 mandibular) | 25 Monolithic zirconia with ceramic veneering limited to non-functional areas. 25 metal-acrylic | Minimum 2 years (average not specified) | 100% | 100% | No complications reported |
| Diéguez-Pereira et al. (2020) [28] | Retrospective Clinical Study | 48 patients (it is not specified how many have full arch rehabilitations) | 58 arches (14 monolithic 44 partially veneered) 154 restorations were included in the study. (82 monolithic and 72 with buccal ceramic stratification) N.B.: crowns, bridges, and full-arch rehabilitations were included | Divides groups in follow up time instead of prosthetic restoration type. | Up to 5 years (average not specified) | Not specified (we assume 100%) | Not specified (we assume 100%) | 1 case of chipping |
| Pozzi A. et al. (2021) [29] | Retrospective Clinical Study | 98 patients | 111 arches (96 zirconia connection, 15 titanium base) All frameworks were cutback and veneered. | 24 complete ISZFDPs with a zirconia connection (12.9 ± 0.97 dental units, minimum 12, maximum 14), 72 partial prostheses with a zirconia connection (3.11 ± 1.12, minimum 2, maximum 7), 15 partial prostheses with a titanium base (3.62 ± 1.02, minimum 2, maximum 5). | Forty ISZFDPs had been in function for more than 10 years (36%), 38 for 5 to 9 years (34.2%), and 33 for 2 to 4 years (22.8%). The mean follow-up time was 7.2 ± 3.4 years. | 98.2% | 91.9% | No zirconia fractures 2 implants and 2 ISFCDPs failed due to chipping (13.5%) The 4 different types of veneering porcelains experienced the following chipping rates: ZI-CT Creation Willi Geller (0 out of 6; 0%), CZR (6 out of 77; 7.8%), IPS e.max Ceram (7 out of 26; 26.9%), and NobelRondo (2 out of 2; 100%). None of the ISZFDPs had to be remade because of esthetic reasons |
| Tirone F. et al. (2021) [30] | Retrospective Clinical Study | 140 patients | 180 arches in monolithic zirconia | Group 1: completely veneered zirconia IFCDP (21 ISFCDP) Group 2: zirconia IFCDP with veneering only on the buccal surface of all teeth (71 ISFCDP) Group 3: monolithic zirconia IFCDP veneered in the gingival portion only (41 ISFCDP) | Min. 12 months, max 87 months MEAN: 41.6 ± 21.2 months | Not specified | 93.3% | 2 prosthetic failures due to implant failures 8 framework fractures (5 type I, all maxillary, and 5 type II, all mandibular) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cinquini, C.; Alfonsi, F.; Marchio, V.; Gallo, F.; Zingari, F.; Bolzoni, A.R.; Romeggio, S.; Barone, A. The Use of Zirconia for Implant-Supported Fixed Complete Dental Prostheses: A Narrative Review. Dent. J. 2023, 11, 144. https://doi.org/10.3390/dj11060144
Cinquini C, Alfonsi F, Marchio V, Gallo F, Zingari F, Bolzoni AR, Romeggio S, Barone A. The Use of Zirconia for Implant-Supported Fixed Complete Dental Prostheses: A Narrative Review. Dentistry Journal. 2023; 11(6):144. https://doi.org/10.3390/dj11060144
Chicago/Turabian StyleCinquini, Chiara, Fortunato Alfonsi, Vincenzo Marchio, Francesco Gallo, Francesco Zingari, Alessandro Remigio Bolzoni, Stefano Romeggio, and Antonio Barone. 2023. "The Use of Zirconia for Implant-Supported Fixed Complete Dental Prostheses: A Narrative Review" Dentistry Journal 11, no. 6: 144. https://doi.org/10.3390/dj11060144