

A Combination of Platelet-Rich Fibrin and Collagen Membranes for Sinus Membrane Repair: A Case Report (Repair of Sinus Membrane Perforation)
 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
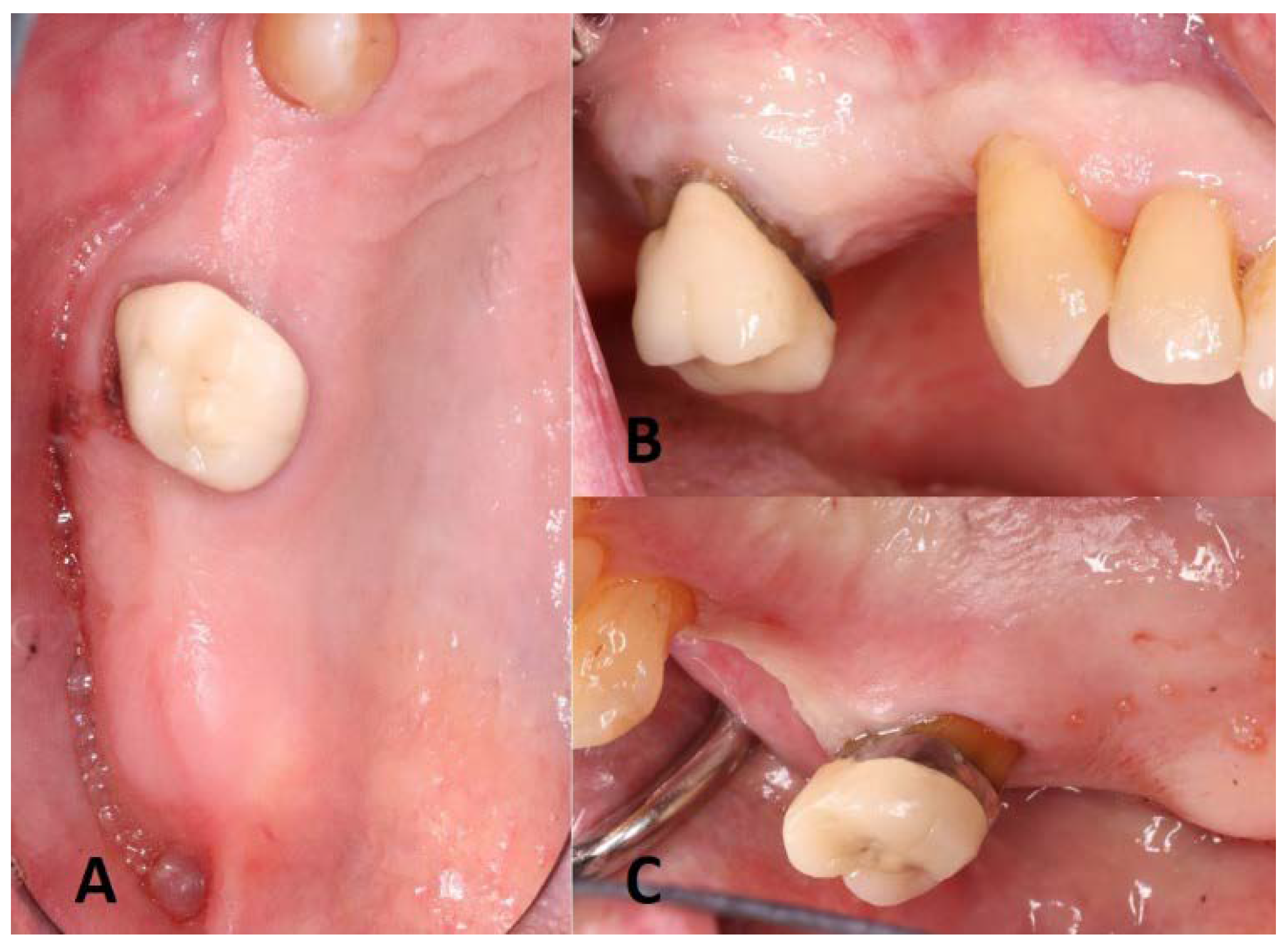
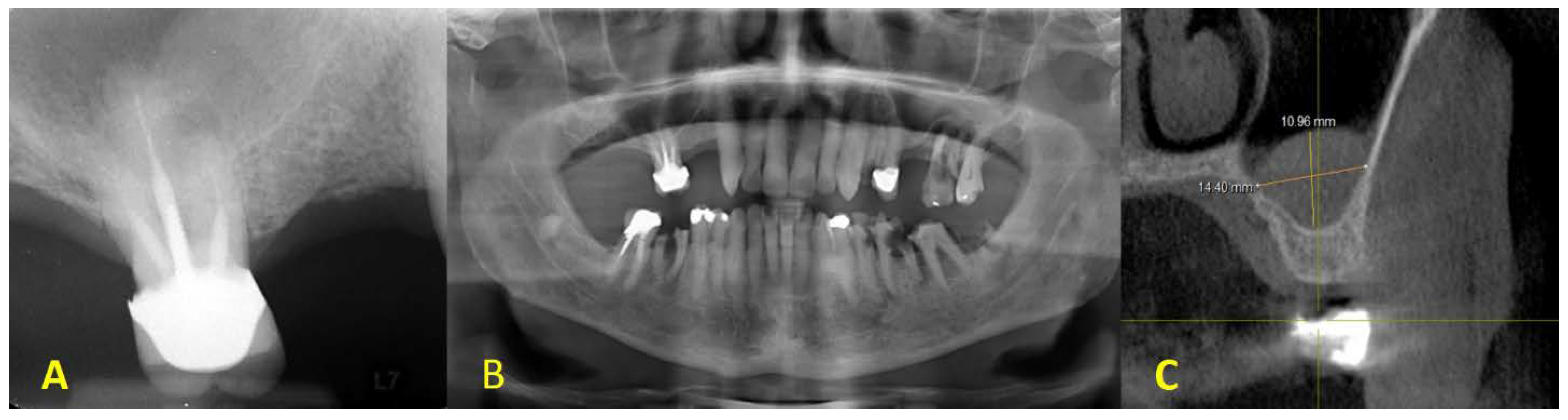
2. Clinical Presentation
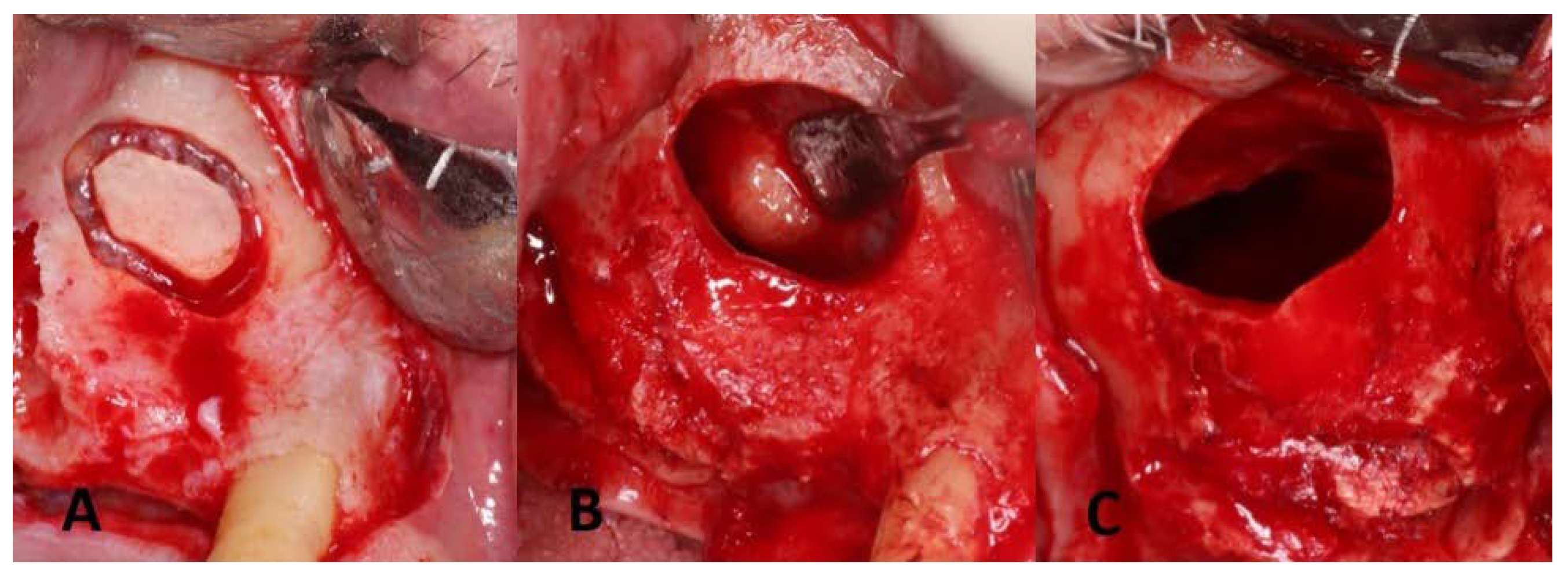
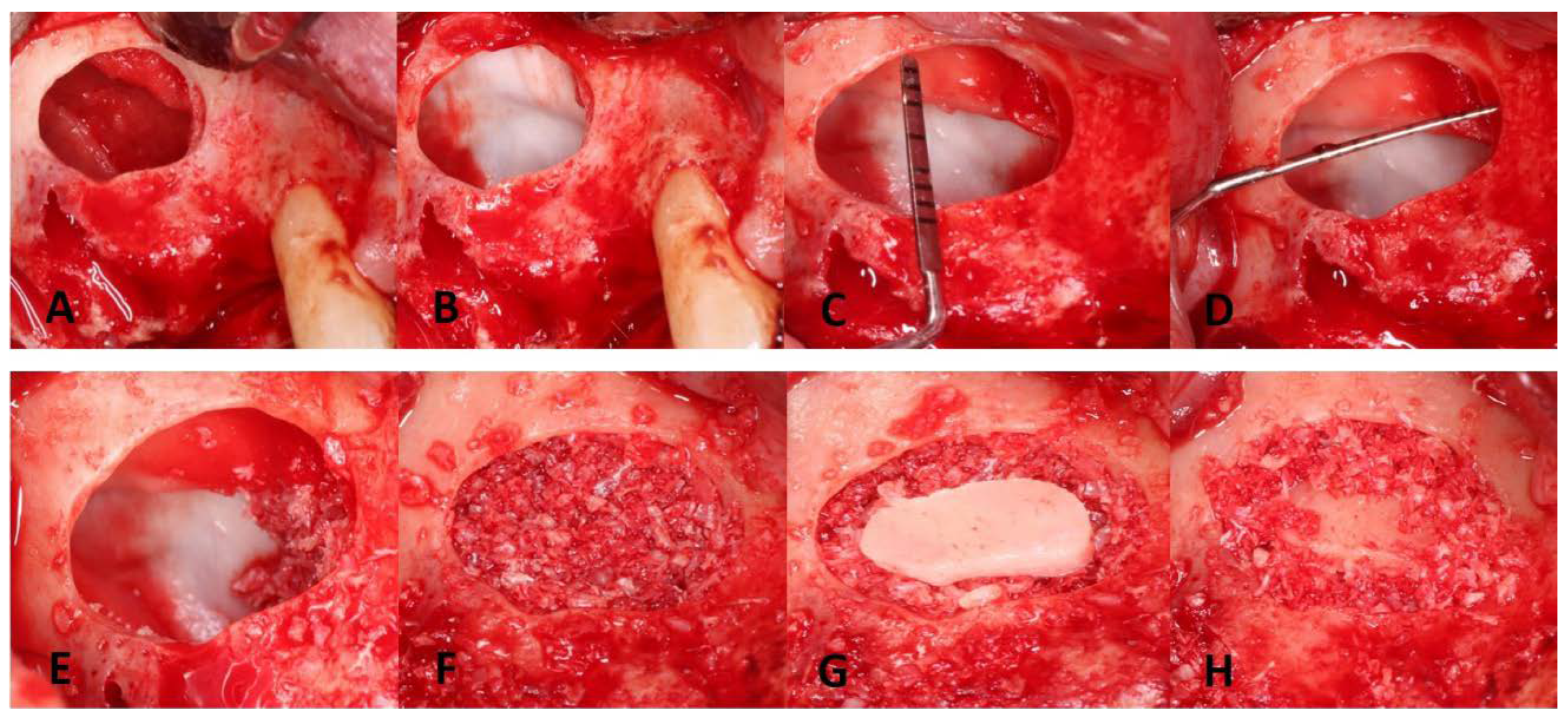
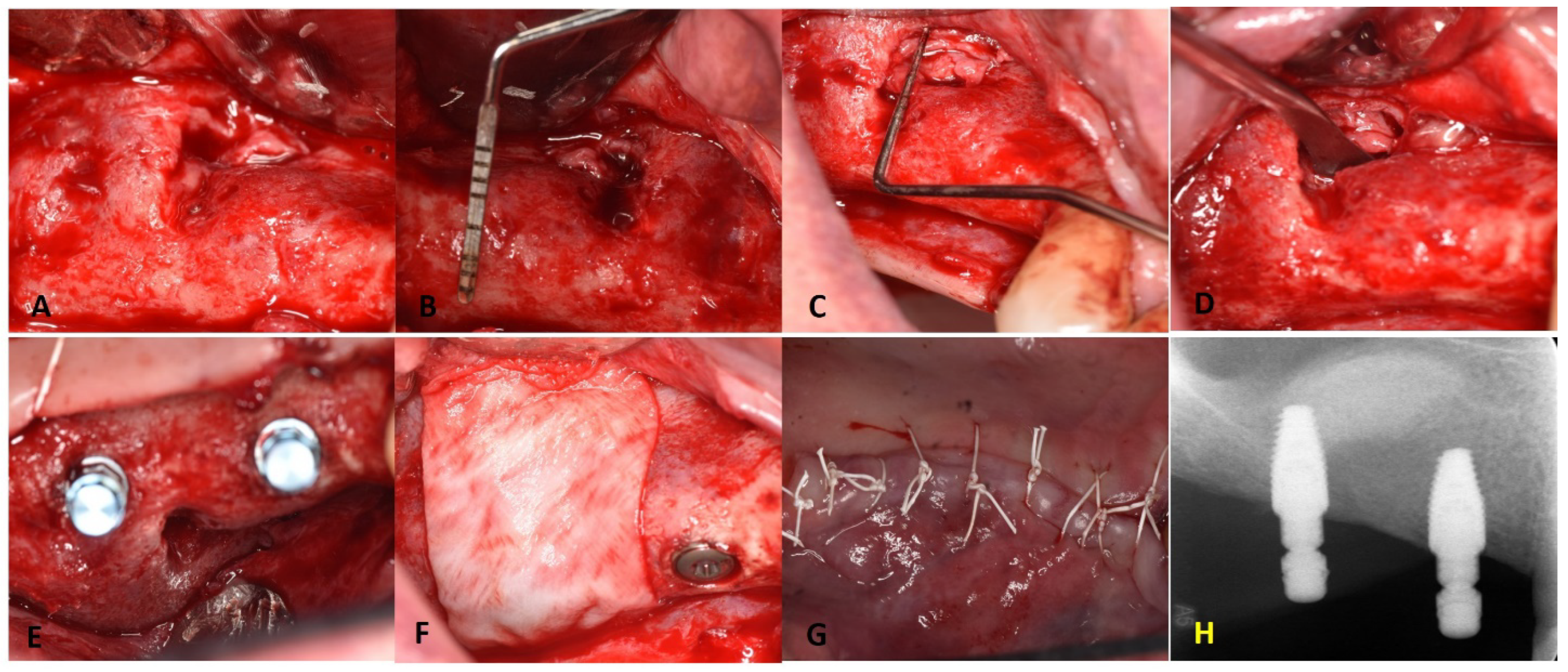
3. Surgical Procedures

4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pjetursson, B.E.; Thoma, D.; Jung, R.; Zwahlen, M.; Zembic, A. A systematic review of the survival and complication rates of implant-supported fixed dental prostheses (FDPs) after a mean observation period of at least 5 years. Clin. Oral. Implant. Res. 2012, 23 (Suppl. 6), 22–38. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E. Contemporary implant dentistry. Implant Dent. 1999, 8, 90. [Google Scholar] [CrossRef]
- Levi, I.; Halperin-Sternfeld, M.; Horwitz, J.; Zigdon-Giladi, H.; Machtei, E.E. Dimensional changes of the maxillary sinus following tooth extraction in the posterior maxilla with and without socket preservation. Clin. Implant Dent. Relat. Res. 2017, 19, 952–958. [Google Scholar] [CrossRef] [PubMed]
- Ha, J.; Son, J.H.; Sung, I.Y.; Cho, Y.C.; Choi, J.H. Clinical outcome of implants placed in grafted maxillary sinus via lateral approach: A 10-year follow-up study. J. Dent. Sci. 2020, 15, 270–277. [Google Scholar] [CrossRef]
- Gökhan, G.; Yasar, Ö. Maxillary Sinus Augmentation for Dental Implants. In Paranasal Sinuses; Balwant Singh, G., Ed.; IntechOpen: Rijeka, Croatia, 2017; p. Ch. 2. [Google Scholar]
- Wallace, S.S.; Froum, S.J. Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review. Ann. Periodontol. 2003, 8, 328–343. [Google Scholar] [CrossRef] [Green Version]
- Cheon, K.-J.; Yang, B.-E.; Cho, S.-W.; Chung, S.-M.; Byun, S.-H. Lateral Window Design for Maxillary Sinus Graft Based on the Implant Position. Int. J. Environ. Res. Public Health 2020, 17, 6335. [Google Scholar] [CrossRef]
- Silva, L.D.; de Lima, V.N.; Faverani, L.P.; de Mendonça, M.R.; Okamoto, R.; Pellizzer, E.P. Maxillary sinus lift surgery-with or without graft material? A systematic review. Int. J. Oral Maxillofac. Surg. 2016, 45, 1570–1576. [Google Scholar] [CrossRef] [Green Version]
- Geurs, N.C.; Wang, I.-C.; Shulman, L.B.; Jeffcoat, M.K. Retrospective radiographic analysis of sinus graft and implant placement procedures from the Academy of Osseointegration Consensus Conference on Sinus Grafts. Int. J. Periodontics Restor. Dent. 2001, 21, 517–523. [Google Scholar]
- Ellegaard, B.; Baelum, V.; Kølsen-Petersen, J. Non-grafted sinus implants in periodontally compromised patients: A time-to-event analysis. Clin. Oral Implant. Res. 2006, 17, 156–164. [Google Scholar] [CrossRef]
- Kim, Y.K.; Ku, J.K. Sinus membrane elevation and implant placement. J. Korean Assoc. Oral Maxillofac. Surg. 2020, 46, 292–298. [Google Scholar] [CrossRef]
- Wallace, S.S.; Mazor, Z.; Froum, S.J.; Cho, S.C.; Tarnow, D.P. Schneiderian membrane perforation rate during sinus elevation using piezosurgery: Clinical results of 100 consecutive cases. Int. J. Periodontics Restor. Dent. 2007, 27, 413–419. [Google Scholar]
- Raghoebar, G.M.; Batenburg, R.H.; Timmenga, N.M.; Vissink, A.; Reintsema, H. Morbidity and complications of bone grafting of the floor of the maxillary sinus for the placement of endosseous implants. Mund Kiefer Gesichtschir. 1999, 3 (Suppl. S1), S65–S69. [Google Scholar] [CrossRef] [PubMed]
- Jordi, C.; Mukaddam, K.; Lambrecht, J.T.; Kühl, S. Membrane perforation rate in lateral maxillary sinus floor augmentation using conventional rotating instruments and piezoelectric device-a meta-analysis. Int. J. Implant Dent. 2018, 29, 3. [Google Scholar] [CrossRef] [Green Version]
- Tükel, H.C.; Tatli, U. Risk factors and clinical outcomes of sinus membrane perforation during lateral window sinus lifting: Analysis of 120 patients. Int. J. Oral Maxillofac. Surg. 2018, 47, 1189–1194. [Google Scholar] [CrossRef] [PubMed]
- Molina, A.; Sanz-Sánchez, I.; Sanz-Martín, I.; Ortiz-Vigón, A.; Sanz, M. Complications in sinus lifting procedures: Classification and management. Periodontology 2000 2022, 88, 103–115. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Olivares, L.A.; Cortés-Bretón Brinkmann, J.; Martínez-Rodríguez, N.; Martínez-González, J.M.; López-Quiles, J.; Leco-Berrocal, I.; Meniz-García, C. Management of Schneiderian membrane perforations during maxillary sinus floor augmentation with lateral approach in relation to subsequent implant survival rates: A systematic review and meta-analysis. Int. J. Implant Dent. 2021, 7, 91. [Google Scholar] [CrossRef] [PubMed]
- Veith, A.P.; Henderson, K.; Spencer, A.; Sligar, A.D.; Baker, A.B. Therapeutic strategies for enhancing angiogenesis in wound healing. Adv. Drug. Deliv. Rev. 2019, 146, 97–125. [Google Scholar] [CrossRef]
- Öncü, E.; Kaymaz, E. Assessment of the effectiveness of platelet rich fibrin in the treatment of Schneiderian membrane perforation. Clin. Implant Dent. Relat. Res. 2017, 19, 1009–1014. [Google Scholar] [CrossRef]
- Damsaz, M.; Castagnoli, C.Z.; Eshghpour, M.; Alamdari, D.H.; Alamdari, A.H.; Noujeim, Z.E.F.; Haidar, Z.S. Evidence-Based Clinical Efficacy of Leukocyte and Platelet-Rich Fibrin in Maxillary Sinus Floor Lift, Graft and Surgical Augmentation Procedures. Front. Surg. 2020, 7, 537138. [Google Scholar] [CrossRef]
- Pavlovic, V.; Ciric, M.; Jovanovic, V.; Trandafilovic, M.; Stojanovic, P. Platelet-rich fibrin: Basics of biological actions and protocol modifications. Open Med. 2021, 16, 446–454. [Google Scholar] [CrossRef]
- Miron, R.J.; Zucchelli, G.; Pikos, M.A.; Salama, M.; Lee, S.; Guillemette, V.; Fujioka-Kobayashi, M.; Bishara, M.; Zhang, Y.; Wang, H.-L.; et al. Use of platelet-rich fibrin in regenerative dentistry: A systematic review. Clin. Oral Investig. 2017, 21, 1913–1927. [Google Scholar] [CrossRef] [PubMed]
- Testori, T.; Weinstein, T.; Taschieri, S.; Wallace, S.S. Risk factors in lateral window sinus elevation surgery. Periodontol. 2000 2019, 81, 91–123. [Google Scholar] [CrossRef] [PubMed]
- Okada, T.; Kawana, H. Two-Step Procedure for the Treatment of a Maxillary Sinus with Complex Sinus Septa: A Highly Predictive Method for Sinus Floor Augmentation After Perforation of the Maxillary Sinus Membrane. Int. J. Periodontics Restor. Dent. 2019, 39, e175–e180. [Google Scholar] [CrossRef] [PubMed]
- Dagba, A.; Mourlaas, J.; Ochoa Durand, D.; Suzuki, T.; Cho, S.; Froum, S. A novel approach to treat large Schneiderian membrane perforation-a case series. Int. J. Dent. Oral Health 2015, 6, 137. [Google Scholar]
- Anitua, E.; Alkhraisat, M.H.; Torre, A.; Eguia, A. Are mucous retention cysts and pseudocysts in the maxillary sinus a risk factor for dental implants? A systematic review. Med. Oral Patol. Oral Cir. Bucal. 2021, 26, e276–e283. [Google Scholar] [CrossRef] [PubMed]
- Baykul, T.; Fındık, Y. Maxillary sinus perforation with presence of an antral pseudocyst, repaired with platelet rich fibrin. Ann. Maxillofac. Surg. 2014, 4, 205–207. [Google Scholar] [PubMed] [Green Version]
- Weiss, R., II.; Read-Fuller, A. Cone Beam Computed Tomography in Oral and Maxillofacial Surgery: An Evidence-Based Review. Dent. J. 2019, 7, 52. [Google Scholar] [CrossRef] [Green Version]
- Mardinger, O.; Manor, I.; Mijiritsky, E.; Hirshberg, A. Maxillary sinus augmentation in the presence of antral pseudocyst: A clinical approach. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, 180–184. [Google Scholar] [CrossRef]
- Esposito, M.; Grusovin, M.G.; Worthington, H.V. Interventions for replacing missing teeth: Antibiotics at dental implant placement to prevent complications. Cochrane Database Syst. Rev. 2013, 2013, Cd004152. [Google Scholar] [CrossRef]
- Shirbhate, U.; Bajaj, P. Third-Generation Platelet Concentrates in Periodontal Regeneration: Gaining Ground in the Field of Regeneration. Cureus 2022, 14, e28072. [Google Scholar] [CrossRef]
- Wagenberg, B.; Froum, S.J. A retrospective study of 1925 consecutively placed immediate implants from 1988 to 2004. Int. J. Oral Maxillofac. Implant. 2006, 21, 71–80. [Google Scholar]
- Pjetursson, B.E.; Tan, W.C.; Zwahlen, M.; Lang, N.P. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. J. Clin. Periodontol. 2008, 35, 216–240. [Google Scholar] [CrossRef]
- Hernández-Alfaro, F.; Torradeflot, M.M.; Marti, C. Prevalence and management of Schneiderian membrane perforations during sinus-lift procedures. Clin. Oral Implant. Res. 2008, 19, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Khoury, F. Augmentation of the sinus floor with mandibular bone block and simultaneous implantation: A 6-year clinical investigation. Int. J. Oral Maxillofac. Implant. 1999, 14, 557–564. [Google Scholar]
- Nolan, P.J.; Freeman, K.; Kraut, R.A. Correlation between Schneiderian membrane perforation and sinus lift graft outcome: A retrospective evaluation of 359 augmented sinus. J. Oral Maxillofac. Surg. 2014, 72, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.L.; Wang, H.L. Sinus pathology and anatomy in relation to complications in lateral window sinus augmentation. Implant Dent. 2011, 20, 406–412. [Google Scholar] [CrossRef] [Green Version]
- Hong, S.L.; Cho, K.S.; Roh, H.J. Maxillary sinus retention cysts protruding into the inferior meatus. Clin. Exp. Otorhinolaryngol. 2014, 7, 226–228. [Google Scholar] [CrossRef]
- Yu, H.; Qiu, L. Histological and clinical outcomes of lateral sinus floor elevation with simultaneous removal of a maxillary sinus pseudocyst. Clin. Implant Dent. Relat. Res. 2019, 21, 94–100. [Google Scholar] [CrossRef] [Green Version]
- Nilesh, K.; Dadhich, A. Unusually large radicular cyst presenting in the maxillary sinus. BMJ Case Rep. 2020, 13, e236582. [Google Scholar] [CrossRef]
- Choi, B.-H.; Zhu, S.-J.; Jung, J.-H.; Lee, S.-H.; Huh, J.-Y. The use of autologous fibrin glue for closing sinus membrane perforations during sinus lifts. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2006, 101, 150–154. [Google Scholar] [CrossRef]
- Pinto, G.; Pigossi, S.C.; Pessoa, T.; Nícoli, L.G.; Araújo, R.; Marcantonio, C.; Marcantonio, E., Jr. Successful Use of Leukocyte Platelet-Rich Fibrin in the Healing of Sinus Membrane Perforation: A Case Report. Implant Dent. 2018, 27, 375–380. [Google Scholar] [CrossRef]
- Salgado-Peralvo, A.O.; Garcia-Sanchez, A.; Kewalramani, N.; Velasco-Ortega, E. Treatment of sinus membrane perforations during sinus lift surgeries using leukocyte and platelet-rich fibrin: A report of three cases. J. Clin. Transl. Res. 2022, 8, 360–368. [Google Scholar] [PubMed]
- Shaikh, M.S.; Zafar, M.S.; Pisani, F.; Lone, M.A.; Malik, Y.R. Critical features of periodontal flaps with regard to blood clot stability: A review. J. Oral Biosci. 2021, 63, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Tajima, N.; Ohba, S.; Sawase, T.; Asahina, I. Evaluation of sinus floor augmentation with simultaneous implant placement using platelet-rich fibrin as sole grafting material. Int. J. Oral Maxillofac. Implant. 2013, 28, 77–83. [Google Scholar] [CrossRef] [Green Version]
- Testori, T.; Wallace, S.S.; Del Fabbro, M.; Taschieri, S.; Trisi, P.; Capelli, M.; Weinstein, R. Repair of large sinus membrane perforations using stabilized collagen barrier membranes: Surgical techniques with histologic and radiographic evidence of success. Int. J. Periodontics Restor. Dent. 2008, 28, 9–17. [Google Scholar]
- Barbu, H.M.; Iancu, S.A.; Hancu, V.; Referendaru, D.; Nissan, J.; Naishlos, S. PRF-Solution in Large Sinus Membrane Perforation with Simultaneous Implant Placement-Micro CT and Histological Analysis. Membranes 2021, 11, 438. [Google Scholar] [CrossRef] [PubMed]
- Chattopadhyay, S.; Raines, R.T. Review collagen-based biomaterials for wound healing. Biopolymers 2014, 101, 821–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lupi, S.M.; Rodriguez, Y.B.A.; Todaro, C.; Ceccarelli, G.; Rodriguez, Y.B.R. Maxillary Sinus Lift Using Autologous Periosteal Micrografts: A New Regenerative Approach and a Case Report of a 3-Year Follow-Up. Case Rep. Dent. 2018, 2018, 3023096. [Google Scholar] [CrossRef]
- Demetter, R.S.; Calahan, B.G.; Mealey, B.L. Histologic Evaluation of Wound Healing After Ridge Preservation With Cortical, Cancellous, and Combined Cortico-Cancellous Freeze-Dried Bone Allograft: A Randomized Controlled Clinical Trial. J. Periodontol. 2017, 88, 860–868. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koleilat, A.; Mansour, A.; Alkassimi, F.M.; Aguirre, A.; Almaghrabi, B. A Combination of Platelet-Rich Fibrin and Collagen Membranes for Sinus Membrane Repair: A Case Report (Repair of Sinus Membrane Perforation). Dent. J. 2023, 11, 84. https://doi.org/10.3390/dj11030084
Koleilat A, Mansour A, Alkassimi FM, Aguirre A, Almaghrabi B. A Combination of Platelet-Rich Fibrin and Collagen Membranes for Sinus Membrane Repair: A Case Report (Repair of Sinus Membrane Perforation). Dentistry Journal. 2023; 11(3):84. https://doi.org/10.3390/dj11030084
Chicago/Turabian StyleKoleilat, Anass, Alaa Mansour, Fatma M. Alkassimi, Alfredo Aguirre, and Bandar Almaghrabi. 2023. "A Combination of Platelet-Rich Fibrin and Collagen Membranes for Sinus Membrane Repair: A Case Report (Repair of Sinus Membrane Perforation)" Dentistry Journal 11, no. 3: 84. https://doi.org/10.3390/dj11030084