

Comparison of Lasers and Desensitizing Agents in Dentinal Hypersensitivity Therapy

 ,
,
Abstract
:1. Introduction
- −
- Gingival recession, an important predisposing factor as it exposes the cervical dentine and the root
- −
- Aging
- −
- Dehiscence of soft tissue
- −
- Brushing that is too aggressive
2. Materials and Methods
Search Strategy and Selection Criteria
- Randomized clinical trials
- Controlled studies
- Double-blind controlled studies
- Studies with split-mouth protocol
- Studies with a follow-up of at least 3 months
- Studies with a minimum of seven patients of both sexes, aged between 20 and 60 years.
- Studies with Nd: YAG laser
- Studies with diode lasers
- Studies comparing the Nd: YAG laser with the diode laser
- In vitro studies
- Animal studies
3. Results
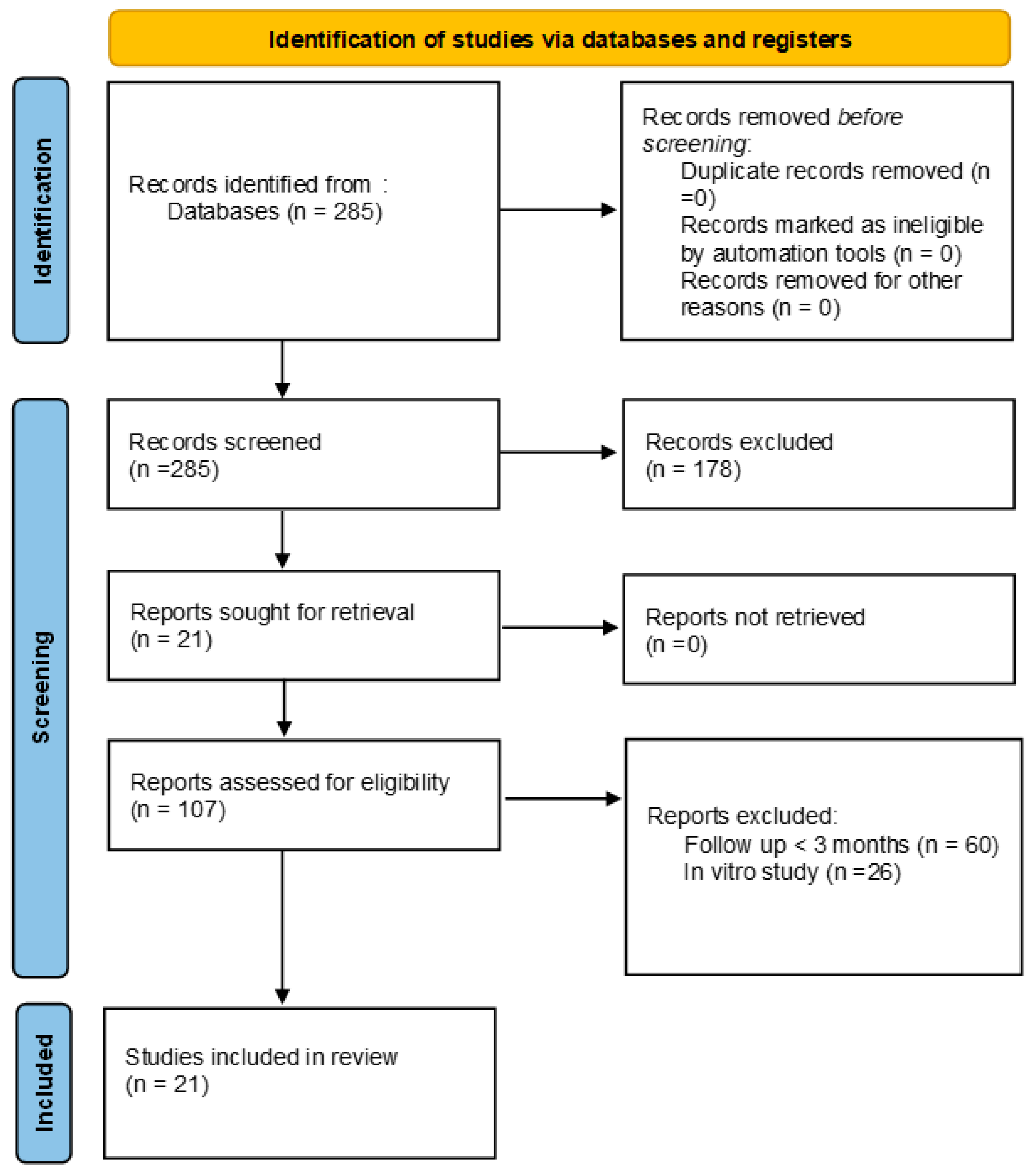
3.1. Selection of Studies
3.2. Main Results of the Studies
3.2.1. Laser Nd: YAG
- 1.5 W at 10 Hz and 100 mJ at 1064 nm for four sessions for a total of 60 s at 10 s intervals
- 1 W at 10 Hz for 60 s at 1064 nm for three sessions at 72 h intervals
3.2.2. Low-Power Diode Laser
- 1.
- Low-power low-dose diode laser:
- 810 nm, 30 mW, and 10 J/cm2 for 9 s per point, with three sessions at 72 h intervals
- 685 nm, 25 mW, and 9 Hz for 100 s for three sessions at 72 h intervals
- 2.
- Low-power, high-dose diode laser
- 810 nm, 100 mW, and 40 J/cm2 for 11 s at one point on the cervical area and one in the apical area per point for three sessions at 72 h intervals
- 810 nm, 0.5 W continuous-emission form; each tooth irradiated for 2 min in non-contact mode
3.2.3. High-Power Diode Laser
- 3 W at 30 Hz and 980 nm for 20 s using a 300 µ fibre in pulsed mode
- 980 nm DL applied at 2 W in continuous-wave mode on the surface of the tooth to be treated, using a 320 µ fibre held perpendicular to the irradiated surface at a distance of 1 mm, each area irradiated twice for 20 s
- The teeth irradiated for 20 s with a beam of 0.2 W (980 nm, fibre 300 s, continuous-wave mode) and then for 20 s with 3 W DL output power in the first session; the teeth treated for 20 s with a 20 Hz and 0.2 W diode laser beam in the second and third sessions 48 and 96 h, respectively, after the initial visit
3.2.4. Nd: YAG Laser vs. Diode Laser
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Jacobsen, P.L.; Bruce, G. Clinical Dentin Hypersensitivity: Understanding the Causes and Prescribing a Treatment. J. Contemp. Dent. Pract. 2001, 2, 27–34. [Google Scholar] [CrossRef]
- Walters, P.A. Dentinal Hypersensitivity: A Review. J. Contemp. Dent. Pract. 2005, 6, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Cummins, D. Dentin hypersensitivity: From diagnosis to a breakthrough therapy for everyday sensitivity relief. J. Clin. Dent. 2009, 20, 1–9. [Google Scholar] [PubMed]
- Addy, M.; Absi, E.G.; Adams, D. Dentine hypersensitivity. The effects in vitro of acids and dietary substances on root-planed and burred dentine. J. Clin. Periodontol. 1987, 14, 274–279. [Google Scholar] [CrossRef]
- Grippo, J.O. Abfractions: A New Classification of Hard Tissue Lesions of Teeth. J. Esthet. Restor. Dent. 1991, 3, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Gillam, D.G.; Aris, A.; Bulman, J.S.; Newman, H.N.; Ley, F. Dentine hypersensitivity in subjects recruited for clinical trials: Clinical evaluation, prevalence and intra-oral distribution. J. Oral. Rehabil. 2002, 29, 226–231, Erratum in J. Oral. Rehabil. 2003, 30, 446. [Google Scholar] [CrossRef] [PubMed]
- Goh, V.; Corbet, E.F.; Leung, W.K. Impact of dentine hypersensitivity on oral health-related quality of life in individuals receiving supportive periodontal care. J. Clin. Periodontol. 2016, 43, 595–602. [Google Scholar] [CrossRef] [Green Version]
- Canadian Advisory Board on Dentin Hypersensitivity. Consensus-based recommendations for the diagnosis and management of dentin hypersensitivity. J. Can. Dent. Assoc. 2003, 69, 221–226. [Google Scholar]
- Douglas-De-Oliveira, D.W.; Vitor, G.P.; Silveira, J.O.; Martins, C.C.; Costa, F.O.; Cota, L.O.M. Effect of dentin hypersensitivity treatment on oral health related quality of life - a systematic review and meta-analysis. J. Dent. 2017, 71, 1–8. [Google Scholar] [CrossRef]
- Ballini, A.; Tetè, S.; Scattarella, A.; Cantore, S.; Mastrangelo, F.; Papa, F.; Nardi, G.; Perillo, L.; Crincoli, V.; Gherlone, E.; et al. The Role of Anti-Cyclic Citrullinated Peptide Antibody in Periodontal Disease. Int. J. Immunopathol. Pharmacol. 2010, 23, 677–681. [Google Scholar] [CrossRef]
- West, N.X.; Lussi, A.; Seong, J.; Hellwig, E. Dentin hypersensitivity: Pain mechanisms and aetiology of exposed cervical dentin. Clin. Oral Investig. 2013, 17 (Suppl. 1), S9–S19. [Google Scholar] [CrossRef] [Green Version]
- Tugnait, A.; Clerehugh, V. Gingival recession—Its significance and management. J. Dent. 2001, 29, 381–394. [Google Scholar] [CrossRef] [PubMed]
- Crespi, R.; Romanos, G.E.; Cassinelli, C.; Gherlone, E. Effects of Er:YAG Laser and Ultrasonic Treatment on Fibroblast Attachment to Root Surfaces: An In Vitro Study. J. Periodontol. 2006, 77, 1217–1222. [Google Scholar] [CrossRef] [PubMed]
- Schmidlin, P.R.; Sahrmann, P. Current management of dentin hypersensitivity. Clin. Oral Investig. 2012, 17 (Suppl. 1), S55–S59. [Google Scholar] [CrossRef] [Green Version]
- Orchardson, R.; Gillam, D. The efficacy of potassium salts as agents for treating dentin hypersensitivity. J. Orofac. Pain 2000, 14, 9–19. [Google Scholar] [PubMed]
- Poulsen, S.; Errboe, M.; Mevil, Y.L.; Glenny, A.-M. Potassium containing toothpastes for dentine hypersensitivity. Cochrane Database Syst. Rev. 2006, 2006, CD001476. [Google Scholar] [CrossRef]
- Kimura, Y.; Wilder-Smith, P.; Yonaga, K.; Matsumoto, K. Treatment of dentine hypersensitivity by lasers: A review. J. Clin. Periodontol. 2000, 27, 715–721. [Google Scholar] [CrossRef] [Green Version]
- Machado, A.C.; Viana, E.L.; Farias-Neto, A.M.; Braga, M.M.; Eduardo, C.D.P.; de Freitas, P.M.; Aranha, A.C.C. Is photobiomodulation (PBM) effective for the treatment of dentin hypersensitivity? A systematic review. Lasers Med. Sci. 2018, 33, 745–753. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Lopes, A.O.; Aranha, A.C.C. Comparative Evaluation of the Effects of Nd:YAG Laser and a Desensitizer Agent on the Treatment of Dentin Hypersensitivity: A Clinical Study. Photomed. Laser Surg. 2013, 31, 132–138. [Google Scholar] [CrossRef]
- Bou Chebel, F.; Zogheib, C.M.; Baba, N.Z.; Corbani, K.A. Clinical Comparative Evaluation of Nd:YAG Laser and a New Varnish Containing Casein Phosphopeptides-Amorphous Calcium Phosphate for the Treatment of Dentin Hypersensitivity: A Prospective Study. J. Prosthodont. 2018, 27, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Ciaramicoli, M.T.; Carvalho, R.C.; Eduardo, C.P. Treatment of cervical dentin hypersensitivity using neodymium: Yttrium-aluminum-garnet laser. Clinical evaluation. Lasers Surg. Med. 2003, 33, 358–362. [Google Scholar] [CrossRef]
- Birang, R.; Poursamimi, J.; Gutknecht, N.; Lampert, F.; Mir, M. Comparative evaluation of the effects of Nd:YAG and Er:YAG laser in dentin hypersensitivity treatment. Lasers Med Sci. 2006, 22, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Talesara, K.; Kulloli, A.; Shetty, S.; Kathariya, R. Evaluation of potassium binoxalate gel and Nd:YAG laser in the management of dentinal hypersensitivity: A split-mouth clinical and ESEM study. Lasers Med Sci. 2014, 29, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Hu, C. [Dentine hypersensitivity treated with Nd: YAG laser: Experience with 262 cases]. Acad. J. First Med Coll. PLA 2004, 24, 319–320. (In Chinese) [Google Scholar]
- Bal, M.V.; Keskiner, I.; Sezer, U.; Açıkel, C.; Saygun, I. Comparison of Low Level Laser and Arginine-Calcium Carbonate Alone or Combination in the Treatment of Dentin Hypersensitivity: A Randomized Split-Mouth Clinical Study. Photomed. Laser Surg. 2015, 33, 200–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polizzi, E.; Tetè, G.; Targa, C.; Salviato, B.; Ferrini, F.; Gastaldi, G. Evaluation of the Effectiveness of the Use of the Diode Laser in the Reduction of the Volume of the Edematous Gingival Tissue after Causal Therapy. Int. J. Environ. Res. Public Health 2020, 17, 6192. [Google Scholar] [CrossRef]
- Jain, A.; Rao, J.; Pal, N.; Singh, A. Effectiveness of fluoride varnish, diode laser, and their combination in treatment of dentin hypersensitivity: A randomized split-mouth clinical trial. J. Indian Soc. Periodontol. 2020, 24, 369. [Google Scholar] [CrossRef] [PubMed]
- Flecha, O.D.; Azevedo, C.G.; Matos, F.R.; Vieira-Barbosa, N.M.; Ramos-Jorge, M.L.; Gonçalves, P.F.; Silva, E.M.K. Cyanoacrylate Versus Laser in the Treatment of Dentin Hypersensitivity: A Controlled, Randomized, Double-Masked and Non-Inferiority Clinical Trial. J. Periodontol. 2013, 84, 287–294. [Google Scholar] [CrossRef]
- Lopes, A.O.; Eduardo, C.D.P.; Aranha, A.C.C. Clinical evaluation of low-power laser and a desensitizing agent on dentin hypersensitivity. Lasers Med. Sci. 2015, 30, 823–829. [Google Scholar] [CrossRef]
- Femiano, F.; Femiano, R.; Lanza, A.; Festa, M.V.; Rullo, R.; Perillo, L. Efficacy of diode laser in association to sodium fluoride vs Gluma desensitizer on treatment of cervical dentin hypersensitivity. A double blind controlled trial. Am. J. Dent. 2013, 26, 214–218. [Google Scholar]
- Raichur, P.S.; Setty, S.B.; Thakur, S.L. Comparative evaluation of diode laser, stannous fluoride gel, and potassium nitrate gel in the treatment of dentinal hypersensitivity. Gen. Dent. 2013, 61, 66–71. [Google Scholar] [PubMed]
- Yilmaz, H.G.; Kurtulmus-Yilmaz, S.; Cengiz, E. Long-Term Effect of Diode Laser Irradiation Compared to Sodium Fluoride Varnish in the Treatment of Dentine Hypersensitivity in Periodontal Maintenance Patients: A Randomized Controlled Clinical Study. Photomed. Laser Surg. 2011, 29, 721–725. [Google Scholar] [CrossRef]
- Tabibzadeh, Z.; Fekrazad, R.; Esmaeelnejad, A.; Shadkar, M.M.; Sadrabad, Z.K.; Ghojazadeh, M. Effect of combined application of high- and low-intensity lasers on dentin hypersensitivity: A randomized clinical trial. J. Dent. Res. Dent. Clin. Dent. Prospect. 2018, 12, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Suri, I.; Shakir, Q.; Shetty, A.; Bapat, R.; Thakur, R. A comparative evaluation to assess the efficacy of 5% sodium fluoride varnish and diode laser and their combined application in the treatment of dentin hypersensitivity. J. Indian Soc. Periodontol. 2016, 20, 307–314. [Google Scholar] [CrossRef]
- Lopes, A.O.; Eduardo, C.D.P.; Aranha, A.C.C. Evaluation of different treatment protocols for dentin hypersensitivity: An 18-month randomized clinical trial. Lasers Med Sci. 2017, 32, 1023–1030. [Google Scholar] [CrossRef]
- Tabatabaei, M.H.; Chiniforush, N.; Hashemi, G.; Valizadeh, S. Efficacy Comparison of Nd:YAG laser, diode laser and dentine bonding agent in dentine hypersensitivity reduction: A clinical trial. Laser Ther. 2018, 27, 265–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dilsiz, A.; Aydin, T.; Canakci, V.; Gungormus, M. Clinical Evaluation of Er:YAG, Nd:YAG, and Diode Laser Therapy for Desensitization of Teeth with Gingival Recession. Photomed. Laser Surg. 2010, 28, S11–S17. [Google Scholar] [CrossRef]
- Dilsiz, A.; Canakci, V.; Ozdemir, A.; Kaya, Y. Clinical Evaluation of Nd:YAG and 685-nm Diode Laser Therapy for Desensitization of Teeth with Gingival Recession. Photomed. Laser Surg. 2009, 27, 843–848. [Google Scholar] [CrossRef] [Green Version]
- Rezazadeh, F.; Dehghanian, P.; Jafarpour, D. Laser Effects on the Prevention and Treatment of Dentinal Hypersensitivity: A Systematic Review. J. Lasers Med. Sci. 2019, 10, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Flynn, J.; Galloway, R.; Orchardson, R. The incidence of ‘hypersensitive’ teeth in the West of Scotland. J. Dent. 1985, 13, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Irwin, C.R.; McCusker, P. Prevalence of dentine hypersensitivity in general dental population. J. Ir. Dent. Assoc. 1997, 43, 7–9. [Google Scholar]
- Chabanski, M.B.; Gillam, D.G.; Bulman, J.S.; Newman, H.N. Prevalence of cervical dentine sensitivity in a population of patients referredto a specialist Periodontology Department. J. Clin. Periodontol. 1996, 23, 989–992. [Google Scholar] [CrossRef] [PubMed]
- Rees, J.; Jin, L.; Lam, S.; Kudanowska, I.; Vowles, R. The prevalence of dentine hypersensitivity in a hospital clinic population in Hong Kong. J. Dent. 2003, 31, 453–461. [Google Scholar] [CrossRef] [PubMed]
- von Troil, B.; Needleman, I.; Sanz, M. A systematic review of the prevalence of root sensitivity following periodontal therapy. J. Clin. Periodontol. 2002, 29 (Suppl. 3), 173–177. [Google Scholar] [CrossRef]
- Haywood, V.B. Dentine hypersensitivity: Bleaching and restorativeconsiderations. Int. Dent. J. 2002, 52 (Suppl. 5), 376–384. [Google Scholar] [CrossRef]
- Biagi, R.; Cossellu, G.; Sarcina, M.; Pizzamiglio, I.T.; Farronato, G. Laser-assisted treatment of dentinal hypersensitivity: A literature review. Ann. Di Stomatol. 2015, 6, 75. [Google Scholar] [CrossRef]
- Kimura, Y.; Goto, Y.; Kimura, H. Hydrogen sulfide increases glutathione production and suppresses oxidative stress in mitochondria. Antioxid. Redox Signal. 2010, 12, 1–13. [Google Scholar] [CrossRef]
- Sgolastra, F.; Petrucci, A.; Gatto, R.; Monaco, A. Effectiveness of Laser in Dentinal Hypersensitivity Treatment: A Systematic Review. J. Endod. 2011, 37, 297–303. [Google Scholar] [CrossRef]
- Holland, G.R.; Narhi, M.N.; Addy, M.; Gangarosa, L.; Orchardson, R. Guidelines for the design and conduct of clinical trials on dentine hypersensitivity*. J. Clin. Periodontol. 1997, 24, 808–813. [Google Scholar] [CrossRef]
- Liu, H.-C.; Lan, W.-H. The combined effectiveness of the semiconductorlaser with Duraphat in the treatment ofdentin hypersensitivity. J. Clin. Med. Surg. 1994, 12, 315–319. [Google Scholar] [CrossRef]
- Guo, L.; Kayastha, P.K.; Chen, L.; Shakya, M.; Chen, X. Clinical Evaluation of Nd:YAG Laser with and without Dentin Bonding Agent for the Treatment of Occlusal Hypersensitivity. Oper. Dent. 2019, 44, 227–234. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors, Date, and Type of Study | Protocol | N° of Patients | N° of Teeth | Age Frames | Methods of Assessment | Follow-Up | Statistically Relevant | Conclusions |
|---|---|---|---|---|---|---|---|---|
| Lopes AO et al. (2013) [20] Randomized clinical study | 1.5 W at 10 Hz and 100 mJ, 85 J/cm2; four irradiations performed, each for 15 s | 24 | 33 | --- | VAS scale | 6 months | Yes | The combination of Nd: YAG and Gluma Desensitizer is an effective treatment strategy that has immediate and lasting effects. |
| Bou Chebel F et al. (2018) [21] Randomized clinical study | 1 W at 15 Hz for 60 s, twice | 12 | 54 | 20–60 years | VAS scale | 6 months | No | There was no significant difference between the two treatments, Nd: YAG laser and MI Varnish. Both treatments were effective and reduced dentin hypersensitivity immediately after treatment for up to 6 months. |
| Ciaramicoli MT et al. (2003) [22] Randomized clinical study | 1 W at 10 Hz for 60 s at 1064 nm | 20 | 145 | 23–63 years | Friedman Termal Test | 6 months | Yes | The reduction in cervical dentinal hypersensitivity was statistically greater when the etiological factors were removed along with the application of the Nd: YAG laser. |
| Birang R et al. (2007) [23] Randomized clinical study | 1 W at 15 Hz for 60 s, twice | 9 | 63 | --- | VAS scale | 6 months | Yes | The Nd: YAG laser is more effective than the Er: YAG laser in reducing pain in patients. |
| Talesara K et al. (2014) [24] Randomized clinical study | 1 W at 10 Hz for 60 s, each element irradiated twice | 20 | 80 | 25–65 years | VAS scale | 6–9 months | Yes | The Nd: YAG laser was better when intra-group comparison was carried out at 9 months after treatment. Nd: YAG lasers are best in long-term treatment (up to 9 months) due to the dissolution of the dentinal tubules. |
| Hu C et al. (2004) [25] Randomized clinical study | 1 W at 10 Hz for 60 s at 1064 nm | 30 | --- | 23–61 years | VAS scale | 6 months | Yes | The Nd: YAG laser is safe and highly effective in the treatment of dentinal hypersensitivity. |
| Authors, Date, and Type of Study | Protocol | N° of Patients | N° of Teeth | Age Frames | Methods of Assessment | Follow-Up | Statistically Relevant | Conclusions |
|---|---|---|---|---|---|---|---|---|
| Bal MV et al. (2015) [26] Randomized clinical study | 25 mW at 9 Hz for 100 s | 21 | 154 | 20–60 years | VAS scale | 6 months | Yes | Application of LLL or DP containing 8% arginine-calcium carbonate appears to be effective in decreasing DH. However, their combined use does not improve efficacy beyond what is achievable with either treatment alone. |
| Aranha AC et al. (2009) [27] Randomized clinical study | 660 nm/3.8 J/cm2/15 mW | 24 | --- | 20–60 years | VAS scale | 6 months | No | All therapies showed lower VAS sensitivity values than baseline, regardless of their different modes of action. |
| Jain A et al. (2020) [28] Randomized split-mouth clinical study | 810 nm, 0.5 W continuous-emission form; each tooth irradiated for 2 min in non-contact mode | 60 | --- | 20–60 years | VAS scale | 6 months | Yes | The diode laser is significantly more effective in dentinal hypersensitivity treatment for more than 6 months post treatment. |
| Flecha OD (2013) [29] Randomized double-blind clinical study | 685 nm, 25 mW, and 9 Hz for 100 s for three sessions at 72 h intervals | 62 | 434 | --- | Numeric rating scale | 6 months | Yes | Cyanoacrylate is as effective as low-intensity laser in reducing DH. Furthermore, it is a more affordable procedure and can be used safely in DH treatment. |
| Lopes AO et al. (2015) [30] Randomized clinical study | Low-power low-dose diode: 30 mW, 10 J/cm2, 9 s per point, 810 nm, three sessions Low-power high-dose diode: 100 mW, 40 J/cm2, 11 s per point, 810 nm, three sessions | 27 | 55 | 22–53 years | VAS scale | 6 months | Yes | For the low-level lasers, distinct effects were observed for the different doses; however, both were effective in reducing pain for up to 6 months of clinical follow-up. |
| Authors, Data, and Type of Study | Protocol 1 | Protocol 2 | N° of Teeth | Age Frames | Methods of Assessment | Follow-Up | Statistically Relevant | Conclusions |
|---|---|---|---|---|---|---|---|---|
| Femiano F et al. (2013) [31] Randomized clinical study | 980 nm DL applied at 2 W in continuous-wave mode on the surface of the tooth to be treated | Application of 5% NaF varnish + 980 nm DL at 2 W | 262 | 21–64 years | VAS scale | 6 months | Yes | Statistically significant improvements in the VAS scale were found at 1, 3, and 6 months in patients treated with high-power diode laser in combination with 5% NaF. |
| Raichur PS (2013) [32] Randomized clinical study | 980 nm DL applied at 1 W | 108 | 25–45 years | --- | 6 months | Yes | The 940 nm DL was not only effective but also resulted in better immediate relief than potassium fluoride and potassium nitrate gels in reducing DH. | |
| Yilmaz HG (2011) [33] Randomized clinical study | 980 nm DL applied at 1 W | 244 | 18–58 years | VAS scale | 6 months | Yes | Within the limitations of the study, GaAlAs laser irradiation was effective in treating DH and is a more comfortable and faster procedure than traditional DH treatment. | |
| Tabibzadeh Z et al. (2018) [34] Randomized clinical study | 3 W for 20 s at 980 nm and 30 Hz using a 300 µ fiber in pulsed mode once in the first group and three times in the second group | 62 | --- | VAS scale | 6 months | Yes | The use of both high-intensity and combined DL beams results in significantly reduced DH. There was no significant difference between combined and single-laser therapies in the treatment of tooth hypersensitivity. | |
| Suri I et al. (2016) [35] Randomized clinical study | 980 nm DL applied at 2 W in continuous-wave, non-contact mode using a 320 µ fiber radiated at 1 mm, each area irradiated twice for 20 s | Application of 5% NaF varnish + 980 nm DL at 2 W | --- | 20–59 years | VAS scale | 6 months | Yes | Although all three groups showed improved DH reduction, 5% NaF paint with DL showed the best results among all groups. |
| Authors, Date, and Type of Study | Protocol 1 | Protocol 2 | N° of Patients | N° of Teeth | Age Frames | Methods of Assessment | Follow-Up | Statistically Relevant | Conclusions |
|---|---|---|---|---|---|---|---|---|---|
| Lopes AO et al. (2017) [36] Randomized clinical study | Nd: YAG: 1.0 W, 10 Hz, 100 mJ, ≈85 J/cm2, 1064 nm | Low-power low-dose diode: 30 mW, 10 J/cm2, 9 s per point, 810 nm, three sessions Low-power high-dose diode: 100 mW, 40 J/cm2, 11 s per point, 810 nm, three sessions | 32 | 117 | 22–53 years | VAS scale | 18 months | No | After statistical analysis, all treatments were shown to be effective in reducing dentin hypersensitivity, and the results were considered not statistically different from those at 12 and 18 months. |
| Tabatabaei MH et al. (2018) [37] Randomized clinical study | Nd: YAG: 1.0 W, 10 Hz, 100 mJ, ≈85 J/cm2, 1064 nm | 810 nm at 30 mW for 9 s per point | 22 | 135 | 25–58 years | VAS scale | 6 months | Yes | The efficacy of the Nd: YAG laser in reducing dentin hypersensitivity was significantly superior to that of other modalities at 3 and 6 months. |
| Dilsiz A et al. (2010) [38] Randomized clinical study | Nd: YAG: 1064 nm, 100 mJ/pulsed mode, 15 Hz, 100 s | Laser diode: 808 nm at 100 mW for 20 s | 24 | 96 | 18–52 years | VAS scale | 3 months | Yes | Er: YAG, Nd: YAG, and diode lasers can be used to reduce DH. Nd: YAG laser irradiation is more effective in treating DH than Er: YAG and diode laser. Within the limitations of the study, the Nd: YAG laser appeared to be a suitable tool for successful DH reduction, especially since the 3 month results of this treatment modality are promising. |
| Dilsiz A et al. (2009) [39] Randomized clinical study | Nd: YAG: 1 W and 10 Hz for 60 s at 1064 nm | Laser diode: 685 nm at 25 mW and 9 Hz for 100 s | 14 | 56 | 19–51 years | VAS scale | 3 months | Yes | Desensitivity of teeth with gingival recession was more effective with the Nd: YAG laser than with the diode laser. The Nd: YAG laser appears to be a promising new tool for successfully reducing DH. |
| Rezazadeh F et al. (2019) [40] Review of the literature | 32 | 117 | 22–53 years | VAS scale | --- | Yes | Among the various types of lasers, the application of the Nd: YAG laser has shown the best results in the treatment of dentinal hypersensitivity. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cattoni, F.; Ferrante, L.; Mandile, S.; Tetè, G.; Polizzi, E.M.; Gastaldi, G. Comparison of Lasers and Desensitizing Agents in Dentinal Hypersensitivity Therapy. Dent. J. 2023, 11, 63. https://doi.org/10.3390/dj11030063
Cattoni F, Ferrante L, Mandile S, Tetè G, Polizzi EM, Gastaldi G. Comparison of Lasers and Desensitizing Agents in Dentinal Hypersensitivity Therapy. Dentistry Journal. 2023; 11(3):63. https://doi.org/10.3390/dj11030063
Chicago/Turabian StyleCattoni, Francesca, Lucrezia Ferrante, Sara Mandile, Giulia Tetè, Elisabetta Maria Polizzi, and Giorgio Gastaldi. 2023. "Comparison of Lasers and Desensitizing Agents in Dentinal Hypersensitivity Therapy" Dentistry Journal 11, no. 3: 63. https://doi.org/10.3390/dj11030063